
Abstract
A 5-year-old, castrated male, domestic shorthair cat presented with firm swelling in the right temporal region of the skull. The cat’s jaws were almost locked in the closed position. Radiographs showed a mass with an irregular mineralized matrix superimposed on the caudal right mandible and temporomandibular joint. Surgical exploration revealed that the mass arose from the proximal part of the vertical ramus, which was removed, with the exclusion of the temporomandibular joint. It was possible to open the cat’s mouth to nearly normal extension immediately after surgery. Recovery was uneventful — the cat has had no problem eating and no mass recurrence has been detected 3 years after surgery. Histological examination of the mass was consistent with chondroma. To the best of our knowledge, this is the first clinical and pathological description of a chondroma in cats, and one of the rare cases describing clinical presentation and management of primary bone tumours involving the vertical ramus of the feline mandible.
Case Report
A 5-year-old, castrated male, domestic shorthair cat presented to our clinic with inactivity and weight loss over the past few months. On physical examination, the cat was alert, slightly underweight and had an unkempt coat. Vital signs were normal. There was a firm swelling, approximately 4 cm in diameter, in the right temporal region of the skull. Oral cavity examination revealed that the cat’s jaws were almost locked in the closed position.
Skull radiographs demonstrated a mass with bone opacity. Ventrodorsal radiographs suggested the mass was superimposed on the caudal right mandible and temporomandibular joint (Figure 1a). Additional oblique projections (not shown) and palpation localised the mass proximal to the right caudal body of the mandible and temporomandibular joint, and medial to the lateral border of the zygomatic arch.

Ventrodorsal radiographs of cat’s skull before (a) and after surgery (b). A mass with irregular radiopacity superimposed on the caudal right mandible and temporomandibular (a). Radiograph demonstrating preservation of the caudal body of the right mandible and temporomandibular joint after the mass removal (b)
Thoracic radiographs were obtained and showed no evidence of metastasis or other abnormalities. Complete blood count and serum biochemistry were also within normal range.
Owing to the possible involvement of feline retroviruses in the induction of neoplastic processes, blood serum from the cat was tested to detect feline leukaemia virus (FeLV) antigen and feline immunodeficiency virus (FIV) antibody. A commercially-available enzyme-linked immunosorbent assay was used (Snap FIV/FELV combo test; Idexx Laboratories). The test was positive for FIV but negative for FELV.
Surgical exploration was performed to attempt to excise the mass. A combination of acepromazine (0.1 mg/kg), butorphanol tartrate (0.4 mg/kg) and midazolam (0.2 mg/kg) given intramuscularly was used as premedication. Induction was carried out by an intravenous combination of ketamine (2 mg/kg) and diazepam (0.5 mg/kg); endotracheal intubation was achieved through tracheotomy incision. Anaesthesia was maintained with isoflurane.
The mass was approached through a skin incision over the right zygomatic arch. Further dissection revealed that the mass arose from the vertical ramus of the right mandible and actually locked the mandible in a closed position between the temporal and zygomatic bones. The zygomatic arch and the entire vertical ramus containing the mass were removed as described previously. 1 Macroscopically, the mass was firm, with a smooth lobular surface covered by a fibrous capsule. The right temporomandibular joint was preserved (Figure 1b). A passive penrose drain was placed and the defect routinely closed.
It was possible to open the cat’s mouth to nearly normal extension immediately after surgery, although a mild limitation in range of motion and some stiffness were present, which were attributed to masseter muscle contracture and periarticular fibrosis due to chronicity of the process.
The day after surgery, the cat was allowed to eat moist commercial food and had no difficulties with prehension or mastication. The cat was treated for 7 days with clavulanate-potentiated amoxicillin (20 mg/kg every 12 h). The penrose drain was removed 3 days after surgery. Moist food was fed for 2 weeks following surgery; thereafter, the cat was allowed to eat dry commercial food. No prehension or mastication problems were observed and no mass recurrence has been detected 3 years after surgery.
Histologically, the mass was characterized by irregular lobules of well-differentiated hyaline cartilage with numerous, rather uniform, chondrocytes embedded in normal hyaline matrix. Numerous dark blue granules were seen under high magnification (Figure 2b) and reflected matrix mineralisation. There were multiple embedded blood vessels surrounded by some mineralised matrix. The mass was well demarcated and encapsulated by a layer of fibrous connective tissue. Mitotic figures were not observed and there was no evidence of bone formation (Figure 2a, b). These morphological features were consistent with a chondroma. 2 Absence of osteoid within the tumour helps to differentiate it from osteoma and other bone tumours containing cartilage, such as osteochondroma. It is sometimes difficult to distinguish between chondroma and chondrosarcoma. However, the uniformity of the cell population, the absence of polymorphism and mitotic activity support our diagnosis. As the chondrocytes were well- differentiated, and the fibroblasts and cartilage matrix were obvious, immunohistochemistry studies were deemed unnecessary in this case.
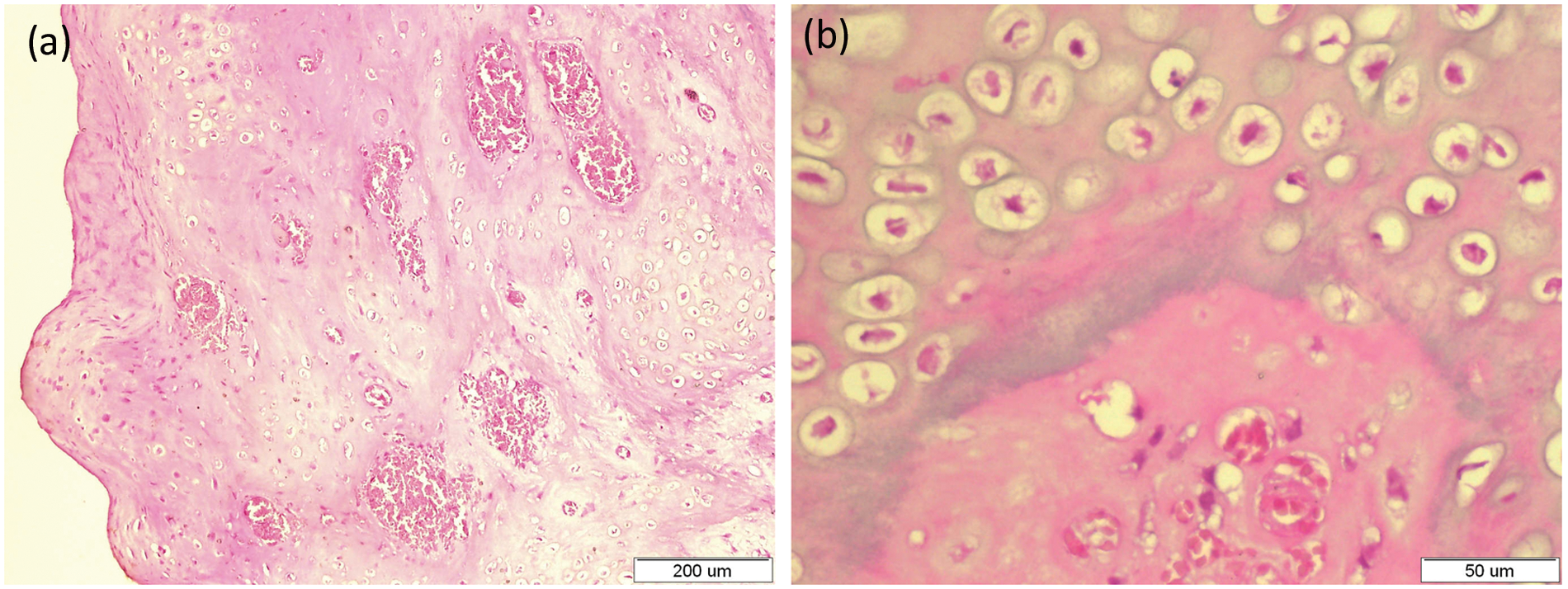
Histological section of the mass: (a) irregular lobules of well-differentiated hyaline cartilage with large blood vessels surrounded by a mineralised matrix and covered by an outer layer of fibrous connective tissue, haematoxylin and eosin stain (H&E) × 100; (b) section of the mass under higher magnification, H&E × 400
Although the tumour described here exhibited morphological features characteristic of chondroma, multiple blood vessels surrounded by mineralised matrix embedded in the tumour (Figure 2) do not correspond with the typical description of chondroma.
With the lack of other reports, it is impossible for us to conclude if these features are characteristic of feline chondroma or unique to the current case.
Primary bone tumours are uncommon in cats, with a reported incidence of 4.9 per 10,000 cases. 3 The vast majority of tumours involving feline bones are malignant. Osteosarcoma, fibrosarcoma and chondrosarcoma are among the most frequently reported.3–5 Feline osteochondromatosis, a polyostotic disease probably of viral aetiology, accounts for approximately 20% of primary bone tumours reported in cats. 5
Reports of benign feline bone tumours are much rarer. Among them, the most frequently reported are osteoma4,6,7 and, much less frequently, solitary osteochondroma5,6 and ossifying fibroma. 5 To the best of our knowledge, the current report is the first to provide a clinical and pathological description of a chondroma originating from the feline mandible.
A chondroma is a benign neoplasm of cartilage. Chondromas of bone are rare in animals but have been reported in several domestic species, particularly aged dogs and sheep. 8 No breed or sex preference is reported, but the number of cases is too small for a valid assessment. 2
Primary chondromas of bone are divided into enchondromas — which originate within the medullary cavity of bone — and ecchondromas — which arise from cartilage elsewhere in the skeleton, most commonly in flat bones, turbinates and the sternocostal cartilage complex. 2 Periosteal chondromas, which develop beneath the periosteum adjacent to the cortical surface in humans, 9 have not been reported in animals. 2
The tumour described herein originated from the vertical ramus of the mandible (flat bone) and was surrounded by fibrous connective tissue rather than bone cortex. These features suggest that the tumour belongs to a category of ecchondromas.
Previous veterinary reports described chondromas as relatively radiolucent growths with smooth outlines. 2 While human enchondromas are rarely calcified, as many as 50% of human periosteal chondromas show radiographic evidence of mineralisation. 10 In our case, the tumour was also radiopaque with a mixed bone opacity (Figure 1a). This radiodense appearance was probably due to matrix mineralisation (Figure 2b) and not due to osteoid formation, as happens in some other radiopaque primary bone tumours, such as ossifying fibromas, osteochondromas, osteomas and osteosarcomas.2,4,5 It was reported previously that radiography failed to distinguish between malignant and benign lesions in a case of feline chondrosarcoma. 11 However, radiographs remain an essential diagnostic tool, as they are helpful in determining the site of lesion, extent of involvement and host response.
Primary bone tumours involving mandibles are extremely rare in cats. In a review of bone tumours in cats, only one case of a primary bone tumour of mandible (osteosarcoma) was described. 4 Another study described only a single case of ossifying fibroma involving the mandibular body over a 10-year period. 5 To the best of our knowledge, there is only one report describing clinical presentation and treatment of a bone tumour involving the coronoid process of the feline mandible. 7 Clinical signs and physical examination findings were similar to this case: resection of the tumour with the caudal two-thirds of the coronoid process, condyloid process and caudal part of the zygomatic arch was curative. Histological examination was not performed and a tentative diagnosis of osteoma was made based on radiographic and cytological examinations.
As there are no previous reports of chondroma in cats, it is impossible to define the clinical behaviour of the tumour in this species. Chondromas are described as slow-growing neoplasms. 2 Unfortunately, the growth rate of the current tumour could not be assessed from the case history.
Nevertheless, numerous studies have demonstrated that the most successful treatment of primary bone tumours of cats, regardless of histological diagnosis, is wide surgical excision or amputation;5,11 the current report strengthens this conclusion.
Footnotes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this case report.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.