
Abstract
A retrospective study assessing treatment-related toxicities in tumor-bearing cats treated with temozolomide (TMZ) alone or in combination with doxorubicin was conducted. TMZ was administered orally once a day for 5 days every 3 weeks at a dose of 20 mg/cat. Tumor response was evaluated with standard World Health Organization criteria and toxicity was monitored using veterinary co-operative oncology group–common terminology criteria for adverse events (VCOG—CTCAE) criteria. Ten tumor-bearing cats with various types of malignancies were treated with TMZ-based chemotherapy. Eight cats were evaluable for response. Two cats achieved a complete response, one achieved stable disease and five achieved a partial response. Four grade III and one grade IV hematological toxicities, and one grade IV gastrointestinal toxicity were observed. Four cats were euthanased as a result of apparent toxicity. One cat was euthanased as a result of severe and prolonged myelosuppression with fever. Three were euthanased for grade III pleural and pericardial effusions. Effusion was seen in cats treated with higher cumulative dose of TMZ (P = 0.0046). Planned additional case accrual was discontinued because of unacceptable levels of toxicity despite evidence of efficacy in some of the cats. Additional investigation is needed to elucidate this unexpected apparent cumulative toxicity.
Introduction
The feline species presents particular pharmacologic challenges, especially in regard to cytotoxic chemotherapy. Specific cytotoxic agents have different spectrums of adverse effects in this species compared to those seen in either canine or human patients. In cats, cisplatin causes potentially fatal pulmonary edema by unknown mechanisms. 1 Doxorubicin may be associated with induction of renal damage, 2 although recent literature disputes this assertion. 3 Neither of these toxicities have been reported in other species. The use of 5-fluorouracil results in lethal neurotoxicosis in cats treated by common routes of administration, 4 whilst neurotoxicosis occurs only at higher doses in dogs 5 or with certain drug combinations. 6 Some drugs appear to be less toxic in cats than in dogs. For example, the recommended dose for ifosfamide in cats is almost three times the recommended dose in dogs,7,8 although this may be a result of inefficient activation of the prodrug to the active form in the feline species. Therefore, particular attention to unanticipated adverse events and care in determination of dose are needed when new chemotherapy drugs are explored in feline patients.
Temozolomide (TMZ) is an oral alkylator of the imidazotetrazine family. Its metabolism and mechanism of action are similar to those of dacarbazine (DTIC). Dacarbazine requires activation by the cytochrome P450 system in the liver to the intermediate active state, 5-(3-methyltriazen-2-yl)imidazole-4-carboxamide (MTIC), while TMZ is converted to the active form MTIC by non-enzymatic hydrolysis in the blood. MTIC rapidly breaks down to form 5-aminoimidazole-4-carboxamide (AIC) and the reactive methyldiazonium ion. The methyldiazonium ion methylates guanine residues in the DNA molecule, resulting in the formation of O6-methylguanine. The formation of O6-methylguanine is reported to be responsible for the main cytotoxic effect of both TMZ and dacarbazine.9,10
In humans, dacarbazine is used in the treatment of melanoma, Hodgkin’s lymphoma and sarcomas, whilst TMZ is used for melanoma, metastatic and primary brain tumors, and cutaneous lymphomas.9,10 The use of dacarbazine and TMZ have been reported in dogs. Dacarbazine is used as a rescue therapy for canine lymphoma, either as a single agent 11 or in combination with doxorubicin,12,13 actinomycin D, 13 or lomustine. 14 TMZ has been used in combination with an anthracycline as a rescue therapy for canine lymphoma. 13
In vitro studies demonstrate a synergistic effect when TMZ is used in association with doxorubicin. 15 The combination of doxorubicin with either dacarbazine or TMZ in canine patients has resulted in higher response rates and longer response durations than those achieved with use of dacarbazine as a single agent,11,13 although randomized prospective trials are required to validate this observation. We initiated this pilot study to test the hypothesis that TMZ or the combination of TMZ and doxorubicin would prove safe and efficacious in the setting of rescue therapy for feline refractory lymphomas and other malignancies.
Dacarbazine use has not been reported in cats. This may be a result of the difficulty of determining an effective therapeutic dose arising from the need for enzymatic drug activation in the liver. Hepatic drug metabolism is less well studied in cats compared to dogs and humans. TMZ, as a directly active agent, is therefore an interesting alternative to dacarbazine for use in cats. To our knowledge there are no previous reports of the use of TMZ in feline patients. The goal of this open-phase pilot study was to evaluate toxicity and response to TMZ as a single agent or in combination with doxorubicin in tumor-bearing cats.
Materials and methods
Patient selection
Cats included in this study were ones with spontaneously arising neoplasms presented for treatment to the Animal Care Cancer Clinic at Michigan State University (MSU) between January 2004 and June 2007. Inclusion criteria were: diagnosis of neoplasia based on cytology, histopathology or advanced imaging findings consistent with a diagnosis of intracranial cancer; signed owner consent and complete medical record; and sufficient follow-up data. Cats were excluded if they had an expected survival of less than 1 month or did not complete one cycle of therapy.
Chemotherapy protocol
The dose of TMZ (Schering-Plough) was 20 mg/cat administered orally at home once a day for 5 consecutive days every 3 weeks. Cats were either treated with TMZ as a single agent or in combination with doxorubicin. Cats that received concurrent doxorubicin were treated on day 1 of TMZ administration. Doxorubicin (Adriamycin; Bedford Laboratories) was administered at a dose of 1 mg/kg diluted in 50 ml of 0.9% NaCl administered IV over 25 min through an indwelling IV catheter.
Combination with doxorubicin was used for sarcomas and rescue therapy for lymphoma, while single agent therapy was selected for cats with tumors limited to the central nervous system (CNS) and tumors with no response rates to doxorubicin reported (mast cell tumor and melanoma).
Complete blood count was performed on days 1, 7 and 21 of a 21-day cycle. Additional diagnostic tests, such as serum chemistry panel, urinalysis and thoracic radiographs, were performed at the discretion of the clinician.
Evaluation of response
Standard World Health Organization response criteria were used to assess response in cats with measurable disease. A complete response (CR) was defined as disappearance of all measurable disease for at least 21 days. A partial response (PR) was defined as >50% but <100% reduction in size of all measurable disease for 21 days. Stable disease (SD) was defined as <50% reduction in measurable disease for 21 days with no new lesions arising during that time period. Progressive disease (PD) was defined as >25% increase in measurable disease or the appearance of new lesions. Transient decreases in measurable disease that persisted for <21 days were defined as PD.
Toxicity
Veterinary co-operative oncology group–common terminology criteria for adverse events (VCOG-CTCAE) toxicity criteria were used to grade gastrointestinal, hematological or other toxicities. 16
Statistical analysis
Statistical analyses were performed with standard software (MedCalc for Windows). A frequency table and χ2 test procedure was used to determine whether toxic events were equally distributed among cats that received different cumulative doses of TMZ. The χ2 test for trend was used to test whether a linear correlation between the cumulative dose of TMZ and the incidence of toxicity existed. The Spearman’s rho rank correlation coefficient was calculated to evaluate the degree of association between the cumulative dose of TMZ and toxicity. Values of P ≤ 0.05 were considered significant.
Results
Ten tumor-bearing cats were treated with a TMZ dose of 20 mg/cat administered once daily for 5 consecutive days per cycle. Four cats were treated with TMZ single agent (two cats with mast cell tumors, one with lymphoma with CNS involvement and one with malignant melanoma). Six cats were treated with TMZ/doxorubicin combination (five cats with refractory or relapsed lymphomas and one cat with hemangiosarcoma). Four cats with refractory or relapsed lymphomas treated with TMZ/doxorubicin combination and the cat with suspected CNS lymphoma treated with single agent TMZ also received concurrent prednisolone. Seven cats were male and three were female. Breeds represented were domestic shorthair (seven) and one each of domestic medium hair, domestic longhair and Maine Coon. Median age was 11.85 years (range 4.3–14.7) and median body weight was 4.51 kg (range 3.34–7.05). The median dose of TMZ was 73.85 mg/m2 (range 61.9–109.3) and cats received a median of one cycle (range 1–10). The median cumulative dose was 511.25 mg/m2 (range 309.5–3695). The demographics of this population are summarized in Table 1.
Demographics of the patient population
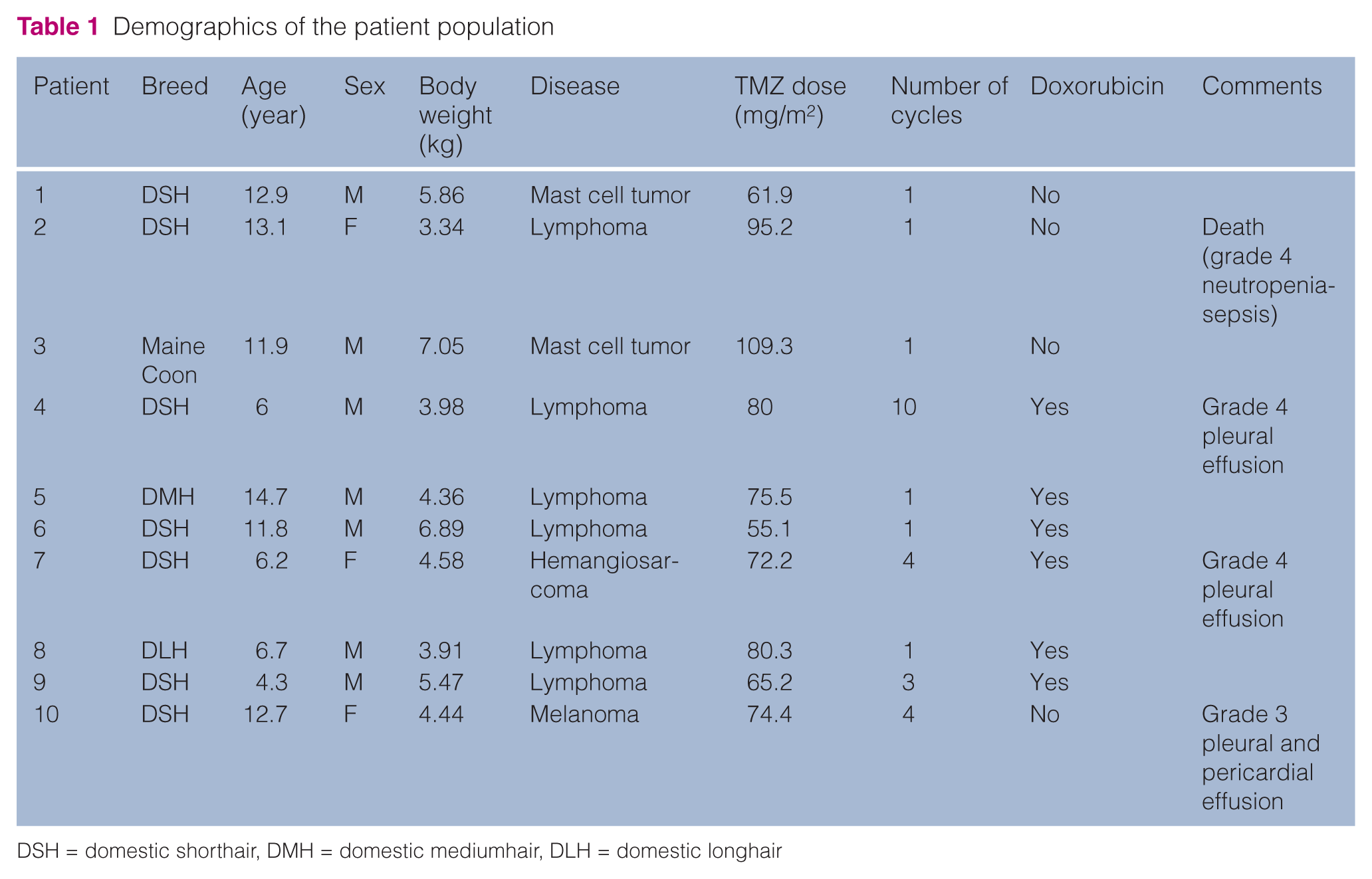
DSH = domestic shorthair, DMH = domestic mediumhair, DLH = domestic longhair
Cats had been treated before accrual to the study with a median of three chemotherapeutic drugs (range 0–7). Cats had failed a number of previous chemotherapy drugs, including vincristine (seven), cyclophosphamide (six), doxorubicin (five), L-asparaginase (five), mechlorethamine (two), procarbazine (two), vinblastine (one), lomustine (one), cytosine arabinoside (one) and cladribine (one).
Eight out of 10 cats were evaluable for response. Excluded from the response assessment were one cat with subcutaneous hemangiosarcoma treated in an adjuvant setting and one cat with malignant melanoma treated with concurrent palliative radiation therapy to local tumor. Two cats evaluable for response achieved CR, whilst one had SD and five experienced PD. All CRs and SDs were observed in cats with refractory or relapsing lymphoma: the two cats with CRs also received doxorubicin and prednisolone and had clinical remissions lasting 22 and 273 days, respectively, and the cat with SD also received doxorubicin but no prednisolone and SD was maintained for 21 days.
Mild gastrointestinal toxicities occurred in two cats. One episode of grade 1 vomiting was reported in each of these two cats. One cat was treated with TMZ as a single agent, while the other was treated with the doxorubicin/TMZ combination.
Eleven episodes of neutropenia were recorded: four grade I, three grade II, three grade III and one grade IV. These episodes occurred in five different cats. Three of these cats were treated with a doxorubicin/TMZ combination and two were treated with TMZ as a single agent. One cat was euthanased as a result of febrile grade IV neutropenia after receiving TMZ as a single agent. The cycle of TMZ was started 10 days following a lomustine treatment because of significant progression of CNS signs caused by lymphoma. This cat had complete resolution of neurologic signs, but the owners elected euthanasia because of the adverse event. Two episodes of thrombocytopenia were reported: one episode of grade II thrombocytopenia occurred in a cat treated with TMZ as a single agent and one episode of grade III toxicity was observed in a cat treated with the doxorubicin/TMZ combination.
An unusual potential toxicity noted in this cohort of TMZ- treated cats was the occurrence of significant pleural and pericardial effusions. Three cats were euthanased because of the development of pleural effusions, one of which also developed pericardial effusion. Two of these cats were treated with TMZ/doxorubicin combination, whilst the third was treated with TMZ single agent.
The first cat euthanased as a result of pleural effusion was being treated for progressive gastrointestinal large granular lymphocyte (LGL) lymphoma. Complete remission (based on normalization of mesenteric lymph node size measured by ultrasonography) was achieved through the use of a TMZ/doxorubicin combination. After a total of 10 cycles of therapy were administered, pleural effusion was observed incidentally on restaging thoracic radiographs. Thoracocentesis revealed a modified transudate. No abnormalities were found on echocardiography. Chemotherapy was discontinued but no thoracic lymphadenomegaly or infiltrative lung diseases were detected on thoracic radiographs, and no neoplastic lymphocytes were observed in the pleural effusion. The cat was treated with periodic thoracocentesis and survived for 3 months following the onset of pleural effusion until the owner elected humane euthanasia. During this period, fluid analysis was repeated twice with similar findings, making the diagnosis of relapsed lymphoma unlikely. Echocardiography was also repeated and no cardiac abnormalities were described.
The second cat to develop pleural effusion was treated with an adjuvant combination of TMZ/doxorubicin after amputation for subcutaneous hemangiosarcoma of the left hind limb. Four cycles of therapy were administered. The cat was presented for lethargy and increased respiratory effort 3 weeks following the last chemotherapy treatment. Thoracic radiographs revealed a large amount of pleural effusion, mild alveolar pattern and thoracocentesis yielded a modified transudate. On echocardiography, severe dilation of the right ventricle with mild tricuspid regurgitation and a small amount of pericardial fluid were seen. Treatment with furosemide was instituted resulting in initial improvement, but thoracocentesis was subsequently required. Five days after adding enalapril to the treatment plan, the cat developed acute renal failure; this improved using diuresis, discontinuing the enalapril and reducing the dose of furosemide. Spironolactone and digoxin were then added to the treatment regimen. Another episode of acute renal failure occurred 13 days later, at which time the owners elected euthanasia.
The third cat that developed pleural effusion was treated with single agent TMZ ( four cycles) and concurrent palliative radiation therapy for an oral amelanotic melanoma metastatic to the submandibular lymph node. Eighty-two days after initiating therapy, the cat was in CR but was presented for signs of respiratory distress caused by marked pleural effusion. Thoracocentesis was performed and 300 ml of a clear, slightly yellow, modified transudate were removed. An echocardiogram revealed significant thickening of the pericardium and pericardial effusion. The owner elected euthanasia based on the grave prognosis. Post-mortem examination of the lungs and heart revealed pericardial adipose tissue and multifocal mesothelial cells with minimal atypia. No significant lesions were noted in sections of the heart. No evidence of neoplasia, infectious agent or significant inflammation were present in any of the examined sections.
Cats with pleural and pericardial effusions received a higher cumulative dose of TMZ (χ2 P = 0.0046; χ2 for trend P = 0.005; Spearman’s rho = 0.732, P = 0.01) than cats that did not develop effusions. During the period of this study, a total of 68 cats with a variety of neoplastic diseases were treated at MSU with doxorubicin at the same dose that was used as described for the cats treated with the TMZ/doxorubicin combination described here. None of these treatments (n = 200) was associated with clinically apparent cardiovascular adverse effects (P = 0.001).
Discussion
The administration of TMZ in combination with doxorubicin and prednisolone induced clinical responses in cats with lymphoma that had been refractory to prior chemotherapy approaches. Single agent TMZ also improved neurologic clinical signs of a cat with refractory lymphoma with CNS involvement. However, we felt it necessary to end the study prematurely because of unexpected apparent cardiovascular toxicity or unexplained thoracic and pericardial effusions. Pleural effusions with or without concurrent pericardial effusions were strongly associated with receiving cumulatively over 1352 mg/m2 of TMZ. No similar adverse effect has been reported in humans or dogs treated with TMZ.
The use of capsule size to determine dose rather than dosing based on body surface area or body weight may have impacted the results of this study. The calculated mg/m2 dose range for the cohort receiving 20 mg/cat ranged from 61.9–109.3 mg/m2. The precedent for this dosing approach in cats was derived from a previous study of lomustine, another oral alkylator, which demonstrated more predictable and shorter duration myelosuppression at a dose of 10 mg per cat when compared with a 60 mg/m2 dose.17, 18
Another limitation of our study is that we have only a temporal association of events between the use of TMZ and the development of pleural and pericardial effusions. The effusions were suspected to be cardiogenic in origin in two cats based on echocardiographic findings. We therefore suspect that the TMZ alone, or in combination with doxorubicin in some cases, induced cardiotoxicity, leading to the observed effusions. Unfortunately, pretreatment echocardiographic studies in these cases was not performed to detect pre-existent but subclinical cardiac abnormalities. The cause of effusion in the third cat did not appear to be of cardiogenic origin. However, it seems unlikely to be related to the cat’s lymphoma or to have arisen from concurrent infection, such as feline infectious peritonitis, based on cytologic analysis of the thoracic fluid. Thus, we strongly suspect that the use of TMZ induced the effusions through an unelucidated mechanism. We base this suspicion on the apparent absence of pre-existing clinical cardiac disease, the lack of evidence for a concurrent infectious disease (lack of fever, character of the effusion on fluid analysis and cytology), the absence of evidence of neoplasia or infection in one post-mortem examination, and the temporal association with administration of TMZ therapy. However, diagnostic tests potentially helpful in determining the underlying cause of the effusions (such as paired serum and fluid triglyceride, and flow cytometry) were, unfortunately, not performed. This is another limitation of our pilot study. Confirmation of our speculation would have been aided by necropsy evaluation to exclude other causes of effusion, but, unfortunately, necropsy was not authorized by all owners. Thus, the underlying etiopathogenesis of the observed effusions remains elusive and toxicity studies in normal cats were not undertaken.
Two of the cats that experienced this toxicity were treated with a combination of doxorubicin/TMZ. Doxorubicin does not generally lead to cardiac disease with heart failure in cats as it does in other species, as evidenced by the study by O’Keefe et al, in which cats treated with 10 cycles of doxorubicin at 30 mg/m2 IV every 21 days did not demonstrate clinical signs of cardiac failure.2,19 It is possible that an interaction between TMZ and doxorubicin may sensitize feline patients to the development of dilated cardiomyopathy, but we feel this is unlikely as none of the cats in our cohort were diagnosed as suffering from dilated cardiomyopathy. The occurrence of idiosyncratic sensitivities to TMZ or the combination would require exploration in a larger cohort size to fully assess any such idiosyncratic effects.
Use of single agent TMZ, or in combination with doxorubicin, is one of the variables in our case series affecting our ability to make a direct correlation between the use of TMZ and this potential toxicity. The combination was used for cats with hemangiosarcoma and refractory lymphoma. This decision was based on the fact that responses have been reported in cats with soft tissue sarcomas treated with a combination of doxorubicin and an alkylating agent, 20 and that doxorubicin is the drug reported to provide a survival advantage in dogs with hemangiosarcoma treated with adjuvant chemotherapy. 21 Our cats with refractory lymphomas were heavily pretreated with various alkylating agents and had a higher likelihood of resistance. As measurable responses occurred in cats treated with the combination only, we feel that this treatment decision was justified. However, the use of the combination may have been contributory to some of the adverse effects we observed.
There is also the potential for interaction with anesthetic agents as a contributor to the toxicities observed in the cat that was treated in combination with radiation therapy for melanoma; therefore, careful monitoring may be indicated in the management of TMZ-treated cats requiring inhalational anesthesia with oxygen as part of the treatment protocol.
The hematological and gastrointestinal toxicities observed in this limited case cohort were judged to be acceptable. Only one cat required hospitalization for hematologic toxicity and was euthanased at the owner’s request because of neutropenia with apparent sepsis. This cat had received treatment with lomustine 10 days prior to attempt salvage treatment with TMZ for rapidly progressing neurologic signs from CNS lymphoma. The recent prior administration of another known myelosuppressive chemotherapy drug is thought to have contributed to the magnitude of myelosuppression in this case. This event may also be attributable to an interaction between TMZ and lomustine, as has been reported in people. 22 The synergism between lomustine and DTIC has also been exploited in dogs, where this combination has been employed as a rescue protocol for canine refractory lymphoma. 14
TMZ might ultimately prove to be beneficial for the treatment of cancer in cats, especially in patients with refractory lymphoma. However, additional investigation is needed to evaluate the apparent correlation of TMZ cumulative dose with cardiovascular toxicity or thoracic effusion before the use of TMZ can be recommended as a clinically useful therapy for feline cancer patients. Traditional dose-escalation studies in normal cats for pharmacokinetic and toxicity assessment might be helpful, as adverse effects might be a function of a species specific effect as is seen with other cytotoxic agents in cats. A standardized phase I study with controlled monitoring of respiratory and cardiovascular function in normal cats followed by a cohort of tumor-bearing cats would help in determining if TMZ is the causal agent of pleural and/or pericardial effusion. We felt compelled to communicate the possibility of pericardial and pleural effusions arising as a consequence of TMZ treatment in cats to aid investigators in designing appropriate toxicity monitoring points for future clinical studies of the agent.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.
Accepted: 19 March 2012