
Abstract
Clinical summary:
A 4-month-old female intact domestic shorthair cat presented to Kansas State University Veterinary Medical Teaching Hospital for investigation of a large, firmly adhered mass in the left mid-cervical region that developed after phlebotomy performed at the referring veterinarian’s clinic. Ultrasound examination of the mass revealed a cystic structure in communication with the left carotid artery, with bidirectional blood flow through the area. A diagnosis of pseudoaneurysm secondary to accidental needle penetration of the carotid artery during jugular venepuncture was made.
Outcome:
Strict cage rest and pain management resulted in complete resolution of clinical and ultrasonographic signs in this cat.
Clinical report
A 4-month-old female intact domestic shorthair cat presented to the referring veterinarian for routine ovariohysterectomy. During phlebotomy for pre-surgical blood work, the cat vocalized, collapsed and defecated, but appeared normal 30 mins later. A large mass in the region of the venepuncture site was subsequently noticed. Complete blood count results were within normal limits (hematocrit 35%); however, the surgery was cancelled and the cat was sent home for observation. The owners observed three or four additional episodes of vocalization, neck extension and apparent pain. Repeat blood work 4 days later showed anemia (hematocrit 17%).
On physical examination at presentation to the authors’ clinic the following day, the patient had pale mucous membranes and a large, firm mass in the left mid-cervical region extending towards the midline (Figure 1). There was no palpable thrill and no turbulent blood flow was heard on auscultation of the mass. Differentials at this time included hematoma, abscess, lymphadenopathy, congenital anomaly and neoplasia. Review of the blood smear taken when the packed cell volume (PCV) was 17% suggested the anemia was regenerative.

Mass in the left mid-cervical region (arrow)
As trauma to the area was suspected and the origin of the mass was unknown, a cervical ultrasound examination was performed. This revealed a layered, mixed echogenic area of approximately 2 cm thickness in the left mid-cervical region. This area was moderately vascular. Deep to this area was an irregularly round (on both transverse and longitudinal scan planes of the neck), thick-walled anechoic/cystic lesion measuring 2 cm in diameter (Figure 2). Differentials for this anechoic lesion included hematoma, aneurysm and pseudoaneurysm. The layered mixed echogenicity superficial to the anechoic lesion was compatible with the variable echogenicity of a hematoma. Other differentials for this area included fibrous or inflammatory tissue. The anechoic mass was adjacent to the carotid artery.

Longitudinal image of the left carotid artery (arrow), showing a cystic structure superficial to the carotid artery (PA). There is a large area of mixed echogenicity surrounding the cystic structure (HM). PA = pseudoaneurysm, HM = hematoma
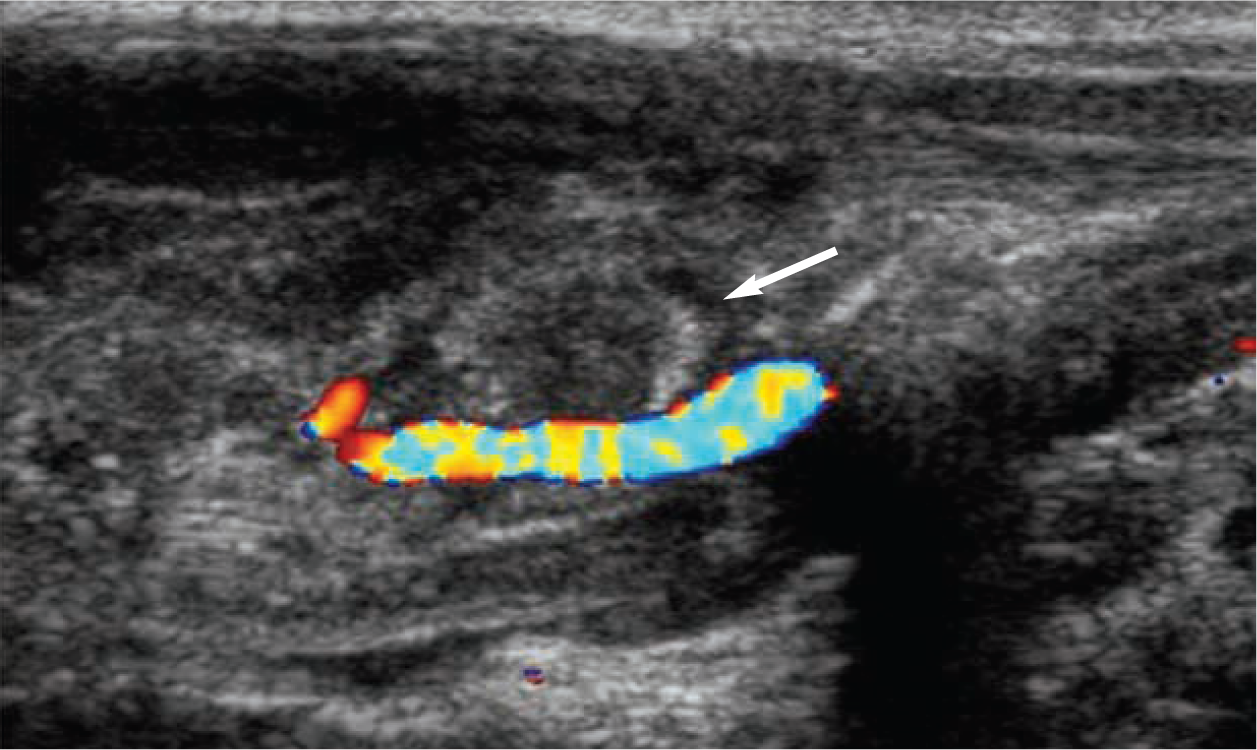
Color Doppler ultrasonography revealed that the carotid artery was adjacent to and also intimately associated with the round anechoic structure, and demonstrated a swirling arterial blood flow pattern (Figure 3). This is referred to as the ‘yin–yang’ sign and is indicative of bidirectional flow within the lesion, resembling its namesake.

Using Doppler ultrasound it could be determined that the cystic structure was in communication with the carotid. There is circular or bidirectional flow of blood into the pseudoaneurysm, referred to as the yin yang sign
These findings were consistent with a pseudoaneurysm resulting from suspected trauma of the carotid artery during attempted jugular venepuncture.
Due to financial constraints, the patient was sent home on buprenorphine, 0.02 mg/kg PO q8h, and exercise restriction to prevent further trauma to the area. The PCV was re-checked by the referring veterinarian 4 days later and was 32%.
At a subsequent re-check examination, 2 weeks after initial presentation to the authors, the cervical mass was substantially decreased in size. There was, however, miosis of the left pupil, elevation of the third eyelid on the left and ptosis of the left eye, consistent with Horner’s syndrome, which responded partially to phenylephrine treatment. Although these signs were suspected to be related to the presence of the cervical mass, as both were lateralized to the left, this could not be definitively determined as the signs were not present on initial presentation.
On ultrasound examination at this time, the pseudoaneurysm had decreased in size to 1 cm. There was a small amount of arterial flow in the area where the ‘neck’ (arterial wall defect) was most likely present. The carotid artery could still be visualized coursing medially. The superficial soft tissue thickening previously thought to be an extravascular hematoma had almost completely resolved. There was only a trace amount of flow into the pseudoaneurysm, which was now echogenic and characteristic of a hematoma or clot formation (Figure 4).
Doppler image obtained at the time of the 2-week re-check. There is only a small amount of flow into the pseudoaneurysm, which is now filled with a clot or hematoma (arrow)
Discussion
An aneurysm can be classified as a true aneurysm or a false aneurysm (pseudoaneurysm or communicating hematoma). True aneurysms are focal or diffuse dilations to greater than 50% of the original vessel diameter, with thinning of the vessel wall; they usually arise as a result of an acquired or congenital weakness in the wall, with all wall layers (intima, media and adventitia) remaining intact. 1 False aneurysms are dilations in the vessel wall where all of the wall layers are not intact. The defect (referred to as the neck) lies in the tunica intima and media, with adventitia or encapsulated hematoma being the outermost layer. The hematoma is in communication with the vessel itself, causing turbulent blood flow through the area.1,2
Doppler ultrasound is the most widely used non-invasive imaging modality for the diagnosis of pseudoaneurysm. Classic findings with color Doppler imaging of pseudoaneurysms are the swirling flow of blood, referred to as the yin–yang sign, and ‘to-and-fro’ flow. To-and-fro flow represents blood entering and leaving through the neck of the pseudoaneurysm during each cardiac cycle.3,4 This flow pattern was not appreciated during the initial diagnosis of this pseudoaneurysm.
In this case, the anemia was thought to be secondary to acute bleeding into the surrounding tissues when the carotid was penetrated. The Horner’s syndrome was likely secondary to trauma to the sympathetic trunk as it coursed through the mid-cervical region.
In man, the most common etiology of carotid artery pseudoaneurysm is penetrating or blunt neck trauma. Pseudoaneurysm formation secondary to arterial catheterization is also common.5,6 Urgent treatment is necessary in humans to prevent rupture, microemboli formation, pain, neuropathies or local skin ischemia. 2 The urgency of treatment in small companion animals is uncertain as there are so few documented case reports.
In humans, various treatment options are reported including thrombin injection, use of stents, coils, ultrasound-guided compression repair, and surgery, with thrombin injection being the most commonly performed and the most successful.7–9
Two cases of pseudoaneurysm have been reported in the small animal literature. The first was a pseudoaneurysm of the celiac artery in a 10-month-old dog, caused by a migrating grass awn. Diagnosis in this case was made with ultrasound and abdominal computed tomography. The dog was deemed an unsuitable surgical candidate and died the next day. Necropsy showed hemoabdomen from pseudoaneurysm rupture, with a grass awn at the central portion of the lesion. 10 The second report involved an 8-year-old Maine Coon cat which developed a radial artery pseudoaneurysm after a suspected cat bite. Ultrasonography and angiography was used for diagnosis, and surgical correction was performed, producing complete resolution of clinical signs. 11
Pseudoaneurysmal formation secondary to a femoral blood draw in a macaque and a case of an idiopathic pseudoaneurysm in a sheep have also been reported.12,13
Conclusion
Pseudoaneurysm formation in this cat was strongly suspected to be traumatic in origin secondary to attempted jugular venepuncture for pre-surgical blood work. The needle likely penetrated the carotid instead of the jugular, causing disruption of the vessel wall, hematoma and pseudoaneurysm formation.
One month after presentation to the authors, the referring veterinarian reported that the Horner’s signs had resolved, the mass was barely palpable, and the cat had exhibited no additional painful episodes. In this case, time and strict exercise restriction with pain management resulted in closure of the pseudoaneurysm via clot formation, without any adjunctive therapy.
Footnotes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this case report.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.
Date accepted: 1 August 2012