
Abstract
Xanthine urolithiasis was diagnosed in a 10-month-old intact female domestic shorthair cat presented with acute renal failure due to bilateral ureteral obstruction. Ultrasonography revealed the presence of multiple uroliths in both kidneys and ureters that were not detectable on previous survey radiographs. Medical management failed and ureteral obstruction persisted with no evidence of stone migration into the bladder. Bilateral ureterotomy with urolith removal was performed in order to relieve the obstruction. The cat recovered from surgery, and blood urea nitrogen and creatinine values decreased within normal limits 6 days postoperatively. Urolith analysis by infrared spectrometry determined xanthine composition, and a higher blood and urine concentration of hypoxanthine and xanthine was also found. At 1-year follow-up, the cat was free of clinical signs. However, ultrasonography of the abdomen revealed small-size calculi in both kidneys, despite the low protein diet intake. The very young age of the animal suggests a possible congenital xanthinuria.
Case Report
Naturally occurring xanthine urolithiasis has been reported rarely in cats.1–3 This case report describes bilateral ureteral obstruction caused by multiple xanthine ureteroliths in a young cat presented with acute renal failure.
A 10-month-old intact female domestic shorthair cat was referred owing to sudden onset of asthenia, anorexia, emesis and anuria of 2 days’ duration. On physical examination the cat was depressed with signs of 6–8% dehydration. Mild abdominal pain was present and emesis was stimulated on palpation. Bilateral kidney enlargement was identified on abdominal palpation and the urinary bladder was empty.
Complete blood count was within normal limits and clinical chemistry profile revealed increased values of blood urea nitrogen (BUN) [674 mg/dl, reference interval (RI) 30–65 mg/dl], creatinine (20.04 mg/dl, RI: 0.6–1.6 mg/dl) and potassium (6.3 mmol/l, RI: 3.5–5.2 mmol/l). Fluid therapy was initiated [sodium chloride (NaCl) 0.9% at a rate of 50 ml/kg/h] and a transurethral catheter was used for the measurement of urine production. Radiographs of the abdomen showed bilateral kidney enlargement (the right kidney was 5.5 × 3.23 cm and the left kidney was 5.4 × 3.16 cm) and an empty bladder (Figure 1). After 4 h of fluid administration, it the absence of urine production was noted and signs of hyper-hydration emerged, including interstitial pulmonary oedema and chemosis, while electrolyte analysis revealed hyponatraemia (124 mmol/l, RI: 147–156 mmol/l). Ultrasonography of the abdomen revealed the presence of multiple nephroliths and ureteroliths associated with signs of bilateral distal ureteral obstruction, including bilateral pelvis dilation and hydroureter (right pelvis 1.8 × 2.53 cm and ureter 0.50 cm; left pelvis 1.17 × 1.38 cm and ureter 0.36 cm) (Figure 2). Electrolytes and blood gas analysis revealed hyperkalaemia (>9 mmol/l, RI: 3.5–5.2 mmol/l) and metabolic acidosis (pH 6.9). Additional therapy for hyperkalaemia was instituted with the administration of glucose at a dosage of 0.5 g/kg and rapid insulin (Actrapid; Penfill) at a dosage of 0.5 UI/kg intramuscularly (IM), every 30 mins for five administrations, coupled to glucose measurements. Despite the medical management, the clinical condition of the cat deteriorated rapidly and emergency surgery was suggested to the owners. Even though the animal was considered an ASA V anaesthetic risk, the owners consented to surgery. The cat was sedated with IM administration of morphine at a dosage of 0.5 mg/kg (Morfina 1%; BBraun) and an epidural administration of 0.8 ml of 2% lidocaine was performed at the dorsal epidural lumbosacral intervertebral space to provide anaesthesia and analgesia.

Ventro-dorsal abdominal X-ray showing bilateral kidney enlargement; nephroliths are radiolucent
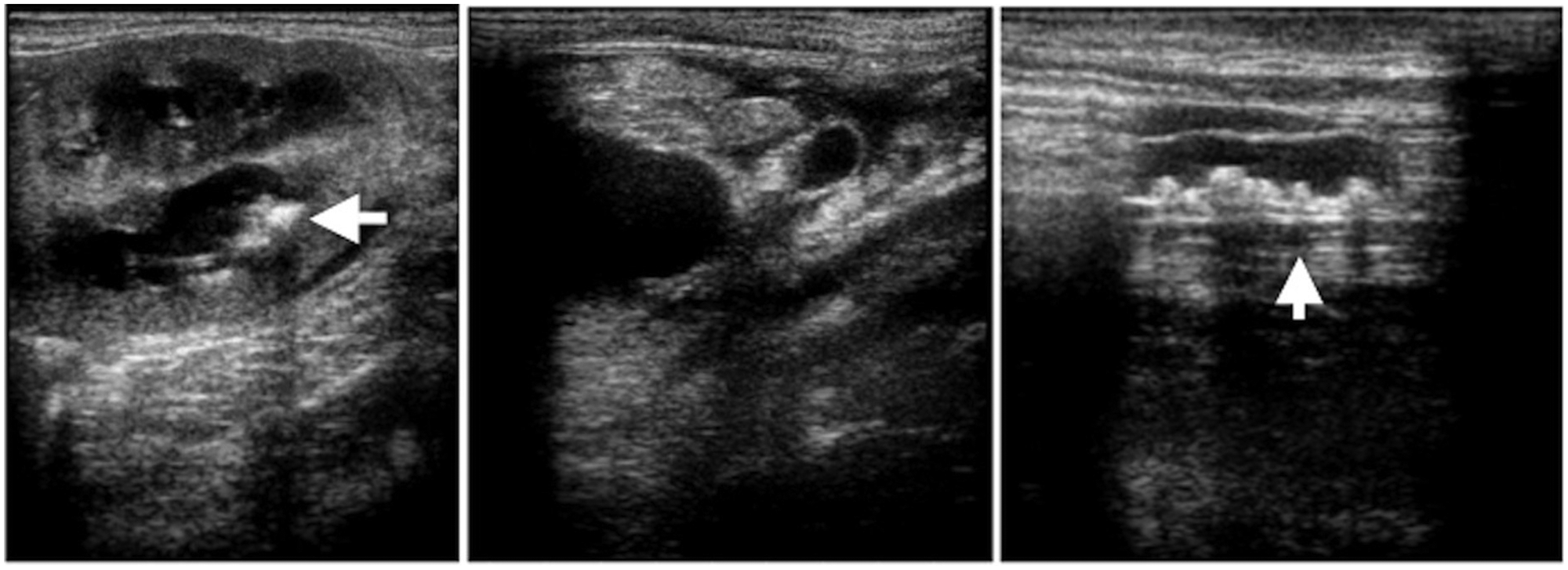
Abdominal ultrasonography showing signs of bilateral ureteral obstruction with multiple ureteroliths. Uroliths are also identified in the pelvis in both kidneys
A ventral midline laparotomy was performed. Bilateral kidney enlargement was obvious and dilation of both ureters was easily identified owing to bilateral distal ureterolith obstruction at the level of the bladder trigone. Bilateral distal ureterotomy was performed and all uroliths were removed (Figure 3a, b). A urine sample was collected from both ureters for bacteriological analysis. Bilateral ureteral catheterisation and lavage was performed before ureteral closure to ensure that no stone was remaining. Ureterotomy closure was performed with a simple continuous suture using 7/0 monofilament polyglyconate. A ventral cystotomy was performed to assure that no ureteral obstruction was still persisting. This was confirmed by direct observation of immediate urine production at the level of the bladder trigone. The linea alba, subcutaneous tissues and skin were closed in a routine manner.

(a) Ureter and bladder secured with stay sutures and removal of uroliths. (b) Uroliths recovered
Postoperatively, urine production was monitored through the transurethral catheter. Glycaemia and kalaemia were monitored every 1 h and every 4 h, respectively, for 12 h. The animal received fluid therapy with NaCl 0.9% at a rate of 45 ml/kg/h, ranitidine (Ranitidine; Labesfal) at a dosage of 0.5 mg/kg IM and ceftriaxone at a dosage of 15 mg/kg intravenously (Ceftriaxona; Labesfal) q12h. The cat regained consciousness 24 h after surgery. Potassium values were within normal limits (5.0 mmol/l, RI: 3.5–5.2 mmol/l), and BUN and creatinine values were decreasing (BUN 130 mg/dl, RI: 30–65 mg/dl; creatinine 12.6 mg/dl, RI: 0.6–1.6 mg/dl). Ultrasonography of the abdomen was performed 48 h and 72 h after surgery. At 48 h, there was no evidence of any remaining uroliths, but renal subcapsular fluid, and right pelvic and ureter dilation (0.4 cm) were still present (Figure 4). At 72 h, right pelvic and ureter dilation were improving, whereas some subcapsular fluid was still present. The size of left kidney and ureter was normal (Figure 5).

Ultrasonography 48 h postoperatively. There is evidence of right subcapsular fluid and dilated pelvis. Right ureter diameter is 0.4 cm and left ureter is of normal diameter

Ultrasonography 72 h postoperatively. There is still evidence of right subcapsular fluid. Right ureter diameter is 0.4 cm
The animal was discharged 4 days after surgery. Oral cephalexin (Rilexine; Virbac) was prescribed at a dosage of 10 mg/kg q12h, while waiting for the urine culture results. Uroliths were submitted for microbiological culture and quantitative mineral analysis by infrared spectrometry. Results revealed xanthine urolith composition and no bacteria were isolated.
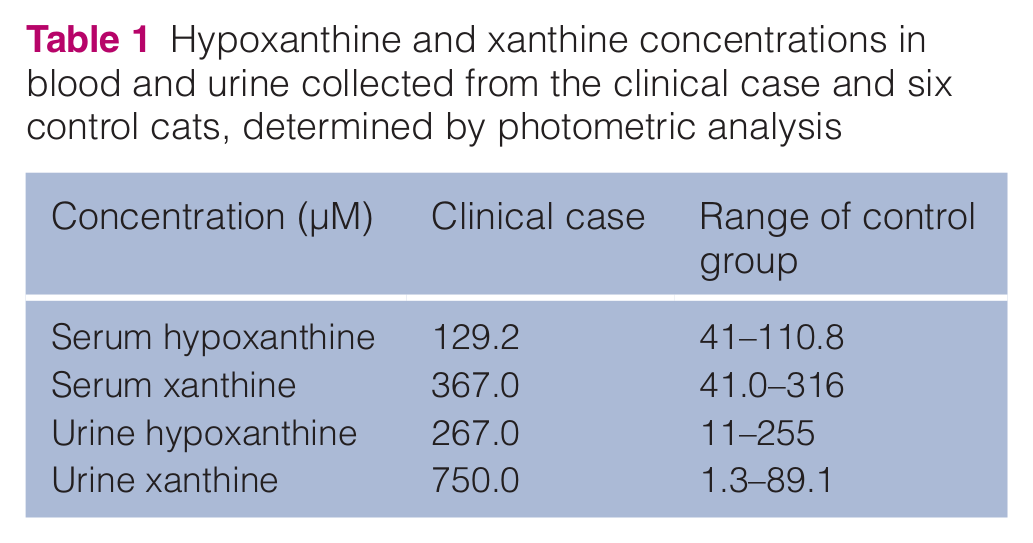
In cats, the normal values of hypoxanthine and xanthine concentrations in blood and urine are unknown. In order to establish approximate normal range values, these concentrations were measured in the cat in this report and in six unrelated healthy control cats using the photometric analysis established for humans (Stat Fax, kit A22182 – Amplex Red Xanthine/Xanthine Oxidase Assay Kit; Molecular Probes, Invitrogen Detection Technologies). Control cats were chosen based on their healthy status, young age (between 1 and 2 years old) and the absence of crystalluria confirmed by urinalysis. Healthy status was determined by haematology, clinical chemistry and urine analysis. For hypoxanthine and xanthine analysis, the serum samples were prepared immediately after blood collection and the urine samples collected by cystocentesis were stored at −20ºC for 4 weeks. Both hypoxanthine and xanthine concentrations were increased in animal’s blood and urine when compared with the results obtained in the control group (Table 1).
Hypoxanthine and xanthine concentrations in blood and urine collected from the clinical case and six control cats, determined by photometric analysis
At 1 month postoperatively, ultrasonography of the abdomen showed both kidneys and ureters to be in the normal size range (right pelvis 2.2 mm, left pelvis 2.4 mm and both ureters <1 mm diameter). The analysis of urine collected by cystocentesis revealed a specific gravity of 1.020, and crystalluria was not detected. A life-long low protein diet along with increased water intake and an ultrasound recheck every 3 months were recommended. At the 1-year recheck, urinalysis results revealed crystalluria. Ultrasonography of the abdomen revealed the presence of one small-size calculus in the left kidney and two calculi in the right kidney (Figure 6). The cat was asymptomatic, and BUN and creatinine values were within normal limits.

Ultrasonography 1 year after surgery; one small calculus on the left kidney and two on the right were identified
Discussion
The description of emergency anaesthetic and surgical management of a young patient cat with an acute renal failure due to bilateral ureteral obstruction is scarce in veterinary literature. The diagnosis of ureteral obstruction seems to be increasing.4,5 Ultrasonography, combined with radiography is able to diagnose 90% of ureteral calculi. 4 In the present case, though radiography could only identify renomegaly, ultrasound detected the presence of bilateral ureteral lithiasis, with numerous calculi in both ureters, hydroureter and hydronephrosis, as well as the precise location of the obstruction. Therefore, both imaging modalities are warranted in order to identify radiolucent uroliths, such as xanthine uroliths.
Surgical removal of ureteroliths is indicated when there is evidence of ureteral obstruction and no evidence of progressive migration into the bladder. If medical management fails or the patient is unstable (eg, hyperkalaemic, overhydrated or oliguric), immediate intervention should be considered. Possible procedures include ureterotomy, ureteral re-implantation, ureteral stenting, nephrostomy tube placement or haemodialysis. 6 In the present case, a bilateral ureterotomy was performed 24 h after initiation of medical treatment because the clinical status of the cat was deteriorating. In order to minimise anaesthetic risks, local epidural anaesthesia was chosen as the haemodynamic and cardiac effects of this anaesthetic modality are minimal. Furthermore, the animal was in a stupor and any further hypotension could have lead to complete and irreversible renal failure and cardiovascular collapse. Relief of the obstruction allowed immediate improvement of azotaemia and electrolyte status, along with prevention of further kidney damage.
In cats, maximum time between ureter occlusion and complete kidney recovery after relief of obstruction is not yet determined. The decision on whether or not to perform surgery depends on the time elapsed since diagnosis, the results of the medical treatment and the presence of signs of calculus migration. In cats with ureteral calculi, the reported survival rate at 12 months is 66% in patients receiving medical treatment and 91% in patients receiving surgical treatment. 5
Up to 70% of nephroliths in cats are composed of calcium oxalate, usually found in both kidneys and/or ureters. 7 In the present case, bilateral ureteral obstruction was caused by xanthine uroliths, which have been reported in only three cases.1–3 The described cases of xanthine calculi in cats were related to bladder stones, and none of them presented nephroliths and acute renal failure due to ureteral obstruction. Only one cat was 10 months old and its signs were not as severe as in the present case; the other two reported cases occurred in older cats.
Hypoxanthine and xanthine are products of purine metabolism converted by xanthine dehydrogenase (XDH) into uric acid, which is converted by the hepatic uricase in allantoin, the end-product of purine degradation.8,9 A XDH deficiency results in accumulation and excessive renal excretion of hypoxanthine and xanthine. Despite the high solubility of hypoxanthine, xanthine has low urine solubility, and xanthinuria may trigger xanthine urolithiasis. 10
Information about normal xanthine and hypoxanthine serum, and urine values in cats is scarce and limited to the two previous case reports.2,3 In order to identify a possible purine metabolism disorder, control values were obtained from six healthy control cats. Interestingly, the range of values obtained from the control group was higher than the reference interval values described previously. This difference may indicate a great variability in the reported values or a difference in the laboratory technique used. Indeed, the values of these parameters may depend on the timing and method of sampling, as well as on the dietary composition. In the present report, the samples were not collected during a fasting period.
The diseased cat had slightly elevated blood concentrations and markedly elevated urine concentrations of both hypoxanthine and xanthine when compared with values obtained in the control cats. A prolonged storage time of samples can lead to a decrease in xanthine concentrations 11 ; however, a markedly elevated concentration could still be measured. It appears that high urine concentrations of hypoxanthine and xanthine, as described in this report, suggests that the use of a single spot urine sample could be a useful diagnostic tool in cases of feline xanthinuria. However, it must be emphasised that the results of this technique are greatly dependent on the timing of sample collection. Other analysis, such as xanthine:creatinine ratio, could add more information
Dissolution protocols for xanthine uroliths have not yet been developed. Surgical removal of uroliths is still a reliable method. In the present case, the location of the uroliths in both distal ureters, along with complete bilateral occlusion, lead to decision for surgery as the only treatment option. 12 Prevention of recurrence involves low purine intake, high water intake and urine alkalinisation in order to reduce urine xanthine concentration and to increase its solubility. In this case, prevention measures included a low protein diet (Hill’s k/d ) as moist renal diets are currently recommended. 12 Ultrasonography of the abdomen was performed every 3–6 months, and, at 1-year follow-up, new calculi were detected in both kidneys, although they were still very small and not associated with any signs. In light of the scarce treatment options, the animal is kept under surveillance in order to detect any signs of developing acute or chronic kidney failure indicating recurrence of ureteral sub-obstruction or obstruction. In such case, ureteral stenting could potentially be an alternative option to surgical removal.
Xanthine urolithiasis has been reported previously in cats.1–3 In two cases, hypoxanthine and xanthine values were determined and compared with values in control cats.2,3 Only one case occurred in a young cat (aged 10 months), but clinical signs were related to the presence of bladder stones and urethral obstruction. 3 The present case also occurred at a very young age but the clinical presentation was much more severe as it was related to bilateral ureteral obstruction and acute renal failure. Differences in clinical presentation could also be due to the fact that our patient was a female cat, as opposed to previously described male cats, as she could have at first eliminated small bladder uroliths during micturition.
Conclusions
In this case report, high urinary excretions of hypoxanthine and xanthine, the patient’s young age and the absence of allopurinol administration raise the hypothesis of a possible congenital xanthinuria and a congenital defect of XDH. In two previous cases, congenital xanthine urolithiasis was suggested, but the hereditary hypothesis was not proven.2,3
Footnotes
Acknowledgements
The authors acknowledge Dr Katia Viana for her contribution in long term follow up of the animal.
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this case report.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.