
Abstract
What is ‘advanced imaging’?
In veterinary medicine, the term ‘advanced imaging’ generally refers to computer-based technologies that produce cross-sectional images of the body: ultrasonography, computed x-ray tomography (CT) and magnetic resonance imaging (MRI). Conventional radiography (film–screen or digital) and planar scintigraphy are not considered advanced, although modern digital x-ray and scintigraphic equipment may contain high technology components. By eliminating the problem of superimposition that affects radiography and planar scintigraphy, cross-sectional imaging modalities enable clearer depiction of anatomy, particularly in parts of the body with relatively complex internal anatomy that is not well suited to planar imaging (Figure 1).
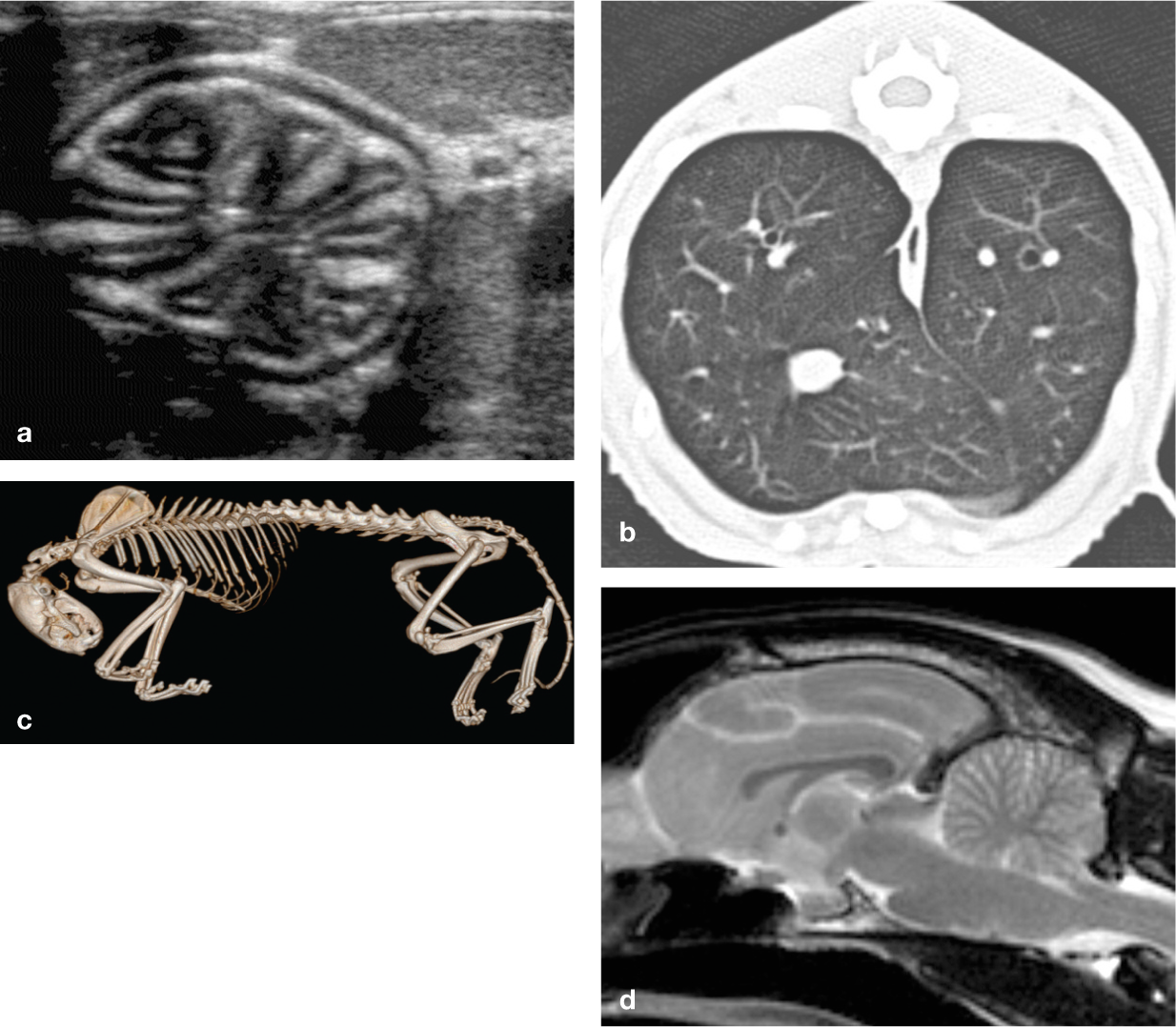
Examples of superior anatomical detail provided by advanced imaging modalities. (a) Ultrasonographic image of the feline stomach; (b) CT image of the feline lung; (c) volume-rendered CT image of the cadaver of a cat examined for forensic purposes; (d) magnetic resonance (MR) image of the feline brain
With clearer depiction of anatomy comes clearer depiction of morphological abnormalities that alter anatomy. Hence, advanced imaging modalities are inherently better detectors of diseases than radiography, despite having lower spatial resolution (Figure 2). Advanced imaging modalities enable superior contrast between anatomical structures in different parts of the body according to their physical characteristics: ultrasonography displays differences in acoustic impedance; 1 CT depicts structures with different physical density; 2 and MRI displays variations in the physicochemical properties of tissues based on proton density and mobility. 3

Examples of diagnoses facilitated by advanced imaging. (a) Ultrasonographic image of small intestinal intussusception in a kitten; (b) CT image of a cat with chronic otitis externa and media; (c) CT image of thickened pleura and trapped fluid (*) in a cat with local spread of pulmonary carcinoma; (d) Sagittal MR image of the brain of a cat with spongiform encephalopathy showing diffuse hyperintensity of cerebellar grey matter
The focus of diagnostic imaging is on morphological features of disease; this is reflected in the terminology of radiology reports, in which abnormalities are described according to their number, size, shape, position and margination. The remaining sign – signal – changes according to the modality: opacity for radiography; echogenicity for ultrasonography; density or attenuation for CT; and intensity for MRI. Although signs of certain functional disorders may be detected by imaging, most animals with functional disorders such as endocrinopathies, immune-mediated conditions, renal insufficiency or diarrhoea may be managed satisfactorily without any imaging.
For decades, veterinary diagnostic imaging meant only radiography. Since the 1980s, ultrasonography, CT and MRI have come into routine use in referral practices around the world. The proliferation of imaging has been fuelled by multiple factors, including technological development, increased expectations and disposable income of companion animal owners, popularity of radiology as a postgraduate speciality and growth of referral practices that compete with the veterinary schools for patients. Popularity of pet health insurance is a significant additional factor in the UK. Increased availability of advanced imaging is good because it increases choice for veterinarians managing patients, but it can be problematical if there is a lack of expertise in making or interpreting the images, or if use of these modalities increases veterinary fees without a corresponding benefit to patients. Increased use of diagnostic imaging in recent years has likely contributed to the increase in veterinary fees per visit. 4
It is clear that advanced imaging is being widely used, but is it also being misused? To answer this question, it is necessary to consider why imaging is used and, if possible, to distinguish uses and misuses.
Is diagnostic imaging necessary?
As its name implies, diagnostic imaging is used primarily to enable clinicians to make correct decisions about their patient’s diagnosis and the severity or stage of their condition and, therefore, to contribute to their effective and efficient treatment. But not all veterinary patients need imaging.
There are three pieces of information that a clinician needs in order to determine whether imaging should be performed: 5
Based on the patient’s clinical history and results of diagnostic tests that have already been performed, what is the probability that this patient has a morphological lesion? This is the pre-test probability – see below.
How accurate is the diagnostic imaging test being considered?
Are the results of imaging likely to have any impact on patient management?
Accuracy of diagnostic imaging
Two fundamental indices of test accuracy are sensitivity (the probability of obtaining a positive test result in a patient with the target condition) and specificity (the probability of obtaining a negative test result in a patient without the target condition). 5 Few diagnostic tests have both high sensitivity and high specificity, and tests are used according to their strengths. The logical way to take advantage of a test with particularly high sensitivity is to use a negative result to rule out disease. 6 An example of an imaging test with high sensitivity is bone scintigraphy in human athletes with suspected stress fracture. 7 A normal bone scintigram can be used to rule out a stress fracture in these patients, and the same rationale is used when interpreting bone scans of young racehorses. 8


Likelihood ratios are another useful index of the accuracy of imaging tests because they give an indication of a test’s effect on the probability of a diagnosis: 9

High likelihood ratios (>10) associated with positive test results (PLR) significantly increase the probability of the target condition, while low likelihood ratios (<0.1) associated with negative test results (NLR) significantly decrease the probability.
Likelihood ratios were calculated in a systematic review of veterinary diagnostic imaging. 10 Out of 5936 articles reviewed spanning the period 1976–2006, only 88 contained sufficient data to assess the diagnostic performance of imaging studies. These 88 articles described 103 studies involving a range of imaging modalities and target conditions, with widely varying sensitivities and specificities (Figure 6). Excluding studies of pregnancy diagnosis, median sensitivity was 78% (range 0–100%) and specificity 92% (range 33–100%). PLR was >10 in 21/77 (27%) studies and NLR was <0.1 in 13/77 (17%). Only eight (10%) diagnostic imaging tests had both high PLR and low NLR (Table 1). For most imaging tests for which performance data are available, accuracy is only moderate, hence it appears that few imaging tests can be used to rule in or rule out a diagnosis. In many cases, the result of imaging may have little impact on the probability of diagnosis.

The effect of a diagnostic test result is to modify the probability that the patient has the target condition

Plots of positive (PPV) and negative predictive value (NPV) against prevalence (logarithmic scale). If the prevalence of disease is low, a positive test result is likely to be a false positive (PPV <50%). The converse is true for negative results: a negative result is likely to be a false negative (NPV <50%) if the prevalence is high
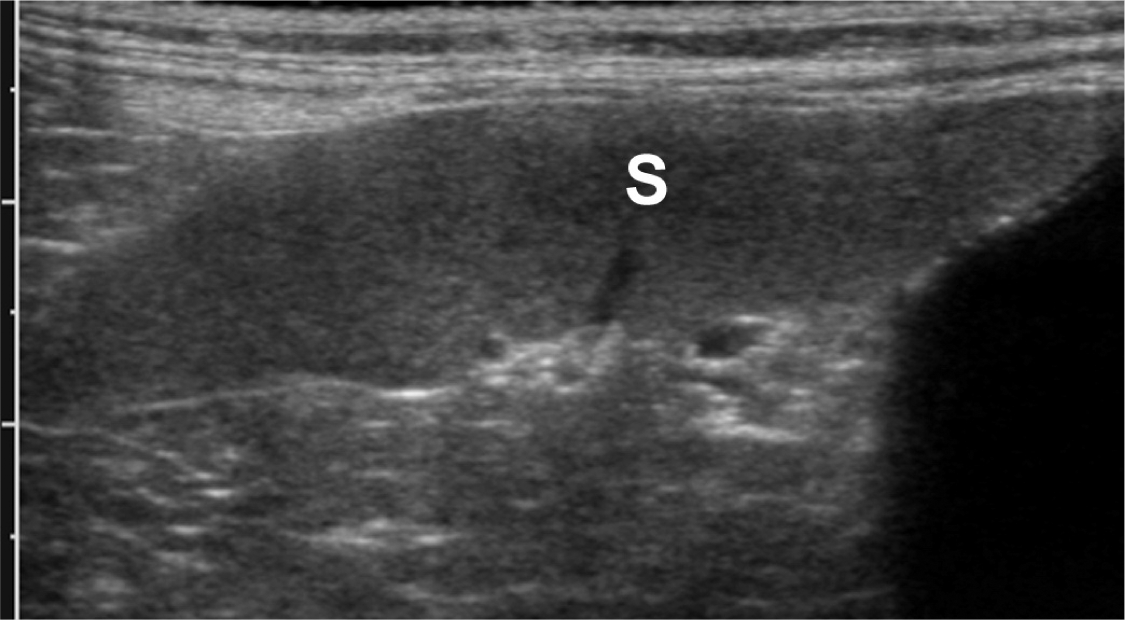
A middle-aged male cat was reported by the owner to be inappetent. Physical examination, haematology and serum chemistry determinations were within normal limits. Abdominal ultrasonography was requested to look for occult signs of disease. The spleen (S) was subjectively considered to be enlarged. Fine needle aspiration of the spleen was undertaken but revealed no cytological abnormalities. Inappetence resolved subsequently without treatment. There is no convincing evidence that this cat was unwell; hence, the ultrasonographic findings represented a false positive result

Receiver operating characteristic plot of results of 103 studies of accuracy of veterinary diagnostic imaging tests for pregnancy diagnosis (solid diamonds) and other conditions (open diamonds). 10 Tests of pregnancy diagnosis had higher sensitivity than tests of other conditions (P <0.0001). Tests with highest accuracy are at the top left corner of the plot. Relatively few imaging tests are very accurate
Studies of veterinary diagnostic imaging (excluding pregnancy diagnosis) with PLR >10 and NLR <0.1

PLR = likelihood ratio for a positive result, NLR = likelihood ratio for a negative result, CI = confidence interval, n = number of subjects, US = ultrasound (including Doppler studies), XR = radiography, NM = nuclear medicine
Impact of imaging on patient management
Although clinical studies often focus on the accuracy of diagnostic imaging, the ultimate standard of the usefulness of a diagnostic test is not its accuracy, but whether it improves patient outcomes. 19 In fact, the appropriateness of diagnostic imaging may be defined as the difference in outcomes between empirical treatment and treatment informed by imaging. 20 Advanced imaging modalities offer the possibility of more accurate diagnosis and staging of disease, with correspondingly better patient outcomes than observed with conventional imaging; however, improvements in patient outcomes do not follow automatically when new imaging modalities are introduced (see Example 1).
Limited diagnostic impact of advanced imaging – CT in dogs with elbow pain
Elbow arthritis as a result of fragmented medial coronoid process (MCP), osteochondritis dissecans of the humeral condyle and joint incongruity is a major problem in young dogs. Survey radiography is not considered accurate enough for reliable diagnosis of these conditions. CT has a higher sensitivity for detection of displaced MCP fragments 21 and is increasingly used instead of radiography.
A retrospective clinical study has reported associations between results of CT and results of arthroscopy in 101 elbow joints of lame dogs. 22 CT showing fragmented MCP was a predictor of displaced fragment on arthroscopy (PLR 5.3, 95% confidence interval [CI] 2.8–10.1) and cartilage erosion affecting the humerus (PLR 3.1, 95% CI 1.8–5.4). Lack of a fragment on CT was a predictor of lack of a displaced fragment on arthroscopy (NLR 0.18, 95% CI 0.085–0.38) and lack of cartilage erosion on the humerus (NLR 0.44, 95% CI 0.29–0.66). Although there were significant associations between certain CT signs and arthroscopic findings, the likelihood ratios were not sufficiently high that CT could be used reliably to rule in or rule out elbow lesions. False positive and false negative results occurred frequently. It was concluded that CT was not sufficiently accurate that it could be used to determine the need for arthroscopy (or arthrotomy) in a young dog with suspected elbow arthritis.
Hence, when faced with a young Retriever or Rottweiler with signs of elbow pain, in which fragmented MCP is considered likely, there may be merit in proceeding straight to arthroscopy for investigation and treatment that is likely to be definitive in the majority of dogs. Under these circumstances, CT would have no impact on patient management. Although CT may detect lesions that will not be visible arthroscopically and lesions that would be better treated by arthrotomy than arthroscopy, it is unclear how CT should be used in order to maximise the benefit to patients.
There is a hierarchy of factors that can influence patient outcomes (Figure 7). 23 For an imaging test to be effective at a high level in this hierarchy, it must also be effective at lower levels; however, the reverse is not true. For example, a technical development that increases spatial resolution does not guarantee increased diagnostic performance. 23 Evidence of the benefit of advanced imaging relies on well designed studies of diagnostic performance and clinical impact; 24 to date, there are relatively few veterinary studies of this type.

Hierarchy of efficacy of diagnostic imaging 23
Examples of the benefit of advanced imaging were evident in two studies of cats and dogs that underwent thoracic radiography followed by CT.25,26 CT images frequently revealed additional features of lesions that enabled the anatomical location of lesions to be determined correctly and resulted in a change to the working (radiographic) diagnosis in many cases. The single most important clue to radiological diagnosis is the anatomical site of a lesion, which explains why the improved anatomical detail of CT compared with radiography has such a marked impact on diagnosis. The improved anatomical depiction associated with advanced imaging is also potentially beneficial when surgical treatment is being considered, for example in animals with fractures27,28 or portosystemic shunts29–31 (Figure 8). The information gained by CT angiography in feline renal donors enabled the average time taken to surgically harvest the kidney to be reduced by 1 hour. 32

CT images of a German shepherd dog with a congenital intrahepatic portosystemic shunt (arrows). (a) Oblique maximum intensity projection; (b) volume-rendered image. Despite its size, this lesion was not detected ultrasonographically. Surgical treatment of intrahepatic shunts is facilitated by preoperative imaging. CVC = caudal vena cava
When an advanced modality is introduced into a veterinary practice, the tendency is for it to replace radiography even when radiography is effective. For example, survey radiography is an accurate diagnostic modality for dogs with chronic nasal signs, with the majority of patients being correctly categorised as having either rhinitis or nasal neoplasia on the basis of dorsoventral (intraoral) and rostrocaudal (skyline) views. 33 In cats, there is more overlap in the radiographic signs associated with neoplasia and rhinitis, 34 which makes it more difficult to distinguish these conditions. In practices with CT, few cats or dogs undergo survey radiography to investigate nasal signs because they have CT instead. A CT scan of the head may be done more quickly and provides a more detailed depiction of most lesions, which may be interpreted with more confidence than a series of radiographs. However, differentiating rhinitis from nasal neoplasia is based on the same criteria as for survey radiography, hence the accuracy of CT is similar.35–37 Furthermore, imaging of the nasal cavity in a referral setting is invariably followed by endoscopy, nasal flushing or biopsy for definitive diagnosis, and this is true for patients having radiography or CT. Hence, the added value of CT for cats and dogs with chronic nasal signs may be negligible for patients in which the remainder of the diagnostic work-up is unchanged.
The extent of invasive nasal neoplasms is more accurately depicted by CT than was possible with radiography, which makes CT highly desirable as a means of planning radiation therapy. 38 However, the majority of cats and dogs with nasal neoplasms do not receive radiation therapy, hence for them this advantage is never realised.

Uses of diagnostic imaging
Confirming or rejecting a diagnosis
The potential for advanced imaging to increase accuracy of diagnosis is well illustrated in neurology, a clinical speciality that has grown rapidly in recent years because of the increased diagnostic capability offered by MRI. Veterinary neurologists are able to examine the brain and spinal cord in greater detail than ever before,39–42 hence ante-mortem diagnosis of neurological conditions has become commonplace. For example, cerebral and cerebellar infarction, which was considered rare 20 years ago, is now well recognised in cats43,44 and dogs45–47 with acute neurological signs. Similarly, in the light of accumulated experience with the MRI features of intracranial neoplasia, a tentative diagnosis is possible in many cases.48–51
MRI has been used extensively to examine cats52–54 and dogs52,55 with neurological signs associated with intracranial inflammatory conditions. Compared with dogs, cats are more prone to intracranial infection as an extension of otitis media/interna 56 or following a cat bite to the head. 57 CT enables detailed examination of aural structures, 58 but visualisation of the caudal fossa is limited by bone-related artifacts when using CT, hence MRI is the modality of choice for cats with suspected intracranial extension of otitis. MRI is particularly useful for investigation of cats with vestibular signs 54 because inner ear anatomy is well depicted, with the endolymph appearing hyperintense relative to adjacent structures in T2-weighted images. MRI has proved useful as a means of differentiating extension of otitis from other causes of intracranial infections, such as feline infectious peritonitis,53,54 which have a poorer prognosis.
In the spine, MRI has contributed to our understanding of the pathophysiology of conditions such as syringohydromyelia in the Cavalier King Charles spaniel59,60 and fibrocartilaginous embolism, which in many suspected cases proves to be a high-velocity/low-volume disc extrusion. 61 Several studies have compared the accuracy of myelography, CT and MRI for spinal conditions, particularly for disc disease in dogs62–67 and this subject was reviewed recently. 68 MRI is more accurate than myelography in determining the site, severity and cause of lesions affecting the spinal cord (Figure 9). In many veterinary institutions, MRI has replaced myelography; however, despite its advantages, it may be difficult to demonstrate improved patient outcomes (see Example 2).

T1-weighted, post-contrast MR images (a, sagittal; b, transverse) of the thoracolumbar spine of a cat with progressive paraparesis. There is a focal hyperintense lesion occupying the vertebral canal at T12
Equivocal health benefit of advanced imaging – MRI of the spine compared with myelography
For many years, myelography was the principal imaging modality used for diagnosis of spinal cord disease in animals; however, where CT or MRI are available, they have largely replaced myelography. 67 MRI avoids the need for intrathecal contrast medium administration and provides a relatively complete anatomical depiction of the spinal cord and vertebral column, which means that lesions affecting the spinal cord may be visualised directly. There is also evidence that MRI can provide prognostic information in spinal patients because the extent of spinal cord T2 hyperintensity is negatively associated with the probability of a full functional recovery.69,70
Given these advantages, what impact does MRI have on patient outcomes? In order to look for evidence of improved outcomes for canine spinal patients undergoing MRI, a retrospective cross-sectional study was done of 107 dogs with non-ambulatory thoracolumbar spinal disease that had myelography or MRI. 71 Outcome variables included length of hospitalisation, total cost of hospitalisation, status at discharge (alive or dead) and change in neurological grade. No significant association was found between the type of imaging and any outcome variables, except cost of hospitalisation, which was £670 higher on average for dogs that had MRI. Therefore, although MRI may be considered advantageous compared with myelography because it is non-invasive and provides superior anatomical detail, no beneficial effect on outcome of dogs with non-ambulatory thoracolumbar spinal disease was found. If MRI does not appear to improve outcome for these patients, myelography may still be considered a reasonable option.
Just as advanced imaging modalities are replacing radiography, 72 there is competition for patients between advanced imaging modalities. In some practices, CT is tending to replace abdominal ultrasonography, particularly for large dogs. A study of 27 dogs found that sensitivity for abdominal lesions was significantly higher for CT than for ultrasonography for dogs >25 kg. 73
Detecting abnormalities in patients with non-specific signs
The choice of imaging modality is facilitated when a patient’s clinical signs strongly suggest the most likely site and nature of a lesion. When patients have persistent non-specific signs, such as pyrexia or weight loss, comprehensive imaging of the animal may be considered. For example, abdominal ultrasonography or, increasingly, whole body CT may be requested in the hope of uncovering a previously occult lesion (Figure 10). 74

Images from a 2-year-old, female Bengal cat that was inactive and pyrexic, and showing signs of possible spinal pain. (a) T2-weighted sagittal MR scan shows an elongated retroperitoneal lesion (arrowheads) on the ventrolateral aspect of the spine, which is predominantly hyperintense with a focal linear hypointense inclusion (arrow). (b) Subsequent ultrasound scan of this lesion revealed a cavity containing a grass seed (between cursors). Ao = aorta
One of the drawbacks of using comprehensive imaging protocols in patients with non-specific signs is the occurrence of incidental findings – that is, unexpected observations of potential clinical significance (Figure 11). It can be difficult to decide if a finding is likely to be incidental or relevant and whether or not to pursue it with further diagnostic tests, such as biopsy. Liaison between the primary clinician and the radiologist is essential when considering what to do next. Incidental findings complicate a diagnostic work-up, can confuse the clinician and/or animal owner and contribute to increased costs, although it appears – on the basis of several studies of humans – that only a small percentage of incidental findings should necessitate a change in patient management. 75 Veterinary examples of frequent incidental findings include middle ear lesions detected by CT or MRI in cats76,77 and dogs, 78 and hyperplastic nodules of the liver, spleen or adrenal glands revealed by ultrasonography in dogs.79–82

A 10-year-old, female mixed-breed dog was referred for investigation of epistaxis. (a) CT scan of the nasal cavity revealed a homogeneous mass (*) compatible with a primary nasal neoplasm. (b) The CT scan included the regional lymph nodes and, coincidentally, the brain. A sessile mass at the right cerebellopontine angle (arrowhead) is compatible with meningioma. (c) The CT scan also included the thorax (although pulmonary metastasis from a primary nasal neoplasm is rare). A multilocular cavitary mass in the cranial mediastinum (arrows) is compatible with thymoma. Decisions about the management of this patient are complicated by finding apparently unrelated neoplasms affecting the brain and mediastinum
Staging disease as an aid to prognosis and optimal treatment
The ability to examine in detail large regions of the body using advanced imaging is potentially useful for patients in whom the extent of disease determines the prognosis and the optimal treatment. Whole body imaging is primarily used in patients with malignant neoplasia, but is also applicable to patients with inflammatory conditions or severe trauma and to forensic examination of cadavers. 83 A protocol for whole body MRI of veterinary patients has been described. 84 CT represents an efficient and less technically demanding method for imaging the whole body.
The results of staging in a patient with cancer should carry a prognostic meaning that predicts the likely patient outcome. However, the World Health Organization staging does not necessarily correlate with outcome measures in veterinary patients. 85 Also, as more sensitive imaging modalities are used for staging neoplasia, signs of nodal or distant metastasis are identified in a larger proportion of patients than those staged previously using less sensitive imaging, such as radiography alone. This effect, known as stage inflation, 85 is a problem because it confounds comparisons between results of clinical trials, which may undermine decisions by clinicians managing patients with neoplasia.
Mast cell tumour is an example of a neoplasm that should be staged for optimal management. Dogs with grade II or III mast cell tumour with infiltration of the liver and/or spleen have shorter survival times than dogs without. 86 Unfortunately, ultrasonography has low sensitivity for detecting mast cell infiltration of these organs, so fine needle aspiration is recommended for dogs with a clinically aggressive mast cell tumour regardless of the ultrasonographic appearance. A similar recommendation applies to cats or dogs with suspected lymphoma, although sensitivity of ultrasonography appears to be higher for lymphoma in the spleen than in the liver.87,88
In the case of pulmonary neoplasia, the presence of metastasis to the tracheobronchial nodes carries a poor prognosis,89,90 but is difficult to detect by radiography. CT enables detection of signs of lymphatic metastasis, including enlargement of nodes and heterogeneous contrast enhancement pattern.91,92
CT has higher sensitivity for pulmonary nodules than radiography; 93 hence, it is recommended for staging animals with malignant neoplasms that frequently metastasise to the lung. However, caution is necessary when interpreting pulmonary CT images of such patients because lack of visible nodules does not rule out the possibility of metastasis (see Example 3) and because a pulmonary nodule could represent a benign lesion unrelated to the primary neoplasm. There are limited veterinary data on this subject; however, in children with cancer, pulmonary nodules that represent benign or incidental findings cannot be reliably distinguished from malignant nodules without biopsy.95,96 The finding of large numbers of pulmonary nodules at CT is associated with malignancy, 95 but finding a solitary nodule is problematical. For nodules that are not amenable to biopsy, it is usual to repeat the CT after a period of time to look for changes. 97 Lack of enlargement of a nodule supports a diagnosis of ‘non-malignant’ (Figure 12).
Increased sensitivity of advanced imaging – CT for pulmonary nodules
In a retrospective study, thoracic radiographs and thoracic CT images of 18 dogs with histologically confirmed pulmonary metastasis were examined independently for signs of pulmonary nodules. 93 Far more small nodules were visible in the CT images and pulmonary nodules were detected in a significantly greater number of lung lobes using CT than using thoracic radiography. Only 9% of CT-detected pulmonary nodules were identified on thoracic radiographs. The smallest nodules that were consistently seen in CT images were approximately 1 mm in diameter, whereas the smallest nodules that were consistently seen in radiographs were 7–9 mm. Based on these results the authors advised that thoracic CT should be considered in any patient with neoplasia that has potential for pulmonary metastasis, particularly when accurate characterisation of the extent and distribution of pulmonary metastatic disease affects therapeutic planning.
Clearly, CT is a more sensitive test for pulmonary nodules than radiography, but is it sufficiently sensitive that the possibility of metastasis can be ruled out when the CT findings are normal? No – other studies show that CT is less sensitive for pulmonary nodules than manual palpation at thoracotomy, 94 so CT cannot be used to rule out macroscopic metastasis, and no current imaging method can rule out microscopic metastasis. Therefore, it is rational that patients with tumours likely to metastasise are treated for metastasis regardless of the imaging findings. Hence, despite increased sensitivity compared with thoracic radiographs, CT may not affect management of these patients.

Images from a 12-year-old male retriever that had perianal adenocarcinoma. (a) CT of the thorax and abdomen to look for metastasis revealed a solitary, 8 mm pulmonary ground-glass opacity compatible with a nodule. The dog received chemotherapy. (b) Repeat CT 10 months later showed no change in size of the lesion, which makes an incidental finding, such as scar tissue, more likely than metastatic disease
Monitoring effects of treatment
Follow-up imaging studies are frequently used to monitor changes in a lesion during a course of treatment, particularly if there is deterioration in clinical signs. When there is a choice of imaging modality, monitoring a lesion over time is best accomplished by using the same modality as used for the original study.
Screening for occult disease
Diagnostic testing is undertaken because of clinical suspicion of disease in an individual patient (or group), whereas screening implies using a test in individuals considered to be at risk of disease in order to identify those affected within a predominantly unaffected population. 98 The aim of screening is generally to identify affected individuals before development of clinical signs, and the potential benefit is easier and/or more effective treatment of the disease, which may lead to reduced morbidity and mortality. The best documented example of screening based on imaging is mammography.99–101
It should not be assumed that screening is beneficial to patients. When the prevalence of disease is low, a positive result is likely to be a false positive unless the specificity of the screening test is unusually high. 102 Screening tests have great potential for harm because of the morbidity that follows unnecessary further testing or treatment of individuals with false positive results.98,101 Advanced imaging modalities are not immune to this problem. 103
Although there are relatively few screening programmes for companion animals (eg, radiography for hip dysplasia), screening for subclinical disease occurs in geriatric health programmes for healthy animals and in comprehensive work-ups for sick animals. For example, the finding of clinically silent neoplasia in 23% of dogs with primary brain tumours prompted a recommendation that screening tests (to look for additional tumours) should be performed before imaging the brain or performing intracranial surgery. 104 We should be cautious about routinely adopting such an approach. Although the incidence of neoplasia in referral practice (about 5%) 82 is higher than in general practice, and incidence increases with age, few patients will benefit from having their work-up delayed to search for unrelated, clinically silent lesions that may never cause clinical signs. As noted earlier, it can be difficult to decide what to do about additional lesions. Inevitably, when another lesion is detected, there is an increased tendency to withhold further work-up and/or treatment for the original condition, with a corresponding increase in mortality. Concentrating on the problem for which the patient presented may seem too simple, but it is preferable to unfocused screening for disease.
Guiding biopsy
Ultrasound-guided and CT-guided biopsy 105 bring virtually the entire body within range of a biopsy needle. Brain lesions revealed by CT may be biopsied using a stereotactic device under CT guidance. 106 For biopsy of brain lesions seen only by MRI, it is necessary to apply fiducial markers to the patient for the scan; these markers are used to register the MR images to a biopsy guide, which is attached after the patient has been removed from the MRI controlled area. 107
Imaging to reassure the clinician and patient/owner
Clinicians may sometimes feel pressured by owners into requesting tests in order to appear to be continuing to work on a patient while definitive tests are pending. Similarly, when a clinician knows that a CT scan is the appropriate imaging test for a patient but is unable to schedule this without some delay, they may request an ultrasound scan instead because it is available, even though it is superfluous.
Medical practitioners in litigation-prone environments spend a considerable amount of money ordering imaging studies primarily to avoid accusations of medical negligence. 108 This behaviour applies not only to novices, but also to experienced practitioners, who might be expected to have the most confidence in their own diagnostic skills and judgement. In this scenario, imaging is undertaken for the benefit of the practitioner and not the patient.
Misuse of diagnostic imaging
Misuse of diagnostic imaging primarily means unnecessary imaging (see box on page 493). Debatably, use of diagnostic testing in human medicine is excessive; 109 hence, unnecessary imaging may be one example of a generic problem. Unnecessary diagnostic testing has various undesirable effects including increased morbidity from harmful and unnecessary secondary testing and inflation of medical costs. Compared with other diagnostic tests, unnecessary use of advanced imaging has the greatest potential to inflate medical costs. 110
Arguably, skills in history taking and physical examination may suffer if practitioners rely too much on imaging or try to use imaging as a short cut to diagnosis. Imaging cannot be a short cut to diagnosis if it is misdirected because of deficient physical examination.
In the UK, it is a legal requirement that doctors who refer patients for radiography must provide sufficient clinical information to establish the justification for the procedure and should be aware of the efficacy of the examination, where evidence is available. 111 The Royal College of Radiologists publishes a pocket guidebook 112 on the appropriate examination for different clinical scenarios. Such guidance is necessary because many radiological investigations requested for human patients are ineffective and result in unnecessary patient exposure. 113 Equally, guidance may be used as a basis for assessing the quality of a clinical practice based on the proportion of inappropriate imaging studies. 114

There is currently no comparable guidance for veterinary surgeons in the UK. For example, the justification for radiography of veterinary patients falls outside the scope of the guidance notes produced by the British Veterinary Association for the safe use of ionising radiations in veterinary practice. 115 In academic referral hospitals, it is usual to hold regular clinical review meetings at which clinicians, radiologists, pathologists and others can review and discuss approaches to patient management, including optimal use of imaging. To hold such meetings is clearly good practice, 116 but this is less likely to occur in a non-academic setting.
In the future, there may be a role for veterinary insurance companies in providing guidance about use of advanced imaging. For example, the cost of MRI might be excluded from insurance policies for patients with conditions that lend themselves to radiography or for which imaging is considered a low-yield procedure. Conversely, early use of MRI might be advocated for certain clinical presentations if it is shown to reduce overall costs by avoiding unnecessary surgery, as has been reported for knee injuries in people.117,118
Unsafe diagnostic imaging
The risks to human patients associated with exposure to x-rays are integrated into guidance about use of clinical imaging. For example, the relatively high radiation dose associated with CT scans of the abdomen, and the need to avoid unnecessary x-ray exposure of a fetus, are emphasised. 112 In veterinary medicine, exposure of the patient to x-rays is not considered as important. Nevertheless, certain imaging procedures may be contraindicated on the grounds of patient safety, such as MRI of an animal with a pacemaker or metallic foreign body. 119 Ferromagnetic material within the body is potentially unsafe for MRI because it is liable to be moved or heated by interactions with the magnetic field. 120 Even with implanted microchips or surgical implants that are relatively safe because they are made of non-ferrous metal (eg, titanium alloy), artifacts may occur that render images uninterpretable.121–123
Conclusions
Advanced imaging modalities offer the possibilities of increased sensitivity and diagnostic confidence, but there is a need for more clinical research to measure their accuracy and determine how they should be used in order to optimise their impact on patient management. Without such research, it will be difficult to justify the increased costs associated with advanced imaging. In the meantime, veterinarians should be selective in their use of advanced imaging and continue to make use of effective lower cost options.
Footnotes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this article.
Conflict of interest
The authors declare that there is no conflict of interest.