
Abstract
A 7-year-old Siamese cat presenting with three ulcerated cutaneous nodules in the lumbosacral region was seen at the Laboratory for Clinical Research on Dermatozoonoses in Domestic Animals in Rio de Janeiro, Brazil. Histopathological analysis showed that the lesions consisted of polyhedral and spindle-shaped voluminous mononuclear cells with loose chromatin and clearly visible nucleoli, few giant cells, and foci of coagulative and caseous necrosis — findings suggestive of a vaccine-induced sarcoma. No significant mitotic rate, cytological atypias or asteroid bodies were observed. Special histopathological staining with periodic acid-Schiff and Grocott’s silver stain demonstrated the presence of small yeast cells characterized by simple and narrow-base budding compatible with Sporothrix schenckii. Mycological culture grew S schenckii. Cytopathology was negative for yeast cells. These atypical clinical and histopathological signs support the importance of histopathological analysis with special staining techniques, in addition to mycological culture in the diagnosis of feline sporotrichosis.
Case Report
A 7-year-old domestic female Siamese cat weighing 3 kg was seen at the Laboratory for Clinical Research on Dermatozoonoses in Domestic Animals, Brazil. The animal presented with ulcerated cutaneous nodules that had been present for 36 months, which measured 1–2 cm in diameter, and swelling in the lumbo-sacral region (Figure 1). No other changes were observed and the cat had been active and in good condition over the period. The owner reported repeated local recurrences at intervals of about 6 months after six surgical resections during the 36-month period.

Three 36-month-old ulcerated cutaneous nodules measuring 1–2 cm in diameter and swelling of the lumbosacral region
After a new surgical resection, cytopathological and histopathological analysis were performed. An imprint smear and an incisional skin biopsy was obtained from one ulcerated cutaneous nodule. Grossly, the lesion presented as a white, firm and poorly circumscribed ulcerated nodule. The specimen was divided into two fragments: one was fixed in 10% buffered formalin, embedded in paraffin, microtome-sectioned and stained with hematoxylin-eosin (HE), periodic acid-Schiff (PAS) and Grocott’s silver stain for histopathological analysis; the other was put in sterile saline solution for mycological examination.
Cytopathological analysis of the smear, stained with giemsa, revealed an inflammatory exudate rich in neutrophils and macrophages. Fungal structures were not observed.
Histopathological analysis of the HE-stained specimen revealed a nodule that consisted of polyhedral or spindle-shaped voluminous mononuclear cells with loose chromatin and clearly visible nucleoli, accompanied by the presence of few giant cells and areas of coagulative and caseous necrosis, simulating a malignant mesenchymal neoplasm (Figures 2 and 3). However, no significant mitotic rate or cytological atypias were observed.
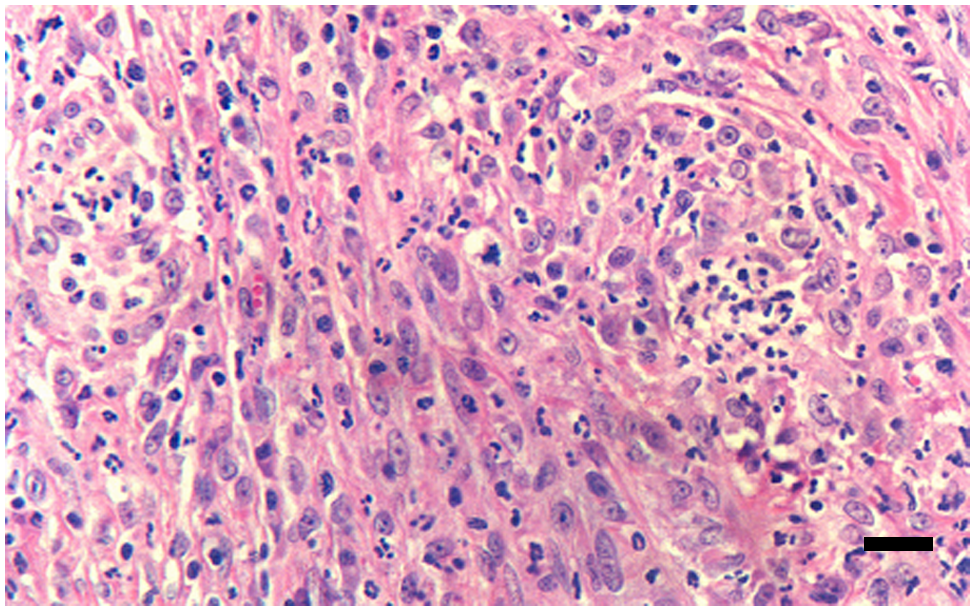
Ulcerated cutaneous nodule of the lumbosacral region. Polyhedral or spindle-shaped voluminous mononuclear cells with loose chromatin and clearly visible nucleoli. HE staining. Bar = 10 µm
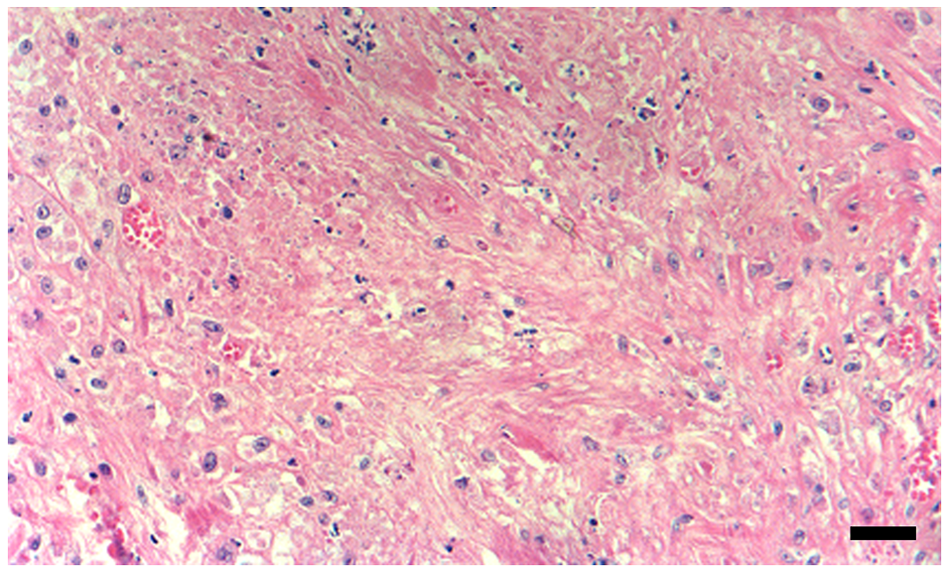
Cutaneous nodule of the lumbosacral region. Coagulative necrosis. HE staining. Bar = 10 µm
Staining with PAS and Grocott’s silver stain demonstrated occasional uniformly small round or oval yeast-like structures, some of them exhibiting simple and narrow-base budding, findings compatible with Sporothrix schenckii (Figure 4).

Cutaneous nodule of the lumbosacral region. Yeast-like structures exhibiting simple and narrow-base budding compatible with S schenckii. Grocott staining. Bar = 10 µm
Under mycological examination, S schenckii was isolated from active lesions by inoculating the specimen in Sabouraud’s agar at 25°C for 4 weeks. Sporothrix schenckii was isolated in the last week. The isolated fungus was cultivated on agar–brain–heart-infusion medium (Difco) at 37°C and dimorphism was demonstrated by conversion to the yeast-like form.
After 30 days the owner returned with the animal for follow-up and the three ulcerated nodular lesions had converged into a single ulcer. Isolation of the patient was recommended and the owners were informed about the elevated zoonotic potential of feline sporotrichosis. An azolic antifungal treatment with ketoconazole (10 mg/kg, PO, q24h) was started and the lesions were completely healed in 6 months. No animal or human contactant manifested similar lesions.
Sporotrichosis is a subcutaneous mycosis caused by S schenckii, a dimorphic fungus widely found in nature, specifically in soil, plants and decomposing organic matter, and which can affect various animal species, including humans. 2 Classically, infection usually occurs by traumatic inoculation of the fungus through contaminated material, mainly affecting individuals who are in contact with soil and plants, and rarely through inhalation of conidia. 1
In the metropolitan region of the State of Rio de Janeiro, a sporotrichosis epidemic involving cats, dogs and humans has been observed since 1998, in which most human cases result from scratches and/or bites of cats with sporotrichosis.2 –4
Feline sporotrichosis usually develops in intact male cats. Clinically, the disease is characterized by the presence of multiple skin lesions, including subcutaneous nodules with purulent secretion that tend to ulcerate, crusty lesions, vegetating ulcers, and extensive and exudative ulcers, which may be accompanied by lymphangitis, lymphadenitis and respiratory signs.5,6
The main histopathological finding of active skin lesions in cats is the presence of a mixed inflammatory infiltrate in the dermis consisting of plasma cells and neutrophils, accompanied by numerous cigar-shaped, round or oval, intracellular structures measuring 5–7 µm in length or diameter, some of them exhibiting single budding. 7
In cats, the development of sarcomas in application sites of vaccine is described. 8 Feline injection-site sarcomas generally present as non-painful solid masses firmly attached to deeper structures. Feline injection-site sarcomas are invasive and tend to recur after surgical excision. Subcutaneous administration of any substance that causes an exaggerated granulomatous inflammation can induce the development of sarcomas. 8 Histological examination of feline injection-site sarcomas reveals marked nuclear and cellular pleomorphism, high mitotic indices and areas of necrosis. 8
In the present case, the history of recurrences of cutaneous nodules over a a 3-year period after several surgical resections, in the absence of cutaneous dissemination of these lesions, led to the clinical suspicion of vaccinal-induced sarcoma and not of sporotrichosis, as in the latter most cats present with cutaneous ulcers in at least three regions of the body over a period of 1–128 months. 6
Atypical histopathological aspects led to the suspicion of malignant mesenchymal neoplasm, but the absence of mitosis or cytological atypias made this possibility less likely. On histopathological examination a mixed inflammatory infiltrate was observed in 87.8% of cats with sporotrichosis and a mononuclear infiltrate in 12.2% was observed. 7 In the present case the fact that S schenckii remained at a single site, without cutaneous dissemination, might be related to the presence of a chronic inflammatory infiltrate with few giant cells, which is common in canine and human sporotrichosis. 9 Differential diagnosis includes other conditions in which histopathological analysis presents granulomatous inflammation and atypical fibroblasts, such as nocardiosis, actinomycosis, atypical mycobacteriosis and foreign-body reaction. 10
Cats with sporotrichosis usually have numerous yeast-like structures upon histopathological analysis with PAS and Grocott’s silver stain,7,11 but in the present case only occasional yeast-like structures were observed.
Cytopathological analysis of the superficial secretions of skin lesions in cat sporotrichosis usually reveals a large number of yeast-like structures.12,13 However, in this case, cytology was negative.
At the first appearance of the cutaneous lesion, cytological analysis of the secretions from the lesion should have been performed, as well as fungal culture and histopathological examination of the lesion. These procedures were not performed in this case because the cat was not presented for veterinary care until 36 months after the appearance of the lesion.
Conclusions
These atypical clinical and histopathological signs of naturally-acquired feline sporotrichosis support the need for special histopathological techniques (PAS and Grocott) for the detection of the fungus and mycological culture in the diagnosis of sporotrichosis.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.