
Abstract
Conditions affecting the brachial plexus and its branches can cause lameness and/or neurological deficits. There are few reports of schwannomas in cats. In reported cases, the tumours arose from the dermis or subcutis of the limbs, head and neck and thorax, but there are no reports of primary tumours that arose from the brachial plexus itself. The purpose of this study is to present the clinical, radiological, ultrasonographical and pathological findings of primary brachial plexus tumour in three cats.
Conditions affecting the brachial plexus and its branches can cause lameness and/or neurological deficits. The most common location for peripheral nerve sheath tumours in dogs is the brachial plexus. 1
Tumours arising from other body organs invading, extending or metastasising to the brachial plexus have been reported infrequently in cats. Lymphosarcoma in the brachial plexus of a cat has been reported by Fox and Guntnick; 2 chondrosarcoma, which originated near the axillary area and infiltrated the brachial plexus, and ascended to the nerve roots and spinal cord was described by Shell et al; 3 and epidural lymphoma in a cat infected with feline leukaemia virus (FeLV) and leukaemic bone marrow that extended into the brachial plexus has been described by Spanchick et al. 4
There are few reports of schwannomas in cats.5 –8 In reported cases the tumours arose from the dermis or subcutis of the limbs, head and neck or thorax, but there are no reports of primary tumours arising from the brachial plexus itself. 8
Cats were identified retrospectively over a 5-year period (2006–2011). They were aged 7, 12 and 9 years at disease onset, and two males and one female were affected. The main clinical feature was the progressive disuse of one thoracic limb from weight-bearing lameness to non-weight-bearing lameness in two cats and to complete paralysis in one cat, over an average period of 7 months. Marked muscle atrophy over the scapula in the supraspinatus and infraspinatus groups was seen in the three cats, although other muscle groups were also involved in two cats. Obvious pain in the axillary area and on shoulder flexion and extension and a palpable lump in the axilla was present in two cats.
Amputation of the affected limb with removal of all involved spinal nerves at as proximal a level as possible was performed in two cats, as local resection of the neoplastic portion of the plexus was impossible.
The two cats who had the affected thoracic limb amputated were still alive at 42 and 55 months following the amputation. The third cat was euthanased on humane grounds.
Primary brachial plexus tumours in dogs arise from the Schwann cells or fibroblasts within the epineurium or endoneurium. 9 A variety of nomenclature has been assigned to these tumours, including neurofibromas, neurofibrosarcomas, schwannomas, neurolemmomas, neuronomas and perineural fibroblastomas. These primary tumours most commonly involve the spinal nerve roots in the caudal cervical and cranial thoracic spinal cord, and the nerves contributing to the brachial plexus.1,10 –13 Survey radiography, myelography, electromyography, computed tomography (CT), magnetic resonance imaging (MRI) and, more recently, ultrasonography are used to detect brachial plexus tumours.1,9,14 –17
The purpose of this study is to present the clinical, radiological, ultrasonographical and pathological findings of primary brachial plexus tumour in three cats.
Material and methods
A retrospective medical records search based on the diagnosis of primary plexus neoplasia in cats was carried out in all hospital records from 2006 and 2011. All cats were referred to, and treated by, the author.
Criteria for inclusion in the study
All cats admitted to the study must have had the diagnosis of brachial plexus schwannoma confirmed by histopathological examinations using both haematoxylin and eosin (H&E) and glial fibrillary acidic protein (GFAP) immunohistochemistry.
Criteria for exclusion from the study
All cats suffering from lameness, paresis or paralysis of one limb as a result of other conditions other than brachial plexus neoplasia, such as traumatic damage to the nerve roots contributing to the brachial plexus; spinal trauma; brachial plexus neuritis or neuropathy; secondary brachial plexus neoplasia, such as osteosarcoma, discospondylitis, intervertebral disc herniation, fibrocartilaginous embolism, granulomatous myelitis caused by feline infectious peritonitis and non-neoplastic (FeLV)-associated myelopathy; and from weakness caused by aortic thromboembolism. Arthritis of a fore limb joint may also produce a similar clinical pattern of progressive lameness, therefore, they were also excluded from the study.
Cats were examined at the hospital. Initially, they were seen weekly as the condition progressed, then every 3 months thereafter. The cats were examined clinically and blood was taken for routine haematological and biochemical testing. An indirect immunofluoresence test was used to detect FeLV antigen and feline coronavirus (veterinary laboratory). Plain radiography of the cervical and thoracic spine, affected thoracic limb, chest and abdomen was performed in each cat. Plain radiography of the chest and abdomen was repeated yearly to detect any tumour metastasis. Contrast radiography using 0.3 ml/kg iohexol (300 mg iodine/ml) (Omnipaque; Nycomed) and cerebrospinal fluid analysis were performed in two cats.
Ultrasonographical examination was performed in all three cats to visualise the brachial plexus from an axillary window, as described by Guilherme and Benigni, 17 using a high frequency 12 MHz linear transducer with a stand-off pad to place the nerve into the focal zone. Imaging was performed using B-mode real-time first and colour flow Dopplers to differentiate vessels from nerves. Cats were placed in dorsal recumbency with the affected thoracic limb abducted, and the transducer was positioned in the axilla lateral to the sternum with the ultrasound beam directed dorsally; the transducer was then rotated 90 degrees. Ultrasound-guided fine needle aspiration of the mass using a 22 G spinal needle, as described by Da Costa et al 18 was performed in all three cats. Ultrasonography of the abdomen and chest was carried out 4 weeks after the amputation and repeated monthly for 3 months, and then every 6 months thereafter in order to detect any tumour metastasis.
Exploratory surgery was carried out in two cats and a post-mortem examination was carried out in one cat. The neural tissue removed during surgical exploration and post-mortem was sent for histopathological examination, using both H&E and GFAP immunohistochemistry,19–21 to a specialist laboratory (FINN-laboratory).
Results
Case 1
A 7-year-old neutered male domestic shorthair cat was presented because of slowly progressive right thoracic limb lameness. There was no history of traumatic incident. The cat had been treated with meloxicam (Metacam; Boehringer), 0.1 mg/kg body weight PO q24h for 4 months, with no improvement.
Initial weight-bearing lameness of the limb progressed over a 6-month period to non-weight-bearing lameness. By the time of referral the cat was holding the affected limb completely off the ground. Abnormalities observed on physical examination consisted of severe atrophy of the axillary area and a palpable firm mass in the axillary area. Apart from the muscle atrophy the cat showed no evidence of other neurological deficits. Haemogram and blood biochemistries were normal. The cat was serologically negative for FeLV and coronavirus. Plain radiography of the right thoracic limb showed a well-defined circular radiodense mass in the region of the brachial plexus (Figure 1).

Lateral radiograph of the right thoracic limb of cat 1 showing a well-defined circular sclerotic mass (arrows) in the area of the brachial plexus
Contrast myelography of the cervical and cranial thoracic spine did not show any evidence of restriction or obstruction to the flow of the contrast material. Ultrasonographical examination of the axilla revealed a round, well-defined hyperechoic mass (4 × 5 cm) along the axis of the brachial plexus (Figure 2). Abdominal ultrasonography was unremarkable.

Longitudinal scan (cat 1) showing a well-defined echogenic circular mass (M) along the axis of the brachial plexus peripheral nerves (N), which appear as an echogenic tubular structure and an anechoic blood vessel below it (V)
Ultrasonographically-guided fine needle aspiration of the palpable mass was performed. Cytological examination of a direct smear of the aspirated material revealed a highly cellular pleiomorphic population of individual and clustered spindleoid cells. The cells contained basophilic, occasionally vaculated, cytoplasm. The nuclei were oval, with stippled chromatin. Multinucleation, as well as moderate anisokaryosis and anisocytosis were also observed. Occasionally, a small amount of eosinophilic extracellular matrix was found in association with cell clusters. A cytological diagnosis of a soft tissue sarcoma was made. Gross pathological examination of the mass during surgical exploration revealed a round circular mass arising from within the median, ulnar and radial nerves of the brachial plexus (Figure 3).

Gross pathological appearance of cat 1 showing the brachial plexus (N) and a round circular mass (M) arising from within the median, ulnar and radial nerves
Surgical removal of the mass proved impossible and fore quarter amputation with removal of spinal nerves C6–T1 as far proximal as was possible. Histological and immunohistochemical examinations of the mass were diagnostic of schwannoma (Figures 4 and 5).

Histological section of the brachial plexus mass of cat 1 stained with H&E (200×) showing a multilobulated tumour of a spindle cell origin. The neoplastic tissue was generally composed of plump spindleoid cells arranged in sheets, interlacing bundles and whorls. These cells have poorly defined cytoplasmic borders and abundant fibrillar to vaculated cytoplasm. The nuclei are oval, with stippled chromatin. In most areas there is only mild atypia and infrequent mitosis. A moderate amount of loose fibrillar stromal material is present. There is moderate multifocal necrosis of the neoplastic tissue

Immunochemistry of the mass glial fibrillary acidic protein (GFAP) (400×) shows intense immunoreactivity. There is strong positive cytoplasmic staining of the neoplastic cell population
The cat was still alive and remained free of any neurological deficits for 42 months following surgical amputation of the affected limb. There were no signs of metastasis on repeated radiographic or ultrasonographical examinations.
Case 2
A 12-year-old, neutered female Burmese cat was referred because of a slowly developing ataxia and paralysis of the left fore thoracic limb. The cat had been treated with meloxicam (Metacam; Boehringer) 0.3/mg/kg body weight PO q24h for 13 weeks with no improvement.
Initial weight-bearing lameness of the affected left thoracic limb progressed over a 9-month period to non-weight-bearing lameness that was followed by paralysis of the limb. Abnormalities on physical examination consisted of marked left shoulder muscle atrophy of the spinatus muscle group over the scapula, a palpable left axillary mass and axillary pain. Neurological examination abnormalities consisted of left-sided Horner’s syndrome. The cat had completely lost the use of the left thoracic limb and knuckled over the foot when walking. Spinal reflexes (triceps and biceps tendon reflexes, extensor carpi radialis muscle reflex and withdrawal reflex), conscious proprioception and postural reaction (hopping and wheel barrowing) were absent and deep pain stimuli was absent in the affected left thoracic limb. The left pelvic limb had a delayed conscious proprioception and an exaggerated patellar reflex. The rest of the neurological examinations were normal.
Blood analysis was unremarkable and the cat was serologically negative for FeLV and coronavirus. Plain radiography revealed no abnormalities and abdominal ultrasonography was unremarkable.
Ultrasonographical examination of the axilla showed an ill-defined hypoechoic mass (3 × 4 cm) along the axis of the brachial plexus (Figure 6). Cytological examination of a smear of the ultrsonographically-guided fine needle aspirate of the mass revealed the same cytological features as mentioned for cat 1. The cytological diagnosis was a sarcoma.

Longitudinal scan (cat 2) showing an ill-defined hypoechogenic mass (M), which has developed along the axis of the brachial plexus (N) and the anechoic blood vessel below it (V)
Left hind limb involvement, which became apparent 6 weeks prior to presentation, raised suspicion of extension of the schwannoma to the spinal cord.
Therefore, a guarded prognosis was given to the owner, who rejected the performance of contrast myelography and requested euthanasia, but gave permission for a post-mortem examination. Post-mortem findings were a soft, haemorrhagic, oedematous and cystic mass arising from within the brachial plexus (Figure 7).
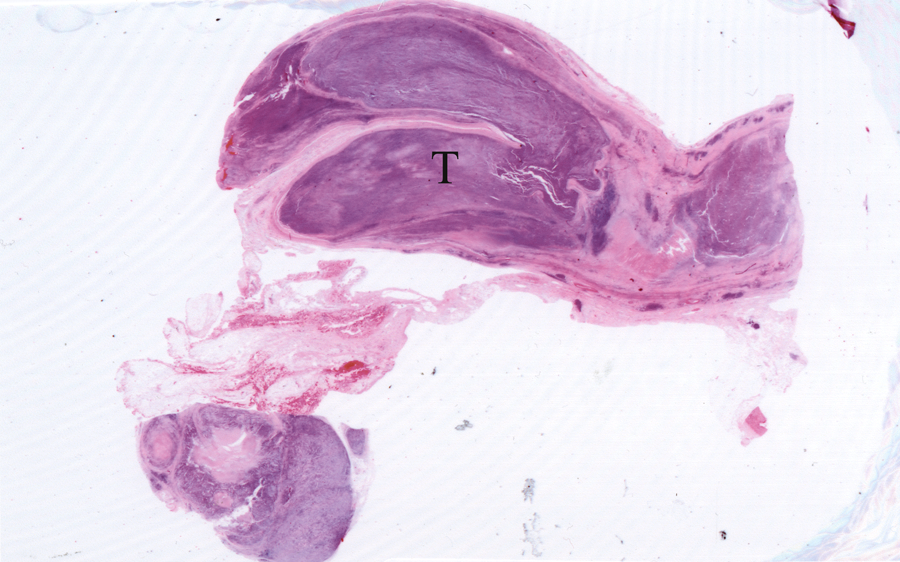
Section of the brachial mass of cat 2 using H&E (10 ×) showing a soft, haemorrhagic, cystic tubular mass (T)
A round mass was present on the left side of the spinal cord at the level C6/C7 (Figure 8). The tumour was growing along C6 and C7 nerve roots and severely compressing the adjacent part of the spine.

Gross appearance of a spinal mass, the cervical spine and C6 and C7 nerve roots. This post-mortem specimen of the spine of cat 2 shows the tumour, a schwanomma (T), the adjacent part of the spine (N) and C6 /C7 nerve roots (NR). Note that the tumour is growing along the nerve roots and severely compressing the adjacent part of the spine
Histological and immunohistochemical examinations of the masses were diagnostic of schwannoma.
Case 3
A 9-year-old male neutered Persian cat was referred because of chronic intractable left thoracic limb lameness for 8 months prior to presentation.
The cat was treated with meloxicam (Metacam; Boehringer), 0.1 mg/kg body weight PO q24h for 16 weeks, with no improvement, seen in as cats 1 and 2. There was marked muscle atrophy of the entire affected limb, particularly in the supraspinatus and infraspinatus muscle groups. The cat was putting very little weight on the affected limb. There was pain on manipulation of the affected limb, but this could not be localised to any specific joint. No mass could be palpated in the axillary area.
Blood analysis was unremarkable and the cat was serologically negative for FeLV and coronavirus. Apart from muscle atrophy the cat showed no evidence of other neurological deficits. Plain radiography of the cervical and cranial thoracic spine, the affected leg, the axillary area, the thorax and abdomen revealed no abnormalities. Myelographical studies of the cervical and cranial thoracic revealed no abnormalities. Ultrasonographical examination revealed an hypoechoic, ill-defined elongated tubular mass (1 × 4 cm) has developed along the axis of the brachial plexus (Figure 9).

Longitudinal scan of the brachial plexus of cat 3 showing a hypoechoic, ill-defined elongated mass (T) along the brachial plexus (N)
Ultrasonographically-guided fine needle aspiration failed to make a diagnosis.
Gross pathological examination of the brachial plexus during left thoracic limb amputation revealed a primary neural mass arising from within the brachial plexus and running along the median ulnar, radial and musculocutaneus peripheral nerves (Figure 10).

Post-mortem specimen of the amputated limb of cat 3 showing a primary neural tumour (T) arising from within the brachial plexus and running along the median, ulnar, radial and musculocutaneous peripheral nerves of the brachial plexus. The nerves are shown in the following order: 1 suprascapular nerve; 2 subscapular nerve; 3 axillary nerve; 4 thoracodorsal nerve; 5 lateral thoracic nerve; 6 median-ulnar nerve (median and ulnar common trunk); 7 median nerve; 8 ulnar nerve; 9 radial nerve; 10 musculocutaneus nerve
The mass appeared soft, cystic, haemorrhagic and oedematous. Histological and immunohistochemical examination of the mass following amputation of the affected limb was diagnostic for schwannoma. The cat was still free of any neurological deficits 55 months following amputation of the affected limb and there were no signs of metastasis on repeated radiographic or ultrasonographical examinations.
Discussion
The slow development of progressive disuse of a limb from weight-bearing lameness to non-weight-bearing lameness or paralysis, and atrophy with or without hyperaesthesia, are typical of a gradually developing lesion affecting peripheral or cranial nerves.8,22 In two cats, physical examinations following amputation of the affected limb did not show signs of pain or neurological deficits in any of the remaining three limbs, which ruled unlikely proximal extension of the tumour to the spinal cord. There were also no signs of metastasis to other body organs on repeated radiographic or ultrasonographical examinations. These findings agree with the reported description of schwannomas in the literature by Bradley et al, 10 who stated that ‘schwannomas of the brachial plexus nerves are usually benign, in a small number of cases, they extend to the spine and do not metastasis, therefore, amputation of the affected limb with removal of the affected spinal nerves as high as possible is likely to be curative’.
The diagnosis of brachial plexus neoplasia in my study relied on collection of information from survey radiographs, myelography, ultrasonography, ultrasound-guided fine needle aspiration, histopathological examinations of samples stained with H&E and GFAP immunohistochemistry.
In the three cats described in this study, plain radiography was not of great diagnostic value, except in cat 1, when the tumour was large, solid and sclerotic, making it visible in plain radiographs.
Ultrasonography is a useful procedure in the diagnosis of brachial plexus neoplasia in dogs.18,23,24 In this cat study, similar variable ultrasonographical features were noted. In cat 1 they were hyperechogenic, while in cats 2 and 3 they were hypoechoic. This may be because the tumours in cats 2 and 3 were soft, fluctuant and cystic in nature owing to large areas of necrosis, haemorrhage, oedema and cavitation; the tumour in cat 1 was solid. Despite the positive finding of a mass on ultrasonography in cat 3, no mass could be palpated in the axillary area; therefore, one should not rely on palpating a mass to diagnose brachial plexus neoplasia. Also, failure to detect the mass using ultrasound because of the size or the location or the shape of the tumour does not eliminate the possibility of a brachial plexus tumour and additional imaging using CT or MRI is indicated if clinical suspicion remains. 9
High-resolution ultrasonography has many advantages over MRI for examination of the brachial plexus. For example, ultrasound is less time consuming, anaesthesia is not required and it offers higher spatial resolution than MRI. It also enables a study in which changes in direction of the nerve can be followed with the transducer, whereas additional acquisition of MR images in different planes may be necessary for optimal visualisation. 25
For these reasons ultrasonography may be performed before MRI in patients with suspected brachial plexus tumour. If ultrasonographical examination is negative MRI can be used. MRI is commonly used to look for lesions in the vertebral canal and may have been helpful in cat 2 in screening the spinal canal when myelography was rejected.
Ultrasound-guided fine needle aspiration from the masses in cats 1 and 2 was suggestive of schwannoma, while samples taken from cat 3 failed to make a diagnosis. A false-negative result of Ultrasound-guided fine needle aspiration in cat 3 could be a result of the shape, position and thickness of the mass, as it was running thinly and too closely along the nerves to obtain sufficient samples to make a diagnosis. Therefore, one should not use this technique as a single diagnostic tool but rather as a complement to other diagnostic tools.
It is important to differentiate primary brachial plexus tumours from secondary brachial plexus tumours because primary plexus tumours, such as schwannomas, originate in the brachial plexus nerves. However, secondary brachial plexus tumours, such as lymphosarcomas, osteosarcomas, chondrosarcomas, fibrosarcomas, haemangiosarcomas and haemangiomas, originate outside the nerve and cause neurological signs by infiltration, compression or metastasis. Secondary brachial plexus tumours appear to be larger than primary brachial plexus tumors and usually encompass large sections of the brachial plexus, making them likely to metastasis to other organs; therefore, they carry worse prognosis. 1 Cytological description of brachial plexus neoplasias are scant within the veterinary literature. 26
The three cats presented in this study exhibited cytological features similar to those described in the literature.19,26,27 Both fine needle aspiration samples and the masses that were removed surgically or at post mortem yielded a predominance of multilobulated spindeloid cells arranged in sheets. Diagnosis of schwannoma is not possible on the basis of cytology alone of samples stained with H&E. However, the additional immunohistochemical evaluation of the tumour for GFAP, which gave a strong positive result, allowed a definite conclusive diagnosis of schwannoma to be made.23,24
Conclusions
Tumours of the brachial plexus are difficult to diagnose. Clinically, most cats present with chronic progressive thoracic limb lameness, indistinguishable from musculoskeletal lameness. The diagnosis of brachial plexus neoplasia has evolved over time from survey radiographs, myelography and surgical exploration of the brachial plexus to CT and, more recently, ultrasonography and MRI.9,10 Some of these diagnostic methods are either expensive or invasive, and others are not widely available to practitioners, thereby delaying the diagnosis of brachial plexus neoplasia.
Widely available ultrasonography, ultrasound-guided fine needle aspiration followed by histopathological examination of samples stained with H&E and GFAP immunohistochemistry of the neural tissue (removed surgically or at post mortem examination) allowed the diagnosis of primary brachial plexus schwannoma in the three cats included in this study. This diagnostic protocol provided early detection of brachial plexus neoplasia in two cats before the tumour spread to the spinal cord, which potentially, and positively, influenced the survival of these two cats.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The author does not have any potential conflicts of interest to declare.