
Abstract
Practical relevance:
Many cats develop cancer and may or may not present with an obvious mass lesion. As our feline patients are living longer and their owners are increasingly seeking veterinary care, the apparent incidence and prevalence of cancer is increasing.
Clinical challenges:
Neoplasia is a differential for many clinical presentations in cats. Often tumours are relatively advanced at the point of presentation, and this can make management difficult. In addition, many cats find clinic visits stressful and this can influence owners’ decisions about treatment.
Audience:
This review provides an overview of the approach to the feline cancer patient, and is aimed at all veterinary practitioners that see cats. It is intended as a starting point for more detailed discussions in accompanying articles in this special issue on feline oncology.
Evidence base:
There is limited data on most feline tumours compared with tumours in canine or human patients, so a robust evidence base is often lacking.
Cancer in cats
The most common tumours in cats are summarised with their presenting features and differentials in Table 1, and some are illustrated on page 368. Often, there may be non-neoplastic differentials for mass lesions as cats develop more granulomatous lesions than other species. They can also develop quite marked lymphadenopathy due to reactive or infectious causes. Furthermore, extranodal lymphoma can arise at any site, and is much more common in feline patients than in their canine counterparts, as are the alimentary/abdominal and cranial mediastinal forms of the disease.
Common tumours in cats – clinical signs and differentials


Intestinal lymphoma, with renal involvement, in the elderly MN DSH cat pictured in Figure 1. This lateral abdominal radiograph shows gastric/intestinal gravel sign consistent with partial obstruction, a large mid-ventral abdominal soft tissue mass, and a rounded irregular enlarged renal shadow. The cat responded well to cyclophosphamide, vincristine and prednisolone, but on relapse did not respond to rescue therapy. Survival time was 7 months

Oral mass, diagnosed as lymphoma, in an adult female neutered (FN) DSH cat (recently rescued). The cat responded well to cyclophosphamide, vincristine and prednisolone and had a survival time of more than 2 years

Unresectable sublingual and lingual squamous cell carcinoma in an 8-year-old MN DSH cat. There was no response to palliative medical therapy or chemotherapy and the cat was euthanased 3 weeks after diagnosis
Advanced rhinarial squamous cell carcinoma in an 8-year-old MN DSH cat, presented for radiation therapy. Short-term palliation was achieved

Early cutaneous squamous cell carcinoma in a 17-year-old FN DSH cat that presented for postoperative radiation therapy of a labial squamous cell carcinoma. Surgical excision of this mass was curative, but there was relapse at the site of the labial squamous cell carcinoma after 5 months

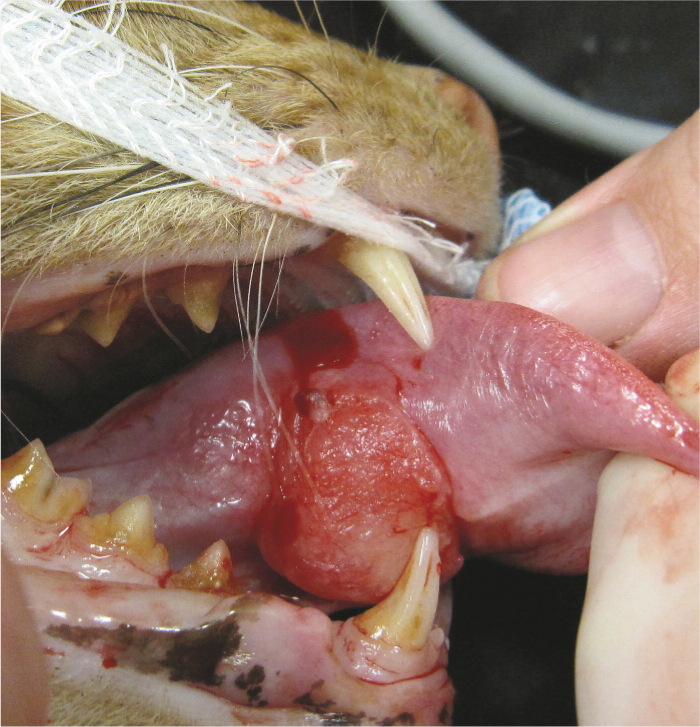
Maxillary fibrosarcoma causing gross facial distortion in an 11-year-old FN DSH cat. Suture is present from a recent biopsy

Large soft tissue sarcoma (suspected injection site-associated sarcoma) in an adult MN DSH cat

Clinical signs
Patients with cancer may present with a mass lesion (eg, a palpable mammary lesion) or with signs secondary to a mass such as halitosis, poor grooming or a malodorous coat in those with oral masses. The different behaviour patterns of individual cats affect how quickly mass lesions are noted and, unfortunately, many cats present late in the disease course. Cats with cancer may present with non-specific signs, such as alterations in appetite, reduced activity levels or weight loss (Figure 1). Nonetheless, a great deal of information can be obtained from clinical examination in cats, as abdominal masses are often readily palpable, and changes in thoracic compressibility may be apparent where there is a cranial mediastinal mass.

Elderly male neutered (MN) domestic shorthair (DSH) cat, which presented with weight loss due to alimentary and renal lymphoma
Some cats present with clinical signs of metastatic disease rather than signs relating to the primary tumour. This is seen most often in cases of lung–digit syndrome (Figure 2), where patients present with metastatic lesions of the digits (usually multiple) secondary to primary lung tumours.1,2 Cats may also infrequently present with signs due to paraneoplastic disease. Cutaneous manifestations of neoplasia are uncommon but dramatic (eg, paraneoplastic alopecia in pancreatic, hepatic or bile duct carcinoma; exfoliative dermatitis with thymoma), and neoplasia should be a differential for cats presenting with these dermatological complaints (Figure 3).3–6
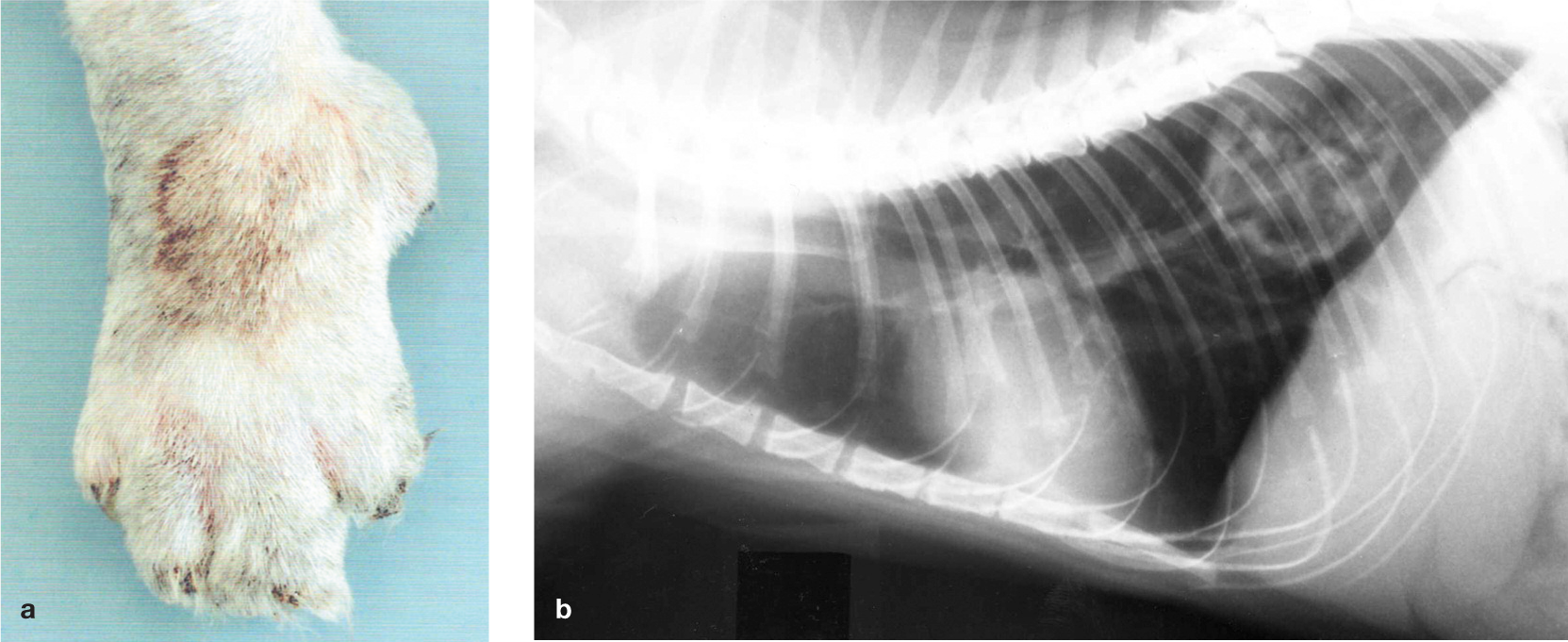
Lung–digit syndrome in an adult DSH cat. The patient presented to the orthopaedic service at the author’s hospital for investigation of lameness and digital swellings (a). A pulmonary mass was found on thoracic radiography, as demonstrated by the right lateral view shown in (b). Reproduced from Corr and Blackwood (2003) 2

Severe exfoliative dermatitis, seborrhoea and alopecia in a 14-year-old MN DSH cat that was presented as a dermatology referral (a). A pulmonary mass was found on thoracic radiography (dorsoventral view, b) and confirmed cytologically as an adenocarcinoma. Courtesy of Dr Tim Nuttall
Getting a diagnosis
Key to appropriately managing cancer cases is having an accurate diagnosis, so that correct tumour staging can be performed and the best treatment recommended. Clinical features typical of a malignant tumour include rapid growth, fixation, invasion into deep tissues or overlying skin, ulceration and poorly defined margins. Clinical criteria can suggest a lesion is malignant, but apparently less aggressive behaviour should not result in the lesion being assumed benign. For example, aggressive mesenchymal tumours may appear well demarcated due to pseudocapsule formation. Sampling of mass lesions by cytology or histology is required.
The advantages and disadvantages of cytology and histopathology are summarised in the box below. Neither technique is 100% sensitive or specific in the diagnosis of tumours, although histopathology remains the gold standard.

Sampling by cytology
Cytology will usually differentiate between neoplastic and inflammatory lesions, and determine if tumours are malignant or benign. Cytology will also broadly ascertain tumour type (epithelial, mesenchymal or round cell tumour) but not the exact histogenesis; for example, sarcoma may be diagnosed, but histology will be required to determine the tissue of origin. There are other pitfalls to be wary of too: dysplastic epithelial or mesenchymal cells may mimic neoplastic change, and this is particularly problematic where there is concurrent inflammation.
Fine needle aspirates may be non-diagnostic due to low yield in some sarcomas. In cats, fine needle aspirates from lymph nodes are less likely to be diagnostic of lymphoma than in dogs, and it may be impossible for the clinical pathologist to differentiate lymphoma from a very reactive node; in many cases, biopsy is required. However, fine needle aspirates are very useful in extranodal lymphoma, and cytology of bone marrow may help support a diagnosis of CNS lymphoma as many affected cats are reported to have bone marrow involvement.
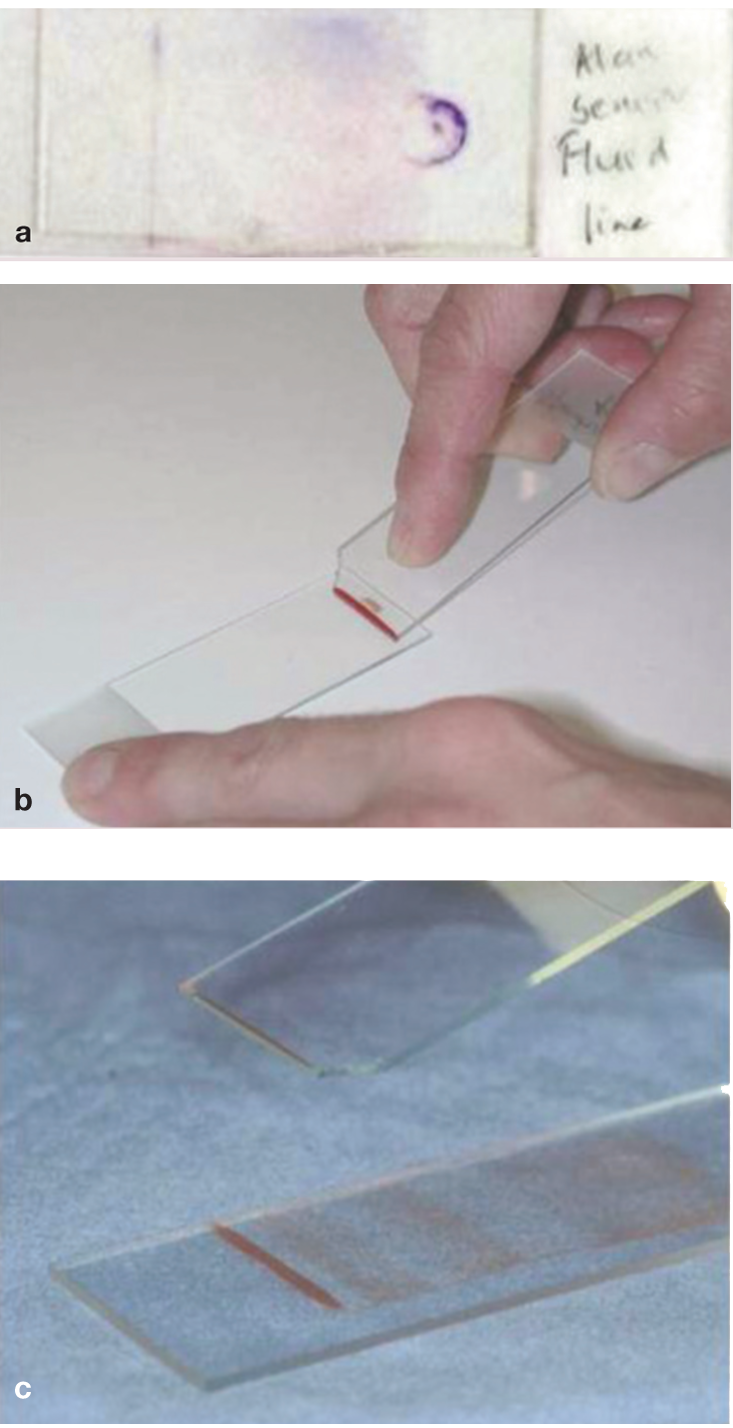
Cytology is also very useful in making a diagnosis from fluid samples. In cases of suspected neoplastic effusion, the detection of tumour cells in samples with low cellularity can be enhanced by preparing a sediment smear (see box).

(a) ‘Line smear’ from a thoracic effusion. The smear is prepared in the same way as a blood smear, but instead of creating a feathered edge, the aim is to create a line where cells are concentrated together. This is achieved by abruptly stopping smearing mid-way and lifting the smearing slide off, creating a line. The technique is illustrated in (b) and (c) using a bloody sample for easy visualisation
Sampling by biopsy
Biopsy is more invasive than harvesting samples for cytology, and there are increased risks of haemorrhage, transplantation of tumour cells, compromise of future surgery and damage to adjacent structures, although good technique minimises these risks. If suspicious of an infectious cause, it is advisable not to fix all biopsy tissue so the procedure does not have to be repeated to perform bacterial, fungal or mycobacterial culture.

(a) Unilateral nasal discharge in a 2-year-old MN Siamese cat. Biopsies in this case confirmed lymphoma. When taking biopsies from nasal tumours, it is important first to measure the grab biopsy forceps or cut-off urinary catheter – either against the patient so that the biopsy/catheter is not inserted any further than the level of the medial canthus, or against a dorsoventral intraoral radiograph (b) to ensure the biopsy/catheter ends within tumour and cranial to the cribriform plate

Clinical staging
Clinical staging involves assessment of the primary tumour (T), including involvement of adjacent structures, and assessment for metastasis to local and regional lymph nodes (N) and distant sites (M). The aim of TMN staging is to inform clinical decision making and ensure the best treatment possible under the individual circumstances of the case.
Assessment of the primary tumour should include evaluation of extent, by clinical examination and appropriate diagnostic imaging or endoscopic techniques, and a diagnosis of tumour type based on cytology or histology (see earlier). The sensitivity of tests should be borne in mind. For example, clinical examination of a maxillary squamous cell carcinoma may suggest a less extensive tumour than would radiography, which in turn is less sensitive than computed tomography (CT).
Exploratory laparotomy in a suspected or confirmed cancer patient should always contribute to tumour staging (see box).

Lymph node evaluation
Carcinomas most commonly metastasise by the lymphatic route, and local and regional lymph nodes should be evaluated in cats with carcinoma by palpation (eg, of axillary and inguinal nodes in cats with mammary tumours), diagnostic imaging, and aspiration and cytology. Mast cell tumours also metastasise by the lymphatic route, but reported metastatic rates for cutaneous mast cell tumours in cats vary, ranging from 0–22%, and most histologically well-differentiated tumours have a low metastatic potential. Poorly differentiated tumours are more malignant. (Visceral mast cell tumours are generally malignant and metastases may be widespread at presentation.)
Thoracic radiographs
Primary lung tumours are relatively readily diagnosed radiographically (Figures 2 and 3). Compared with dogs, cats less frequently develop classical well-defined ‘cannon ball’ metastases, and metastatic disease can appear as ill-defined mass lesions or diffuse alveolar, interstitial or mixed patterns (Figure 5). 9 A bronchial component is relatively common in metastatic patterns in bronchoalveolar carcinoma. 10 Cytology of lung aspirates or broncho alveolar lavage fluid may be required to confirm a diagnosis.

Lateral thoracic radiograph (inflated) of an elderly FN DSH cat. Multiple poorly defined soft tissue opacities are seen, which represent metastases from an unknown primary. There are also increased interstitial and bronchial markings
Abdominal ultrasound
Mass lesions and markedly enlarged lymph nodes may be detectable on abdominal palpation, but abdominal ultrasound allows detection of lesions not apparent on clinical examination, including lesions within hepatic, splenic and renal parenchyma, as well as changes in layering of the gastrointestinal tract and more subtle lymph node enlargement.
Advanced imaging
Advanced imaging is increasingly available for veterinary patients, and is very valuable. However, it is expensive, and, as with any diagnostic test, should be utilised with full consideration of the value of the study and the cost implications for future management of the case. When mass lesions are found, samples should be harvested to allow a diagnosis.

(a) Transverse CT scan of an 8-year-old MN DSH cat with poorly controlled diabetes mellitus due to acromegaly, showing a mass in the pituitary fossa. The positioning device seen is a thermoplastic mould, which is shaped round the patient, whose head is supported on a mouldable pillow (not visible on this window). The mould is secured to a baseplate. (b) CT scan of a 7-year-old FN cat with a nasal tumour (extending into the orbit) after positioning in the same mould system (c)
Blood tests
Most blood tests do not help to make a diagnosis of cancer in cats, but they can help to identify common co-morbidities, and this can be very important in decision making.
On haematology, there may be a mild non-regenerative anaemia and a stress haemogram. These are the commonest findings in lymphoma patients. 11 Abnormal circulating cells and/or lymphocytosis is relatively uncommon. Even in cats with leukaemia, there may be no abnormal circulating cells on haematology.
On biochemistry, changes are often non-specific and may reflect stress (eg, hyperglycaemia), co-morbidity or organ involvement (eg, hypoalbuminaemia in diffuse alimentary lymphoma). Urine specific gravity should be measured in azotaemic patients to confirm renal or pre-renal origin. (Urine specific gravity will be low in azotaemic hyper calcaemic patients even if the renal concentrating ability is normal because of antagonism of antidiuretic hormone.) Paraneoplastic hypercalcaemia is uncommon in cases of feline lymphoma, and is more commonly seen in patients with myeloma. Hypercalcaemia can also be seen with other tumours, particularly carcinomas.
In the UK, most cats with lymphoma now are FeLV antigen negative on ELISA. However, testing is valid where there is an infection risk to others, and where concurrent disease may affect treatment decision making.
Treatment options and considerations
In broad terms, surgery and radiotherapy can be considered as local treatments for primary disease or primary disease with local lymph node involvment, and chemotherapy as systemic treatment for disseminated disease.
Surgery
In cats, treatment of primary mass lesions may be limited by small patient size and difficulties in achieving wide local excision. However, surgery remains the mainstay of treatment for solid tumours.
Mammary tumours are most often resected by radical mastectomy, as most feline mamma-ry tumours are malignant. Both axillary and inguinal lymph nodes on the affected side should be resected en bloc with the mammary tissue, but often the axillary nodes are not removed if deemed normal as they are less readily identifiable than the inguinal nodes. Local excision of malignant mammary tumours is associated with a high rate of recurrence.
Oral tumours are often unresectable by the time of presentation: the overall cure rate for oral squamous cell carcinoma is less than 5%. Where excision is possible, consideration should be given to placing a feeding tube at the time of surgery to facilitate postoperative care and recovery, as cats may cope less well with, for example, mandibulectomy than dogs do, particularly in the immediate postoperative period. Cosmetic and functional results may be very good in the longer term (Figure 7).

An 8-year-old MN DSH cat, which presented with an early mandibular fibrosarcoma. A partial mandibulectomy was performed, and a feeding tube placed, visible in (a), which shows the patient 2 days postsurgery. (b) The cat 6 months later. In this case, surgery was curative, but complete excision of feline oral tumours is frequently impossible
Excision of soft tissue sarcomas, which may have extensive fronds of invading tumour cells, is particularly challenging in small patients, and compartmental excision is only achievable for tumours on (distal) limbs.
Radiotherapy
Radiation therapy is most often used either as a postoperative adjunctive therapy, ideally in a minimal residual disease setting, or palliatively in the face of unresectable gross disease. When radiation is used postoperatively, it is very important to ensure that the radiation therapist is aware of the original tumour site, extent and dimensions, or the planned radiation field may not include all of the affected tissue. This can result in a geographical miss, where microscopic residual disease is not included in the treated area. The risk of geographical miss increases as repeat surgeries are performed and normal anatomy becomes increasingly distorted.
The best results are likely to be achieved if radiotherapy is considered prior to surgery, and presurgical measurements and images are available (ie, photographs with measurements, drawings, radiographic or other images) to help plan the treatment. Placement of metal surgical clips at the margins of the surgical bed also helps to avoid geographical miss during radiotherapy, as there may be migration of subcutaneous tissues that may contain residual tumour (Figure 8).

Dorsoventral radiograph obtained to check the radiation field in an adult MN DSH cat receiving postoperative adjunctive radiation therapy for an incompletely resected soft tissue sarcoma. The solid line is the scar, and dots represent a margin round this of 5 cm. Two of the dots along the caudal margin are joined by a dotted line to show where the caudal edge of the treatment field lies. Two clips are positioned beyond (caudal to) this margin, indicating that a larger margin must be used. This illustrates the limitations of basing radiation treatment fields on surgical scars
In the clinic, radiation therapy is used to treat feline patients in a variety of ways (see box).


A 9-year-old MN Birman being prepared for postoperative adjunctive radiation therapy using electrons, for treatment of an incompletely excised, high grade injection site-associated sarcoma. The electron applicator has a cut out made to shape the field for the individual patient. The treatment field is illuminated on the patient. Unfortunately, this cat, which also received chemotherapy with epirubicin, developed widespread metastatic disease (but no local recurrence) 18 months after radiotherapy

A 14-year-old MN DSH cat with a maxillary squamous cell carcinoma at the beginning (a) and end (b) of a course of hypofractionated radiation therapy for a gingival squamous cell carcinoma. After an initial favourable response, the tumour recurred and the patient was euthanased just over 3 months after radiotherapy
Chemotherapy
Chemotherapy is used where systemic delivery of treatment is required to treat widely disseminated but chemoresponsive disease (eg, lymphoma) or where there is a high risk of development of metastatic disease and micrometastases are likely to be present (eg, some high grade sarcomas). It is generally not a suitable option as the primary treatment for a large solid non-lymphoid tumour, which is likely to be poorly chemosensitive.
Further discussion on the use of chemotherapy and targeted therapies in cats, with a particular focus on the idiosyncracies of feline patients, is provided in an accompanying article in this special issue.
Footnotes
Key Points
Funding
The author received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this article.
Conflict of interest
The author does not have any potential conflicts of interest to declare.