
Abstract
A 14-year-old male neutered Burmese cat presented for investigation of right fore limb lameness that was non-responsive to anti-inflammatory drugs and opioids. Thoracic radiography showed multiple pulmonary soft tissue nodules and a larger cavitated mass. Right elbow radiographs revealed marked peri-articular proliferation of new bone and periosteal reaction primarily affecting the ulna. Histopathological examination of an incisional biopsy of the right ulna revealed neoplastic proliferation of epithelial cells; this was confirmed as a poorly differentiated carcinoma with immunohistochemistry. Amputation of the right fore limb was performed at the owner’s request. After surgery, radiographs of the limb showed progression of bone proliferation. Repeat pathological analysis confirmed a metastatic carcinoma. The cat deteriorated 3 days after surgery and was euthanased a week later as a result of severe respiratory distress. This case represents an unusual case of metastasis of a suspected primary lung tumour to the ulna in a Burmese cat.
Case Report
A 14-year-old, male neutered, Burmese cat was admitted to a University teaching hospital for investigation of sudden onset non-weight-bearing lameness on the right fore limb. The referring veterinarian had prescribed chondroitin sulphate (Cosequin; Nutramax Laboratories), meloxicam 0.1 mg/kg q24h (Metacam; Boehringer Ingelheim) and buprenorphine 0.02 mg/kg q12h (Vetergesic; Alstoe) for suspected degenerative joint disease. The cat improved in activity but remained severely lame on that limb.
Physical examination revealed a non-weight-bearing lameness of the right fore limb. The elbow was firm, painful and swollen on palpation. Auscultation of the thorax revealed decreased generalised lung sounds and mildly increased respiratory effort.
Haematological analysis revealed low haematocrit [0.25 l/l, reference interval (RI) 0.26–0.47 l/l] and mild lymphopenia (1.43 x 109 /l, RI 2–7 x 109/l). Biochemistry revealed slight hyperproteinaemia (80.6 g/l, RI 60–80 g/l) with hypoalbuminaemia (22.4 g/l, RI 25–45 g/l) and hyperglobulinaemia (58.2 g/l, RI 25–45 g/l). Routine blood tests were otherwise unremarkable.
Radiographs of the chest showed multiple pulmonary soft tissue nodules (mean diameter 5 mm) throughout the lungs and a larger cavitated lung mass (Figure 1a, b). A generalised broncho-interstitial lung pattern was also seen.

Dorsoventral (a) and left lateral (b) thoracic radiographs at first evaluation. There are multiple soft tissue masses (black arrow heads) and a cavitated mass (white arrow head). Diffuse broncho-interstitial pattern is noted in all the lung fields
Radiographs of the right elbow revealed marked peri-articular proliferation of new bone with an irregular, interrupted periosteal reaction along the caudal aspect of the olecranon, medial aspect of the ulna, lateral radius and around the humeral condyle. No obvious cortical destruction was detected (Figure 2). Both elbows had radiographic changes characteristic of degenerative joint disease, with peri-articular osteophytosis and joint mice. Differential diagnoses for the bone lesion in the right ulna were primary bone tumour (osteosarcoma, chondrosarcoma, fibrosarcoma and haemangiosarcoma), metastasis from unidentified primary carcinoma, osteomyelitis (bacterial, fungal), periosteal proliferative arthritis, osteochondromatosis and hypervitaminosis A.

A mediolateral radiograph of the right elbow at first presentation revealed marked proliferation of new bone with no obvious cortical destruction
Arthrocentesis of the right elbow was performed and an incisional biopsy of the right ulna was obtained under general anaesthesia. Analysis of the synovial fluid revealed elevated protein (80 g/l, RI 10–30 g/l) with an increased number of red blood cells (0.1 × 1012/l) and nucleated cells (20.5 × 109/l). Cytology of synovial fluid was consistent with neutrophilic inflammation; no neoplastic cells were identified. Bacteriological culture of the synovial fluid was negative. No fungi were isolated and Ziehl Neelsen staining was negative for Mycobacterium species.
Histological examination of the ulna was suggestive of neoplasia of epithelial origin. This was confirmed by immunohistochemistry, with neoplastic cells demonstrating strongly positive cytoplasmic staining for cytokeratin. On the basis of the histopathological and imaging findings, a diagnosis of poorly differentiated metastatic carcinoma in the right ulna was made.
The cat was discharged and continued on buprenorphine 0.02 mg/kg q12h subcutaneously and meloxicam 0.1 mg/kg q24h, orally. Although the cat’s demeanour improved and no overt respiratory signs were present, the right fore limb lameness persisted. Two months after the histopathological diagnosis of metastatic carcinoma, the owner requested amputation of the limb, which was performed by the referring veterinarian. Radiographs of the right fore limb after amputation revealed significant progression of the lesion. There was an increased amount of new bone formation with an irregular sunburst-type spiculated periosteal reaction around the proximal ulna and evidence of cortical destruction. A pathological fracture of the olecranon was present with associated severe soft tissue swelling.
Histopathological examination of the limb was performed after amputation. The cells were arranged in small acinar structures, interspersed throughout areas of trabecular bone. There was abundant dense fibrous connective tissue associated with the neoplastic cells. The cells lining the acini were cuboidal-to-columnar in shape, with a moderate amount of eosinophilic cytoplasm and a poorly defined margin. The nuclei were round with a finely stippled chromatin pattern and a single nucleolus. The mitotic index was 15 per 10 high-power fields. Throughout the section examined there were large areas of pale staining eosinophilic necrotic bone, as well as areas of necrosis within the surrounding connective tissue. Histopathological diagnosis confirmed an aggressive carcinoma (Figure 3). It was not possible to determine the definite primary site for the neoplasia owing to its poorly differentiated nature, but the two differentials were pulmonary or mammary carcinoma.
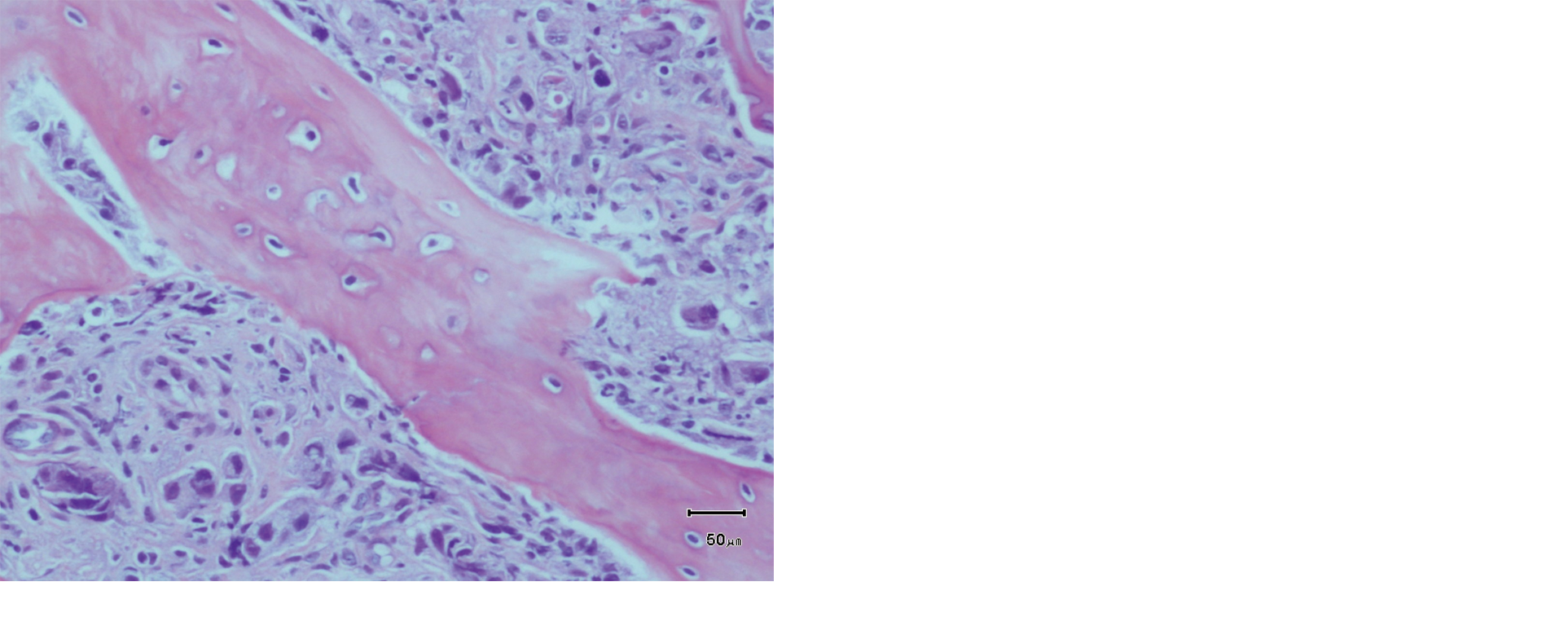
Histological appearance of the right elbow of a cat showing a poorly differentiated metastatic carcinoma affecting the ulna. The cells are forming small acinar structures and clusters, showing epithelial differentiation, interspersed throughout trabecular bone where the bone marrow should be (a) [haematoxylin and eosin (HE); 20×; bar: 50 μm]. The neoplastic cells also involve the soft tissue around the bone, including the muscles (b) (HE; 10×; bar: 300 μm)
The patient deteriorated rapidly 3 days after the amputation. Severe respiratory signs developed and the cat was euthanased a week after the surgery. At the owners request no further radiographs of the chest were taken and a full post-mortem examination was declined.
The differential diagnosis by the pathologist for this poorly differentiated carcinoma within the proximal ulna was metastatic spread from either a mammary carcinoma or a lung tumour. Metastatic spread to the bone is uncommon in cats and is reported most commonly from primary lung cancer. The affected cat was male with no mammary masses either historically or at presentation. The combination of the changes seen on thoracic radiography and the histopathology of the metastatic lesions were strongly suggestive of primary pulmonary neoplasia. The radiographic appearance of the lungs was compatible with a diagnosis of pulmonary adenocarcinoma. Cytology, broncho-alveolar lavage and/or histopathology of the lung masses would have been necessary for a definitive diagnosis.
Seventy-five percent of feline primary lung tumours metastasise to other locations (regional lymph nodes, pleura, mediastinum, bones, muscles, heart, brain, spleen, skin, eyes, or even intravascularly).1–5 In dogs and humans the most common sites for bone metastases for lung tumours are the ribs, vertebrae and proximal long bones; it is less common to have metastases to bones distal to the elbow or stifle.6,7 A syndrome of multiple digital metastases (acrometastases) from primary lung carcinoma in cats has been described in several publications.6–13 The reason for this metastatic spread is still unclear, although it could be the result of tumour emboli passing into small arteries supplying the digits, increased blood flow to the limbs in order to dissipate body heat from the footpads or a result of haemodynamic changes. We are aware of only three other reported sites of skeletal metastases in cats aside from the digits: to the talus from a mammary carcinoma; to the ulna; and to the ribs, sternum and thoracic vertebrae. The last two cases were metastases from a pulmonary adenocarcinoma.6,14,15
In cats, primary lung tumours often have a diffuse distribution and the radiographic pattern may be suggestive of bronchitis, oedema or pneumonia. The adenocarcinomatous pattern in cats is often combined with a mixture of glandular elements and oval-to-spindle cells contributing to the neoplastic mass. This oval cell component has been demonstrated to be of epithelial origin. These tumour types can form cystic spaces lined with stratified layers of epithelial cells, forming cavitary lesions seen on thoracic radiography. 16 This cat presented with a combination of soft tissue nodules and a larger cavitary lesion in the pulmonary parenchyma.
Interestingly, signs of metastatic disease may become evident before signs of respiratory tract disease have developed. 17 The lack of clinical signs in cats with pulmonary tumours may be attributable, in part, to the ability of cats to compensate for the reduced lung function by exercising less. In the present report, the main problem was the persistent right fore limb lameness and there was only a mildly increased respiratory effort on presentation. Clinically relevant respiratory signs only appeared 3 days after amputation, and these signs progressed very rapidly. The precise cause of this was attributable to the suspected primary pulmonary adenocarcinoma; however, it was not investigated as the cat was euthanased owing to the poor prognosis.
Bone metastases are associated with poor survival times. Median survival times for poorly differentiated primary lung tumours are 2.5 months and 23 months for moderately differentiated primary lung tumours. 18 In this case, the cat was euthanased 2.5 months after the onset of the clinical signs and just over 2 months after the histopathological diagnosis of metastatic carcinoma.
It was unfortunate that confirmation of primary pulmonary broncho-adenocarcinoma by histopathological analysis was not obtained in this cat. In the multiple reports on digital metastases in cats, cytological or histopathological confirmation of pulmonary carcinoma was only obtained in eight cases;6,8,9,11,17,19 in the other 49 cases the radiographic changes in the pulmonary parenchyma were considered as a confirmation of the primary lung tumour.6–9,11,17,19
In conclusion, metastatic disease to the bone should be included in the differential diagnosis for lameness in elderly cats, independent of the location of the lesion. Whilst bone metastases in the digits have been described secondary to primary pulmonary tumours, this is the second report where metastatic carcinoma in the ulna of a cat is described. This case is an example of a suspected primary lung carcinoma being the cause of metastasis to the appendicular skeleton in a cat with presenting clinical signs that did not relate to the underlying respiratory disease.
Footnotes
Acknowledgements
The authors would like to thank the referring veterinarian for her help with the follow-up and treatment and the Pathology and Diagnostic Imaging Department of the Queen’s Veterinary Hospital in Cambridge.
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this case report.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.