
Abstract
The clinicopathological and immunohistochemical findings of a primary feline mammary tumour with features similar to human and canine primary inflammatory carcinoma are described for the first time. The cat presented to the clinic for the rapid onset of oedema, severe erythema, local pain and warmth of the inguinal region, with a pustular-to-nodular cutaneous lesion in association with an ill-defined underlying mass. An epithelial malignant tumour was diagnosed by cytological investigation. Necropsy revealed a thickening of the skin with oedema of the subcutis in the right inguinal area, and regional and distant metastases. Histology showed an unencapsulated tubulopapillary proliferation of malignant epithelial cells, with a massive embolisation in the dermal lymphatics and a mild inflammatory infiltrate. Through immunohistochemistry, the tumour was found to be oestrogen (ER)-alpha-, androgen (AR)- and progesterone (PR)-negative; neoplastic cells were ER-alpha, AR-negative and focally PR-positive. An irregular, mild and focal HER-2 immunoreactivity was present (score +1, non-HER-2 overexpressing). The neoplastic cells were cyclo-oxygenase-2 and vascular endothelial growth factor positive.
Case Report
A 9-year-old, common European shorthair breed, intact female cat was presented to the clinic for the rapid onset of an erythema, oedema and papular-to-nodular, non-pruritic, exudative lesions at the right inguinal region (Figure 1a) in association with an ill-defined underlying mass. Local pain was present and the subcutis was firm. The right inguinal lymph node was enlarged and the homolateral hind leg was slightly swollen and oedematous. At physical examination, weight loss and dyspnoea were also noticed. A cytological examination of the mass by fine needle aspiration biopsy was performed to discriminate between a neoplastic or inflammatory process. A population of poorly cohesive epithelial cells, either single or arranged in small cluster with papillary architectures, was observed. The cells were characterised by a variable amount of hyperbasophilic cytoplasm, occasionally microvacuolated and with round, pleomorphic nuclei with irregularly coarse chromatin and prominent, multiple nucleoli. Some inflammatory cells were observed — mainly macrophages and neutrophils. A diagnosis of malignant glandular epithelial tumour was made and the queen was submitted to haematological investigations, a biochemical profile and a radiological evaluation of the thorax. Haematology revealed no abnormalities of the red blood cell line, leukocytosis with increased neutrophil count and lymphopenia. The biochemistry profile showed increased urea and creatinine, as well as elevated levels of aspartate aminotransferase and alanine aminotransferase. Clotting times were within the reference intervals. Radiology of the lungs showed a multifocal micronodular pattern suggestive of a recent metastatic process and an abundant thoracic effusion. A thoracic centesis was performed and cytology showed the presence of numerous clusters of atypical epithelial cells, organised in acinar-to-papillary cytoarchitectures (Figure 2a).

(a) Post-mortem examination of the right inguinal area showing an erythematous and exudative, popular-to-nodular lesion of the skin. (b) Right inguinal lymph node enlargement and diffuse subcutaneous oedema
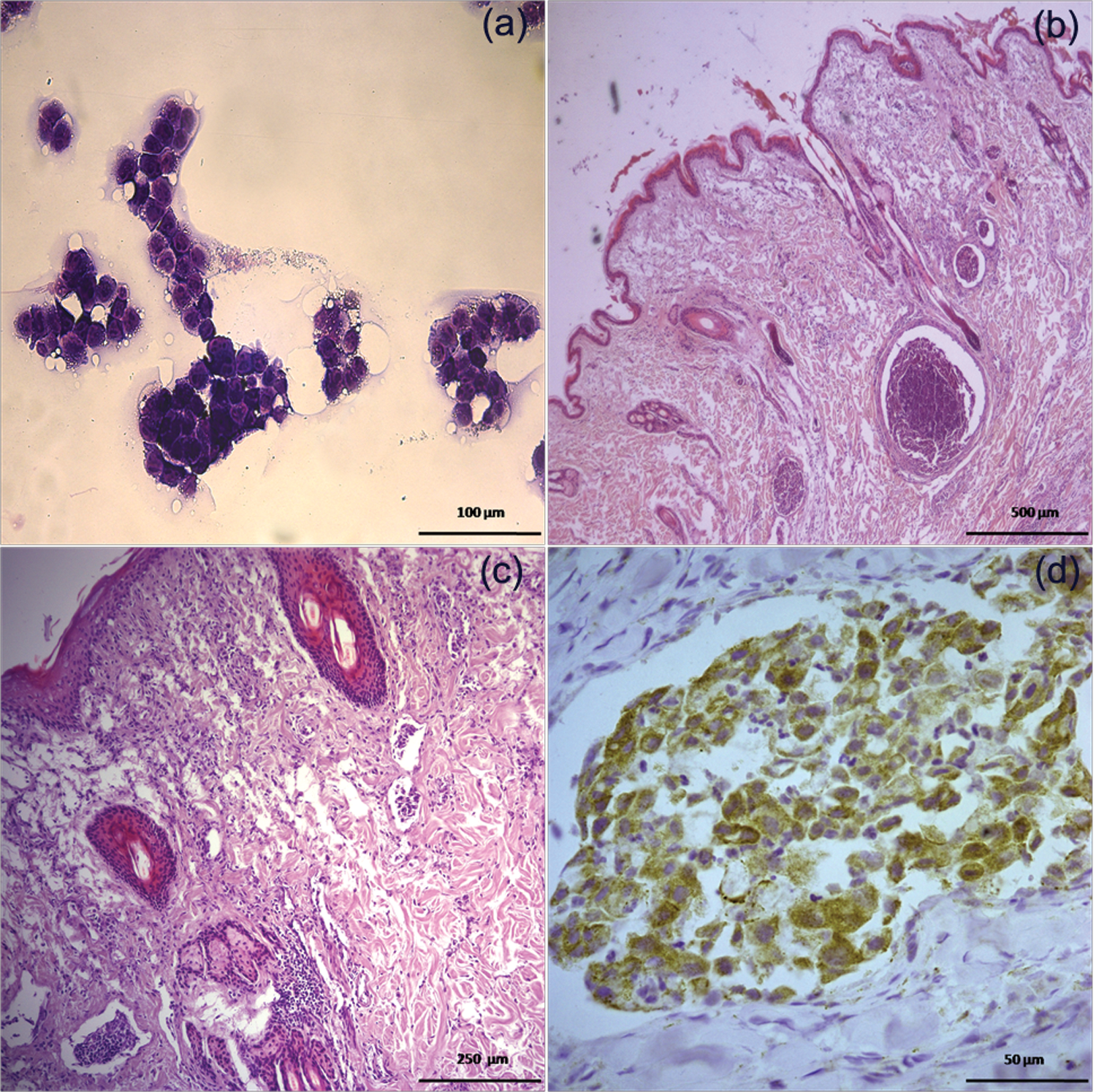
(a) Fine needle aspiration cytology from the mammary lesion showing atypical epithelial cells arranged in small clusters with papillary architectures. Diff-Quik stain (40×). (b) Mammary gland showing an uncapsulated, malignant mammary tumour in the subcutis and neoplastic emboli in dermal lymphatic vessels. Haematoxylin and eosin (H&E) stain (5×). (c) Multiple embolisation of neoplastic epithelial cells in superficial dermal ectasic lymphatic vessel with an interstitial inflammatory infiltrate. H&E stain (20×). (d) Intense cytoplasmic immunoreactivity to VEGF in neoplastic embolised epithelial cells. Streptavidin-biotin-peroxidase, haematoxylin counterstain (40×)
On the basis of the radiological and cytological investigations a diagnosis of pulmonary metastasis of adenocarcinoma and carcinomatosis was made. According to the owners’ decision, the queen was humanely euthanased. Significant gross pathological findings at post mortem were a severe thickening of the skin with oedema of the subcutaneous tissues of the right inguinal area and homolateral inguinal lymph node enlargement (Figure 1b). An ill-defined, non-encapsulated subcutaneous mass was detected. The spleen was slightly enlarged as a result of acute congestion and the liver showed multifocal-to-coalescing whitish nodules unconstantly umbelicated, ranging from a few millimetres to 1 cm in size. Right lomboaortic lymph nodes were enlarged. Abundant serous fluid was observed in the thoracic cavity. Lungs showed multifocal-to-confluent small (less that 0.5 cm in size) nodular lesions scattered throughout the parenchyma. In cross section, the nodules were unencapsulated and the cut surface, usually firm and greyish in colour, showed, in the larger nodules, varied coloration produced by haemorrhage and necrosis. Samples from the skin, inguinal and lomboaortic lymph nodes, spleen, liver and lungs were collected, formalin-fixed and submitted to histological examination according to routine procedures. Light microscopic evaluation of the skin and the subcutis showed the presence of an ill-defined, very infiltrative, proliferation of atypical epithelial cells arranged in a tubulopapillary fashion, with multiple foci of necrosis. A massive dermal embolisation of neoplastic cells in the lymphatic vessels, especially of the superficial dermis, was evident (Figure 2b and c). The lymphatic vessels were often ectasic. A mild fibrosis of the panniculus was detected and a scant inflammatory dermal infiltrate of inflammatory cells (macrophages, neutrophils and small lymphocytes) was observed. Tissues from the lymph nodes, liver and lungs showed the presence of multiple, unencapsulated, nodular proliferations of atypical epithelial cells arranged in tubular to papillary structures. Necrosis was also present.
On the basis of the clinical features, the presence of an ill-defined, poorly differentiated and infiltrative neoplasm with massive embolisation of neoplastic cells in ectasic dermal lymphatic vessels and the presence of inflammatory infiltrate, a diagnosis of primary inflammatory carcinoma (IC) with distant metastases was made. The primary tumour and the metastatic lesions were then submitted to immunohistochemical assays to investigate the oestrogen-alpha (ER), progesterone (PR) and androgen (AR) receptor expression, and cyclo-oxygenase (COX)-2, HER-2 and vascular endothelial growth factor (VEGF) expression. The adopted antibodies had already been used on feline mammary tissues.1–4 A streptavidin-biotin method was adopted. The colourimetric reaction was developed using diaminobenzidine (Impact DAB; Vector Labs). The primary antibodies used were as follows: mouse monoclonal anti-ER (clone 6F11, Novocastra Labs), mouse monoclonal anti-PR (clone PR88; Biogenex Labs), rabbit polyclonal anti-AR (Novocastra Labs), rabbit polyclonal anti-VEGF (Santa Cruz Biotec), goat polyclonal anti-COX-2 (Santa Cruz Biotec) and rabbit polyclonal anti HER-2 (Dako). Tumour cells showed no immunostaining to ER and AR. A focal, weak immunostaining to PR was observed. The percentage of PR-positive nuclei was under the already established 5% cut-off value; thus, the tumour was considered as PR-negative. 2 A mild and irregular membranous positivity to HER-2 was detected and the tumour was thus defined as non-overexpressing this receptor. However, the neoplastic cells were strongly immunoreactive to the anti-COX-2 (score +3) and anti-VEGF antibodies (Figure 2d).
IC is the most aggressive type of mammary tumour in humans and dogs. In humans, IC refers to a special type of locally advanced breast cancer characterised by the rapid onset of a mammary mass with inflammatory signs, such as erythema and oedema, induration of the gland and warmth. IC is not a specific subtype of tumour; however, it is characterised histologically by a massive embolisation of neoplastic cells in the dermal lymphatic vessels and is associated with the presence of a variable amount of inflammatory infiltrate.4,5 IC can be mistaken as an inflammatory process, such as a dermatitis or mastitis, and, as this disease is characterised by a high metastatic potential and short overall survival (usually not more than 1 month after diagnosis), it has to be promptly diagnosed. 6 In a recent study on canine ICs, 86% of the examined dogs had evidence of metastases at the time of the clinical presentation. This may have been caused by the rapid evolution of this disease, as well as by frequent initial misdiagnosis 9 .
In humans and dogs, two subtypes of IC are described: primary IC, with or without an appreciable palpable mass (defined as an ‘occult’ IC), and secondary IC, which occurs after the surgical excision of a previous mammary tumour. 6 Only three cases of feline mammary secondary IC have been described. 7 All three cases were characterised by highly malignant behaviour, poor histological differentiation, dermal embolisation in superficial lymphatic vessels, poor outcome, and metastasis to regional lymph nodes and lungs. Up until now, the present case is the first description of a primary, spontaneously occurring feline inflammatory mammary carcinoma with clinical and pathological features similar to the human and canine counterparts. The rapid onset of the clinical signs, the inflammatory cutaneous condition, the presence of an ill-detectable mass associated with the induration of the skin are features similar to those described in humans and dogs. The histological pattern, with a poorly differentiated invasive mammary tumour associated with a massive embolisation of the superficial dermal lymphatic vessels is comparable to the histological hallmarks of human and canine ICs. The immunohistochemical absence of immunoreactivity to ER and AR, and the low percentage of PR-positive neoplastic cells differs from what has previously been described in secondary ICs in cats, where all cases (three) were PR- and AR-positive, and two out of the three cases were ER-positive. 7
The negative receptor profile recorded may be owing to the particularly aggressive behaviour of the primary IC described herein or to the different methodology adopted to quantify the steroid receptor status. The steroid receptor profile of this neoplasm is, however, in agreement with previous findings in feline invasive mammary carcinomas, 2 where a loss of ER and PR expression has been detected in more aggressive tumours. HER-2 status in feline mammary tumours is still under evaluation; however, our result are not in disagreement with previous reports, where HER-2 status is not associated with tumour histotype or grading. 3 Similar to canine ICs, the neoplastic cells in this case showed an intense COX-2 immunolabelling. 8 Furthermore, the intense immunoreactivity to VEGF suggests, in agreement with previous findings on canine ICs, 4 that feline ICs may be characterised by a high angiogenic phenotype, which explains the poor outcome and high metastatic potential.
Footnotes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this case report.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.