
Abstract
A 3.5-year-old male neutered cat was presented for investigation of renomegaly appreciated during a routine physical examination. Marked renomegaly due to bilateral hydronephrosis was detected and further testing identified International Renal Interest Society stage 2, non-hypertensive, non-proteinuric chronic kidney disease. Ten months later the cat was evaluated for acute lethargy; severe azotemia with oliguria was documented. Medical therapy failed to result in clinical improvement and the cat was euthanased. Necropsy revealed bilateral marked hydronephrosis secondary to a tortuous proximal ureter consistent with proximal ureteropelvic junction stenosis. This is the first report of this disorder leading to progressive renal failure in a cat.
Case Report
A 3.5-year-old castrated male domestic shorthair cat was presented to the University of Wisconsin Veterinary Medical Teaching Hospital (UW-VMTH) for investigation of asymptomatic renomegaly. One month earlier, the referring veterinarian appreciated bilateral renomegaly during an annual wellness examination. The owners reported the cat to be apparently healthy with no change in thirst, urine volume, appetite or body weight. A biochemistry panel, complete blood count and urinalysis were performed by the referring veterinarian when renomegaly was appreciated. The results indicated mild azotemia with a creatinine of 2.8 mg/dl [reference interval (RI) 0.8–2.3 mg/dl] and blood urea nitrogen (BUN) of 40 mg/dl (RI 15/34 mg/dl). A mild increase in alanine transferase activity was also present at 145 U/l (RI 28–100 U/l). The complete blood count was within normal limits. Urine was dilute within the range of minimal concentration (specific gravity 1.019) with an inactive sediment. No urine culture was performed. The urine protein:creatinine was normal at 0.1 (RI <0.4).
On physical examination at the UW-VMTH the cat was in good body condition [body condition score (BCS) 6/9], with normal hydration and vital parameters. Bilateral renomegaly was palpable, with the left kidney larger than the right. Both kidneys were smooth and non-painful. Doppler systolic blood pressure was found to be normal at 110 mmHg. Urine was obtained via cystocentesis for aerobic culture, which produced no growth of bacteria. Urinalysis confirmed the presence of minimally concentrated urine (specific gravity of 1.017). An abdominal ultrasound confirmed bilateral renomegaly. The left kidney was markedly enlarged (long axis measurement 6.68 cm) with a dilated pelvis and calices (Figure 1); almost no cortical or medullary structures were present. The proximal left ureter was dilated (0.55 cm) at the insertion to the renal pelvis, but could not be traced distally. The right kidney was also enlarged (5.2 cm) with dilated pelvis and calices. There was more cortical tissue present than in the left kidney and the right ureter was not dilated.
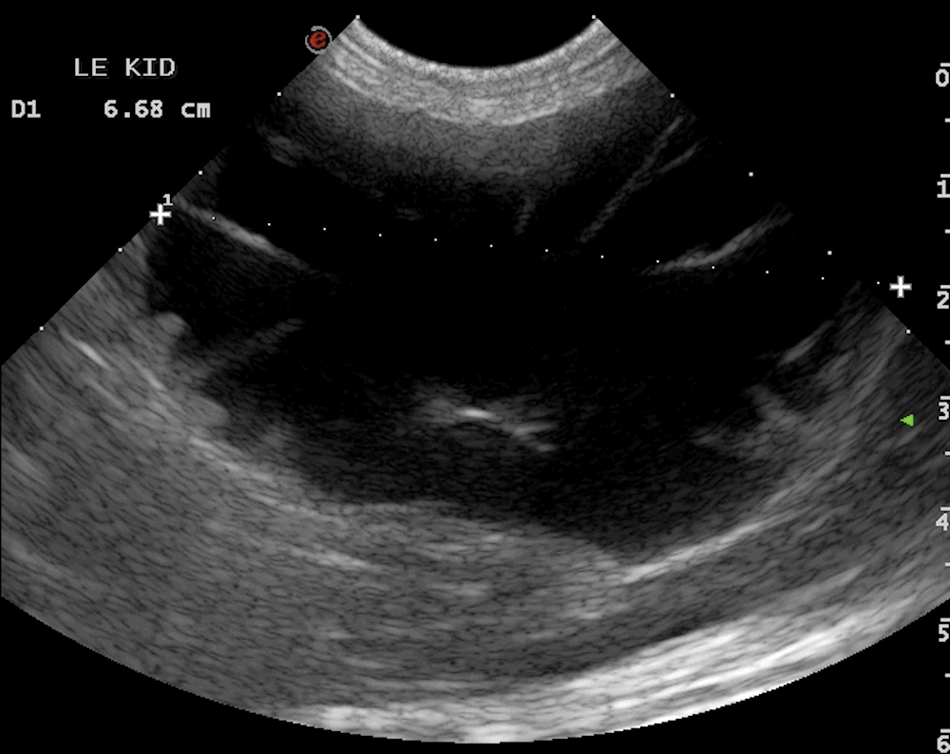
Ultrasound appearance of left kidney at time of initial presentation. Renomegaly with severe hydronephrosis and calyceal dilation is present. Minimal renal cortical tissue remains
The cat was diagnosed with International Renal Interest Society (IRIS) stage 2AQ2: Please confirm whether it should be IRIS stage II or IRIS stage 2 and update the text and abstract as necessary for consistency. chronic kidney disease (non-hypertensive, non-proteinuric) with bilateral hydronephrosis. The hydronephrosis was suspected to have occurred secondary to a congenital malformation, as the cat had displayed no previous illness suggestive of ureteral obstruction. Dietary phosphorus and protein restriction was started (Royal Canin Renal LP). Bloodwork was monitored every few months for progression of azotemia. Nine months later the azotemia had not yet progressed: creatinine was 2.1 mg/dl (RI 0.8–2.3 mg/dl) and BUN was 46 mg/dl (RI 15–34 mg/dl). The increased alanine aminotransferase activity had resolved.
The cat was again presented approximately 10 months after the initial visit for evaluation of acute lethargy, anorexia and abdominal distention noted by the owners. On physical examination, the cat was still in good body condition (BCS 7/9) and had normal vital parameters. Marked renomegaly and a small bladder were appreciated on abdominal palpation. Hematology showed a mild normocytic hypochromic anemia of 29% (RI 31–48%) and a mild leukocytosis of 14.03 × 103/μl (RI 3.4–13.5 × 103/μl) due to a mild neutrophilia of 12.07 × 103/μl (RI 1.5–9.6 × 103/μl). Marked azotemia was now present with a creatinine of 8.2 mg/dl and a BUN of 113 mg/dl, with a mild hyperglobulinemia of 4.3 g/dl (RI 2.3–3.8 g/dl). A clinical diagnosis of acute kidney injury on a background of chronic kidney disease was made and the cat was admitted to the hospital for further diagnostics and treatment.
The cat was hospitalized for 3 days. Intravenous (IV) fluid therapy, famotidine (0.5 mg/kg IV q12h), maropitant (1 mg/kg SQ q24h) and buprenorphine (0.025 mg/kg IV q8h) were administered throughout hospitalization. Empiric antibiotic therapy [ampicillin/sulbactam (Unasyn; Pfizer) 22 mg/kg IV q8h] was initiated to treat for possible pyelonephritis while awaiting urine culture results. A urethral catheter and closed collection system was placed to monitor urine output. Despite a bolus of IV crystalloids and a maintenance fluid rate calculated to replace 6% dehydration of body water over 12 h, the cat was oliguric, with urine production not exceeding 1.6 ml/kg/h. Mannitol (0.5 g/kg IV) was administered, resulting in an initial transient increase in urine production to 3 ml/kg/h; however, this response was not sustained with repeat mannitol administration. IV furosemide was administered as a 2 mg/kg bolus, followed by a 0.5 mg/kg/h constant rate infusion. After furosemide administration the cat’s urine production increased to 3 ml/kg/h.
Abdominal radiographs showed marked bilateral renomegaly (Figure 2) with no ureteroliths identified. Abdominal ultrasound demonstrated progressive renomegaly due to hydronephrosis. The left kidney had increased in size to 9.78 cm with minimal cortex present. The right kidney had increased in size to 7.93 cm and now also had a loss of cortical tissue, which was less advanced compared with the left kidney. Neither ureter was dilated. A urine culture obtained at the time of admission grew 10,000 colony forming units/ml of Escherichia coli that were susceptible to ampicillin/sulbactam.

Left lateral radiograph obtained at time of second presentation, demonstrating marked bilateral renomegaly
The cat’s clinical condition declined despite therapy, with worsening depression and lethargy. The azotemia progressed with a creatinine of 12.7 mg/dl, BUN of 193 mg/dl and phosphorus of 11.1 mg/dl (RI 2.2–7.9 mg/dl) obtained approximately 48 h after the initiation of fluid therapy. Based on the progressive azotemia, scant remaining renal cortical tissue on abdominal ultrasound and the cat’s clinical decline, the owners elected euthanasia.
Gross necropsy confirmed bilateral renomegaly and hydronephrosis, with severe attenuation of the renal cortices (Figure 3). The right renal cortex was ≤3 mm thick throughout and the left renal cortex was typically ≤1–2 mm thick. Both proximal ureters had a segment of marked tortuosity at the ureteropelvic junction (UPJ) (Figure 4).

Bilateral renomegaly in situ (R = right kidney, L = left kidney, B = urinary bladder)
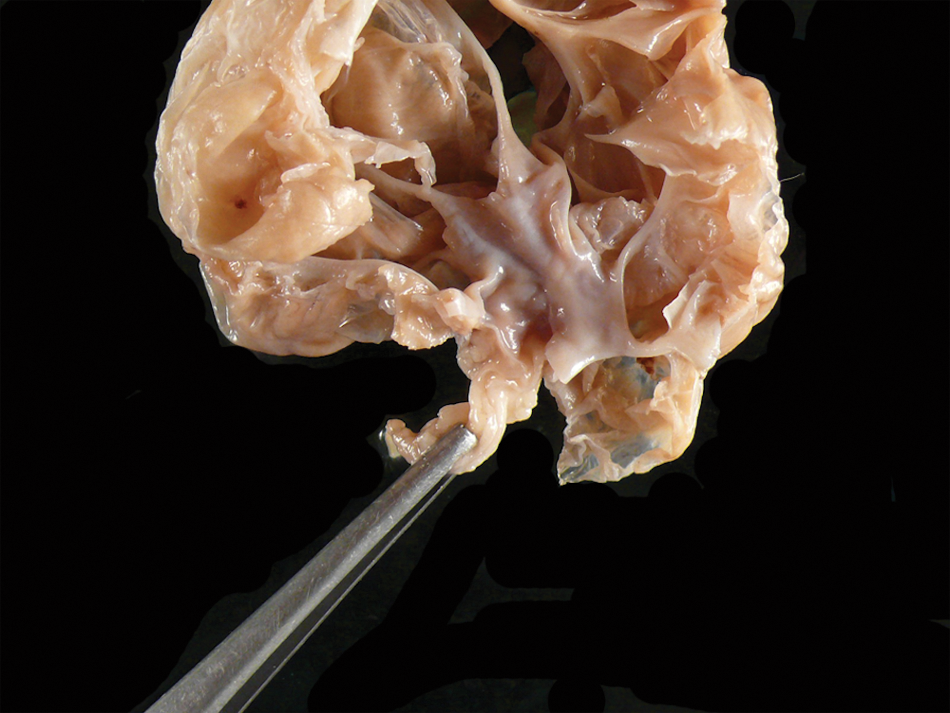
Left kidney and proximal ureter. Severe hydronephrosis and tortuous proximal ureter. The ureter is under mild traction and is rotated to bring the tortuosity into one visible plane
The left proximal ureter was approximately 10 mm in circumference at the pelvic opening, then formed two acute angle turns within a 1 cm long segment with a folded ureteral wall at the first angle. The ureter luminal circumference was 2 mm at the first turn, then narrowed to 1 mm at the second turn. The right proximal ureter had similar tortuosity; the circumference was 5 mm at the UPJ, then decreased to 2 mm just proximal to a 180° turn, with multiple folds in various planes affecting approximately 1 cm of the length of the ureter. The diameter at the distal end of this segment was 1 mm. Bilaterally, the tortuous proximal segments were tightly folded, collapsing the lumen but not completely eliminating patency; the segments retained elasticity with no gross evidence of fibrosis. The distal portions of both ureters were of uniform, normal diameter with no evidence of obstruction or stricture.
Histopathologic examination of the left proximal ureter revealed a tortuous, serpentine ureter with a patent lumen when in section. Masson’s trichrome stain of the ureter showed longitudinal and circular layers of smooth muscle in the wall, with no evidence of smooth muscle dysplasia or fibrosis. Histopathologic examination of the kidneys revealed severe bilateral renal cortical and medullary atrophy with interstitial fibrosis, mild lymphoplasmacytic interstitial nephritis and mild multifocal acute tubular necrosis. There was severe subcapsular hemorrhage in the right kidney. A diagnosis of bilateral UPJ stenosis was made; stenosis presumably led to progressive increases in intra-renal pressure, severe acquired hydronephrosis with corticomedullary atrophy and, ultimately, acute hemorrhage from high intracapsular pressures.
This case report documents bilateral UPJ stenosis leading to renal failure and eventual euthanasia in a cat. This was presumed to be a congenital deformity leading to a gradual progression of hydronephrosis, which was not detected until renomegaly was first palpated. Ureteral stenosis is a rarely reported condition in the cat. Unilateral proximal and mid-ureteral (double) stricture has been reported in an 8-month-old cat during presurgical evaluation of cryptorchidism. 1 This was an incidental finding — the cat was asymptomatic, was not azotemic and had normal urine concentrating ability. No histopathology was performed to determine if this cat had fibrosis and stricture, rather than a congenital stenosis; however, the authors suspected a congenital anomaly. A case of congenital bilateral ureteral stenosis and hydronephrosis has been reported in one dog, who died at 10 days of age. 2 Bloodwork was not performed; however, the authors suspected uremia as the cause of death. A second report, in a 5-year-old dog, documented successful management of congenital ureteral stenosis with the use of ureteral stents. 3 To the our knowledge, the present report documents the first case of feline congenital UPJ stenosis leading to progressive kidney failure.
UPJ obstruction is the most common cause of hydronephrosis in human fetuses and young children 4 and is thought to result from abnormal mesenchymal development. The condition is diagnosed by demonstration of obstructed urine flow in a kidney with hydronephrosis and dilation of calyces, but with a ureter of normal diameter. 5 The degree of renal pelvicalyceal dilation and renal impairment is quite variable. 5 Approximately 25% of cases are bilateral; 6 bilateral hydronephrosis requires intervention, whereas neonatal surgery for unilateral hydronephrosis remains controversial. This condition may not be discovered until adulthood; in one report, over 50% of patients diagnosed with congenital UPJ obstruction were older than 20 years of age. 7
Hydronephrosis in cats may result from ectopic ureters, pyelonephritis, or ureteral obstruction from uroliths or acquired strictures.8–10 Ureteral stricture (ureteral fibrosis leading to a narrowed lumen) is most commonly unilateral in cats and is typically secondary to ureteral surgery, ureteritis or ureterolithiasis, but can also be idiopathic. 11 In the cat in this report the bilateral lesions were most consistent with malformation, rather than fibrosis and stricture. The acute decompensation was likely due to progressive increases in intra-renal pressure, leading to subcapsular hemorrhage and acute renal ischemia. Pyelonephritis may have contributed; however, the renal histology suggested ischemic damage was the prevailing pathology, with only mild inflammation present. The severe loss of renal cortical tissue and low numbers of residual functional nephrons would allow any minor injury to the kidney to result in more severe consequences.
It is possible, had it been discovered earlier, that this cat’s condition might have responded to ureteral stenting, as previously reported in one dog. 3 Although UPJ stenosis is apparently quite rare in cats, this condition should be considered in a patient with unilateral or bilateral hydronephrosis of undetermined cause. Additional diagnostics, including blood and urine testing, imaging and, possibly, contrast studies, should be offered to further define an underlying cause and to explore treatment options early in the course of disease.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.