
Abstract
Vomiting is a common presenting complaint in feline practice. This article differs from previous reviews in that it is an evidence-based review of the mechanisms, causes, investigation and management of vomiting in the domestic cat. Published evidence was reviewed, and then used to make recommendations for clinical assessment, diagnosis, antiemetic drug treatment, dietary management and monitoring of cats presenting with vomiting. The strength of the evidence on which recommendations are made (and areas where evidence is lacking for cats) has been highlighted throughout.
Introduction
Vomiting is a common presenting complaint in feline practice and occurs in an enormous range of disease processes. It is amongst the most common clinical signs reported in cats examined at private veterinary practices. 1 The aim of this study was to perform an evidence-based review of the mechanisms, causes, investigation and management of vomiting in the domestic cat. In each area recommendations have been made, and the strength of the published literature, upon which the recommendations were based, has been presented.
Methods
A systematic literature search was performed in PubMed using the search terms [(‘vomit*’ OR ‘emesis’) AND (‘cat’ OR ‘feline’)] and [‘antiemetic*’ AND (‘cat’ OR ‘feline’)]. All articles relevant to domestic cats were collected, ignoring those dealing solely with captive large felids. Only articles relevant to actual vomiting (defined for these purposes as the forceful ejection of stomach contents via the mouth) were considered; any articles that dealt solely with nausea were not included. Similar searches were made in the Centre for Agricultural Bioscience International database (CAB direct), Google Scholar and Web of Science, identifying additional references not listed in PubMed. To indicate the strength of available evidence in support of the statements and recommendations made, references were assigned a level of evidence (LOE), and an overall evidence grade (OEG) for each aspect was also assigned (Table 1), as described previously. 2

The all or none principle is met when all patients died before the treatment became available, but some now survive on it; or when some patients died before the treatment became available, but none now die on it
The emetic reflex and causes of vomiting
Vomiting in cats is a complex reflex involving the gastrointestinal system, respiratory and abdominal muscles, and changes in posture [2b3–6]. Some of these coordinated reflex events are a reduction in gastric motility, retrograde movement of gut contents from the proximal intestine to the stomach, and relaxation of the gastro-oesophageal junction followed by expulsion of gastric contents brought about by forceful contractions of the diaphragm and abdominal muscles, and closure of the glottis [2b3,5–13] [OEG B].
Vomiting may be triggered by peripheral stimuli, such as afferent neural input from the gastrointestinal tract or other visceral organs, or central stimuli, such as circulating toxins that activate the central nervous system (CNS) via the area postrema (AP) [2b8,13,14]. The AP is a bilateral structure adjacent to the fourth ventricle, considered to be outside the CNS because it lacks a blood–brain barrier [2b 15 ]. It is a chemoreceptive area that triggers vomiting, and its ablation abolishes the emetic response to most (but not all) emetogens [2b16–19]. Vestibular stimuli (motion sickness) can also cause vomiting in cats, although susceptibility varies between individuals [2b20,21]. The AP is not involved in motion sickness [2b22,23]. As in other species, input from midbrain or forebrain structures also may trigger vomiting [2b6,13] [OEG B].
Regardless of how it is triggered, the motor act of vomiting is coordinated at the level of the brainstem by the same set of structures [2b 6 ]. In cats, vomiting is coordinated by a distributed control system, not a discrete vomiting centre: neurons activated during vomiting are distributed in the brainstem in an area extending from the AP and dorsal motor nucleus of the vagus through the nucleus of the solitary tract (NTS) and lateral tegmental field of the reticular formation to the region of the retrofacial nucleus in the ventrolateral medulla [2b18,19,24]. This area also contains neurons controlling related functions, such as respiration, cranial nerve integration, swallowing and salivation [2b 19 ]. The NTS is thought to be the beginning of a final common pathway by which different triggers produce vomiting, and receives inputs from sources that can trigger vomiting, such as the vagus nerve, the AP, and vestibular and limbic systems [2b6,18,23,25–27] [OEG B].
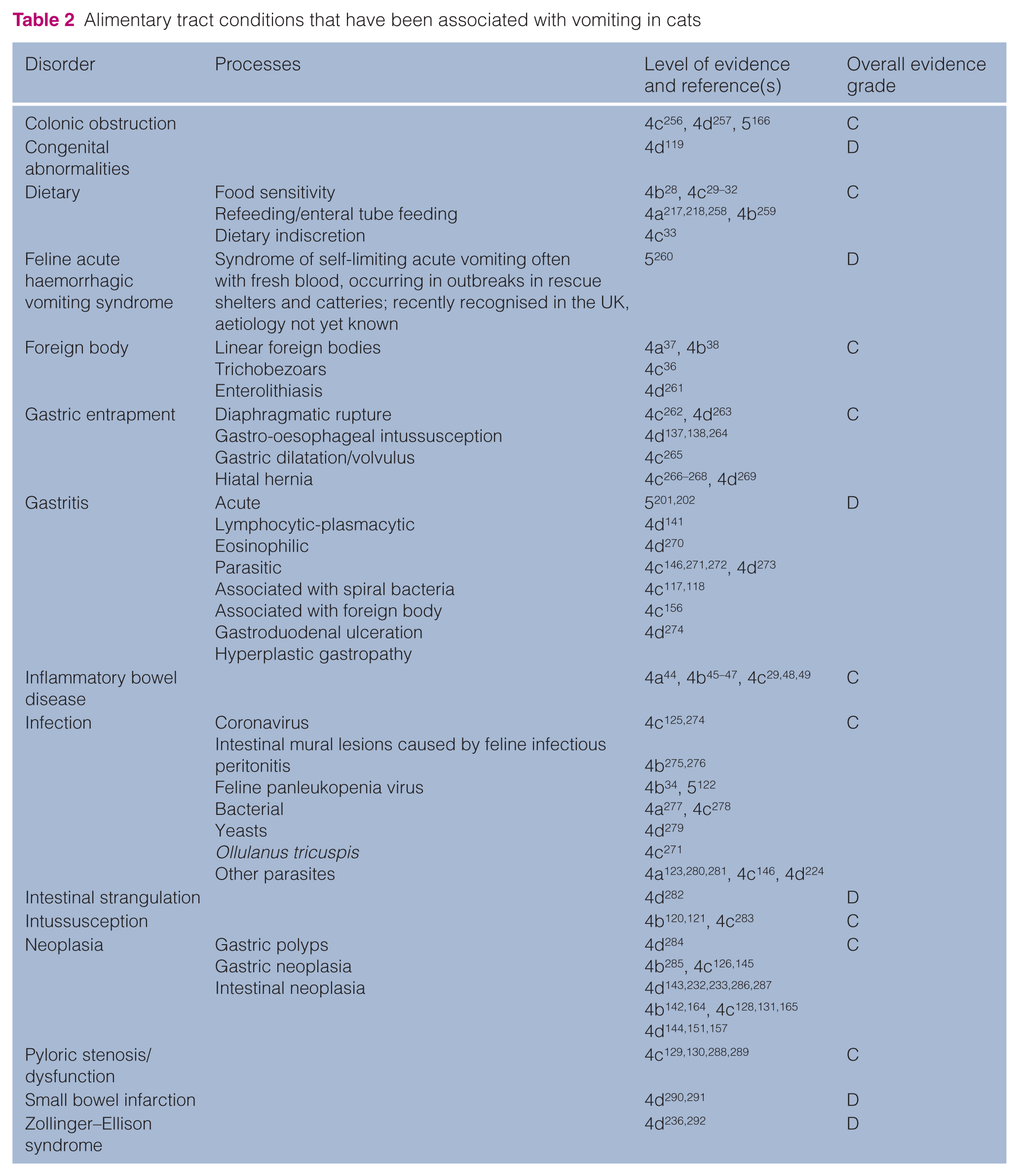
The conditions that have been reported to be associated with vomiting in cats are listed in Tables 2–4, mostly at LOE grade 4 or 5. Based upon these reports, the most common causes include adverse reactions to food [4b 28 , 4c29–33], infectious agents (such as feline panleukopenia virus [4b 34 ] and feline infectious peritonitis virus [4c 35 ]), and acute self-limiting emesis of undetermined cause (so-called ‘acute gastritis’)[5]. Compared with other veterinary species, cats frequently vomit trichobezoars (hairballs) [4c 36 ], probably because of their fastidious grooming behaviour. They do not commonly ingest foreign bodies, but when they do, linear foreign bodies (string, sewing thread) are often reported [4a 37 , 4b 38 ]. Furthermore, cats frequently vomit after administration of α2 adrenergic drugs [2b21,39–42, 4a 43 ], reflecting the importance of these receptors in the brainstem areas controlling vomiting. The most common causes of chronic vomiting in cats seem to be idiopathic inflammatory gastritis or enteritis (‘inflammatory bowel disease’) [4a 44 , 4b45–47, 4c29,48,49], adverse reactions to food [4b 28 , 4c29–32], liver disease [2b 50 , 4a51,52, 4b53–55, 4c56–62, 4d56,58,63–70] and uraemia [2b 71 , 4a72,73, 4b74,75, 4c 76 , 4d77,78]. Hyperthyroidism is common in cats and is also associated with vomiting [4a79,80] [OEG D].
Alimentary tract conditions that have been associated with vomiting in cats
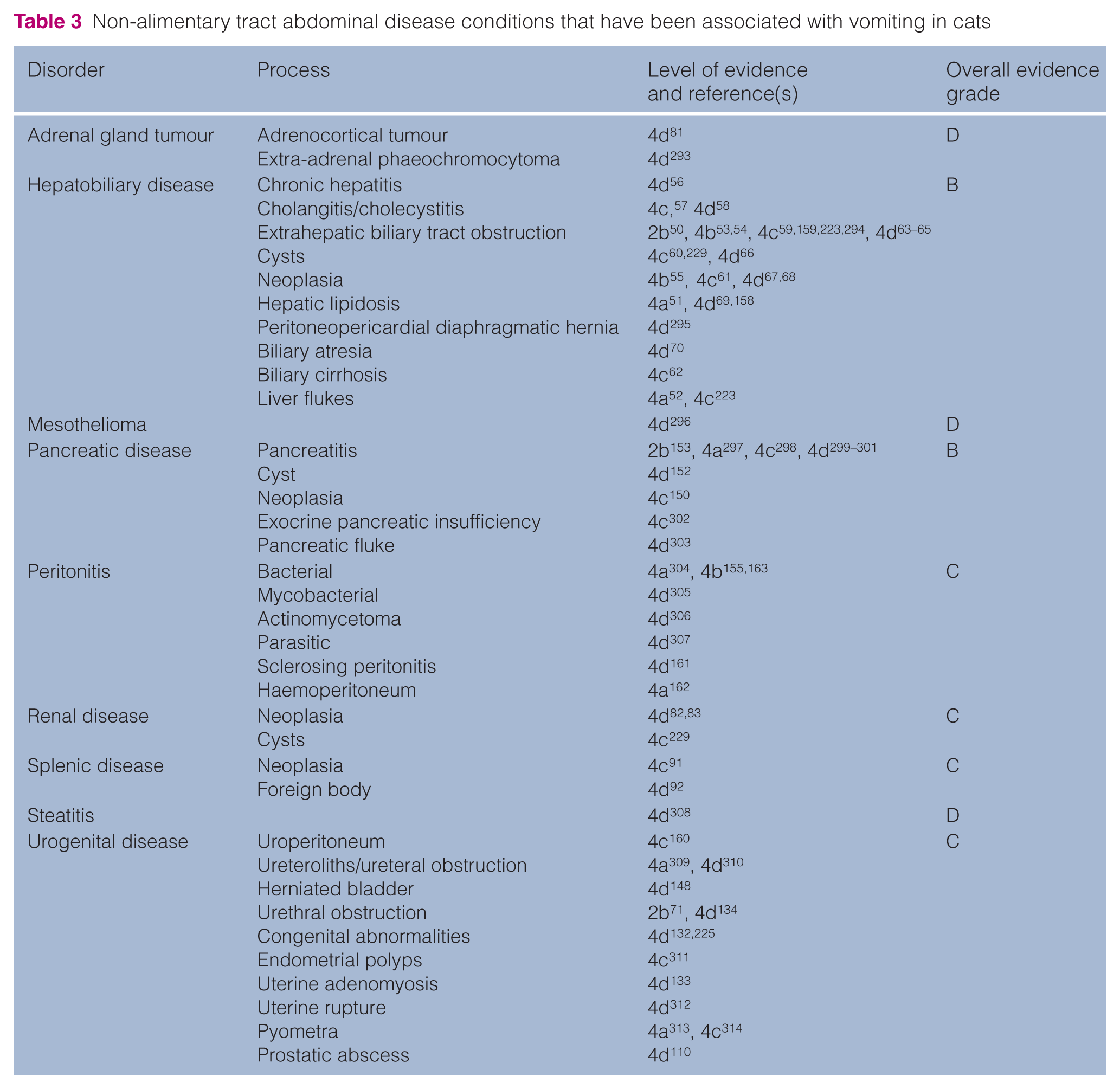
Non-alimentary tract abdominal disease conditions that have been associated with vomiting in cats
Systemic and other disease conditions that have been associated with vomiting in cats

NSAIDs = non-steroidal anti-inflammatory drugs; FeLV = feline leukaemia virus; FIV = feline immunodeficiency virus; FIP = feline infectious peritonitis
Although most causes of vomiting are likely to be the result of the diseases listed above, clinicians should be aware of the many other conditions where vomiting has also been reported (Tables 2–4). Most notably, vomiting has been associated with many non-alimentary diseases, either involving other abdominal organs (Table 3) or other systemic conditions (Table 4), including various types of neoplasia [4c 87 , 4d81–90], splenic disease [4d91,92], many infectious disorders [3b 104 , 4a 96 , 4b 93 , 106 , 4c 35 ,94,105, 4d 95 ], prostatic abscessation [4d 110 ], chronic nasal disease [4a 111 ], pyothorax [4b 112 ], aortic thromboembolism [4b 113 , 4c 114 ] and bronchial disease [4a115,116]. While these tables can serve as a broad indication of possible differential diagnoses, associations should be made cautiously. In this respect, most of these reports are from isolated case series or single case reports and, as a result, it is impossible to determine the relative importance of these disease associations. Furthermore, the reason for the vomiting is often not explored in detail and may, in fact, have been incidental to the case. For example, two reported infectious causes of vomiting are gastric spiral organisms117,118 and Ollulanus tricuspis, 271 although the evidence in support of a causal link is weak. Indeed, in one of the articles regarding gastric spiral organisms, the authors highlight the fact that other reasons for vomiting were not adequately excluded. 117 Furthermore, in the single article reporting an association between O tricuspis infection and vomiting [OEG 4c 271 ], only two of the four cats vomited, and both of these cats responded to dietary manipulation.
Clinical presentation and initial assessment
During the initial assessment of cats with vomiting, the severity of the disease process should be determined, with the aim of differentiating those cats that need limited further examination and can be treated symptomatically from those that need extensive investigations or therapy. Although not its primary purpose, the initial assessment may also give a clear indication as to the underlying cause of the vomiting [OEG D].
Assessment starts with the age, breed and gender of the cat, along with presence of signs in other cats in the household. Age is important because some diseases are more common in young cats, such as ingestion of foreign bodies [4a 37 ], intussusception [4b 120 , 4c 121 ] or infectious diseases, such as panleukopenia virus [5 122 ], parasites [4a123,124] or coronavirus enteritis [4c 125 ], while other diseases, such as hyperthyroidism or gastrointestinal or hepatobiliary neoplasia, are more common in older cats [4b 55 , 127 , 4c 126 , 128 ] [OEG C]. Breed is an important consideration: Siamese cats are predisposed to gastrointestinal adenocarcinoma [4c 126 ] and to pyloric stenosis [4c129,130]; lymphoplasmacytic gastroenteritis is more commonly seen in purebred cats [4c 48 ]; and adenomatous polyps of the duodenum are seen more in cats of Asian ancestry [4c 131 ] [OEG C]. Adenomatous polyps of the duodenum are more commonly seen in castrated males [4b 131 ] and, not surprisingly, some disorders only affect one gender, such as uterine abnormalities [4d132,133] or prostatic disease [4d110,134] [OEG C].
A complete history is essential for evaluation of a vomiting cat. Information that should be obtained is listed in Table 5. The distinction between vomiting and regurgitation is less clear in cats than in dogs, and cats with megaoesophagus, oesophagitis or hiatal hernia are often reported as vomiting [4b 135 , 4c 136 , 4d137–139]. A sudden onset of vomiting can suggest dietary indiscretion [4c 140 ]. Acute onset of vomiting is also seen with intestinal foreign bodies in cats, and the vomiting tends to be persistent and severe [4a 37 ]. Furthermore, in approximately one third of cases, the owner either reports seeing the foreign body or it is identified during the physical examination (at the mouth or anus) [4b 38 ]. Intermittent vomiting or recurrent episodes more often suggests a chronic alimentary tract disorder, for example, inflammatory bowel disease (IBD) [4d 141 ], gastrointestinal neoplasia [4b 142 , 4d143,144] or hepatobiliary disease [4b 55 ]. Furthermore, when haematemesis or melaena are present, gastric adenocarcinoma [4c 145 ], gastric ulceration [5], Physaloptera preputialis infection [4c 146 ] or gastrointestinal polyps [4c 131 ] should be considered; in contrast, haemorrhagic diarrhoea (large volumes of fresh blood) can indicate panleukopenia infection [5 122 ] and, occasionally, linear foreign bodies [4b 38 ]. Given the wide array of possible causes of vomiting (Tables 2–4), clinicians should also pay attention to the presence of other clinical signs. For instance, polydipsia may suggest a systemic disorder, such as renal disease [4d77,78], hyperthyroidism [4a79,80] or diabetes mellitus [4a 147 ], while lower urinary tract disorders should be considered if there is dysuria, pollakiuria or stranguria [4d134,148,149]. In such cases, there may also be associated physical examination findings, such as a distended painful bladder in cases of urethral obstruction [4d 134 ].
History taking for the vomiting cat

Physical examination is important and should include assessment of the features shown in Table 6. Abdominal palpation is of particular importance given the multitude of abdominal disorders in which vomiting is seen (Tables 2 and 3). In cats, gastrointestinal mass lesions [4b 142 , 4c 126 ], pancreatic masses [4c128,150, 4d82,151,152] and hepatomegaly [4a 51 , 4c 61 ] can be identified readily, and can help to narrow the list of possible differential diagnoses and refine the diagnostic approach. Further, gastrointestinal obstructive disorders commonly have abnormalities identified on physical examination [4b38,120, 4c 121 ]. However, while abdominal pain has been reported in cases of pancreatitis [2b 153 ], it is suggested to be less consistent than in dogs with pancreatitis [2b 153 , 5154,59] and is seen with other disorders, including cholecystitis or cholangitis [4c 57 ], septic peritonitis, [4b 155 ] and gastroduodenal ulceration [4c 156 ]. When icterus is seen in vomiting cats, it tends to be due to hepatic and post-hepatic diseases (rather than prehepatic causes), including extrahepatic biliary obstruction [4b53,54,59, 4d65,157], cholecystitis or cholangitis/cholangiohepatitis [4c 57 , 4d 58 ], hepatic lipidosis [4a 51 , 4d69,158], cholelithiasis [4c 159 ], and hepatobiliary neoplasia [4c 61 ]. Finally, careful palpation of the cervical area should be performed in all older cats with chronic vomiting, given that a palpable goitre is usually noted when hyperthyroidism is present [4a 80 ].
Important considerations in the physical examination of the vomiting cat

From the signalment, history and physical examination, the clinician should be able to categorise the patient as systemically ‘well’ (stable patient with no criteria for further assessment or treatment; Table 7) or ‘unwell’ (unstable patient with one or more criteria for intervention), establish a problem list, and identify appropriate diagnostic investigations and therapy [OEG D].
Criteria suggesting the need for further intervention in vomiting cats

PU/PD = polyuria/polydipsia; FIP = feline infectious peritonitis
Diagnostic approach
Cats with simple, mild, acute self-limiting emesis do not need further investigation, and can be treated symptomatically (see below) or simply monitored [OEG D]. In such cases, signs resolve after 1–2 days, with or without symptomatic and supportive therapy. However, this syndrome of acute and self-limiting emesis, a common reason for dogs presenting to veterinary surgeons, is probably less common in cats, and cats that are presented are relatively more likely than dogs to require treatment and investigation [OEG D]. Suggested criteria, whereby further assessment and management should strongly be considered when identified in a cat that is vomiting, are shown in Table 7 [OEG D]. These include: frequent acute vomiting [4a 37 , 4c 140 ], the presence of blood in the vomitus or melaenic faeces [4c131,145,146,156], abdominal pain [2b 153 , 4b 160 , 4c 156 , 4d 92,161 ], abdominal distension [4a120,162, 4b 163 ] and pyrexia [2b 153 , 4c 57 , 5 122 ]. Other criteria that suggest the need for further intervention include severe dehydration, signs of shock, a history of vomiting for more than 2 weeks or persistent vomiting despite symptomatic treatment [5]. All of these latter criteria have been suggested by expert opinion; although we would agree that these criteria are sensible, no objective information in support of their use could be identified.
Where signs of dehydration, shock or hypothermia are present, intravenous fluid resuscitation should be a priority and further examinations should also be considered, including haematological examination, a biochemistry profile and urinalysis [5]. If no abnormalities are discovered by abdominal palpation, it is appropriate to await the results of haematological examination, biochemistry profile and urinalysis [5]. In cats >6 years old, total T4 measurement should be considered in addition to routine clinicopathological assessments, given the possibility of hyperthyroidism [4a79,80] [OEG D].
Thoracic radiographs are indicated if the cat is dyspnoeic, tachypnoeic, has abnormalities on auscultation or if there is a suspicion of oesophageal disease based on the presenting history [4b 135 , 4c 136 , 4d137–139]. Diagnostic imaging of the abdomen should be considered in any vomiting cat, especially if abnormalities are found on abdominal palpation (eg, abdominal pain, mass, thickened intestines) [4a 51 , 4b 142 , 4c61,126,128,150, 4d82,151,152]: ultrasonography is the most appropriate imaging modality in many cases, but the information obtained is often complemented by the findings of radiography. Contrast radiography, endoscopy, exploratory coeliotomy or laparoscopy may also be considered (Table 8). If the cat is icteric, hepatic ultrasonography (with liver fine needle aspiration cytology, biopsy and/or cholecystocentesis) is indicated [OEG D].
Diagnostic tests used in the investigation of cats with vomiting

fTLI = feline trypsin-like immunoreactivity; fPLI = feline pancreatic lipase immunoreactivty; FNA = fine needle aspirate; ACTH = adrenocorticotropic hormone; CT = computed tomography; MRI = magnetic resonance imaging; PCR = polymerase chain reaction; FISH = fluorescent in situ hybridisation; IBD = inflammatory bowel disease; FPLV = feline panleukopenia virus; SNAP = SNAP Giardia test; EPI = exocrine pancreatic insufficiency; LPE = lymphoplasmacytic enteritis; CNS = central nervous system; MALT = mucosa-associated lymphoid tissue
There are numerous causes of gastrointestinal obstruction in small animals, but several are more commonly seen in cats, namely linear foreign bodies [4a 37 , 4b 38 ], trichobezoars [4c 36 ], focal intestinal neoplasia [4b142,164, 4c128,131,165, 4d144,151,157] and megacolon [5 166 ] [OEG D]. When diagnostic imaging findings suggest obstruction, exploratory coeliotomy should be performed [OEG D].
In those cases where further investigation is considered necessary or abnormalities are identified on initial diagnostic tests, a variety of other diagnostic tests may be indicated (Table 8). Additional tests to be considered include other blood tests (eg, trypsin-like immunoreactivity, pancreatic lipase, folate and cobalamin, lactate, coagulation tests), serology (eg, testing for feline leukaemia virus, feline immunodeficiency virus and coronavirus), faecal examinations [for flotation, culture, cytology and/or polymerase chain reaction (PCR)], examination of the vomitus, examination of peritoneal or thoracic effusion, fine needle aspiration cytology of any abnormal organs or masses found, testing for heartworm infection (in endemic areas), advanced imaging and an elimination diet trial. Furthermore, either endoscopy or exploratory coeliotomy can be used to examine the alimentary tract directly and to collect biopsies. Biopsies can then be used for histopathology, immunohistochemistry (to identify cell lineages and Coronavirus), fluorescence in situ hybridisation (to identify invasive bacteria), bacterial culture or PCR, if indicated by specific findings in the history or physical examination, and depending on availability [OEG D]. When endoscopy is performed, either the upper alimentary tract (eg, oesophagus, stomach and duodenum) the lower gastrointestinal tract (eg, rectum, colon, caecum and ileum) or both can be examined. Recent evidence suggests that, for some causes of vomiting (eg, IBD), both regions should be examined because the results of histopathological examination may not correlate [4a 167 ]. Exploratory coeliotomy may be more suitable in some cases of vomiting because of the frequency with which lesions outside the gastrointestinal tract are noted in cats with gastrointestinal signs [4b168] [OEG C]. These recommendations are made based on the available evidence but, as shown in Table 8, this evidence is frequently only of level 4 or 5. For example, it has long been accepted that assays for total amylase and total lipase are not useful in the investigation of pancreatitis in cats. While this may be true, the only objective evidence currently available for this supposition is a meeting abstract [5 169 ].
Treatment
Vomiting is unpleasant for cats and distressing to owners, and can be associated with adverse consequences, including anorexia, weight loss, food aversion and disturbances of fluid, acid–base and electrolyte balance. It may also cause aspiration pneumonia in severely sick cats [OEG D]. Although most cases of acute vomiting are likely to resolve without specific treatment, no objective data are available to determine the likelihood of this happening. When vomiting does not resolve spontaneously, a diagnosis should be sought to allow specific treatment of the underlying cause. Pending results of investigations, supportive care for the vomiting cat can include fluid and electrolyte therapy, and antiemetics (see below). However, antiemetics may be contraindicated where there is gastrointestinal obstruction [OEG D].
Antiemetic therapy
To date, there are no published clinical trials of antiemetics in naturally occurring cases of emesis in cats. Therefore, information on antiemetic efficacy must be drawn from experimental studies. In interpreting the results of these studies, consideration should be given to the emetic stimulus used in the study and, therefore, the likely emetic pathways involved. Certain important differences exist between dogs, cats and ferrets — the three species most commonly used in experimental emesis research and, therefore, extrapolating the results of experiments in different species to cats must be undertaken with caution. For example, D2 dopamine receptors in the AP are much less important in cats than in dogs, explaining the comparative resistance to apomorphine-induced vomiting cats [2b17,170]. In contrast, α2 adrenergic receptors are important in the areas of the cat brainstem controlling vomiting, explaining why the α2 agonist xylazine is an effective emetic agent in cats [2b171–173]. A schematic diagram showing the various receptors implicated in emesis in cats is shown in Figure 1 [OEG B].

Schematic diagram showing receptor types potentially involved in emetic pathways in the cat [OEG B]. 5HT = serotonin (5-hydroxytryptamine); α2 receptor = alpha-2 adrenergic receptor; ACh = acetyl choline; CRTZ = chemoreceptor trigger zone; H1 receptor = histamine type 1 receptor; NK1 = neurokinin 1
The antiemetics available in veterinary practice, and evidence of efficacy, are shown in Table 9. As mentioned above, published evidence in support of their use in this species is limited. The most effective antiemetics for cats appear to be those that work via NK1 (eg, maropitant) or serotonin (5-hydroxytryptamine, 5HT3) (eg, ondansetron) receptors [OEG B]. Drugs with α2 antagonist activity are anecdotally reported to be effective antiemetics in cats, but robust evidence to support their use is lacking [OEG D].
Antiemetic drugs in cats
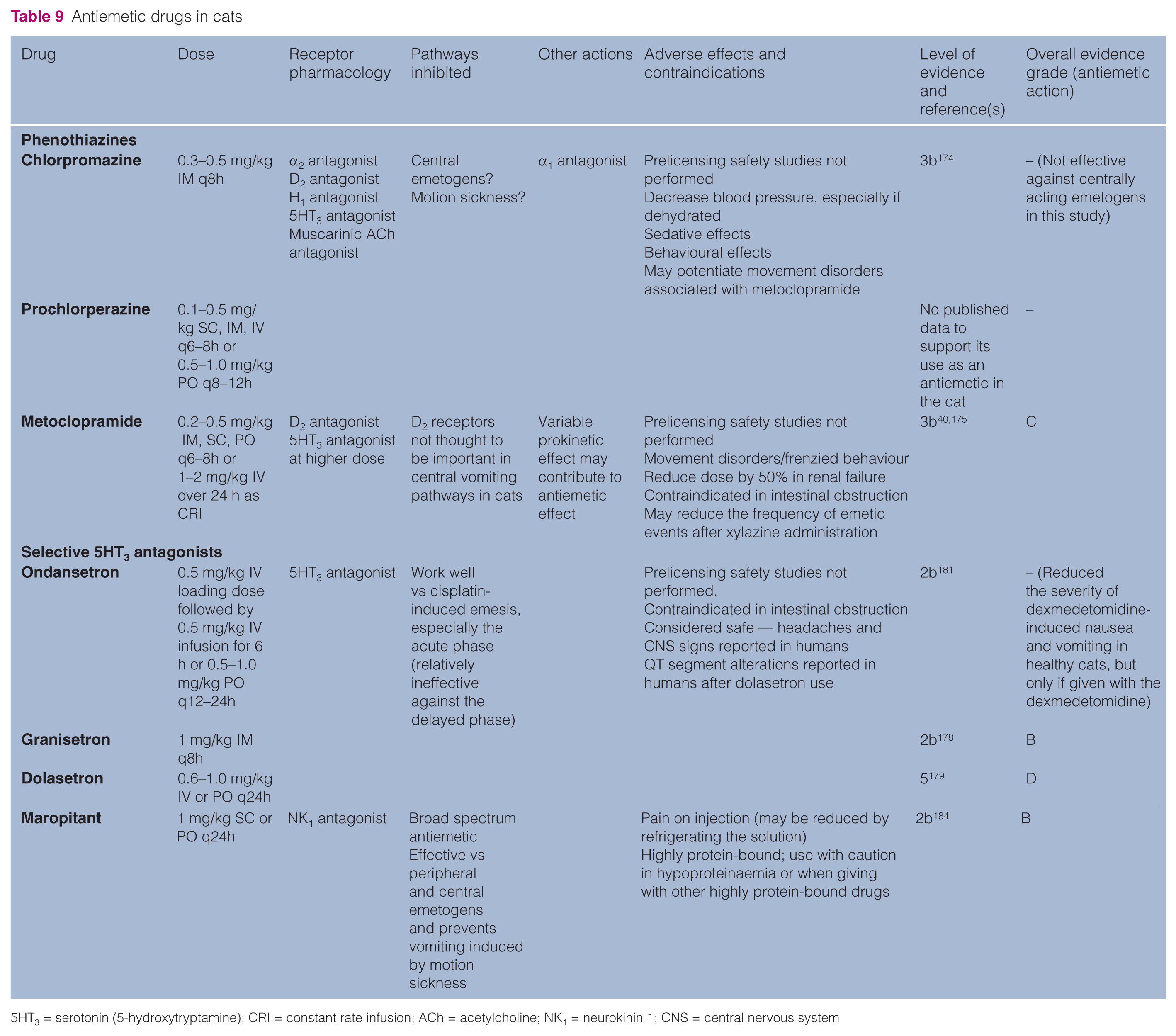
5HT3 = serotonin (5-hydroxytryptamine); CRI = constant rate infusion; ACh = acetylcholine; NK1 = neurokinin 1; CNS = central nervous system
Chlorpromazine was not effective against emetogens working via the AP in cats [3b 174 ], and there are no published reports on the use of prochlorperazine as an antiemetic in cats.
Although often listed as a first line antiemetic, metoclopramide, a D2 antagonist, is of questionable use as a central antiemetic in cats, and it failed to block the emetic response to dopamine administration in cats [2b 173 ]. Administration of metoclopramide to cats prior to xylazine injection reduced the frequency of emetic events in one study, but not in another [3b40,175]. The possibility that tolerance to xylazine caused the reduction in emetic events was not adequately excluded in that study. 40 Metoclopramide may be used in some circumstances where a gastrointestinal prokinetic action is desired, for example for ileus or delayed gastric emptying, but its prokinetic action is weak in the cat [2b176,177] [OEG B].
The 5HT3 receptor antagonist granisetron was effective against the acute phase of cisplatin-induced emesis (peripheral emetogen) in cats [2b 178 ], and there are anecdotal reports that the related drug dolasetron is also effective in this species [5 179 ]. In laboratory studies 5HT3 receptor antagonists prevented cisplatin-induced vomiting, but not vomiting induced by xylazine or motion [2b 180 ]. Ondansetron reduced the severity of dexmedetomidine-induced nausea and vomiting in healthy cats, but only if given at the time of dexmedetomidine administration [2b 181 ]. These drugs appear to act via peripheral 5HT3 receptors, although action at central sites may contribute to their efficacy [2b178,180,182,183] [OEG B].
Maropitant is a potent, highly selective NK1 receptor antagonist, which is well tolerated and safe in cats [2b184]. In a preliminary study, at the dose used in dogs (1 mg/kg SC), maropitant was effective in preventing xylazine-induced emesis (central emetogen) and motion sickness-induced vomiting in cats [4d 184 ]. It was effective when given subcutaneously or orally, and had a half-life in the cat suitable for once-daily dosing. However, use in larger numbers of cats is needed before strong recommendations can be made for its efficacy and to identify any uncommon adverse effects [OEG B].
For the treatment or prevention of motion sickness in cats, NK1 receptor antagonists are effective in the laboratory setting.184,185 Antihistamines are thought to be effective against motion sickness in some species. However, in cats, although an irreversible inhibitor of histamine synthesis prevented motion sickness, an H1 antagonist did not [OEG B] [2b 186 ].
5HT1A receptor agonists were shown to be effective against a range of emetic stimuli in the cat, but have not found their way into the clinic [2b187–190]. In particular, many cats showed marked defensive behaviour with these drugs, limiting their use [OEG B].
A variety of other drugs have been assessed for antiemetic effects in cats, but are not likely to be useful antiemetics in a clinical setting [OEG B] [2b191–200].
Dietary management
Many vomiting cats are systemically well and have self-limiting conditions, for example acute gastroenteritis. Dietary recommendations for this group are commonplace in review articles, but have little scientific basis [5201,202]. Nonetheless, the self-limiting nature of clinical signs in these cases, and absence of evidence to the contrary, mean that these practices will likely continue for the current time.
The standard dietary recommendation for cats with acute gastrointestinal disorders is to withhold food for 24–48 h, followed by administration of small quantities of a bland, highly digestible diet three or four times per day for 3–7 days [5203,204]. Such short-term fasting is said to provide ‘bowel rest’, thereby reducing gastrointestinal secretions and bacterial numbers, while avoiding the adverse effects of non-absorbed, osmotically-active food particles [5203,204]. Arguably, the bowel can also be ‘rested’ if a highly digestible diet is fed, as this is assimilated rapidly in the proximal small bowel [5 201 ] [OEG D].
In contrast, in human gastroenterology there is strong evidence in favour of feeding during gastroenteritis [2b 205 ]. Unfortunately, there are no equivalent published studies in cats. Some authors have argued that continuing to feed may exacerbate vomiting. Further, if present, diarrhoea may be exacerbated by the osmotic action of luminal food particles. For these reasons, food withholding is likely to remain as the most widely adopted strategy. That said, care must be taken in sick cats, especially if they are obese, given concerns over invoking hepatic lipidosis, a consequence of starvation in an obligate carnivore [2b206–208] [OEG C].
The term ‘bland diet’ is used commonly but defined rarely. Arguably, most canned foods are ‘bland’ because of their easy assimilation, while dry foods may be less suitable [5 201 ]. Many clinicians advocate switching to a diet containing a novel protein source, given concerns in humans that food allergies can develop to proteins eaten during a bout of acute gastroenteritis and delay recovery [2b 209 ]. However, no similar evidence is available in cats. Although a reaction to the novel ingredient could occur, adverse reactions to foodstuffs not typically part of the normal diet (eg, poultry meat) may be easier to manage than for a constituent of a commercially available pet food [OEG D].
Gastric emptying is slower for foods with greater fat content, so fat restriction is commonly advocated. That said, the response in cats with chronic gastrointestinal signs is similar when using diets of differing fat content [2b 210 ]. Diets with greater liquid content also empty faster: fully-liquid diets are quickest, followed by canned food, and dry kibbled diets are slowest [5 202 ]. Finally, fibre content may also influence emptying [5 202 ]. The feline stomach is less distensible than that of other species as their alimentary tracts are adapted to small, frequent meals [5 202 ]. As a result, large-volume meals may provoke further vomiting. Taken together, this would suggest that a moderately energy dense, low fibre, wet (or liquid) diet should be used in small meals frequently [5 202 ]. However, there has been no critical appraisal of this advice [OEG D].
Adverse reactions to food are reportedly a common cause of chronic gastrointestinal signs, including vomiting [2b28,30], with at least 50% of such cases responding when a diet based on novel ingredients is fed [2b 28 ]. Some have suggested favourable responses when using hydrolysed protein diets [4c 29 ], but no controlled studies exist. Nonetheless, favourable results were reported in a recent controlled trial assessing efficacy of hydrolysed protein diets for management of canine chronic enteropathy [2b 211 ] [OEG B].
In contrast to stable acute vomiting cases with self-limiting disease, nutritional requirements for hospitalised cats are different, and withholding food is not usually recommended. In humans, enteral feeding methods are superior to parenteral nutrition in critically ill patients [1b 212 ]. Such an approach improves survival, decreases infection rate, decreases bacterial translocation, has fewer complications and enables earlier discharge from hospital. There may be similar benefits in dogs, with experimental studies suggesting advantages of enteral nutrition over parenteral nutrition in a model of acute pancreatitis [2b213,214]. These findings are supported by two randomised controlled clinical studies comparing the efficacy of enteral nutrition in severe cases of gastroenteritis [2b215,216]. By extrapolation such strategies may be preferable in sick vomiting cats and may also reduce the likelihood of hepatic lipidosis [2b206–208] [OEG B].
A number of studies have provided information on the methods, applications and benefits of enteral nutrition [4a 217 , 4b 218 ]. Further, complications are well established, with vomiting being a prominent side effect [4a218,219]. There are also two experimental studies in cats assessing the benefits of enteral nutrition in cats given methotrexate chemotherapy [2b221,222]. These studies concluded that feeding a complex diet, containing intact protein as the nitrogen source, was preferable to the use of ‘elemental’ diets containing free amino acids as the only nitrogen source. While these findings may be most relevant to cats receiving chemotherapy, the conclusions may be pertinent to cats with other gastrointestinal disorders [OEG C].
In conclusion, limited information is available on appropriate nutritional management of vomiting cats. For those requiring hospitalisation, published studies in other species support the use of early enteral feeding. Enteral nutrition would also be favoured in cats with severe acute pancreatitis, although the only veterinary data would suggest that jejunostomy tube feeding is suitable. There is no direct evidence to support or refute the use of early enteral feeding in acutely vomiting cats that are managed as outpatients.
Monitoring
There are no published studies specifically addressing the most appropriate methods for monitoring vomiting cats. Most case series and reviews mentioning monitoring recommend using techniques appropriate to the underlying disease, including frequent clinical assessment during hospitalisation (especially postoperatively) [4b53,163, 4c 223 , 4d224,225], laboratory investigations [4a226,227], [4a226,227, 4b 155 , 4d64,228], indirect blood pressure measurement [4b 229 ], and diagnostic imaging [5230,231] [OEG C].
The optimal timeframe for reassessment has also not been addressed specifically; when symptomatic treatment is administered to a vomiting cat suspected to have self-limiting disease, an initial maximum of 24 h antiemetic treatment is the usual recommendation. If vomiting continues beyond this time, if other signs have not improved, or if new signs are evident (eg, deterioration in appetite or general demeanour, or appearance of diarrhoea), we recommend that reassessment should occur no more than 48 h after the first visit. Owners should be warned that the use of an antiemetic drug can mask signs of vomiting associated with an underlying disease and should be asked to return sooner if there is no improvement or there is any clinical deterioration. At revisit, the cat should be reassessed for criteria that may necessitate further assessment or management (Table 7), and further treatment and investigations should be performed as appropriate (see above) [OEG D].
Vomiting in cats with cancer
Cats with benign or malignant tumours may vomit because of the presence of the tumour (eg, in the alimentary tract [4b46,127,142,164, 4c126,128,131,145,165, 4d86,143,157,232–234]; in the hepatobiliary system [4b53,55, 4c 61 ]; affecting the pancreas [4c 150 ], or present systemically [4c 87 , 4d84–86]) or because of paraneoplastic effects [4c 235 , 4d149,228,236–238] [OEG B].
Cancer chemotherapy also is associated with vomiting and nausea in cats, and can lead to adverse consequences, including anorexia [2b 239 , 4b 240 ]. Data from other species suggest that some anticancer drugs are more likely to cause vomiting than others [3a2,241], but similar data are not available for the cat. Anticancer drugs that have been associated with vomiting in tumour-bearing cats include cyclophosphamide [2b 242 ] ifosfamide (vomiting was mild and self-limiting) [2b243,244], doxorubicin [2b245,246], methotrexate [2b221,222], vincristine/cyclophosphamide combined [4b 247 ], mitoxantrone [4b 240 ], idarubicin [4b 248 ], chlorambucil (NB, treated cats had alimentary lymphoma) [4c 128 ] and vincristine [5 249 ]. Vomiting occurred in 16% of cats receiving piroxicam, more often when the cat was also receiving cancer chemotherapy, particularly doxorubicin or carboplatin [4a 250 ]. However, carboplatin did not cause vomiting in nine healthy cats [3b 239 ]. Cisplatin is used frequently in experimental emesis research and causes vomiting in cats [2b178,251], associated with serotonin release from the intestine [2b 252 ], but the mechanism of cisplatin-induced vomiting in the cat may be different to other species [2b 14 ]. Cisplatin is not used clinically in cats because of extreme toxicity in this species [2b178,251] [OEG B].
There are no published studies of antiemetic use in tumour-bearing cats receiving cancer chemotherapy. Some antiemetics that have been evaluated for protecting against chemotherapy-induced vomiting are not likely to be useful in the clinic [2b187,190–192]. 5HT3 antagonists have shown some efficacy against cisplatin-induced vomiting in the cat [2b178,180], but, as mentioned above, this is not directly relevant to chemotherapy in the cat because cisplatin should not be used. Anecdotally, dolasetron combined with metoclopramide could reduce the emetic potential of many drugs [5 179 ] [OEG D]. While maropitant has demonstrated efficacy in preventing and treating nausea and vomiting induced by cisplatin in dogs, 254 there is no available evidence in cats.
Discussion
The current study is the first to attempt a comprehensive review the available evidence for causes, consequences, diagnosis and management of vomiting in the cat. The main aim of such a systematic review was, as far as possible, to present the available published evidence without prejudice or bias. For instance, it was necessary to report all the conditions where the published evidence suggests that it is a clinical sign. This can be helpful as it emphasises the necessity for keeping an open mind when investigating cats with signs of vomiting. Nonetheless, it is accepted that many clinicians may have their own opinions as to the validity of some of the reported associations. In this respect, the pathogenetic mechanisms for many of the conditions listed may not be clear and associations may actually be indirect (eg, disease A causes condition B which causes the vomiting). As a result, we have also attempted to highlight the most important causes of vomiting, especially those conditions that are especially important in cats. Such information represents our opinion, albeit after detailed review of the available literature and, thus, should be considered cautiously. It is possible that such information will need to be revised should new information become available in the future. In a similar manner, a wide array of diagnostic tests has been reported in the literature, yet many are uncommonly used in clinical practice owing to cost, availability or the fact that they have been superseded by better techniques. Again, therefore, we have highlighted those tests that we think to be of most use, based upon current knowledge, but recognise that opinions may change in time.
As is the case with many systematic reviews, a key study finding is that, despite the availability of numerous relevant publications, much of the evidence is weak (eg, LOE 4 or weaker, OEG C or D). The main exception is the information available on the emetic reflex in cats, largely as a result of the fact that much of the fundamental physiological knowledge has been derived from work in this species. While the relative dearth of more robust evidence, in other areas of the review, does not mean that the data available are invalid, it highlights the limit to our current knowledge and the need for further studies to be performed at more robust evidence levels. In our opinion, many areas require further study, including the need to clarify which historical and physical examination findings are most useful in determining the need for further intervention, and which novel tests will be of use for vomiting cases. However, most important is the need for more objective clinical evidence on the efficacy of the various treatments for vomiting in cats, including the potential benefits of nutritional support, antiemetic drugs and ancillary therapies. This last area is likely to provide the greatest benefit to feline patients.
One limitation of the study is the methodology used, namely limiting the information reported to that identified on literature searches using terms to describe vomiting (eg, vomit, emesis, antiemetic, etc). Although this enables much of the relevant literature to be identified, we recognise that some publications may be missed, for instance if they did not mention a relevant term in the title, abstract or keywords. Nonetheless, arguably, limiting the review in such a way ensures that the most relevant articles are used, as the vomiting is more likely to be a significant part of the disease condition reported. Such missing information is better identified by performing further evidence-based reviews but from the perspective of specific conditions. These approaches are complementary and would be the best way to ensure that no gaps in knowledge are left.
Conclusions
This systematic review of the literature relating to causes, diagnosis and management of vomiting in cats has identified and summarised a large body of information. This review highlights the unfortunate fact that much of what we consider standard practice for cats is based on limited scientific evidence, on evidence extrapolated from other species or on expert opinion alone. Nonetheless, in some areas good evidence does exist, most notably concerning the mechanisms of vomiting. It is hoped that further research will improve knowledge in other areas, most notably concerning therapy for vomiting cats.
Footnotes
Acknowledgements
We would like to acknowledge the help and support of Pfizer Animal Health. AJG’s senior lectureship is supported by Royal Canin. The individual author contributions are as follows: DJB performed literature searches and collated information, drafted the initial manuscript, and reviewed and revised the manuscript for submission; PD and JE were involved in planning discussions and reviewed the manuscript; CME, VF, MG, EJH, EdH, DP and XR were involved in planning discussions, contributed to initial draft and reviewed the manuscript; RN was involved in planning discussions and reviewed the manuscript; KSB reviewed the manuscript; AJG was involved in planning discussions, contributed to initial draft, and reviewed and revised the manuscript for submission.
Funding
Pfizer Animal Health provided financial support to cover the costs of performing the initial literature searches.
Conflicts of interest
The European Emesis Council is supported financially by Pfizer Animal Health, the manufacturers of maropitant. One of the authors (KB) is an employee of Pfizer Animal Health, who was involved in reviewing the manuscript prior to submission. However, while comments could be made on the article content, Pfizer Animal Health were not allowed to draft or review the ‘antiemetic therapy’ section, could not prevent information from being included and could not prevent the work from being submitted for publication.