
Abstract
Feline injection-site sarcoma (FISS) may be a consequence of subcutaneous injection. In the present study, the medical records and the computed tomography (CT) features of 22 cats with a FISS, histopathological subtype fibrosarcoma, were used. The majority of the fibrosarcomas (45%) were located in the interscapular region. All fibrosarcomas, except one with mild enhancement, showed strong contrast uptake, characterised as ring (42%), heterogeneous (36%), homogeneous (9%), heterogeneous/ring (6.5%) or mixed heterogeneous/homogeneous enhancement (6.5%). The longest axis of the mass was in a cranio-caudal (68%) or dorso-ventral (32%) direction. The median volume calculated on CT was 7.57 cm3. Common features were a marked local invasiveness of the musculature and heterogeneity of the tissue in the periphery of the neoplasia. When the fibrosarcoma was interscapular, performing an additional post-contrast scan with the forelimbs positioned caudally along the body, in addition to the standard protocol with the forelimbs extended cranially, allowed better evaluation of the actual relationship between the tumour and the surrounding tissues. The mean number of muscles involved with the tumour was 2.09 with extended and 1.95 with flexed forelimbs. When a lower number of structures was considered infiltrated through the double positioning, a less invasive surgical approach to underlying muscles and scapula was performed.
Introduction
Feline injection site sarcoma (FISS) was described for the first time in 1991 in the USA. 1 The exact aetiopathogenesis of FISS is still unknown; however, the basic mechanism is an anomalous response to a chronic inflammatory process developed after administration of vaccines, long-acting antibiotics, methylprednisolone or non-adsorbable suture material, associated with some genomic imbalances.2 –5 Biologically, FISSs are characterised by rapid growth, locally invasive behaviour and a low distant metastatic rate (5–20%), with the lungs, abdominal organs and regional lymph nodes as predilection sites.3,4,6 Histologically, FISSs can be differentiated in fibrosarcoma, myofibroblastic sarcoma, myxosarcoma, undifferentiated sarcoma, malignant fibrous histiocytoma, rabdomyosarcoma, osteosarcoma and chondrosarcoma, all typically characterised by large necrotic areas and a prominent peri-lesional inflammatory/lymphocytic reaction.3,4,6
Many efforts have been made to establish an appropriate, standardised approach to FISS, leading to the assessment of some guidelines from the Vaccine-Associated Feline Sarcoma Task Force and from the Vaccination Guidelines Group of the World Small Animal Veterinary Association.7,8 The most critical point in the treatment of FISS is performing, at first presentation, an aggressive surgical resection to ensure a complete excision of the tumour and to reduce the rate of local recurrence.3,4,6,9,10 However, even with a radical resection, local recurrence is common (14–50%). 3 Typically, in the closeness of the sarcoma, small neoplastic lesions missing any anatomical connection with the primary mass (‘skip metastasis’) are present. These represent true subcutaneous metastasis. The assessment of the microscopic margins of the tumour, as well as the relationships with the surrounding structures, can be challenging for the surgeon in the pre-operative staging. Therefore, computed tomography (CT) and/or magnetic resonance imaging (MRI) represent essential pre-operative steps for optimal characterisation and staging of the tumour. These modalities allow evaluation of the tumour size and its relationship with surrounding soft tissues and bones, as well as the presence of skip and distant metastasis. The tumour content can be further classified by the enhancement characteristics of the FISS after intravenous administration of contrast medium. Both modalities are also useful for follow-up evaluation after chemotherapy and/or radiation therapy, which are frequently combined with surgical therapy. 11
The aim of this study is to describe the CT features of FISS at first presentation attributable to the fibrosarcoma histological subtype. Fibrosarcomas represent the most common histological subtype among FISSs.6,10
Materials and methods
A search was performed in the database of the Veterinary Faculty of Milan for all cats with a histopathological diagnosis of fibrosarcoma and that underwent a CT examination between January 2005 and December 2011.
The following criteria were retrieved from the database: signalment and body condition score of the patient; anatomical site and clinical longest axis of the tumour (using calipers from the outside); CT features of the fibrosarcoma, surrounding tissues and thorax; surgical technique and postoperative complications; recurrence; and follow-up, if available.
In all cats, helical CT studies were performed using a fourth-generation single-slice CT (PQ2000S; Philips MD), with a slice thickness of 3–5 mm (depending on tumour size), 200–250 mAs, soft tissue algorithm, before and after intravenous administration of Iodixanol (Visipaque 320, 320 mg iodine/ml; GE Healthcare) at 600 mg I/kg. The studies were performed with the patient in sternal recumbency with the forelimbs extended cranially. Both the mass and the thorax were scanned. When the disease involved the interscapular region, an additional sequence with the forelimbs positioned along the body was performed immediately after the post-contrast scan. After acquisition, the images were reprocessed with 2 mm thickness and a high-resolution algorithm to evaluate the lung parenchyma for metastasis. The first author reviewed all the studies. On the pre-contrast studies, tumour location (with respect to surrounding structures) and the number of muscles in direct contact with the mass were assessed. On the post-contrast images, contrast enhancement (presence or absence, pattern), aspect of the margins (capsulated or irregular), prominent peripheral vascularisation (present or absent), distant metastasis (absent, suspected, present), regional lymph nodes (normal or enlarged, degree of contrast enhancement) and volume of the tumour (cm3) were evaluated. The volume of the tumour was assessed following multiplanar reconstruction (MPR) of post-contrast images through the formula for the ellipsoid volume: 4/3π(1/2 X*1/2Y*1/2Z), where X represented the latero-lateral, Y the dorso-ventral, and Z the cranio-caudal dimension. When a double positioning was performed, the new position of the tumour in respect to the surrounding structures was assessed after MPR.
Results
Twenty-two cats fulfilled the criteria and were included, of which 21 were domestic shorthair cats and one a Chartreux. Fourteen cats were neutered males, seven were neutered females and one was a non-castrated male. The mean age was 11.2 years (range 7–16 years). Mean body weight was 4.9 kg (range 3–8 kg). The mean body condition score was 3.13. The FISS was interscapular (n = 10), located at the right flank (n = 3), in the right paravertebral region (n = 3), in the right paracostal region (n = 3), in the left paracostal region (n = 2) and in the right axillary region (n = 1). On physical examination, the longest axis of the mass ranged from 1.5 to 10 cm (mean 3.88 cm). Clinically, the longest dimension of the mass was in a cranio-caudal (82%) or latero-lateral (18%) direction; the dorso-ventral direction was not assessable clinically.
Ten cats were scanned with both extended and flexed limbs. In eight of these cats there was no difference between the two positionings in the number of muscles or structures coming into contact with the tumour. In the other two cats, the flexed position revealed fewer muscles invaded by the tumour compared with the extended position. In one of these cats, the right trapezius muscle appeared involved with forelimbs extended, while with forelimbs flexed a fat margin was visible between the tumour and this muscle. In the second cat, six muscles seemed to be involved with the forelimbs extended (right and left trapezius and rhomboideus, right supraspinatus and right semispinalis), while with the forelimbs flexed the right supraspinatus and right semispinalis muscles appeared intact. The mean number of muscles involved was 2.09 with forelimbs extended and 1.95 with forelimbs flexed. The longest axis on CT was the cranio-caudal dimension in 15 cats and the dorso-ventral dimension in seven cats. It measured between 1.2 and 6 cm (mean, 3.6 cm). The calculated volume ranged from 0.1 to 185.38 cm3 (mean volume 21.97 cm3; median volume 7.57 cm3).
On post-contrast CT, all the tumours, except one, showed contrast enhancement characterised as ring enhancement (n = 9) (Figure 1), heterogeneous (n = 8), homogeneous (n = 2), mixed heterogeneous/ring (n = 1) and mixed heterogeneous/homogeneous (n = 1). The heterogenous pattern was characterised by the presence of areas of irregularly outlined enhanced tissue adjacent to one or multiple non-enhancing areas, likely corresponding to necrotic centres (Figure 2). A well-defined outer pseudo-capsule was visible surrounding the mass in 13 cats, while in nine cats the margins were poorly defined. The mass frequently sent multiple linear peripheral extensions of variable thickness into the muscular layers (Figure 3). The fat surrounding the periphery of the tumour was often heterogeneous, presenting some linear or nodular hyperdensities. After contrast medium administration, these densities appeared to be either small vessels or a skip metastasis (Figure 4a, b). In two cats, there was consistent vascular supply peripheral to the mass. A skip metastasis was present in one cat, but no cat showed distant metastasis. Enlargement (compared with the contralateral node) and contrast enhancement of the ipsilateral axillary lymph node were present in five cats. Surgical excision was performed in all cats following either a ‘Y’ (n = 18) or a linear pattern (n = 4). After surgery, 10 patients developed complications represented by dehiscence (n = 8), seroma (n = 1) or unspecified (n = 1). The follow-up period ranged from 69 to 2555 days (mean, 778.41 days). At follow-up after 12 months, 14 cats were alive and recurrence-free, three died after recurrence of the tumour, three died for a cause unrelated to the tumour, one was alive with recurrence and one died of unknown cause.

Post-contrast computed tomography image (window level: 40; window width: 350) of an elliptical right interscapular fibrosarcoma. The deepest part of the mass is in contact with the spinous process of a cranial thoracic vertebra and the caudo-dorsal aspect of the scapula (arrowheads). There is a well-defined, highly enhancing peripheral rim, outlining a central non-enhancing area, mimicking a pseudocapsule (ring-like enhancement)

Post-contrast computed tomography image (window level: 0, window width: 354) of a fibrosarcoma of the flank. The lesion involves the skin and the subcutaneous tissue, with mass effect on the right abdominal wall. There are areas of irregularly outlined enhancing tissue adjacent to others characterised by minimal enhancement (heterogeneous enhancement)
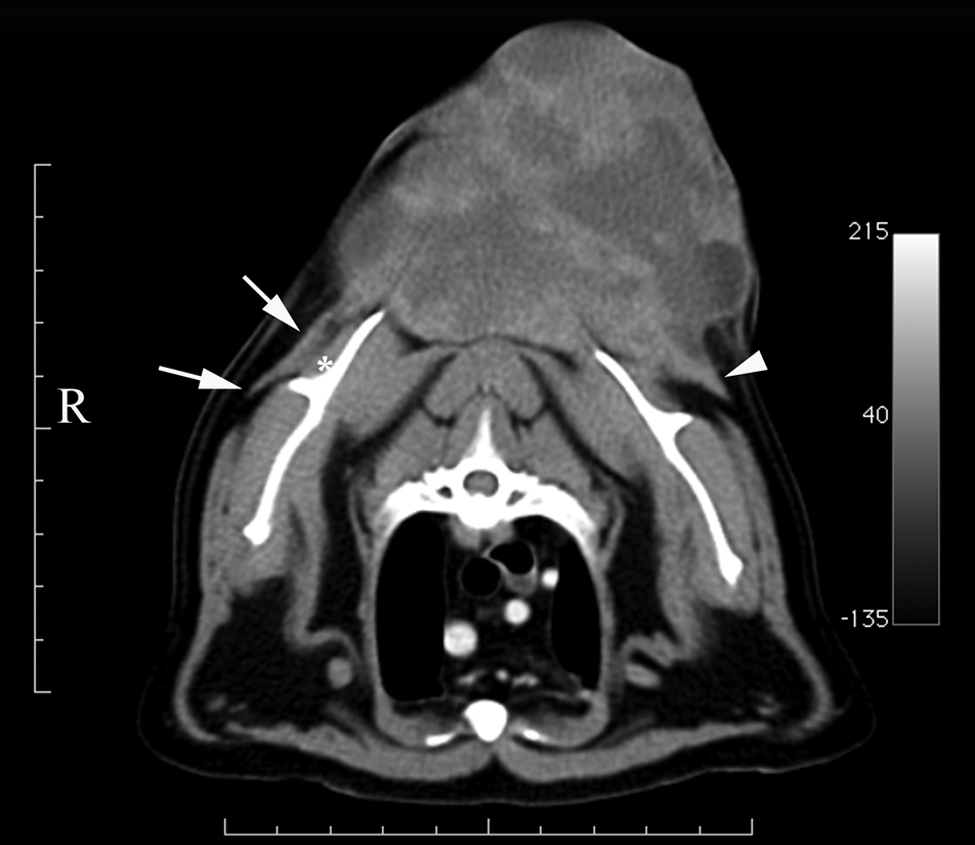
Post-contrast computed tomography image (window level: 40, window width: 350) of a globoid interscapular fibrosarcoma, characterised by heterogeneous enhancement. There are two thick linear extensions arising from the periphery of the deepest portion of the mass, on each side (arrowhead). The extension visible on the right side (arrows) is in contact with the supraspinatus muscle (asterisk) and with the scapular spine

(a) Post-contrast computed tomography image (WL: 11, WW: 354) of a paracostal fibrosarcoma infiltrating the midportion of the longissimus thoracis muscle (arrowheads), showing heterogeneous contrast enhancement. (b) Post-contrast CT image (WL: 11, WW: 354) of the same paracostal fibrosarcoma taken some centimetres cranially with respect to (a). Within the middle-right aspect of the subcutaneous tissue, dorsal to the spinous process, a soft tissue nodular structure is visible, presenting an enhancement similar to the muscular tissue (arrows). This small nodule was not palpated clinically and is highly suspicious for a skip metastasis
Of the four cats experiencing local recurrence, one cat had tumour extending to one surgical margin on histopathology, one cat had one unclear surgical margin and an enlarged contrast enhancing regional lymph node at initial CT, and two had clear surgical margins and a normal regional lymph node.
Discussion
Despite many articles’ focus on the clinical or surgical aspects of FISS,2 –4,6,8,10–15 the imaging literature only deals with this disorder briefly.
The role of CT in the approach to FISS is related to the biological behaviour of the neoplasia. CT allows objective assessment of the local extension, including the involvement of underlying fasciae, muscles and bones, and can detect skip metastases — both essential prerequisites for adequate surgical planning. At the same time, CT allows evaluation of local lymph nodes not assessable clinically, as well as detection of distant metastasis.2,3,7,11 Furthermore, CT is a way to investigate the characteristics of the tissues surrounding the sarcoma before surgery. As mentioned previously, a distinctive feature of FISS is the prominent peri-tumoural vascular supply and inflammatory reaction.3,6 The inflamed, highly vascularised tissue is actually an active part of the neoplasia, and has to be included within the surgical plan, but is not detectable clinically at palpation (Figure 5). A wide margin resection, combined with radiation therapy and chemotherapy, is critical for the local control of the neoplasia.2 –4,6,15 MRI has superior soft tissue resolution than CT, but because FISS is frequently located in the thoracic region, specific respiratory and cardiac gating sequences are needed. This restricts the use of MRI in cats with FISS to high-field units. Additionally, CT is less time consuming and allows assessment of the lung parenchyma for distant metastases at the same time. In this study, the majority of the tumours were located in the interscapular region, which, for a long time, has been the most common site, worldwide, for subcutaneous injection of vaccines and other drugs in cats. Subsequently, it has been proposed that vaccines, especially those that are adjuvanted, should be injected in subcutaneous sites that are more amenable to surgical resection than the interscapular region, for example, the distal part of the hindlimbs.5,16 It is unknown, however, whether this recommendation is followed in daily veterinary practice, as cats rarely have a record of their vaccination sites. On CT, adopting the flexed positioning in addition to the standard extended one allowed better appreciation of the degree of involvement of adjacent structures that were in direct contact with the tumour compared with the study performed in a standard position (Figure 6a, b). This differentiation is useful in order to spare normal tissues from surgical excision. In our study population, 10 cats were scanned with double positioning and, in two cases, the flexed position detected fewer muscles infiltrated by the tumour. In both cases, histopathology confirmed the findings made on the CT examination with flexed limbs, determining that the corresponding specimen margin was not infiltrated. In one case, the muscle was adjacent to the scapula and by assessing its integrity on CT, scapulectomy was avoided at surgery. Double positioning should always be performed with interscapular FISSs in order to avoid needlessly invasive surgical excision. The difference in structure involvement noted between these positions is probably related to the fact that moving the forelimbs caudally along the body allows the interscapular tumour to move together with the subcutaneous tissue following the movement of the forelimbs. This allows the tumour to slide over the tissues to which it is not attached and to drag with itself the tissues that have been infiltrated.

Post-contrast computed tomography image (WL:15, WW: 370) at the level of the thorax. The fibrosarcoma is elliptical and includes a peripheral part showing ring enhancement and a deeper portion, with homogeneous uptake, adherent to the lateral surface of the right rhomboideus muscle (arrow). The overall pattern of contrast uptake is considered heterogeneous. Two linear hyperattenuating structures converge on the superficial portion of the mass from the periphery, most likely representing vessels (arrowheads). The subcutaneous fat is markedly irregular in the closeness of the mass

(a) Post-contrast computed tomography image (WL: 40, WW: 350) of an interscapular fibrosarcoma. The forelimbs are extended cranially. The mass, presenting a heterogeneous contrast enhancement, is in contact with the caudal part of the infraspinous fossa of the right scapula, which is not abnormal (arrow). (b) Post-contrast CT image (WL:40, WW: 350) of the same fibrosarcoma. The forelimbs are flexed along the body. The tumour involves the right rhomboideus muscle and the most dorsal part of the longissimus thoracis muscle (arrowheads). The caudal part of the scapula has moved cranially by flexing the forelimbs along the body. The combination of the two images demonstrates that the tumour is not attached to the scapular surface
A larger FISS is more invasive locally, involving a greater number of muscles and underlying bony structures. 17 In our study, the local invasiveness and the volume of the fibrosarcoma were not compared statistically owing to the limited number of cases, however our results seem to agree with what was stated previously. 17
There was a discrepancy between the tumour’s longest axes, as measured clinically and by CT. Clinically, only two dimensions could be measured, with the third deep margin being hidden. In contrast, on cross-sectional imaging, complete evaluation of all three axes was performed. Consequently, a discrepancy between the clinical and CT longest axes arose, and a comparison between clinical and CT tumour dimension was not feasible.
At CT, the mass frequently sent multiple linear peripheral extensions of variable thickness into the depth of the muscular layers. Therefore, a complete CT study of a wide subcutaneous area is strongly advised to depict these ramifications and correctly estimate the size of the mass, as well as to detect any additional nodules. The measurement of the three dimensions of the tumour is challenging when the mass is poorly outlined. In our study, when peripheral extensions arising from the main mass were present, these were taken into account when estimating the dimensions because they represent an active part of the tumour.
According to the literature, all tumours enhanced after contrast administration. In one cat in our study, the fibrosarcoma showed only mild contrast enhancement. In this cat, the tumour was very small (0.1 cm3), so it may be postulated that the neoplasia was imaged at an early, poorly vascularised stage.
In five cases the axillary lymph node ipsilateral to the tumour had a more prominent contrast uptake and was larger than the contralateral one, but it was always ≤1 cm in diameter. Surgical exploration of the axillary region in order to detect the lymph node within the fat typically present in this region would, potentially, have been dangerous for the brachial plexus owing to the small dimension of the lymph node, so it was not performed. In human medicine methylene blue is used in similar cases, allowing removal or biopsy of even smaller lymph nodes. Contrast-enhanced ultrasonography may represent an interesting alternative for non-invasive diagnosis of lymph node metastasis. 18 Distant metastases were not observed on CT in this cat population; however, we cannot rule out that the observed lymph nodes changes represented early metastatic invasion.
Conclusions
Performance of a CT study of a wide subcutaneous area around the fibrosarcoma to assess the peripheral tissues is strongly recommended. When a fibrosarcoma is located in the interscapular region, an additional post-contrast scan with flexed forelimbs may be necessary to correctly estimate the extent of the local invasion and avoid unnecessarily invasive surgical resection. It is recommended that abnormal regional lymph nodes are assessed cytologically, through scintigraphy or contrast-enhanced ultrasonography before surgery whenever feasible.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.