
Abstract
Practical relevance:
Mandibular fractures occur commonly in cats and appropriate treatment is vital to ensure restoration of dental occlusion and masticatory function.
Clinical challenges:
Historically, a relatively high complication rate has been reported in association with mandibular fracture repair, and these complications can represent a significant challenge for the veterinary surgeon.
Audience:
General practitioners as well as specialists in small animal surgery are presented with fractures of the mandible on a regular basis.
Patient group:
Cats of all ages can suffer mandibular fracture; however, young cats (mean age 30 months) are over-represented. No sex predilection is reported.
Equipment:
The nature of the equipment required for mandibular fracture repair varies greatly, depending on the fracture type and location. An uncomplicated mandibular symphyseal fracture requires only basic orthopaedic equipment whereas the surgeon must ensure they have access to a wide range of orthopaedic equipment prior to undertaking repair of a complex mandibular fracture.
Evidence base:
Management of mandibular fractures is a complex subject. Over the past three decades many fixation techniques have been described in the veterinary literature, with authors analysing and discussing the surgical management of these potentially challenging injuries.
Mandibular contribution to the feline fracture case load
Feline mandibular fractures are commonly seen in veterinary medicine, comprising approximately 16% of the fractures identified in cats. 1 The most common location for a mandibular fracture is the mandibular symphysis, followed by the mandibular body, and then the condyle and coronoid process. 2 The most frequent causes of mandibular fractures are road traffic accidents, fights and falls from a height. 3
Preoperative considerations
Concomitant injuries
The frequent causal relationship between major trauma and mandibular fracture necessitates that a thorough physical and neurological examination is performed in affected cases. Furthermore, a period of stabilisation and appropriate treatment is often required prior to consideration being given to fracture repair.
Thoracic injury is a common cause of death following a traumatic incident. In a study of 93 cats, Griffon et al found that 57% of cats with mandibular fractures suffered thoracic injury, most commonly lung contusions and pneumothorax. 4 When investigating cats with mandibular fractures, a minimum of two orthogonal radiographic projections of the thorax should be obtained. Some authors advise that an electrocardiogram should be obtained to investigate for evidence of traumatic myocarditis, 5 although it would appear appropriate to restrict use of electrocardiography to animals with clinically detectable cardiovascular output compromise.
Nutritional support
In cats with unstabilised, unmanaged mandibular fractures, calorific intake is likely to be reduced and reduced voluntary food intake may continue in the early postoperative period depending on the degree of trauma sustained, the severity of fracture and the chosen method of fracture fixation. Therefore, early intervention to ensure enteral nutrition, comprising either naso-oesophageal or oesophageal feeding tube placement, should be considered.

Determination of fracture configuration
Palpation under anaesthesia and radiological examination (including intra-oral views with oblique projections, as necessary) can aid the diagnosis and determination of the nature of the fracture. When making the radiological assessment, superimposition of structures can hamper the identification and understanding of fracture fragments and the fracture configuration, especially when examining the mandibular condyle and vertical ramus. Therefore, when an injury to these regions is suspected, computed tomographic (CT) examination, when available, should be considered.
Note that routine endotracheal intubation reduces the surgeon’s ability to assess dental occlusion for all but mandibular symphyseal separations, and therefore intubation via pharyngostomy has been recommended. In cats, tracheostomy in order to bypass the mouth is not recommended for inhalational anaesthesia because of the post-recovery risks in this species.
Antimicrobial prophylaxis
A high proportion of mandibular fractures are open and despite the relative resistance to infection of these injuries, prompt prophylactic broad spectrum bactericidal treatment is recommended due to the high number of bacteria within the oral cavity. 8
Placement of implants
The alveolar surface of the mandible is the tension surface of the bone and, therefore, under ideal (theoretical) circumstances, considering the biomechanics of the injury, fracture repair implants should be positioned here. In practice, the alveolar surface of the bone is not a suitable location for the placement of implants. Regardless of the location of implant placement, the tooth roots and the mandibular canal must be avoided. The mandibular artery is often damaged during the inciting injury that led to mandibular fracture and therefore the blood supply to fracture fragments rostral to the arterial disruption is reliant on collateral blood supply from surrounding soft tissues.
Dental occlusion
Once a mandibular fracture is identified it should be classified. Both fracture assessment score and fracture location govern the prognosis for successful fracture repair and influence the method of fracture fixation. 9 The goals of fracture fixation are to re-establish jaw function and dental occlusion, 10 and to achieve fracture healing in the process. During fracture fixation, the mouth should preferably be closed and the dental arcades closely inspected to ensure proper occlusion. 11 When assessing for occlusion, the mandibular canine teeth should lie between the maxillary canine teeth and the respective lateral incisors. In cats, as little as 2 mm of malalignment can prevent the jaw from fully closing. 12 In young animals with deciduous teeth, caution should be exercised when planning and performing fracture stabilisation due to the risk of damaging the developing teeth.
Mandibular symphysis fractures
Uncomplicated symphyseal fractures are best treated with cerclage wire (Figure 1). A small ventral midline skin incision is made just caudal to the symphysis, at the level of the caudal edge of the canine teeth. A large gauge hypodermic needle can then be passed through the midline incision and directed dorsally, running adjacent to the lateral aspect of the mandible so that it exits into the oral cavity through the gingiva just caudal and lateral to the canine tooth. A length of 1.0 mm orthopaedic wire is passed through the lumen of the needle, allowing one end of the wire to exit in the mouth. The needle is withdrawn ventrally over the wire and the needle is then reinserted in the same fashion adjacent to the contralateral mandible. The orthopaedic wire is directed from the oral cavity into the needle, with the end of the wire exiting ventrally through the hub of the needle. Once the needle is removed over the wire, the symphysis is encircled. The mandible is then aligned prior to the cerclage wire being tightened and secured with a twist knot. 13 Pointed reduction forceps placed across the mandible at the level of the canines can be helpful sometimes to maintain reduction during wire tightening. The skin should be closed over the wire twist.

Cerclage wire placement using a hypodermic needle to stabilise a simple mandibular symphyseal fracture
Clinical union of symphyseal fractures reportedly occurs on average in 6 weeks, 2 although, in the authors’ experience, stability sufficient to enable implant removal is often achieved after 3 weeks of fixation.
Mandibular body fractures
Numerous fixation methods are described for treatment of mandibular body fractures. Conservative methods include the BEARD (bignathic encircling and retaining device), 14 and the use of a muzzle. Surgical techniques include interdental wiring, interarcuate stabilisation, interfragmentary wiring, use of dental acrylic, external skeletal fixator (ESF) placement, internal fixation using plate and screws, intramedullary pin placement, modified interdental wiring and use of lingual arch bars. For some severe mandibular fractures, rather than attempting fracture fixation, rostral partial mandibulectomy can be considered as an alternative to restoration of mandibular integrity.
Interarcuate stabilisation
For many mandibular fractures, interarcuate stabilisation offers a preferable approach to fracture management compared with primary fixation. Methods of interarcuate stabilisation include maxillary–mandibular wiring, 15 use of dental acrylic 12 and maxillary–mandibular ESF placement secured rigidly or with elastic bands. 16
Maxillary–mandibular wiring
This technique has been described with successful outcomes. 15 A small hole is drilled through the maxilla caudal to the canine tooth roots. A hole in the same plane and at the same level as the maxillary hole is then drilled through both halves of the mandible, just caudal to the canines. Orthopaedic wire is passed through the holes and secured using a twist knot.
Dental acrylic
For stabilisation using dental acrylic, the canine teeth are pumiced or acid-etched, and then secured in alignment using the acrylic. One study by Bennett et al reported that this technique was successful in 11/11 cats treated. 12 An ultraviolet light-cured bonding agent must be applied to the surface of the teeth before the acrylic is applied, to prevent failure of adhesion of the acrylic to the teeth. Ultraviolet light-cured acrylic is significantly more effective than the non-light cured acrylics, the latter tending to readily debond from the teeth.
Transarticular ESF placement
The use of elastic bands to join the mandible to the maxilla rostrally allows limited and controlled jaw opening. Kirschner wires are placed laterolaterally caudal to the mandibular and maxillary canine tooth roots and the two wires are looped at each end prior to the application of small elastic bands (Figure 2). Tension in the elastic bands maintains the mouth closed and interarcade maxillary–mandibular dental occlusion by interlocking of the canine teeth should ensure fracture alignment. Although there may be some variation between individual cases, 3–4 weeks of interarcuate stabilisation is often sufficient. 15
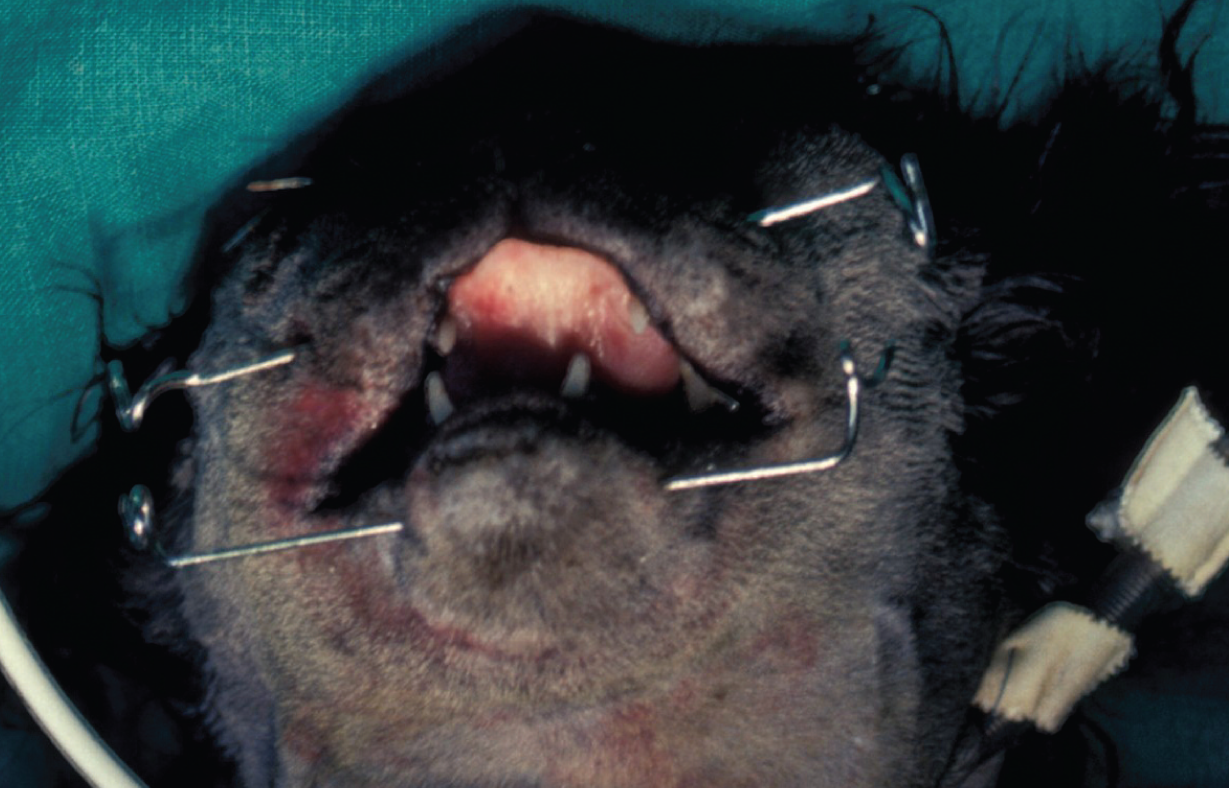
Maxillary and mandibular Kirschner wires in position prior to elastic band application
All three of these techniques benefit from ease of application and, in each case, cats can lick small amounts of liquid food. Nevertheless, use of a feeding tube to deliver enteral nutrition should be considered to fulfil nutritional requirements. In order to achieve a satisfactory outcome, these techniques, which rely on accurate restoration of dental occlusion through anatomic interlocking of the dental arcades, require at least partially intact canine teeth. When this condition is not met, stabilisation can still be attempted using dental acrylic if a canine tooth is damaged because the pulp can be capped.
Due to the risk of aspiration pneumonia, interarcuate stabilisation is contraindicated in patients at significant risk of regurgitating or vomiting. 16 Furthermore, continued vigilance is required during the postoperative period because of this ongoing risk.
Primary fixation
Interfragmentary wiring
Interfragmentary wires can be used to repair selected mandibular body fractures. Careful consideration of the suitability of this fixation modality must be given prior to use. Ideally suited fractures are simple, unilateral, oblique, and stable in reduction with a fracture alignment that results in fracture compression during mouth closure. 3 Interfragmentary wiring is contraindicated in cats with bilateral mandibular body fractures. In addition, most comminuted fractures do not lend themselves to this repair technique.
Holes are drilled in each fragment in an oblique direction aimed towards the fracture, perpendicular to the fracture line. This configuration facilitates wire tightening and limits shearing as the wires are tightened. 16 The most stable position for wire placement is the alveolar border. The wire should be placed in an appropriate fashion to ensure interfragmentary stability without sacrificing fracture biology as a result of surgical elevation of soft tissue attachments to the fracture fragments.
External fixation
ESF placement (Figures 3–6) provides a simple and effective method of fracture repair. Numerous methods of applying external fixators to mandibular fractures exist, with multiple frame configurations reported. 17 Techniques and frame types include unilateral (rostral pins crossing the symphysis), bilateral, bilateral with bumper bar, and bilateral with interfragmentary implants. ESF pins are placed in the aboral surface of the mandible, directed into the ventral mandible, aiming to avoid the mandibular canal. The use of epoxy resin and acrylic connecting bars allows greater variation in pin placement.

Placement of the first interarcade dental acrylic column

Subsequent curing of the acrylic with ultraviolet light

Two columns of interarcade acrylic following ultraviolet light curing

Cat with a mandibular bilateral bumper bar acrylic ESF
The most common indications for ESF use include comminuted fractures and fractures in which soft tissue wounds prevent the use of internal fixation. 13 One study of eight fractures in cats repaired using external fixation reported an average time to fracture union of 5.5 weeks. 17 The authors also noted that management of mandibular fractures using an ESF resulted in a beneficial early return to voluntary prehension of food and normal eating. Pin loosening occurred commonly, but this was not clinically significant and the overall outcome reported in the study was good. 17
Rostral mandibular fractures can also be successfully managed with a lingual arch bar made from orthodontic wire and applied to the lingual alveolar margin. In a study of 16 cats, 11 were able to eat within 24 h following this procedure. In 5/16 cats, fracture non-union occurred and, in one case, corrective surgery was required. 18

Application of mini-plate and screws
Internal fixation of mandibular fractures using plates and screws is limited by the anatomy of the region. Titanium mini-plate fixation systems, which offer a greater ease of screw placement, have been used to treat mandibular body fractures. 19 Plates are applied to the tension aspect of the mandible, with the screws placed between the tooth roots or into the ventral mandible, avoiding the mandibular canal. In one study reporting the use of mini-titanium plate fixation systems for mandibular fracture repair in three cats, healing time ranged from 6–9 weeks. The implants necessitated removal in two of the three cats treated (after 3.5 months in one case and after 18 months in the other), following documented fracture healing. 19
Mandibulectomy
A mandibulectomy is indicated for the treatment of some severe mandibular fractures in which fracture stabilisation is not possible, as well as when fracture healing is considered extremely unlikely and in certain cases of fracture(s) that have failed to heal following attempted repair. The area of mandible excised is determined by the fracture location. Rostral (hemi)mandibulectomy, central and caudal hemimandibulectomy, total hemimandibulectomy and three-quarter mandibulectomy have variously been described. Consideration should, however, be given to potential postoperative complications prior to performing a mandibulectomy in a cat. In one study of 42 cats that underwent mandibulectomy to treat oral tumours, 12% of cats did not regain the ability to eat postoperatively and 76% of cats had long-term morbidity. 20
When a mandibulectomy is performed, a feeding tube should be placed to allow early enteral nutrition as there is often a significant postoperative delay before the patient will eat voluntarily.
Caudal mandibular fractures
Primary fixation is more technically demanding for caudal mandibular fractures than for rostral fractures. The anatomy of this region makes surgical exposure of the fracture challenging and there is reduced bone stock, which reduces the potential for placement of implants with mechanical security or bone–implant interface longevity. Conservative treatment should be considered for such cases if dental occlusion can be maintained. Surgical techniques for primary fixation include interfragmentary wiring with placement of orthopaedic wire using a ventral approach. Interarcuate stabilisation can also be effective for many fractures in this region.
Temporomandibular joint luxations
Fracture luxations of the temporomandibular joint (TMJ) can be unilateral or bilateral, with the unilateral presentation predominating. Luxations normally occur rostrally. Caudal luxations occasionally occur in association with fracture of the retroarticular process.
For simple luxations, closed reduction should be attempted initially, using a caudally placed intra-oral rod (ideally a wooden dowel or a pencil). The rod is placed laterolaterally between the caudal molars of both mandibles/maxillae. The mouth is forcibly closed with digital pressure exerted rostrally over the mandible and over the nasal planum. Leverage over the rod, which acts as a fulcrum, distracts the TMJ and release of the leverage allows the joint to reduce through tension in the soft tissues surrounding the TMJ.
Very rarely, closed reduction is not successful and, under these circumstances, an open reduction via a lateral approach may be indicated.

Caudal TMJ luxations are often unstable after closed reduction and these injuries may require additional stabilisation via interarcuate stabilisation using dental acrylic or a maxillary–mandibular ESF. 7
Footnotes
Key Points
Case notes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this article.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.