
Abstract
An 11-year-old, spayed female domestic shorthair cat was presented for a right flank wound. On clinical examination, a single non-painful skin tear lesion with irregular edges was detected. During the examination, star-shaped cigarette paper-like skin lesions appeared spontaneously. An abdominal mass was also palpated. Feline skin fragility syndrome (FSFS) was suspected and a multicentric lymphoma was diagnosed by fine needle aspiration. The cat’s condition declined and it died spontaneously. Post-mortem examination confirmed the diagnosis of lymphoma. Neoplastic lymphocytes were not observed in the skin. Histological analysis of the skin was consistent with the morphological aspects of FSFS. A possible direct link between the two conditions remains a matter of speculation, but this case report provides the first description of FSFS associated with multicentric follicular lymphoma. Thus, multicentric follicular lymphoma should be considered as a differential diagnosis in cats presenting with FSFS.
Case Report
Acquired feline skin fragility syndrome (FSFS) is a rare disorder. Affected animals have extremely fragile skin and often suffer from other severe and serious underlying diseases.1–3 We provide here the first report of a case of FSFS associated with multicentric follicular lymphoma.
An 11-year-old spayed female domestic shorthair cat weighing 2.5 kg was presented with an 8-day-old wound to the right flank without any other clinical sign. The cat lived exclusively indoors with two congeners with no dermatological signs. One of these cats tested positive by enzyme-linked immunosorbent assay (ELISA) for feline leukaemia virus (FeLV) antigen p27 and the other tested positive for serum antibodies against feline immunodeficiency virus (FIV). The cat’s vaccinations were not up-to-date. It was fed commercially-prepared dry and wet cat food, with occasional raw fish (salmon, tuna). The cat had an insignificant medical history, with the exception of gingivitis diagnosed by the veterinary surgeon 9 months before admission and treated with doxycycline (20 mg q24h over 15 days). At the time, serum biochemistry tests showed alkaline phosphatase (ALP) activity to be above the upper limit of the reference interval at 184 IU/l (reference interval 20–90 IU/l). The cat had not been seen by any other veterinary surgeon in the meantime and was not receiving any medication at the time of admission.
On initial physical examination, rectal temperature was 37.8°C, and the cat was considered to be 5% dehydrated. The mucous membranes were pale. A cranial abdominal mass was palpated. The skin was thin with no scarring or hyperextensibility, and the blood vessels were clearly visible. The cat had a single, non-painful skin tear with irregular edges on the right flank. This lesion was 7 cm long and 2 cm wide revealing the underlying muscle, without bleeding (Figure 1). Star-shaped cigarette paper-like skin lesions were visible on the abdomen and during physical examination and restraint some of them tore spontaneously.

Feline acquired skin fragility with a skin tear (see the general view of the cat on the top left corner for localisation)
The urine had a specific gravity of >1.060 and no abnormality was detected on urine analysis. Serum biochemistry (Prestige 24i Chemistry Analyzer, Tokyo Boeki Medical System; Nova Biomedical) findings included ALP activity and bilirubin concentration above the upper limit of the reference interval, and albumin concentration below the lower limit of the reference interval (Table 1). Activated coagulation time was 131 s (reference interval 70–120 s) and thrombin (Coag Dx Analyzer; Idexx Laboratories) time was 28 s (reference interval 15–23 s). Major abnormalities were detected for complete blood counts (Sysmex XT 2000iV Analyzer; Sysmex Corporation): lymphocyte leukocytosis with no morphological abnormality, monocytosis and regenerative anaemia (Table 2).
Serum biochemistry results for the cat with skin fragility syndrome and multicentric follicular lymphoma
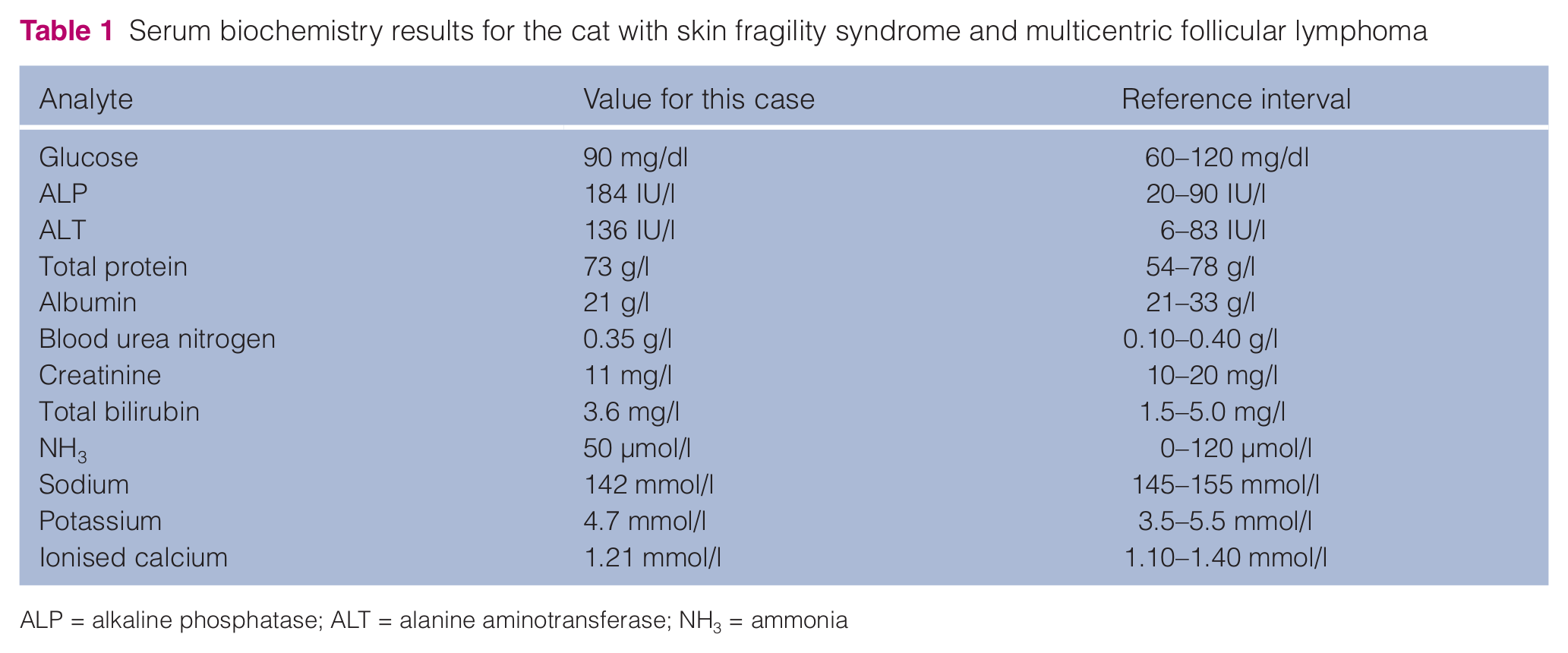
ALP = alkaline phosphatase; ALT = alanine aminotransferase; NH3 = ammonia
Haematological findings for the cat with skin fragility syndrome and multicentric follicular lymphoma

Abdominal echography (ATL HDI 5000 Ultrasound System) revealed a moderate amount of peritoneal fluid associated with severe hepatomegaly, splenomegaly and pancreas enlargement. A generalised thickening of the gastrointestinal tract was also observed. Abdominal lymphadenopathy was noted. The adrenal glands were normal in shape and size: the right adrenal gland was 0.68 cm long and 0.31 cm thick; the left adrenal gland was 0.72 cm long and 0.27 cm thick.4,5
Cytological examination of liver samples obtained by ultrasound-guided fine-needle aspiration showed normal hepatocytes and large numbers of lymphoid cells with round nuclei, readily visible nucleoli and abundant basophil cytoplasm, suggesting malignancy. Minimal levels of anisocytosis and anisokaryosis were observed. Similar neoplastic lymphoid cells were identified after ultrasound-guided fine-needle aspiration of the spleen, pancreas and mesenteric lymph node, consistent with a diagnosis of lymphoma.
ELISA (SNAP FIV/FeLV Combo Test; Idexx Laboratories) tests on blood for FeLV and FIV were negative. The urine cortisol:creatinine ratio (UCCR) (Immulite cortisol, Siemens Medical Solutions Diagnostics; Konelab creatinine (Enzymatic), Thermo Fisher Scientific) was within the reference interval (17 × 10-6; reference interval 4–36 × 10-6).
At this time, the cat’s condition declined and it died spontaneously. Post-mortem examination showed a poor body condition with enlarged abdominal lymphatic nodes. The skin was thin, with several areas of hair loss. There was a skin tear, 7 cm × 2 cm in size, on the skin of the right flank. The liver was heterogeneous, enlarged and infiltrated with numerous nodules. The spleen was pale and enlarged. The adrenal glands, pituitary gland and other organs were normal macroscopically. Histopathological analysis showed a population of numerous neoplastic lymphocytes forming large lymphoid follicles with a prominent germinal centre infiltrating numerous lymph nodes, including the pancreatic, mesenteric and colic nodes. The cells were round, of small-to-medium size, with a scant basophilic cytoplasm and a round nucleolated, sometimes notched, nucleus. They were predominantly centrocytes and centroblasts. Anisocytosis and anisokaryosis were moderate and the mitotic index was low. These morphological characteristics were suggestive of a multicentric follicular lymphoma. 6 A portal and periportal lymphoid infiltrate was observed in the liver that resembled the tumour follicles observed in lymph nodes (Figure 2). The spleen, small intestine, colon, pancreas and bone marrow were also infiltrated with several tumour cell follicles, whereas the kidneys, lungs, parathyroid and pituitary glands were involved to a lesser extent. Liver immunohistochemistry using CD3 antibody against T lymphocytes (Monoclonal Mouse Anti-Human CD3 antibody, clone F7.2.38; Dako) and CD20 antibody against B lymphocytes (Mouse Anti-Human CD20cy, clone L26; Dako) revealed a B labelling of the centrofollicular cells and B and T cells around the follicles. These characteristics confirmed the diagnosis of a multicentric follicular mixed low-grade lymphoma

Photomicrographs of the liver. (a) In the liver, a portal and periportal lymphoid infiltrate is present. Lymphoid cells formed numerous follicles (green arrows) disseminated in the parenchyma, sometimes coalescing, with a large germinal center (G) and an irregular darker peripheral ring (R). (b) A follicle with a large germinal centre (*) composed of neoplastic lymphocytes. (c) On closer magnification, the cells are spherical, have small irregular nuclei and a scant basophilic cytoplasm. Around the follicle, the parenchyma is infiltrated more diffusely. Haematoxylin–eosin–saffron staining
Histopathological examination of the skin revealed an atrophied (single layer of nucleated keratinocytes) epidermis and extreme atrophy of the dermis (Figure 3). The collagen fibres were few in number, thin and fragmented. There were also few hair follicles and they were in the telogen phase. They were atrophic in appearance, and the epithelium was thin and consisted of a single layer of cells. A mixed inflammatory infiltrate consisting of normal lymphocytes, macrophages and plasma cells was present in some cutaneous sections as a secondary inflammation without B cell immunolabelling. On these slides, the arrector pili muscles were prominent. At some sites, a granulation tissue overlaid by fibrin was present in the dermis corresponding to older lesions and underlying epidermal tears. These findings are consistent with atrophic dermal connective tissue, reflecting the morphological features of skin fragility syndrome.
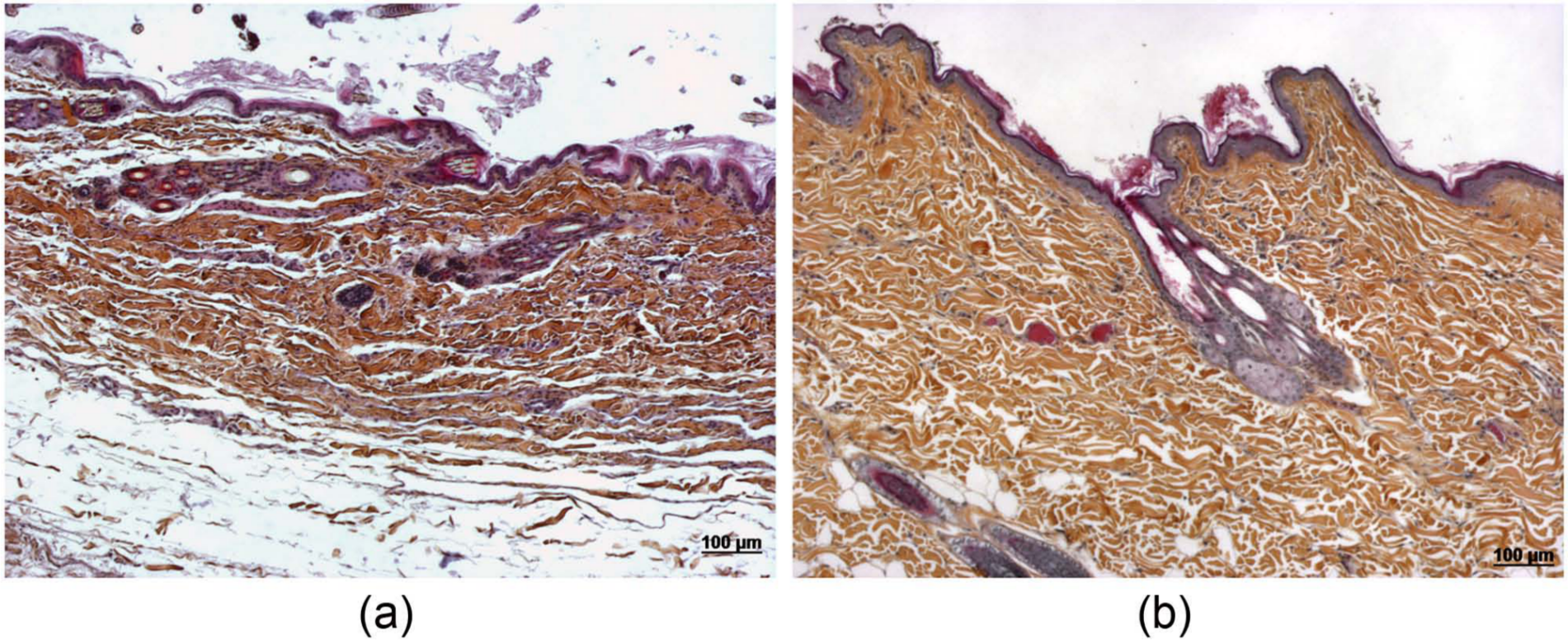
(a) Photomicrograph of the skin of the cat (right flank). Epidermal and dermal atrophy. (b) Photomicrograph of a section of the skin of a normal cat (matched to the location on the body). Haematoxylin–eosin–saffron staining
Discussion
Acquired FSFS is a rare disorder of multifactorial aetiology characterised by extreme fragility of the skin and an absence of hyperextensibility. It must be differentiated from congenital cutaneous asthenia (Ehlers–Danlos syndrome), which is reported in animals from a very early age and is characterised by skin elasticity and extensibility progressing spontaneously to skin lesions.7,8 Fewer than 12 cases of FSFS have been described in the literature.9–19 All occurred in middle-aged-to-old cats with no history of dermatological signs before onset. In most of these cases, FSFS was observed in association with a serious disease, as observed here.10,11,17–20 The most common cause of acquired FSFS is spontaneous or iatrogenic hyperadrenocorticism.2,20,21 The clinical signs displayed by cats with feline hyperadrenocorticism include poorly-controlled diabetes mellitus associated with polyuria and polydipsia, weight loss, polyphagia, abdominal distension, muscle weakness and lethargy. In most cases, the cat has a pot-bellied appearance and muscle atrophy. However, we were able to exclude this disease in the case reported here based on the absence of these clinical features and a UCCR result within the reference interval — this test having been chosen for its high sensitivity. Furthermore, ultrasound scan measurements showed that both adrenal glands were similar in size to those of healthy cats.4,5 Post-mortem examination and histological analyses of the adrenal and pituitary glands identified no abnormality of corticotrophs or adrenocortical cells — definitively ruling out this disease.
Histological examination of the necropsy skin specimens was entirely consistent with FSFS 3 and no infiltration by tumoural lymphocytes was detected in the skin. To our knowledge, this is the first report of an association between FSFS and lymphoma. This cat displayed extensive infiltration of the liver, associated with an increase in liver enzyme activity in serum and biochemical modifications suggestive of liver insufficiency (hypoalbuminaemia, hyperbilirubinaemia, long coagulation times) and pancreatic infiltration.
With the exception of the confirmed cases of hyperadrenocorticism, the pancreatic and liver involvement observed here resembled that in all other described cases of FSFS, with cholangiocarcinoma, 10 pancreatic and hepatic carcinoma, 16 hepatic lipidosis with feline infectious peritonitis, 17 cholangiohepatitis and hepatic lipidosis 18 and recently, disseminated histoplasmosis extending to the liver parenchyma. 19 Similar to the present case, these cats died spontaneously without therapeutic response or were euthanased. Thus, it is not possible to demonstrate definitively a causal relationship between any of these conditions and FSFS.
The pathophysiology of acquired FSFS is entirely unknown. In animals with extra-adrenal diseases, a role for adrenal gland steroids in the general context of the stress response has been considered occasionally because of the common association of FSFS with hyperadrenocorticism.17,20,22 Conversely, steroid hepatopathy has been described in some cats with skin fragility associated with hyperadrenocorticism, again calling into question the role of liver involvement in the pathophysiology of the disease.12,13
Lymphoma localised to the dermis and epidermis has been described in cats.23,24 Classical dermatological signs include erythematous plaques or patches that may mimic eosinophilic plaques in case of epitheliotropic lymphoma, scaly alopecic patches, non-healing ulcers or nodules. No dermatological sign consistent with epitheliotropic or non-epitheliotropic lymphoma was identified in this cat. Moreover, histological analysis provided no evidence of infiltration of the cutaneous tissue by the lymphoma.
Conclusions
This is the first description of FSFS associated with a multicentric follicular lymphoma. We cannot rule out the possibility of this association being incidental in this case but, subject to confirmation in other cases, it may be necessary to include lymphoma on the list of differential diagnoses associated with FSFS.
Footnotes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this case report.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.