
Abstract
Diagnosis of Histoplasma capsulatum infection in cats traditionally relies upon identification of organisms in circulating monocytes or in tissue specimens from affected organs. In this retrospective study, results of a urine antigen assay were compared with standard diagnostic methods in cats with clinical signs suggestive of histoplasmosis. Antigenuria was detected in 17/18 cats with a histopathologic or cytopathologic diagnosis of histoplasmosis. This preliminary evaluation of the Histoplasma urine antigen test suggests it may be a useful aid in diagnosing this disease in cats.
Introduction
Histoplasma capsulatum is a soil-borne dimorphic fungus, found in temperate and subtropical areas. Infection occurs via inhalation of the microconidia, and is followed by hematogenous and lymphatic spread. 1 Cats appear to be susceptible hosts and disseminated disease is the most common clinical presentation in affected animals. Clinical signs may be non-specific, but include anorexia, depression, and weight loss. Pulmonary involvement is common, and may result in dyspnea or abnormal findings on thoracic auscultation. Enlargement of the liver, spleen, and lymph nodes may be evident, and ocular or osseous involvement may be noted.2–6
Establishing a diagnosis of histoplasmosis traditionally relies upon demonstration of the organism in circulating monocytes or within phagocytic cells in affected organs.1,7 These diagnostic methods have substantial limitations, including misidentification of other intracellular inclusions as H capsulatum, and the need for invasive procedures to obtain suitable specimens. Patients must be restrained or sedated in order to collect tissue samples, and morbidity due to anesthetic complications, hemorrhage, or iatrogenic infection may arise.
Fungal culture may be used to verify a cytologic or histopathologic diagnosis, but often requires several weeks for isolation and identification of the organism. Conversely, the organism may be missed by routine cytopathologic and histopathologic methods if organism numbers are low, or overlooked if an unsuitable stain is used.
Serologic tests for antibodies against Histoplasma species are generally regarded as an unreliable way to identify infected cats, with a risk of false-negative results in patients with active disease. Seroconversion takes 2–6 weeks in infected humans, and may not occur before the patient seeks medical care. 8 In earlier studies, only two of six cats with histoplasmosis were seropositive using immunodiffusion methods, and only four of nine were positive using complement fixation tests.3–6 Conversely, prior exposure and recovery may result in a false-positive serologic result in cats with clinical disease due to other disorders. Although molecular-based methods using polymerase chain reaction are likely to be faster than culture, more sensitive than traditional serologic tests, and more specific than simple visualization of the organism, such tests are not presently available for routine clinical use in cats.
In patients with active infection, Histoplasma species antigens are released into affected tissues and enter body fluids, including plasma, urine, and cerebrospinal fluid. 9 In the last decade, detection of cell wall galactomannan antigen in blood, urine, or other body fluids has been used routinely to identify disseminated histoplasmosis in human patients. 8 This test has been shown to be a reliable diagnostic modality in this species, with a reported sensitivity of 90% for patients with progressive disseminated disease and 80% with those with acute pulmonary histoplasmosis.10,11 Cross reactivity is nearly complete in blastomycosis (~95%), slightly less so in paracoccidioidomycosis and systemic infection caused by Penicillium marneffei (~80%), common in coccidioidomycosis (~60%), uncommon in aspergillosis (~10%), and absent in cryptococcosis.10,12,13–15 Specificity has been well characterized in humans and is >95% for patients with non-myoctic diseases using current methods for antigen detection.10,12,16,17 It should be noted, however, that a recent review stressed that the urine antigen test should not be used as the sole basis for establishing a diagnosis of histoplasmosis in humans. 12
Although this antigen test is now available for use in veterinary patients, there is little information regarding its utility in the routine clinical diagnosis of feline histoplasmosis. The goal of this study was to provide a preliminary assessment of a Histoplasma species urine antigen test (MiraVista Diagnostics) in cats with histopathologic or cytopathologic confirmation of histoplasmosis.
Materials and methods
A database search at the testing facility (MiraVista Diagnostics, Indianapolis, IN, USA) identified all feline submissions for the Histoplasma species urine antigen assay from three veterinary hospitals. Antigen assays were performed by an enzyme-linked immunoassay method, as previously described. 10 Any detectable antigen was classified as a positive result.
Medical records at the three institutions were reviewed, and information was collected regarding clinical complaint(s) and additional diagnostic findings (eg, cytologic and histopathologic results, or necropsy examination).
Information recorded in the medical record was used to determine the infection status of each patient. Cases were classified as having a diagnosis of histoplasmosis if organisms resembling H capsulatum (ie, ovoid or round yeast-like structures, 2–5 µm in diameter, with a central, spherical, lightly basophilic body surrounded by a clear halo) were identified on cytologic or histopathologic examination of blood or affected organs by a board-certified veterinary pathologist or clinical pathologist.1,7 Information regarding staining methods was inconsistently available and was therefore not collected. Cases were classified as negative for histoplasmosis if cytologic or histopathologic evaluation of affected organ(s) did not indicate infection by H capsulatum and an appropriate alternate diagnosis was established.
The sensitivity of the H capsulatum antigen assay in this patient population was calculated using cytopathologic and histopathologic findings as the diagnostic gold standard for infection.
Serial antigen assays were performed in some cats. For these patients, only the results from the initial submission were included in the data analysis.
Results
Eighteen cats had a cytologic (n = 16) or histopathologic (n = 2) diagnosis of histoplasmosis. Confirmatory fungal cultures were not performed in any of these patients. Multiple organs were sampled in many cats, including the spleen, liver, lymph nodes, airways, and eyes. Organisms were most often noted in the spleen (n = 8) and/or liver (n = 4). Seventeen of these 18 cats had a positive result with the urine antigen assay, with antigen concentrations ranging from <0.6 to 39.0 ng/ml (median: 4.43 ng/ml) (Figure 1).
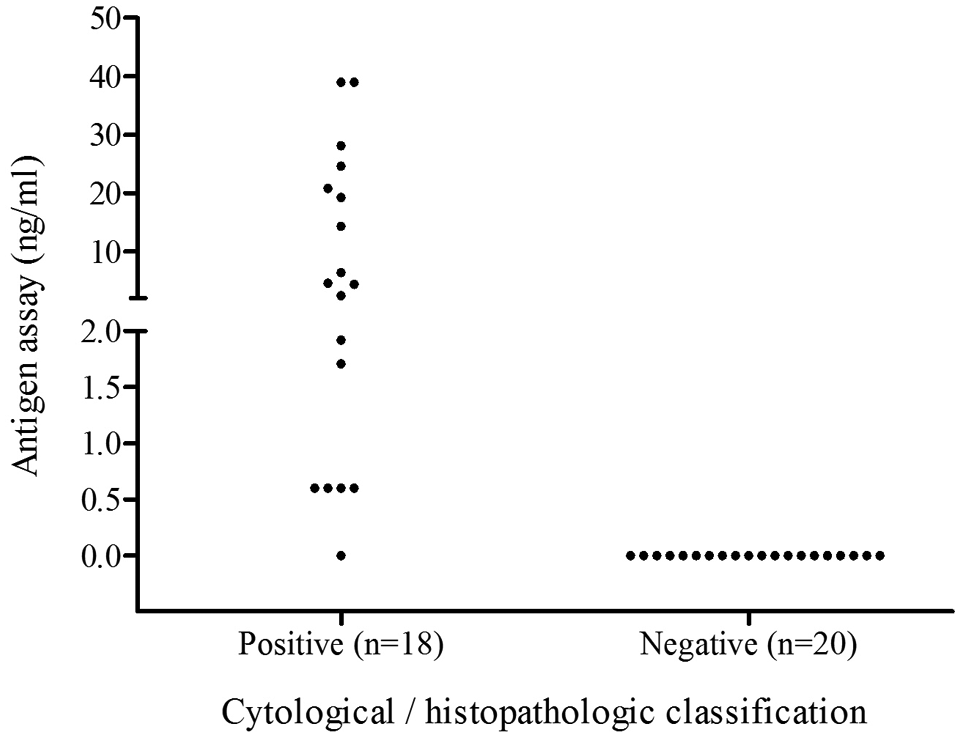
Graph of initial H capsulatum urine antigen assay for 38 cats with suspected histoplasmosis
The one cat with a negative urine antigen result was diagnosed with rectal histoplasmosis on the basis of visual identification of organisms on a mucosal cytologic specimen. No other tissues were examined in this patient, so the extent of organ involvement was uncertain.
Twenty cats were diagnosed with diseases other than disseminated histoplasmosis. Six of these cats underwent necropsy examination; no evidence of fungal infection was reported, although not all tissues were examined microscopically in all cases and special stains were not routinely used. Disseminated histoplasmosis was excluded in the other 14 patients by cytologic (n = 10) or histopathologic (n = 4) examination of affected organs, along with other clinicopathologic findings ± appropriate serologic test results. Final diagnoses for these 20 cases included feline infectious peritonitis (n = 6), non-fungal inflammatory airway disease (n = 4), neoplasia (n = 3), inflammatory bowel disease (n = 2), steroid-responsive stomatitis (n = 1), immune-mediated polyarthritis (n = 1), cytauzoonosis (n = 1), actinomycosis (n = 1), and toxoplasmosis (n = 1). All of these cats had negative urine results for Histoplasma species antigen (Figure 1).
On the basis of these findings, overall sensitivity for the urine antigen assay was 17/18 (94.4%, with a 95% confidence interval of 74.2–99.0%) when compared with the results of routine cytologic and histopathologic testing.
Discussion
This study retrospectively evaluated the diagnostic utility of a urine antigen test for H capsulatum infection in feline patients. Antigen was detected in the urine of 94% of cats diagnosed with disseminated histoplasmosis on the basis of cytopathologic and histopathologic findings, which is similar to findings in human patients.10,12 The findings from this preliminary study suggest that this test may be a useful ancillary diagnostic option in cats with suspected histoplasmosis. False-positive results were not detected in 20 cats with conditions other than histoplasmosis, but the small number of cats undergoing post-mortem examination (n = 6) precludes a reliable evaluation of the specificity of this test and further studies are needed to validate these preliminary findings.
One of the 18 infected cats in this study was falsely negative on urine antigen assay testing. This finding supports those of human studies and indicates that a diagnosis of H capsulatum infection cannot be definitively excluded on the basis of a negative urine antigen assay.11,12 Possible reasons for false-negative antigen tests include low concentrations of antigenuria, antigenic differences within strains, poor specimen handling, or laboratory error. Studies in humans with acute pulmonary histoplasmosis suggest that testing of both urine and serum increases the sensitivity for diagnosis by antigen detection over that of testing urine alone.11,12 Further studies are needed to evaluate serum testing in cats.
A major limitation to this study was the small number of cases with a proven basis for diagnosis. Ideally, a large prospective study requiring independent verification of infection status based on cytologic/histopathologic evaluation of all affected tissues, along with fungal culture and/or molecular identification methods, should be performed in order to provide more information regarding the diagnostic reliability of this Histoplasma species antigen assay.
Another limitation to this study was the reliance on cytologic or histopathologic examination to establish a diagnosis of infection with H capsulatum. In order to reliably determine the diagnostic accuracy of a test result, it should be compared with a true ‘gold standard’. Whilst the strongest evidence for histoplasmosis would be isolation of the organism by culture or by molecular methods, neither of these were performed in any of the cases described here. Although microscopic demonstration of compatible structures in body fluids or tissues is widely regarded as another basis for proven histoplasmosis, it could be argued that infection was not irrefutably proven as other organisms, including Sporothrix schenckii, Candida glabrata, Leishmania species, Pneumocystis carinii, or stain artifact may be mistakenly reported as H capsulatum.8,16
Conversely, some of the Histoplasma-negative cases may have been misclassified, as a full necropsy examination was performed in only 6/20 cases, and not all tissues were examined microscopically in all patients. In addition, small numbers of organisms may have been overlooked on either cytologic or histopathologic examination. Routine Wright or Giemsa’s hematologic stains are usually adequate for cytologic specimens, but staining methods used for tissue sections may substantially impact the identification of organisms. Infection within tissues may be overlooked with routine hematoxylin and eosin stain, and special stains, such as periodic acid-Schiff or Gomori’s methenamine silver, are recommended if fungal disease is suspected.1,7
Despite its inherent limitations, this preliminary study suggests that the Histoplasma species antigen assay may be a useful diagnostic tool in cats with clinical signs suggestive of disseminated histoplasmosis. Timely information may be collected in a non-invasive manner, and may provide guidance regarding further diagnostic options in cats with signs consistent with Histoplasma species infection. However, it is clear from this data that a diagnosis of histoplasmosis should not be discounted on the basis of a negative urine antigen test. Whether testing both urine and serum improves sensitivity over testing urine alone needs to be studied, as reports in human patients with acute pulmonary histoplasmosis suggest that testing both fluids increases the likelihood of antigen detection. 11 Additionally, more information is needed about the specificity of this antigen test in cats with other fungal infections. Prospective studies including large numbers of cats with confirmed Histoplasma species infection and other defined disorders are needed to comprehensively determine the diagnostic reliability of this test in cats.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
Dr LJ Wheat is the President and Director of MiraVista Diagnostics, which currently offers the antigen test described in this study on a commercial basis.
Accepted: 11 July 2011