
Abstract
Two cats with intractable idiopathic chylothorax and a history of unsuccessful medical management were treated thoracoscopically with en bloc thoracic duct sealing and subtotal pericardectomy using a bipolar feedback-controlled vessel sealing device. No surgical complications were observed. Twenty-four and 26 months after surgery, both cats were free of thoracic effusion and clinical signs.
Case Report
Chylothorax results from the accumulation of chyle in the thoracic cavity and leads to dyspnoea and fibrosing pleuritis in affected cats and dogs. 1 Although several aetiological factors have been discovered, the disease is considered idiopathic in most cases. 2 Medical therapy typically involves dietary management, needle thoracocentesis or drainage via chest tube. Oral benzopyrones, such as rutosid, have also been advocated.3–5 If the disease is idiopathic and the patient does not respond to medical management, surgical intervention is warranted. In cats, the current recommendations combine thoracic duct (TD) ligation with partial pericardectomy with or without omentalisation.6–8 A thoracoscopic treatment has not yet been described in cats.
A 7-year-old, male castrated European shorthair cat was referred to the Clinic for Surgery, Ophthalmology and Dentistry of the University of Veterinary Medicine of Vienna, with a 3-week history of increasing dyspnoea, which was exacerbated by feeding. On clinical examination, the cat showed a body condition score of 8 (range 1–9). 9 The respiratory rate was 60 breaths/min with increased bronchio-vesicular lung sounds in the dorsal regions and decreased lung sounds over the ventral part of the lung field. Other clinical parameters were unremarkable. Blood work abnormalities included a mild leukopenia 5.5 × 109/l (reference interval 6–18 × 109/l) and lymphopenia 0.51 × 109/l (reference interval 0.9–5.1 × 109/l), an elevated serum creatinine 185.64 µmol/l (reference value <141.44 µmol/l) and a total protein level of 86.8 g/l (reference interval 60–75 g/l). Thoracic radiographs revealed bilateral pleural effusion and a loss of contour of the cardiac silhouette. Bilateral thoracocentesis yielded 400 ml of an odourless, opaque, milky fluid. Pleural fluid analysis revealed a total cell count of 3.38 × 109/l, a total protein content of 39 g/l and a cholesterol to triglyceride ratio of 0.09. On cytopathological evaluation, the predominant cell types were small lymphocytes (50%) and non-toxic neutrophils (50%). A diagnosis of chylous effusion was made. Echocardiography and computed tomography (CT) did not reveal any abnormality that would explain an underlying cause for the chylous pleural effusion. Bilateral thoracic drains were placed and medical treatment was started with a low-fat diet (obesity management, Royal Canin), 15 mg/kg q12h of oral amoxicillin–clavulanic acid (Clavaseptin; Vétoquinol) and 50 mg/kg q6h of oral rutosid (Rutin; Twardy). Owing to persistent chylous pleural effusion, a surgical intervention was performed 10 days later. Under general anaesthesia, the cat was positioned in slightly oblique right sterno-lateral recumbency and the entire left hemithorax and abdomen were clipped, aseptically prepared and draped. A 5 mm portal was created in the left tenth intercostal space (ICS) midway between the sternum and the vertebral column, and a 5 mm 30° videoscope (Karl Storz Veterinary Endoscopy), was introduced. Two 5 mm instrument portals were placed at the dorsal third of the thoracic wall in the ninth and tenth ICS. The caudo-dorsal mediastinum was dissected dorsal to the aorta with a L hook tip, Opti2 monopolar laparoscopic electrode (Valleylab). A Ligasure V 5 mm vessel sealing system (LVSS) (Valleylab) device was inserted through the second instrument port. Tissues dorsal to the aorta and ventral to the sympathetic trunk were sealed and transected en bloc (Figure 1). A 3 mm stab incision was made in the ventral third of the left fourth ICS, and a curved haemostat was introduced under thoracoscopic guidance and used to grab the pericardium. In addition, a partial pericardectomy was thoracoscopically performed using the LVSS. The pericardium was removed through one portal hole. Using a 3-cm left paracostal abdominal approach and a fenestrated bowel grasping forceps (Karl Storz Veterinary Endoscopy), the omentum was mobilised from the greater curvature of the stomach and advanced into the thorax through a 2 cm paracostal diaphragmatic incision. New thoracostomy tubes were placed bilaterally. The thoracoscopic cannulas were removed and the surgical sites were closed in a routine manner. Total surgical time from skin incision to complete skin closure was 210 min for cat 1. The thoracic drains were removed on day 8 after the thoracic fluid production decreased to 1.2 ml/kg/24 h and pleural effusion changed from opaque–milky to a clear, serous effusion. Bacterial culture obtained from the tip of the thoracic drains resulted in sporadic growth of positive haemolytic and coagulase-negative staphylococci. As those were suspected to be contaminants, the antibiotic treatment was discontinued and the cat was discharged 9 days post-surgery. The owner was instructed to feed the cat with a low-fat diet. No other medications were prescribed. Two years and 2 months post-surgery, no signs of dyspnoea were reported. On clinical examination the cat showed a normal breathing pattern with a 28 breaths/min respiration rate and mildly increased bronchio-vesicular lung sounds were audible during auscultation. On follow-up radiographs, no signs of pleural effusion could be identified.
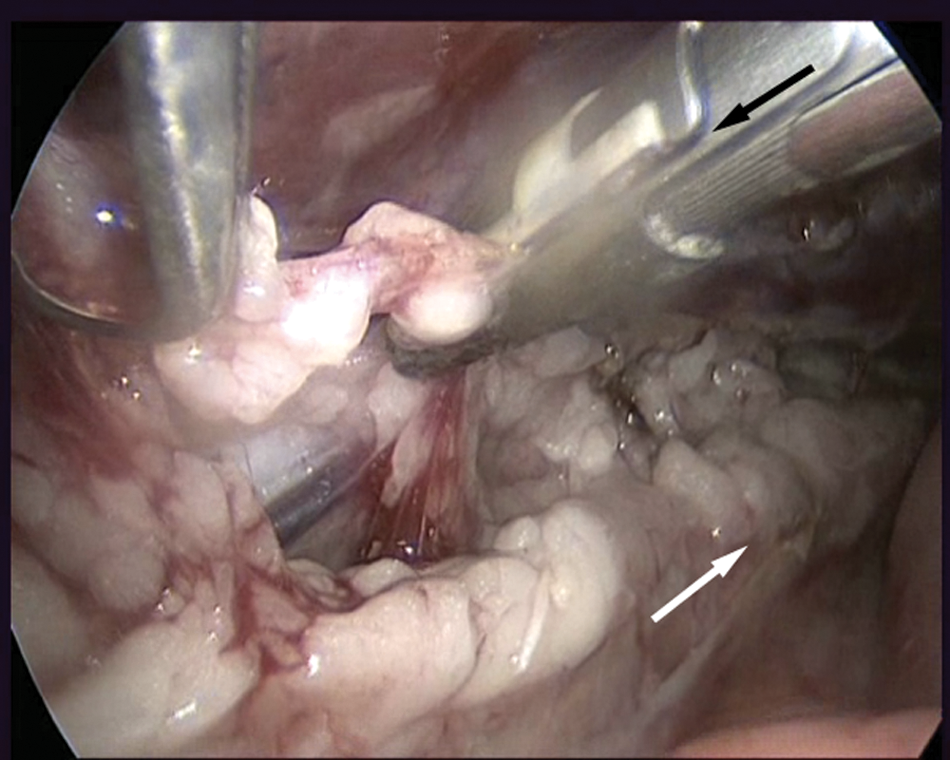
Left thoracoscopic view of cat 1. The TD and the tissue surrounding the TD between the aorta (white arrow) and ventral to the sympathetic trunk are sealed using the LVSS (black arrow)
The second cat, a 4-year-old male castrated Ragdoll, presented with a history of chronic dyspnoea for 2 months. The clinical signs included tachypnoea and bilateral crackling lung sounds. The core body temperature was 39.6 °C. Serum creatinine level was elevated at 176.8 µmol/l (reference <141.44 µmol/l), and the rest of the blood chemistry panel and the cell blood count were within normal limits. Subsequent thoracic radiographs showed bilateral pleural effusion. Thoracocentesis revealed a milky, opaque fluid with a total cell count of 22.5 × 109/l and a total protein content of 49 g/l. The cell population consisted of 70% small lymphocytes, 25% neutrophils and 5% macrophages on the cytological evaluation. Bacteriological fluid examination was negative for aerobes and anaerobes. Although the cholesterol to triglyceride ratio of the thoracic fluid was not calculated for cat 2, the macroscopic appearance and the laboratory and cytological findings were consistent with a chylous effusion. Further diagnostics included follow-up thoracic radiographs, echocardiography and CT of the thorax, which failed to identify any underlying cause. A presumptive diagnosis of idiopathic chylothorax was made. Treatment was started and consisted of a low-fat diet (obesity management, Royal Canin), 50 mg/kg q6h of oral rutosid (Rutin; Twardy), 0.2 mg/kg q12h of oral prednisolone (Prednisolon; Nycomed) and thoracocentesis if necessary. Despite initial clinical improvement, pleural effusion persisted and 100–200 ml of chylous effusion were removed by thoracocentesis every 3–4 weeks. After 6 months of conservative treatment, the owners elected to perform surgery. The surgical procedure for cat 2 was similar to that for cat 1, but no omentalisation was performed. Total surgical time was 125 min. Thoracic drains were removed on day 7, when pleural fluid production decreased to 1.3 ml/kg/24h. Nine days post-surgery, the cat was discharged and the owner was instructed to feed the cat a low-fat diet. No other medications were prescribed. One year and 10 months after surgery, the cat remained clinically healthy without any signs of dyspnoea. Follow-up thoracic radiographs taken at the time showed a well-ventilated lung field without any signs of concurrent pleural effusion (Figure 2).

Right lateral thoracic radiograph of cat 2, 1 year and 10 months after surgery. Note the absence of concurrent pleural effusion
The Ligasure vessel sealing system LVSS (Valleylab) was used in both cats for thoracoscopic partial pericardectomy, and en bloc sealing and transection of the tissues encompassing the TD. In an experimental study on pigs, Novitsky et al 10 first validated the effectiveness of the LVSS to obtain a tight seal of the TD. Khelif et al 11 reported two successful cases of thoracoscopic TD sealing using LVSS in children with chylothorax. To the best of our knowledge, the use of LVSS for the treatment of chylothorax in dogs or cats has not yet been reported. In veterinary medicine, suture material, haemostatic clips and, recently, ultrasonically-activated shears have been used for TD occlusion.6,12,13 The aim is a complete occlusion of the TD and all its collateral branches to promote the formation of alternate lymphatico-venous drainage routes. 14 Incomplete ligation and anastomosis formation around the ligated TD are reported to be causes for late failure.6,15 Viehoff et al 16 reported a 50% clinical success rate in dogs that were treated with en bloc ligation of the TD alone. In a cadaver study, MacDonald et al 17 showed that en bloc TD ligation successfully prevented contrast agent passage cranial to the ligature in 13/14 dogs. In cats, en bloc ligation in combination with a subphrenic pericardectomy and omentalisation led to a resolution of clinical signs in 3/4 cats in one study. 7 In human medicine, thoracoscopic TD sealing has become the technique of choice for the treatment of chylothorax. 18 Despite a suspected longer operative time, thoracoscopy provides a magnified view and, therefore, better visualisation of anatomic structures. Its reported advantages in human and veterinary literature comprise reduced postoperative pain, shorter hospital stays and decreased morbidity.19–22 In these two cats, using the LVSS, en bloc sealing and transection of the soft tissues located in the caudo-dorsal mediastinum between the aorta and the sympathetic trunk was feasible thoracoscopically. This technique, combined with a thoracoscopically performed partial pericardectomy, resulted in the resolution of clinical and radiographic signs in both cats. The need for and the role of omentalisation in cat 1 cannot be evaluated.
Footnotes
Acknowledgements
Radiographs were provided by the central diagnostic unit of the University of Veterinary Medicine Vienna.
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this case report.
Conflict of interest
The authors declare that there is no conflict of interest.