
Abstract
A 10-year-old spayed female chinchilla feline presented with gradually progressive tetraparesis and cervical pain that had begun 1 month before the onset of a 4-day tetraplegic episode. Magnetic resonance imaging revealed a large elliptical intramedullary mass at the fourth cervical vertebrae. The mass was removed surgically and diagnosed as an anaplastic astrocytoma. No neurological abnormalities were observed 3 weeks postsurgery. Magnetic resonance at 3.5 year follow-up revealed neither mass regrowth nor recurrence of signs.
Case Report
Spinal cord tumours are typically classified as extradural, intradural extramedullary or intramedullary based upon the relationship between the tumour and the meninges. 1 Extradural tumours include primary and secondary vertebral and soft tissue tumours. 1 Osteosarc-omas,2–9 fibrosarcomas,2–5 chondrosarcomas,2–5 undifferentiated sarcomas,2,3 plasma cell tumours,2,3 histiocytic tumours,2,3 peripheral nerve sheath tumours (PNSTs),2–5 lipomas,4,5 chordomas, 5 paragangliomas, 5 neurolemmomas 10 and metastatic tumours2,3 have been reported in felines. Meningiomas2–5,11–15 and PNSTs2–5 have been reported as intradural extramedullary tumours in felines. Intramedullary tumours are encountered rarely in animals, including primary spinal parencymal tumours and metastatic tumours. 1 Glial tumours2,3,16,17 and primitive neuroectodermal tumours (PNETs)2,3 are reported in felines. Of all the types of tumours, lymphomas are the most likely to induce spinal cord dysfunction in felines. Lymphomas develop in both the extradural and intradural space,2,3,18,19 and may involve the nerve roots. 10 Although various feline spinal neoplasias have been reported, little research has examined the types of treatment for these tumours and the outcomes of felines who have been treated for them. Of the studies that described treatment of feline spinal tumours with definitive therapy,2,4,5,19 the survival duration reported after surgical treatment ranged between 88 and 518 days for osteosarcomas; 5 365 4 and 391 5 days for chondrosarcomas; 186 days for a chordoma; 5 a range of between 70 and 2190 days 4 and between 67 to 275 days for PNSTs; 5 106 days for a paragangliomas; 5 122 days for a lipoma; 5 and 7 months, 2 a range of 30 and 1400 days 4 and a range of 211 and 842 days 5 for meningiomas. Of the studies that described treatment of lymphosarcoma with other forms of therapy, the survival durations reported were a median of 14 weeks after chemotherapy (specifically, a median duration of complete remission), 19 of 38 days after irradiation and chemotherapy, 2 and a mean of 60 days 2 and 62 weeks 19 after surgery followed by chemotherapy. To the best of our knowledge, no study to date has investigated treatment of feline intramedullary tumours, which lie in the spinal cord parenchyma and require highly invasive surgery for removal. Here, we describe the successful treatment of one case of an apparent intramedullary mass in a feline subsequent to histopathological diagnosis as anaplastic astrocytoma.
A 10-year-old spayed female chinchilla feline presented at our clinic with a history of gradually progressive tetraparesis and discomfort upon touching that had begun 1 month before the onset of a 4-day tetraplegic episode. Neurological examination revealed non-ambulatory tetraparesis, absence of proprioception, normal-to-heightened spinal reflexes in all four limbs and hyperalgesia upon cervical manipulation. All other findings of the neurological examination were normal. The neuroanatomic localisation was suspected to be the C1–C5 spinal cord segments, and the differential diagnoses considered were intervertebral disc disease, meningoencephalitis, syringomyelia, spinal tumour and vertebral fracture/luxation. Routine laboratory testing revealed complete blood count and serum chemistry profiles within normal reference intervals, thoracic and abdominal radiography revealed no abnormalities, and the results of enzyme-linked immunosorbent assay testing for feline leukaemia virus-specific antigen and feline immunodeficiency virus-specific antibody were negative.
Using the 0.3 T Airis II Comfort MRI machine (Hitachi Medical Corporation), cervical magnetic resonance imaging (MRI) was performed to obtain T1-wieghted (T1W) sagittal and axial images; T2-weighted (T2W) sagittal and axial images; and contrast-enhanced T1W sagittal, axial and dorsal images using meglumine gadopentetate (Magnevist Bayer; 0.1 mmol/kg body weight). MRI revealed an elliptical intramedullary mass at the fourth cervical vertebrae, with T1W imaging revealing isointense-to-grey matter and T2W imaging revealing hyperintense-to-grey matter (Figure 1a, b). Subsequent contrast-enhanced T1W imaging revealed strong homogenous contrast enhancement of a relatively well-delineated mass that appeared to be surrounded by parenchyma on both T2W images and contrast-enhanced T1W images (Figure 1c–e). T2W imaging also revealed the presence of spinal oedema from the level of the second vertebrae to the mass (Figure 1a).

Midsagittal (a) and transverse (b) T2-weighted images. A large elliptical intramedullary mass at the fourth cervical vertebrae showing hyperintense-to-grey matter. Spinal oedema could be observed from the level of the second vertebrae to the mass. Midsagittal (c), dorsal (d) and transverse (e) contrast-enhanced T1-weighted imaging revealed a large elliptical intramedullary mass
Analysis of cerebrospinal fluid obtained via atlanto–occipital puncture revealed mild neutrophilic pleocytosis (6 nucleated cells/µl; normal level <5 cells/µl) and a normal protein level (15.9 mg/dl; normal level <40 mg/dl). Based on these findings, a tentative diagnosis of intramedullary tumour, suspected to be either glioma or ependymoma, was made. In accordance with this diagnosis, dorsal laminectomy of the C3–C6 vertebrae was performed, during which an area of grey discoloration remained visible through the dura at the level of the fourth vertebrae (Figure 2a). The dural membranes were incised at the midline, and the pial membrane was incised at the surface of the mass using a surgical knife. When the mass was dissected from the parenchyma, on the part of the mass exposed on the surface of the spinal cord, using a combination of gentle traction and blunt dissection, the border between the mass and spinal cord appeared clearly demarcated (Figure 2b). After the mass had been removed from the space of the mass exposed on the surface of the spinal cord to prevent incision of normal spinal tissue, the dura was closed with 5-0 nylon sutures. Contrast-enhanced T1W and T2W sagittal and axial imaging performed immediately postsurgery revealed an intramedullary lesion that was slightly hyperintense on T2W imaging and showed mild contrast enhancement on postcontrast T1W imaging at the original site of the mass, as well as complete excision of the mass that had been strongly enhanced on initial MRI (Figure 3).
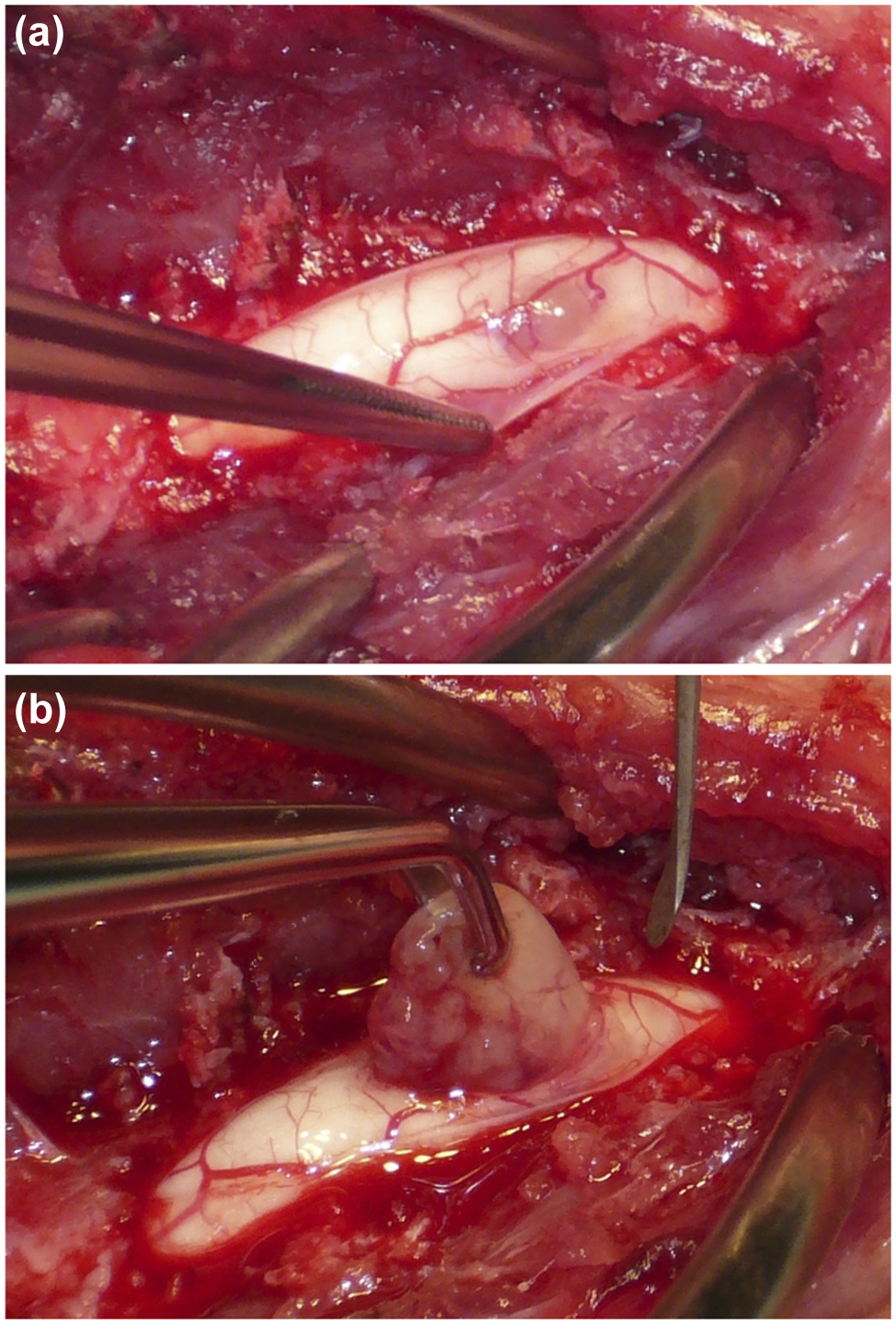
(a) An area of grey discoloration could be observed at the level of the fourth cervical vertebra, as well as pial vessels running along the surface of both the spinal cord and the mass. Based on these observations, the dural membranes were incised. (b) The mass was dissected from the parenchyma using a combination of gentle traction and blunt dissection

Midsagittal T2-weighted (T2W) image (a), and midsagittal (b) and transverse (c) contrast-enhanced T1-weighted images obtained immediately postsurgery revealed a lesion showing slight hyperintensity on T2W imaging and mild contrast enhancement in the spinal cord at the original site of the mass. The mass, which had been strongly enhanced on initial imaging, was shown to have been completely excised
Histological examination of the surgically removed tissue revealed the presence of haemorrhage, necrosis, vascular proliferation and strongly heteromorphic regions; a high frequency of mitotic figures and abnormal mitosis; and the arrangement of cells in pseudorosettes. The gemistocytic neoplastic population was characterised by pleomorphic, angular-to-polyhedral cells with distinct borders frequently containing an abundant, homogeneous-to-finely granular cytoplasm that extended frequently into variably sized fibrillar processes. The nuclei were large, oval-to-indented, and primarily eccentric, with hyperchromatic nucleoli and finely stippled chromatin. Rare binucleate cells could be observed at the periphery of the lesion (Figure 4). The neoplastic cells stained strongly positive for glial fibrillary acidic protein (GFAP; Figure 5), positive for nestin and negative for neurofilament. Based on these findings, the mass was diagnosed as anaplastic astrocytoma. 20
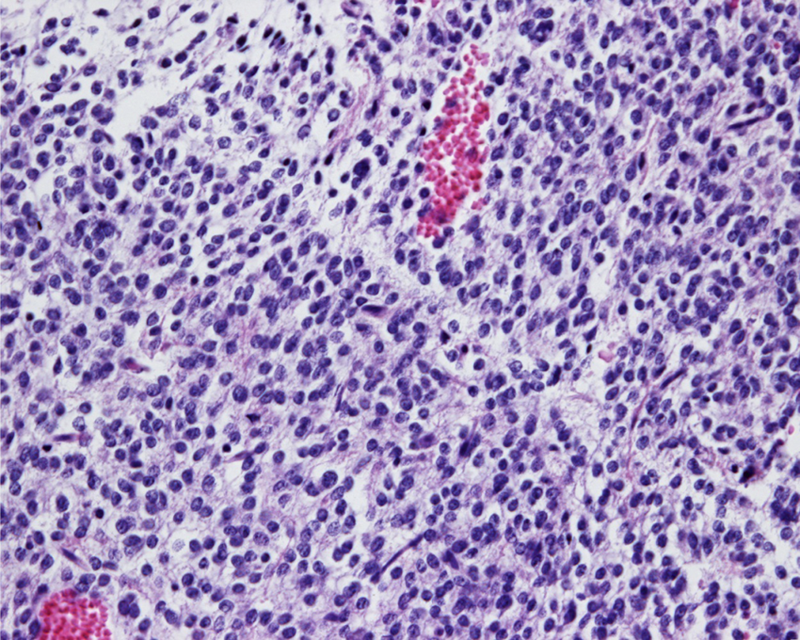
The gemistocytic neoplastic population was characterised by pleomorphic angular-to-polyhedral cells with distinct borders often characterised by an abundant, homogeneous-to-finely granular cytoplasm that extended frequently into variably sized fibrillar processes (haematoxylin and eosin staining, 400×)

After neoplastic cells had stained strongly positive for glial fibrillary acidic protein (GFAP) (GFAP staining, 400×), the mass was identified as an anaplastic astrocytoma
The feline was ambulatory 1 week postsurgery with only simple rehabilitation, and showed no neurological abnormalities 3 weeks postsurgery. Contrast-enhanced T1W sagittal and axial imaging, and T2W sagittal imaging performed 3.5 years postsurgery, when the feline required sedation for removal of tangled fur, revealed that the spinal cord was pulled dorsally owing to postoperative adhesion at the level of the fourth cervical vertebrae (Figure 6), but with the absence of abnormal signal lesions in the spinal cord. The feline remained ambulatory 3 years and 9 months after surgery, and showed neither neurological abnormality nor cervical hyperaesthesia.

Midsagittal T2-weighted (a), contrast-enhanced T1-weighted (T1W) (b) and transverse contrast-enhanced T1W (c) images obtained 3.5 years after surgery revealed the absence of high-signal intensity lesions in the spinal cord. The spinal cord could be observed to have been pulled dorsally owing to postoperative adhesion at the level of fourth cervical vertebrae (arrowhead)
Astrocytoma is rare in felines, accounting for only 2.8% of all feline intracranial neoplasms 21 and 3.5% of spinal cord neoplasms. 3 Among the different types of astrocytoma, anaplastic astrocytoma (medium-grade astrocytoma) is considered a comparatively malignant type classified generally between differentiated low-grade astrocytoma and glioblastoma multiforme (high-grade astrocytoma). 20 Prior research into feline intramedullary tumours, which is limited to three studies examining 10 cats in total,3,16,17 examined the treatment of four astrocytomas,3,16 one anaplastic astrocytoma, 17 two oligodendrogliomas 3 one ependymoma, 3 one anaplastic giant-cell tumour, 3 and one poorly differentiated glial tumour, 3 according to a non-specific treatment protocol because their prognosis were evaluated as poor. To the best of our knowledge, no study prior to the current study has investigated the outcomes of definitive therapy for treatment of feline spinal astrocytoma. There are only four prior studies that investigated five cases of canine spinal astrocytomas,22–25 even though dogs are the domestic animals most frequently affected by astrocytomas 26 and astrocytomas represent 17% of canine intracranial neoplasms. 27 None of the cases had been treated according to a specific protocol. In humans, most spinal astrocytomas are low grade (fibrillary astrocytomas), with anaplastic astrocytomas rarely and glioblastoma multiformes even more rarely observed.28,29 As human astrocytomas tend to infiltrate normal spinal parenchyma, surgical excision and postsurgical radiation are required for their treatment, even for those that are low grade and for which complete excision is difficult.28,29 The progression-free survival and survival rates after treatment for human astrocytoma at 5, 10 and 15 years have been reported as 42% and 59%, 29% and 53%, and 13% and 32%, respectively. 28
There have been several case reports30–33 and a small case series 34 on canine intramedullary tumours. Survival times for dogs with ependymoma receiving surgical and adjunctive radiation therapy have ranged from 3 to 70 months.30–32 Most cases of nephroblastomas are of extramedullary nephroblastoma, with only a small percentage of intramedullary nephroblastoma cases. 34 In a case study of intramedullary nephroblastoma, two surgical excisions were performed, but euthanasia was required 17 months after first excision owing to recurrence. 33 A case series of 10 cases of canine nephroblastoma reported a post-treatment survival duration for the four cases of intramedullary nephroblastoma ranging from 38 to 269 days (median, 140 days). 34 These findings suggest that some canine intramedullary tumours are operable and that surgical management can prolong survival. As the spinal parenchyma has no nociceptors, 1 intramedullary masses generally do not cause pain. The cervical pain experienced by the cat examined here had likely been due to stretching of the meninges by swelling of the spinal cord from extensive spinal oedema.
The temporary contrast enhancement observed on MRI obtained immediately postsurgery may have indicated the presence of a neoplastic lesion. Nevertheless, no enhancement was observed 3.5 years postsurgery. In one case of canine intramedullary haematoma, contrast enhancement consistent with scarring after surgical invasion was observed 15 days after resection. 35 This phenomenon, as well as the fact that leakage of medium into the resection cavity rather than pathological soft-tissue enhancement is typically the cause of contrast enhancement on T1W images obtained less than 24 h after surgery, 36 increases the difficulty of evaluating whether a mass has been excised completely by review of MRI performed soon after surgery. Indeed, the contrast enhancement observed immediately postsurgery in this case was suspected to have been caused by the leakage of the contrast medium.
Conclusions
The cat examined here recovered rapidly from tetraplegia and showed no signs of recurrence at 3 years and 9 month follow-up after removal of the malignant intramedullary tumour using the same surgical technique generally used for removal of human intramedullary tumours.28,29 Although surgical resection was performed macroscopically, microsurgery using a surgical microscope would have provided for greater precision. Specifically, using an ultrasonic aspirator28,29 or performing intraoperative somatosensory-evoked potential monitoring28,29,37 would have provided greater safety during the procedure and better outcomes. Based on analysis of the successful outcome obtained in the case examined here, we recommend that first-line treatment for canine and feline intramedullary tumours should be surgery, ideally microsurgery, followed by postoperative radiation therapy if indicated, as in the treatment of human intramedullary tumours.
Footnotes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this case report.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.