
Abstract
The feline nasopharynx
For the purpose of this review, nasopharyngeal disease is defined as any condition affecting the respiratory tract from the level of the nares to the nasopharynx (Figure 1). While published studies have looked at the incidence of various causes of nasopharyngeal disease,1–3 the overall prevalence of nasopharyngeal disease in the feline population as a whole is unknown; however, it is recognised as a common presenting problem in feline medicine.
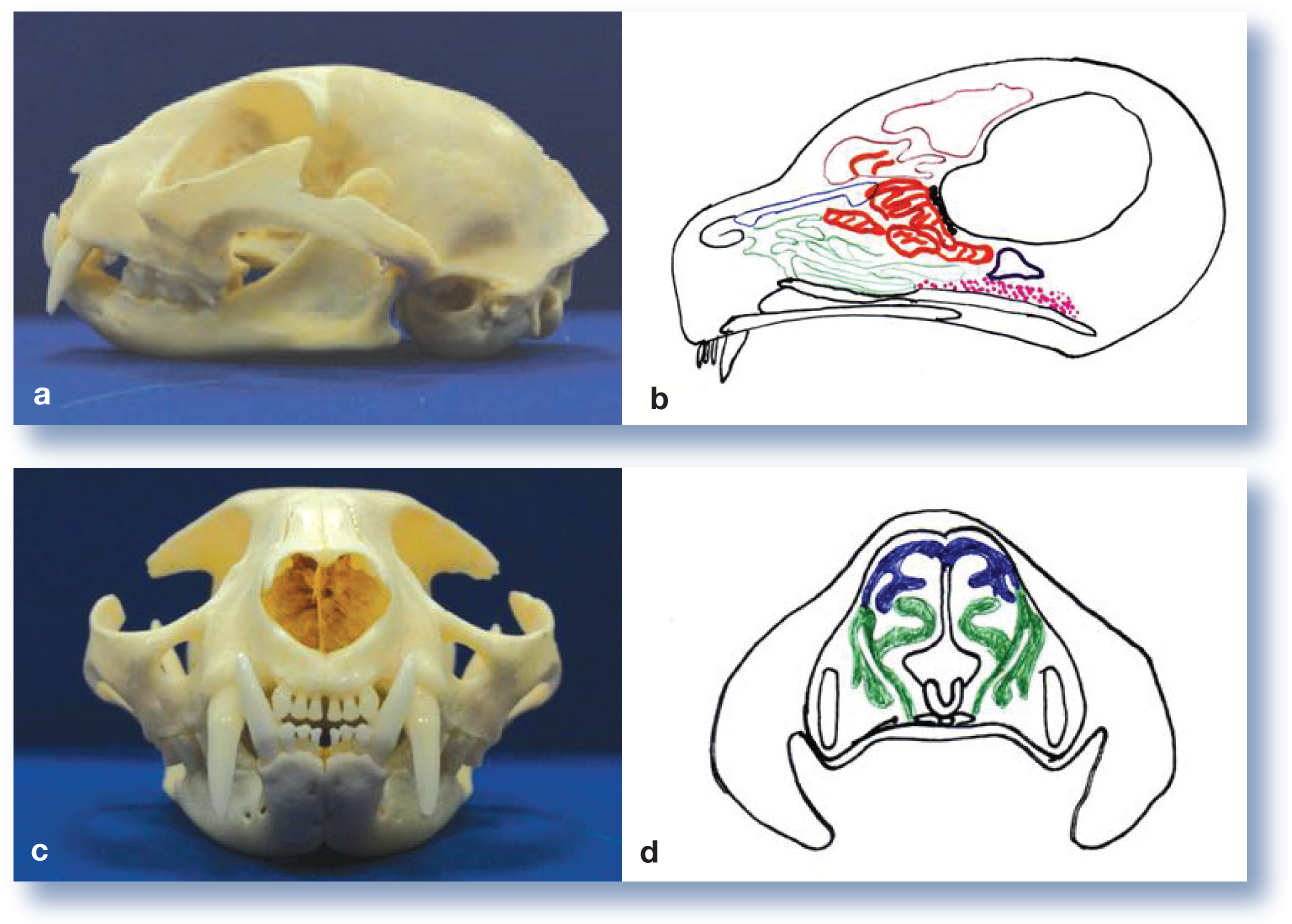
Anatomy of the feline nasopharynx. (a) Lateral view of the skull. (b) Diagrammatic representation of a sagittal section through the skull to demonstrate the turbinate bones: blue = dorsal turbinates; green = ventral turbinates; red = ethmoturbinates; pink = nasopharynx; brown = frontal sinus; black = cribriform plate. (c) Rostral view of the skull. (d) Diagrammatic representation of a transverse section through the skull at the level of the canine tooth: blue = dorsal turbinates; green = ventral turbinates
Aetiology
Clinical signs of nasopharyngeal disease may be associated with a wide variety of underlying conditions (Table 1). The signalment can be of help in evaluating the aetiology: congenital defects will usually cause clinical signs within a few days of birth; ‘cat ‘flu’ is seen most frequently in older kittens; and neoplasia is seen most typically in middle-aged and older cats. While breed rarely has a bearing on upper respiratory tract disease, the authors have seen nasal polyps (inflammatory polyps of the nasal turbinates) most frequently in Oriental breeds, and these cats may be at increased risk of nasal lymphoma.4–6 Frustratingly, in cats with signs of nasal disease an underlying aetiology is often not identified, leading to a diagnosis of ‘chronic rhinosinusitis’.
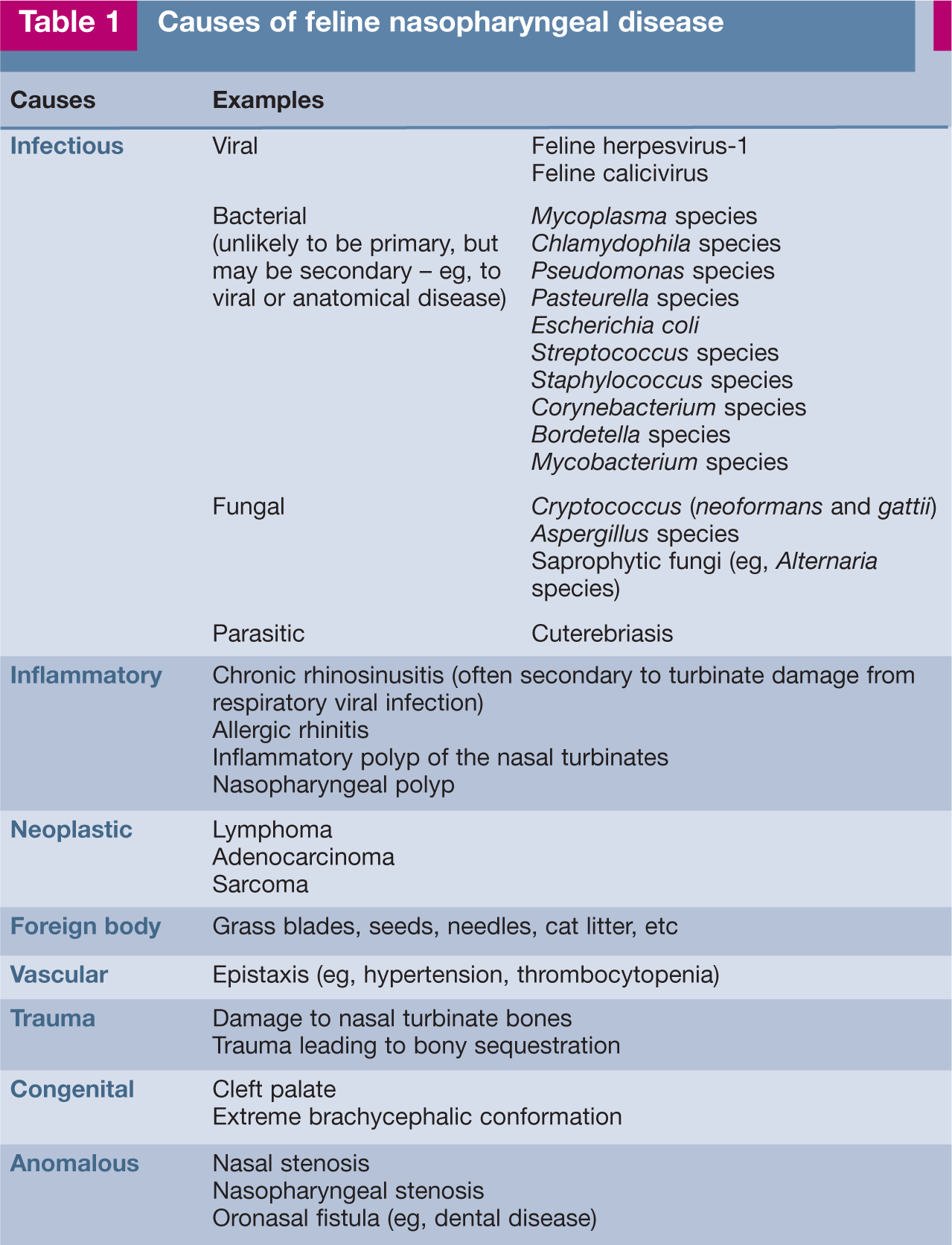
Causes of feline nasopharyngeal disease
Clinical signs
Clinical signs seen with nasal disease may include nasal discharge, stertor, sneezing, epistaxis and epiphora. Diseases of the nasopharynx may give rise to reverse sneezing, gagging or dysphagia. Diffuse disease may produce a combination of these signs, and inspiratory dyspnoea may be a feature of disease at either location. Facial deformity may be seen with neoplasia, severe chronic rhinitis or fungal rhinitis (Figure 2). Halitosis may be an indicator of dental disease or a foreign body. Stridor, by contrast, is typically associated with laryngeal or tracheal disease. Laryngeal disease may also result in dysphonia. (For definitions, see box on page 315.)

Facial deformity in a cat with mycobacterial infection. Courtesy of E Robertson

History and physical examination
A large amount of important information can be gained from the history (see box on page 307). Specific features of the physical examination should be noted (see left). This should enable the clinician to establish whether the problem is affecting the upper or lower respiratory tract, and whether it is primarily located in the rostral nasal cavity, or if the more caudal nasopharynx is involved. Alternatively, diffuse disease may be present (eg, in an asthmatic cat that also has allergic rhinitis).


Laboratory investigations
Routine haematology, biochemistry and urinalysis
The standard minimum database is rarely helpful in the diagnosis of nasopharyngeal disease. However, particularly in older cats, it enables an assessment of general health status (eg, prior to general anaesthesia).
Infectious disease testing
It is recommended that cats with nasopharyngeal disease are tested for feline leukaemia virus (FeLV) and feline immunodeficiency virus (FIV). However, the retroviral status of a cat may be more useful with regard to prognosis than diagnosis, particularly if it comes from a multi-cat household. Cryptococcal antigen testing may be considered in endemic areas or in the light of suggestive histopathological findings.
Coagulation screen and blood pressure measurement
A coagulation screen should be assessed in patients with epistaxis and, ideally, prior to rhinoscopy (see later). Blood pressure should also be checked if epistaxis is present.
Oropharyngeal and conjunctival swabs
An oropharyngeal sample may be obtained by moistening a swab with saline and rolling it around the oropharynx. Although unusual, the authors have had to perform endoscopy on a cat that bit through a swab during this procedure; care should, therefore, be taken to ensure that the patient is adequately restrained! Conjunctival samples may be obtained by rolling a moistened swab in the conjunctival sac; note that sampling must be performed before fluorescein dye is applied, as this can inhibit viral growth.
The swabs should be submitted for virus isolation (FCV and FHV-1). Viral transport medium is required, and should be obtained from the laboratory prior to submission. Alternatively, the swabs may be submitted for polymerase chain reaction (PCR) analysis; however, very variable results were obtained when samples were submitted to different laboratories for assessment of FHV-1 by this technique. 7 Consideration should also be given to assessing for the presence of Bordetella bronchiseptica, C felis and Mycoplasma species. Different transport media may be required for these organisms and Mycoplasma species may be difficult to culture. Alternatively, samples may be submitted for PCR where available.
Interpretation of results is complex, as recently vaccinated cats or chronic carriers may shed virus without it necessarily being the cause of the clinical signs. Conversely, the intermittent shedding of FHV-1 may produce a negative result, even though this agent is contributing to disease.
Sampling of nasal discharge
With the exception of Cryptococcus species infection, sampling of nasal discharge is rarely useful. Cryptococci have a characteristic appearance of round organisms, surrounded by a lucent halo (Figure 3) when stained with Romanowsky stains, new methylene blue or Gram stain. 8 Cytology in other cases is frequently inflammatory in nature, and cultures typically reveal a mixed bacterial infection of normal nasopharyngeal commensal organisms. 9
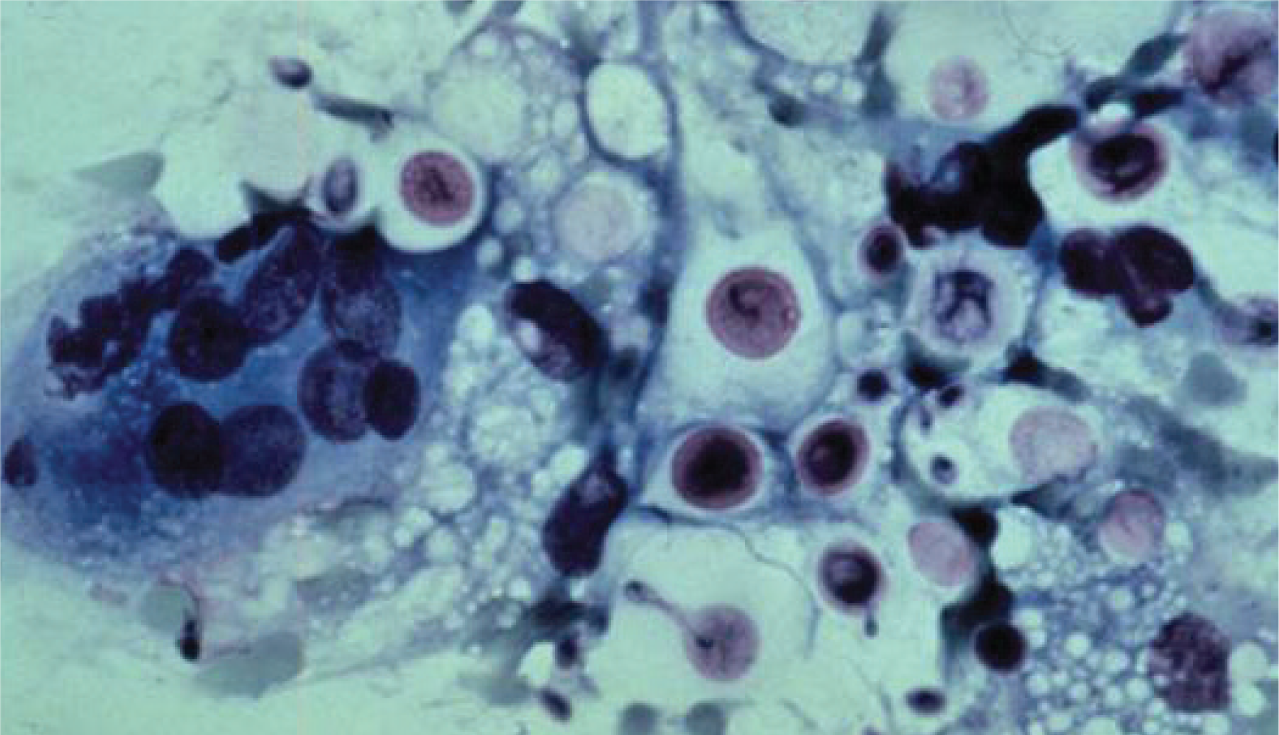
Nasal cytology preparation stained with a modified Romanowsky stain showing dark pink yeast organisms surrounded by a clear halo, characteristic of Cryptococcus neoformans. Courtesy of R Malik
Radiography
Choice of views
Radiographic evaluation should comprise at least the standard lateral and dorsoventral views of the skull, along with targeted views for the area of interest (see boxes on pages 310 and 311). To evaluate subtle changes that may be seen with nasopharyngeal disease, accurate positioning to achieve symmetry is required. As such, general anaesthesia is generally preferred, although care should be taken that, if intubated, the endotracheal tube is not occluded when the neck is flexed for some of the views described. In general, it is preferable to remove the endotracheal tube, as it may be misinterpreted as a lesion on the radiographs.



Assessment
Radiographs should be assessed for:
Presence of dental disease;
Evidence of middle ear disease;
Obstruction of the nasopharynx by soft tissue/fluid opacity;
Soft tissue/fluid opacity within the frontal sinuses;
Loss of integrity of the nasal septum;
Loss of turbinate detail.
Whether any loss of turbinate detail is unilateral or bilateral, and its position within the nasal chambers, may help to localise the disease. The loss of detail may be due to an overall loss of turbinate bone, or an overlying increase in soft tissue/fluid opacity. While the nature of the change should be assessed, it is rarely specific. An overall loss of turbinate bone may be seen with chronic destructive post-viral rhinitis, neoplasia, reaction to a foreign body, or fungal rhinitis. An overlying increase in soft tissue/fluid opacity may be seen with chronic post-viral rhinitis, neoplasia, inflammatory polyps of the nasal turbinates, discharge/fluid within the nasal meati and allergic rhinitis. It should be noted that deviation of the nasal septum is a frequent finding in normal cats.
Radiography should be performed before nasal flushing, rhinoscopy or biopsy procedures, as these techniques may interfere with radiographic interpretation.
Radiographic findings in cats with upper respiratory tract diseases have been reviewed elsewhere.10,11
Examination under general anaesthesia
In addition to facilitating imaging, general anaesthesia allows a more complete physical examination to be performed than is possible in the conscious cat. Before assessing the nasopharynx and nasal cavities, the teeth should be evaluated fully, including probing the sulci and checking for oronasal fistulae. The hard and soft palates should be palpated for the presence of masses, and the oropharynx and tonsils assessed for mass lesions or ulceration.
Evaluation of the nasopharynx
The nasopharynx can be assessed either with or without a flexible (3–5 mm) endoscope.


CT examination of a cat with chronic rhinitis. Transverse sections progress from left to right in a caudal to rostral direction. The images show fluid within the right frontal sinuses, destruction of the nasal septum and, more rostrally, destruction of the nasal turbinates
If no endoscope is available, the soft palate may be drawn rostrally with a spey hook and the nasopharynx evaluated with a dental mirror. Alternatively, a stay suture may be used for retraction of the soft palate. This method requires a good light source.
If an endoscope is available, a gag should be used to prevent damage to the equipment and to facilitate visualisation. The endoscope is advanced into the proximal oesophagus and retroflexed 180° so that the tip is directed rostrally. The endoscope is then withdrawn rostrally, at which point its tip should hook over the soft palate, allowing assessment of the roof and floor of the nasopharynx and the nasal choanae (Figure 5). This procedure is often accompanied by gagging or coughing, which may necessitate deepening of the plane of anaesthesia. Prior application of local anaesthetic to the area may reduce or prevent this response.
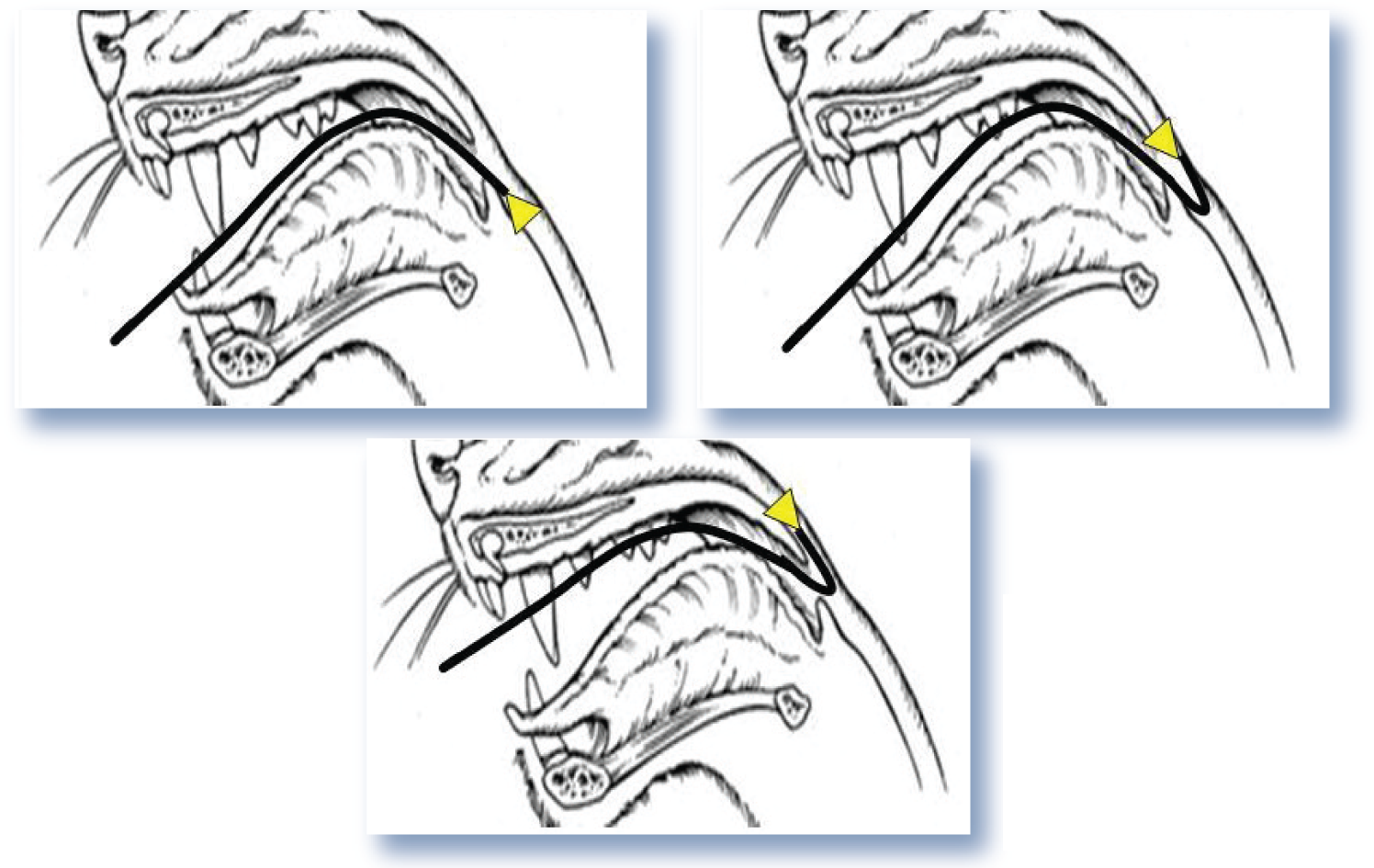
Examination of the nasopharynx with a flexible endoscope. The endoscope is advanced into the proximal oesophagus, then retroflexed 180°, before being withdrawn rostrally so that its tip is lodged dorsal to the soft palate
Evaluation of the nasal cavity
Before investigating the nasal chambers an assessment of coagulation status is recommended, particularly if there is a history of epistaxis, and the caudal oropharynx should be packed with surgical swabs. This is advisable because even minor trauma to the nasal mucosa can result in significant haemorrhage. Primary haemostasis can be assessed with a manual platelet count and buccal mucosal bleeding time. Secondary haemostasis can be assessed by measuring prothrombin time and activated partial thromboplastin time (± measurement of fibrinogen). It is important to prevent any blood from entering the trachea. For this reason it is also advisable to use a gently cuffed endotracheal tube.
While the rostral nasal chambers can be assessed using an auroscope fitted with a small cone, this approach generally affords very poor visualisation. Where available, a narrow (2–3 mm) rigid rhinoscope/arthroscope with a viewing angle of 0–30° is more suitable, and in large cats may even permit biopsies to be collected under endoscope guidance. If secretions obscure the field of view, vigorous flushing with saline via the nares or endoscope can improve visualisation.
When using either a rhinoscope or taking blind biopsies it is important that the instrument is measured against the animal’s face, and marked with a tape tag at the distance from the tip of the nose to the medial canthus of the eye on the same side (Figure 6). This prevents iatrogenic damage to the brain when the instrument is introduced into the nose.

Normograde rhinoscopy. The rhinoscope has been measured from the medial canthus of the eye to the nares, and a tape strip marker applied, to prevent advancement of the endoscope beyond the cribriform plate

Technique for performing a forced flush. (a) The use of forceps facilitates placement of a swab in the caudal pharynx. (b) The pharynx is packed. (c) A 10 ml syringe of sterile saline is applied to the right nostril and the left nostril is occluded. (d) Rapid flushing of the right nasal cavity is carried out

Rhinotomy performed to remove infected turbinates and gain representative samples
Further information on rhinoscopy is available elsewhere.15,16

Summary
Having obtained a complete history, performed a thorough clinical examination and carried out a series of diagnostic investigations, it is hoped that, in the majority of cases, a diagnosis will have been established. Even where no specific diagnosis is achieved, many conditions will have been eliminated from the initial list of possible differential diagnoses.

Footnotes
Key Points
Acknowledgements
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this review article.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.