
Abstract
A 2-month-old, intact, female domestic shorthair kitten presented with a history of acute-onset dyspnoea. Severe dyspnoea and tachypnoea were noted on physical examination. Serosanguinous fluid, consistent with a modified transudate, was aspirated from the pleural cavity immediately after the physical examination, with an immediate decrease in respiratory rate and effort. The thorax was radiographed and the entire left hemithorax appeared to be filled with a large soft tissue density mass. Thoracic ultrasound was performed and a cystic structure, measuring 3.0 cm × 1.5 cm, was seen in the left hemithorax. An explorative thoracotomy was performed and a mass obliterating the left hemithorax was found. The mass was removed by a combination of blunt and sharp dissection. A final diagnosis of thoracic pseudocyst was made on histological examination of the tissue. The mass was described as a sterile process characteristic of an organised seroma or haematoma. Recovery from surgery was uneventful and the kitten was discharged 48 h postoperatively. The kitten was still alive with no recurrence of clinical signs at the time of writing this report, 8 months postoperatively.
Case Report
A 2-month-old, intact, female domestic shorthair kitten, weighing 0.8 kg, was presented to the Veterinary Teaching Hospital with a history of acute onset dyspnoea. The kitten had been in the possession of the owners for 5 weeks and during this time her behaviour was considered to be normal. Severe dyspnoea and tachypnoea (80 respirations/min) were noted on physical examination, and the heart and lung sounds were muffled on auscultation of the left hemithorax. The skin over the left side of the chest was clipped and prepared for an aseptic procedure and 125 ml of serosanguinous fluid was aspirated from the left hemithorax. There was an immediate decrease in respiratory rate and effort with concurrent clinical improvement once the chest was drained. The packed cell volume of the fluid aspirated from the chest was 2% and the total solids were 4.8 mg/dl. There was a low cellularity of predominantly pyknotic neutrophils, and occasional erythrocytes and lymphocytes on a direct smear of the fluid.
Complete blood count and blood glucose were performed. A mildly elevated white blood cell count (25 × 109/l; range 5.5–19.5 × 109/l), normal haematocrit (24.2%; range 24–45%) with haemoglobin of 7.7 g/dl, (range 8–15g/dl) and mild hyperglycaemia (186 mg/dl; range 80–150 mg/dl) were found. The blood smear showed a mild neutrophilia with no toxic changes. Treatment with ampicillin (Penibrin; Sandoz), 25 mg/kg IV q12h was initiated and the kitten was hospitalised in an oxygen-supplemented cage.
A single, 3.0 cm × 1.5 cm, soft tissue density mass, obliterating the left hemithorax and causing mediastinal shift to the right, was seen on chest radiographs (Figure 1a, b). Ultrasound of the chest was performed to further characterize the mass and an echogenic capsule surrounding anechoic fluid was seen. The mass was consistent with a cystic structure and it occupied the entire left hemithorax (Figure 2). Thoracic ultrasound was repeated 3 h later owing to recurrence of dyspnoea and an increased volume of the cyst was evident.

Right lateral (a) and ventrodorsal (b) radiographic views of the thorax. The entire left hemithorax is filled with a soft tissue density mass (narrow arrows). The mediastinum is shifted to the right hemithorax (the displaced trachea and main-stem bronchi are marked by the wide arrows)
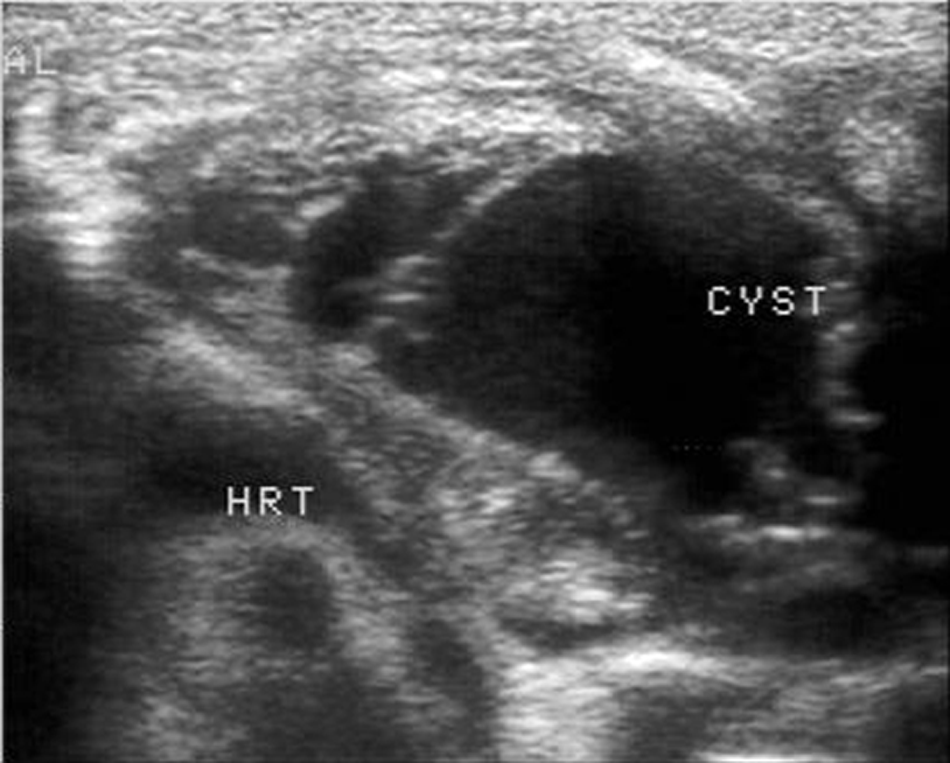
Ultrasonographic image of the left hemithorax showing a cystic structure with a thin-walled echogenic capsule filled with anechoic fluid
Explorative surgery was recommended. The kitten was premedicated with 0.1 mg/kg morphine (Morphine HCl; Teva), and 0.04 mg/kg acepromazine (PromAce; Fort Dodge) subcutaneously. It was induced with intravenous propofol (Lipuro; B-Braun), 1.25 mg/kg, intubated and maintained on isoflurane (Isoflurane; Nicolas piramal) in oxygen. Ampicillin (25 mg/kg) (Penibrin; Sandoz) was administered intravenously 10 mins prior to the skin incision and every 2 h during surgery.
An explorative thoracotomy was performed via a median sternotomy. The entire length of the sternum was incised on the midline using an osteotome and bone-cutting forceps. Once the chest was open, the mass within the left hemithorax was seen. The mass extended from, and was adhered to, the diaphragm caudally, the cupula pleura cranially, the parietal pleura laterally, and the visceral pleura of the left lung lobes and pericardium medially. The mass was removed by a combination of blunt and sharp dissection (Figure 3a, b). Once the mass was removed, the normal anatomy of the left hemithorax could be seen. The left lung lobes were compressed, but intact, and a possible origin of the cyst could not be identified. The chest was closed, after placing a transdiaphragmatic chest tube, by pre-placing 2/0 nylon suture around the sternebra in a cruciate pattern. A ‘soaker’ catheter (Contiplex D; B-Braun) was placed ventral to the sternum to enable the administration of local analgesics postoperatively.

(a) Intraoperative photograph. The cyst within the left hemithorax is marked with a black arrow and the heart is marked with a white arrow. The cat is in dorsal recumbency and points of reference are given within the photo (cranial, caudal, left and right). (b) Post-excision cystic mass. Dimensions compared to 1 ml syringe
Postoperative analgesia included morphine (Morphine HCl; Teva), 0.1 mg/kg, administered subcutaneously q6h, and local infiltration of bupivacaine HCl 0.5% (Kamacaine; Kamada) 0.3 mg/kg, q6h via the ‘soaker’ catheter. Recovery was uneventful and the chest tube was removed 12 h postoperatively. The kitten was discharged the following day with amoxicillin (Moxipen; Teva) 25 mg/kg, PO, q12h for 7 days and meloxicam (Metacam; Boehringer Ingelheim Pharma), 0.1 mg/kg q24h for 3 days and then 0.025 mg/kg every 3 days for an additional two treatments.
Histopathology was performed on the tissue removed from the thorax (Figure 4). Representative specimens of tissue removed intraoperatively were fixed in 10% neutral buffered formalin. The fixed samples were processed routinely, embedded in paraffin, trimmed at 5 μm and stained with haematoxylin and eosin. The slides were examined by an American College of Veterinary Pathologists-certified pathologist. The lesion consisted of a lumen filled with fibrin, red blood cells and a small amount of cellular debris surrounded by a 1–3 mm-thick capsule of granulation tissue. The granulation tissue was loose and composed of active fibroblasts and newly formed capillaries within abundant amphophilic extracellular matrix. In the capsule there was mild multifocal lymphoplasmacytic and occasionally neutrophilic infiltration. There were several clusters of siderophages. On the inner aspect of the capsule there was multifocal proliferation and extension of fibroblasts into the haemorrhagic and proteinaceous material, typical of organisation. In several areas the external aspect of the capsule was continuous with bundles of striated muscle, thought to originate from the chest wall. Focally there was proliferation of a small amount of irregular woven bone, presumably in an area where the capsule was apposed to a rib. Infectious agents or neoplastic cells were not detected. The histologic features were those of a sterile process, most likely an organised seroma or haematoma. The lesion may also be referred to as a pseudocyst, ie, an abnormal or dilated cavity resembling a true cyst but not lined with epithelium (cyst lacking epithelial or endothelial lining, called also adventitious or false cyst). 1
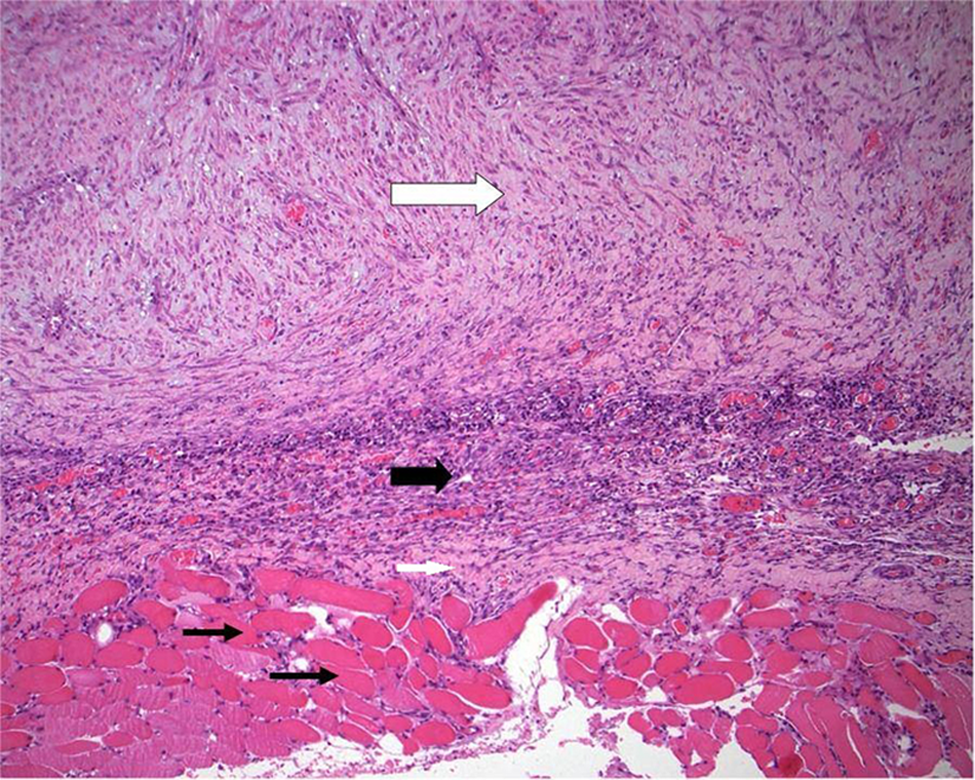
Histopathology of the mass removed from the thorax (magnification ×10). The most external layer is striated muscle (thin black arrows), followed by the pleura (thin white arrow), a layer of fibrous tissue infiltrated by a moderate number of macrophages, plasma cells and neutrophils (thick black arrow), and, most internally, a thick layer of granulation tissue (thick white arrow). The lumen, not seen in this image, is above the granulation tissue
At follow-up examination, 10 days after surgery, the kitten was clinically normal. The owner reported a return to usual activity and appetite, without any signs of dyspnoea. The kitten was followed up, via telephone, 8 months after surgery and the owner reported that she was growing normally with no recurrence of the clinical signs.
Thoracic cysts can be divided by location into mediastinal cysts and pleural cysts, with the majority of cysts occurring in the mediastinum. 2 The tissue of origin varies between cases and can be identified definitively upon histologic examination of the cyst.2,3 Thymic branchial cyst, parathyroid cyst, cystic thymoma, thymic cyst, thyroglossal duct cyst, pleural cyst and idiopathic cysts have been reported.3,4 Other cyst-like thoracic or mediastinal lesions that have been reported in cats include chest granuloma, abscess, lymphosarcoma, lymphangioma, ectopic thyroid carcinoma and mesothelioma.5–10 Cysts are usually lined by epithelium and surrounded by a stromal capsule. 11 Congenital or acquired cystic lesions of the thorax affecting kittens have not yet been reported.
To the authors’ knowledge, this case report is the first report of a thoracic pseudocyst in a kitten. Cystic fluid is usually clear, colourless, and low in protein and cellular content. 11 The fluid aspirated from this pseudocyst had high total solids, which is inconsistent with the aforementioned; however, a definitive diagnosis was based on the histological findings. Culture and sensitivity of the fluid aspirated from the cyst was not performed as there was no evidence of an infectious process in the aspirated fluid or on histology of the pseudocyst.
Treatment of thoracic cysts in asymptomatic patients is controversial because benign lesions are not readily distinguishable from malignant lesions based on imaging alone. It has been suggested that treatment may not be required in patients without clinical signs.3,4 Excision of accumulative thoracic cysts or lesions causing clinical signs, such as was seen in this case, is recommended, however. In this kitten, draining the fluid within the cyst improved the clinical signs, but did not provide relief for more than a few hours. A surgical solution was sought and appears to have been curative. Prognosis depends on the primary cause of the lesion, which, in this case, is good owing to the benign nature of the lesion.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.