
Abstract
Records of 11 cats with transitional cell carcinoma of the urinary bladder, which had been treated with meloxicam, were reviewed for signalment, duration of clinical signs prior to diagnosis, results of diagnostic imaging, whether or not concurrent surgery was performed and survival. Immunohistochemical expression of cyclo-oxygenase-1 (COX-1) and cyclo-oxygenase-2 (COX-2) was assessed in the tumours of seven cats. Tumour location varied greatly. The cats had a mean age of 13 years. Three cats had a previous diagnosis of feline idiopathic cystitis of up to 2008 days duration. Ten of the cats showed clinical improvement (reduction of haematuria and/or dysuria), with a mean survival time (MST) of 311 days (range 10–1064); 1-year survival of 50%. All seven bladders assessed for COX staining were COX-1 positive and five were COX-2 positive. The MST for the COX-2-positive cats was 123 days, the MST for the COX-2-negative cases was 375 days.
Introduction
Transitional cell carcinoma (TCC) is the most prevalent neoplasm of the urinary bladder in dogs and cats.1,2 The most common tumour location in dogs is at the trigone. 3 However, in the largest study of feline bladder TCC to date, 55% of 20 tumours occurred at sites distant to the trigone. 4
Several risk factors have been identified in dogs, including female gender, breed (Scottish Terrier, Shetland Sheepdog, Fox Terrier, Beagle, West Highland White terrier and Airedale Terriers), obesity, exposure to topical and environmental insecticides, local industrial activity and possibly cyclophosphamide treatment.5–9 However, risk factors are largely unknown in cats, although older cats and male cats appear to be predisposed.4,10,11
In canine studies, treatment may involve surgery and/or medical management. Treatment by surgery alone, using partial cystectomy, resulted in median survival times (MST) of 86 12 and 106 days. 13 However, owing to the trigonal location of TCC in dogs and the difficulty in achieving complete surgical margins, several studies have focussed on medical management. Chemotherapy regimes used in dogs with TCC have included an anthracyclin with a platinum drug; doxorubicin with cyclophosphamide; intravesicular thiotepa; carboplatin with piroxicam; cisplatin; mitoxantrone with piroxicam, gemcitabine with piroxicam; and vinblastine; with MST of 358, 259, 57, 161, <180, 350, 230 and 147 days, respectively.12,14–19 Therapy with the non-steroid anti-inflammatory drug (NSAID) piroxicam given alone resulted in an MST of 181 days in 34 dogs, with six complete/partial remissions and 18 dogs with stable disease. 20 Therapy with another NSAID, deracoxib, given alone resulted in an MST of 323 days in 26 dogs, with four partial remissions and 17 dogs with stable disease. 21
There are few studies on the treatment of TCC of the urinary bladder in cats, with only 48 confirmed cases reported in the literature, of which only 31 have accompanying clinical information.4,10,11,22–32 While it is therefore difficult to draw meaningful conclusions as to the efficacy of different treatment options, the MST in the largest of these studies (n = 20 cats) was 261 days. 4 The majority of cats that were not treated were euthanased at the time of diagnosis.4,11,24,31 However, one cat was euthanased after 10 days, 32 two cats survived 3 weeks10,27 and another survived for 276 days 4 without specific treatment. Cats treated with surgery alone (n = 5) have survived for between 2 days and 6 months.4,10,11 Eight of the cats in the study by Wilson et al were treated with surgery alone or with adjunctive therapy; in these cats the progression-free interval was 89 days. 4 Owing to the demonstrated efficacy of piroxicam in dogs, NSAIDs have also been investigated for the treatment of TCC in a small number of cats. Wilson et al demonstrated survival times of 1, 23 and 208 days with the use of piroxicam alone in three cats. 4
The exact anti-tumour action of piroxicam is unknown. 33 One proposed mechanism is the inhibition of cyclo-oxygenase 2 (COX-2), as this isoenzyme is over-expressed in various neoplasms, including bladder TCC, as seen in all 21 dogs in one study. 34 However, Beam et al demonstrated COX-2 expression in only 37% of feline TCCs, 35 suggesting that COX-2 inhibitors may have less potential as anti-tumour agents in cats compared to dogs. Meloxicam, rather than piroxicam, was chosen in the current study for a number of reasons: it is believed to have more selective inhibition of COX-2 over COX-1 and so may have potentially less gastrointestinal and renal side effects; it has been shown to inhibit proliferation in cell lines (albeit canine) in a dose-dependent manner similar to piroxicam; 33 the authors had experienced significant side effects when using piroxicam in cats in their clinic but had, anecdotally, heard of good responses with meloxicam treatment of feline TCC in other clinics. Meloxicam is relatively safe for the long-term treatment of cats, 36 even elderly cats with concomitant diseases (such as osteoarthritis and stable chronic kidney disease); 37 it is licensed for long-term use in cats in the UK, albeit for the treatment of osteoarthritis.
Therefore, the aim of this study was to evaluate the clinical features and outcome of cats with TCC of the urinary bladder that were treated with meloxicam. Additionally, COX expression in TCC samples was evaluated and related to the clinical response to treatment.
Materials and methods
Clinical information
Clinical records were reviewed for all cats that presented with a urinary bladder mass to the Royal (Dick) School of Veterinary Studies (RDSVS), University of Edinburgh, between January 2001 and February 2008. Additional cases were collected during the same time frame from UK veterinary practitioners who contacted the RDSVS for advice. Inclusion criteria included the presence of a bladder mass identified on radiographic and/or ultrasonographic diagnostic imaging or direct visualisation at surgery, a diagnosis of TCC based on histopathology or cytology, a history of medical management with meloxicam (Metacam; Boehringer Ingelheim) and follow-up information being obtainable.
Data collected included age at diagnosis, breed, gender, duration of urinary tract-related clinical signs prior to the diagnosis of TCC and previous diagnoses if known, clinical signs at presentation, method of diagnosis, location of mass within the urinary bladder and size of the mass, whether metastases were detected, duration and dose of meloxicam therapy, history of concurrent surgical treatment, response to treatment, presence of concurrent urinary tract infection or evidence of renal failure, duration of survival and cause of death. The symptom-free interval (SFI) was defined as the time from initiation of treatment to the first episode of urinary-tract related signs. This and the MST were calculated using the Kaplan-Meier product limit method. Information for follow-up was determined by examination of the case records or by email communication with the referring veterinarians.
COX immunohistochemistry
Archived formalin-fixed, paraffin wax-embedded tissue blocks, where available, were retrieved from the pathologists who made the original definitive diagnosis. The original histopathological diagnosis was re-confirmed by one of the authors (TJS). Any drug treatment (including NSAIDs and glucocorticoids) administered prior to biopsy was ascertained from medical records.
Positive control samples comprised formalin-fixed, paraffin wax-embedded normal feline bladder mucosa and feline fetal kidney stained with antibodies to COX-1 and COX-2, respectively. The choice of control tissues was based on previous studies.34,38–41 Additionally, bladder tissue from five cats that had been euthanased as a result of non-urological disease had COX-2 immunohistochemistry performed.
Immunolabelling and scoring were performed using the technique of Hayes et al 41 and briefly comprised microwaving antigen retrieval at pH 6, followed by automated labelling (Techmate Horizon; LJL Biosystems), using a standard, two-layer indirect method (EnVision; DakoCytomation). Chromogen staining was developed with diaminobenzidine and slides were counterstained with haematoxylin. Polyclonal rabbit anti-ovine COX-1 antibody (Cayman Chemical) at a 1 in 400 dilution, plus a negative control comprising normal rabbit immunoglobulin fraction (DakoCytomation), diluted 1 in 8000 was used for the COX-1 arm. For COX-2 immunolabelling, the primary antibody (Polyclonal Anti-PGHS-2 Human C-terminus) was diluted 1 in 800. A specific pre-immune serum (Oxford Biomedical Research), diluted 1 in 800, was used for negative control purposes. A further negative control was performed for all samples in both the COX-1 and COX-2 arms, using antibody diluent alone instead of an immunoreactive fraction. Immunolabelling was described as focal (a single area), multifocal, patchy (numerous groups, fairly evenly distributed) or diffuse. A semi-quantitative estimation of the number of immunolabelled neoplastic cells was made and recorded as <1%, 2–10%, 11–50%, 51–75% and 75–100%. Intensity of labelling was categorised as weak (+), moderate (++) or marked (+++); relative to the positive control tissue which was categorised as moderate (++). The intensity of labelling in the nucleus and cytoplasm was recorded separately.
Results
The medical records of 17 cats were examined. Three were excluded owing to lack of definitive diagnosis of TCC, one had insufficient clinical history and two cases were not included because they were not treated with meloxicam. Details of the 11 cats included in the study are given on Table 1 (eight domestic shorthair cats, one Siamese, one Chinchilla Persian and one Abyssinian cat). All cats were neutered; there were seven (64%) male and four (36%) female cats. The median age at diagnosis was 14 years (range 9–18 years; mean 13.1 years).
Details of the 11 cats included in the study

FN = female neuter; MN = male neuter; DSH = domestic shorthair; NP = not performed
Censored at 10 days when the treatment was changed to piroxicam
No recurrence of bladder signs, but died of congestive heart failure at 390 days
The clinical signs exhibited prior to diagnosis included haematuria (10/11; 91%), stranguria/dysuria (8/11; 73%) and acute urethral obstruction (1/11; 9%). One cat had no urinary tract-associated clinical signs; the bladder mass was detected during abdominal ultrasonography performed to investigate vomiting. The median duration of urinary-related clinical signs prior to diagnosis was 61.5 days (range 1–2008; mean 310 days). Three cats had a previous diagnosis of feline idiopathic cystitis (FIC), based on urinalysis and diagnostic imaging, with intermittent clinical signs from 365, 425 and 2008 days prior to the diagnosis of TCC.
Abdominal contrast radiography and/or ultrasonography were performed in 10 of the cats to determine bladder mass size, and extent and location of the mass(es). The remaining cat had TCC characterised by direct visualisation at exploratory celiotomy. Radiography was performed in eight (73%) cats and ultrasonography in seven (64%) cats. Five (46%) cats had both imaging modalities performed. Tumour location varied widely between cats, being craniodorsal 4/11 (36%), cranioventral 4/11 (36%), affecting multiple sites 1/11 (9%), causing diffuse thickening of the entire wall 1/11 (9%) and affecting only the trigone area 1/11 (9%). The trigone was only affected in three (27%) cats.
The diagnosis of TCC was confirmed by histopathology in nine (82%) cats and by cytology of suction catheter biopsies in two (18%) cats. Two cats had neoplastic transitional cells recorded on urine sediment examination. One cat had a prior fine needle aspiration biopsy, which was consistent with the histopathological diagnosis.
Staging for the presence of metastases was performed at the time of diagnosis in six cats. Three cats had both thoracic radiography and abdominal ultrasonography, two cats had only abdominal ultrasonography and one cat had only thoracic radiography. No metastases were detected in any cats at the time of diagnosis.
All cats were treated by oral administration of meloxicam. A mean initial dose of 0.09 mg/kg (range 0.01–0.3) was given q24h for the first 3–7 days and a mean maintenance dose of 0.04 mg/kg (range 0.01–0.1) was given thereafter. For 10 (91%) cats, meloxicam was the primary medical therapy used for treatment of TCC. The cat with acute urethral obstruction was given meloxicam 0.05 mg/kg q24h for the first 10 days of treatment then changed to piroxicam (Feldene, Pfizer)
0.3 mg/kg orally q48h for the following 66 days until euthanasia. This was instituted because of the severity of disease and the previously demonstrated efficacy of piroxicam for the treatment of TCC in dogs. 20 That cat also had a cytostomy tube placed followed by pre-pubic urethrostomy to relieve urinary obstruction. Partial cystectomy was performed in four cats; surgical margins were reported as complete for one cat and incomplete in the other three cats.
Ten of the 11 cats showed clinical improvement. Only the cat with acute urethral obstruction continued to show haematuria and dysuria, although its demeanour did improve. The median SFI was 243 days (range 0–630) for haematuria and 334 days (range 0–630) for dysuria. Possible gastrointestinal side effects were seen as diarrhoea in the cat treated with piroxicam (which resolved in 24 h after missing one treatment dose) and an episode of melaena in a meloxicam-treated cat. One cat developed renal failure after 1 week of treatment with meloxicam and another cat developed renal failure after 6 months of treatment. The first cat had a trigonal tumour and hydronephrosis, so the azotaemia was likely to have been obstructive in origin. Two cats had chronic renal disease at the time of diagnosis, which did not deteriorate appreciably on therapy.
The MST for all 11 cats was 311 days (range 10–1064) and a 1-year survival of 50% (Figure 1). The MST for those cats treated by partial cystectomy and meloxicam 375 days was not statistically different from those treated with meloxicam alone (123 days; P = 0.87).
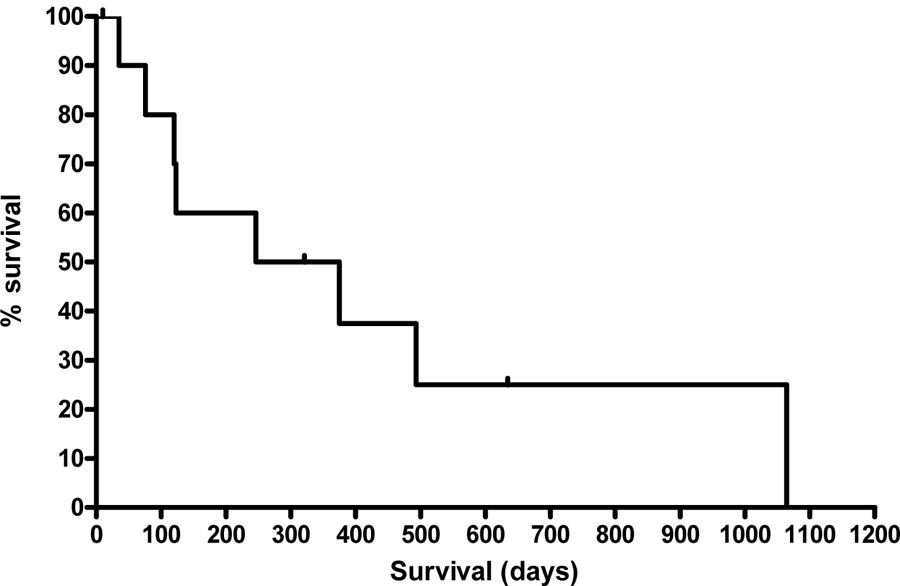
Kaplan-Meier survival curve for the nine cats that died during this study. Mean survival time was 264 days. The short vertical lines represent censored cases: cats 6 and 7 as they were still alive at the time of writing, and cat 9 that was censored at 10 days as treatment was changed from meloxicam to piroxicam at that point
Death in eight out of the nine cats that died or were euthanased was related to the TCC; the remaining patient was euthanased owing to worsening arthritic pain and reduced mobility (cat 7). For those cats where death was a result of complications of TCC, five were euthanased because of recurrence of lower urinary tract-related clinical signs; two were euthanased owing to surgical complications [one because of pre-pubic urethrostomy stoma necrosis (cat 9) and the other as a result of uroperitoneum following partial cystectomy (cat 11)]; one died spontaneously following dyspnoea caused by pulmonary metastases and neoplastic pleural effusion (cat 10).
Post-mortem examination was performed in four (44%) of the cats that were euthanased or died. Three cats had TCC metastases at the time of death: in the lungs, kidney and local lymph nodes in one cat, in the lungs and pleura of another and in the peritoneum of the third cat.
COX immunohistochemistry was performed on TCC tissue samples from seven (64%) cats (Table 2). The TCC of all seven cats were COX-1 positive. Five of the TCCs (71%) were COX-2 positive and two (29%) were COX-2 negative. All of the normal bladder tissue samples from the five control cats were COX-2 negative. Treatments administered within 1 month of biopsy sampling for histopathology included meloxicam (n = 2), meloxicam and marbofloxacin (Marbocyl; Vétoquinol) (n = 1) and no medication (n = 2) for the COX-2-positive cats. One of the COX-2-negative cats received meloxicam and amlodipine (Istin; Pfizer) and the other received pentosan polysulphate sodium (Cartrophen Vet; Arthropharm) and fluoxetine hydrochloride (Prozac; Eli Lilly). The MST for cats with COX-2-positive TCC was 123 days and 375 days for cats with COX-2-negative TCC.
COX-1 and COX-2 staining of seven of the cases

Three cases ++, two cases + to ++
Discussion
This study is the first to demonstrate the clinical features and response to meloxicam therapy (plus or minus surgery) of a group of feline patients with bladder TCC. As this is a relatively rare neoplasm with a paucity of information in the veterinary literature, this study serves to augment the body of knowledge on feline TCC in general. Our findings agree with other studies in a number of areas. Our study confirms that feline TCC is a disease of geriatric cats, with no breed predisposition and a male bias. 4 Also, unlike dogs and humans, our findings suggest that the majority of feline cases do not involve the bladder trigone.4,10 Haematuria is the most common clinical sign, with urination abnormalities, such as dysuria, stranguria and pollakiuria, also being prevalent,4,10 as our results demonstrate.
In previous studies, the median duration of clinical signs prior to diagnosis was 28 days,11,25,29–32 compared with 2 months in our case series. Three cats in the current study had a prior diagnosis of FIC, with clinical signs having been present over a prolonged period. While it is important not to over-interpret these findings when the numbers are so small, it could potentially be speculated that these were cases of TCC with a very long time course that had been originally misdiagnosed. However, it would seem unlikely that a cat with TCC would survive between 1 and 5.5 years. Alternatively, it could be postulated that the chronic inflammation from FIC predisposed the cats to the development of TCC. There is a well-documented link between chronic inflammation and the development of some cancers in both animals and humans. 42
In the current study, cats with TCC that were treated with meloxicam therapy (with or without surgical extirpation) had a MST of 8 months (311 days). This compares to canine patients treated with piroxicam having a MST of 181 days, 20 or those treated with deracoxib having a MST of 323 days. 21 Survival times of our cats treated with meloxicam were similar to those achieved by Wilson et al (MST 261 days); 4 however, their 20 cats were treated with chemotherapy, piroxicam, surgery or a combination of these modalities, so it is difficult to compare treatment options as there was an insufficient number receiving each treatment to allow for direct comparison.
Our data suggest that meloxicam may have a role to play in the palliative management of TCC in the urinary bladder of the cat. Further studies will be required to improve our knowledge of this drug’s efficacy in feline TCC and to determine whether a combination of NSAIDs and cytotoxic agents could confer a survival advantage, as seen in dogs given piroxicam and mitoxantrone (reported median survival of 291 days). 17
Meloxicam inhibits COX enzymes, preferentially inhibiting COX-2 over COX-1. As COX-2 is over-expressed in many neoplasms, including canine TCC, 34 we were interested in investigating whether COX-2 was over-expressed in the TCCs in our cases and whether COX-2 expression was associated with a positive response to therapy with meloxicam. In order to document over-expression, we first had to determine the level of COX-2 expression in normal feline bladder. None of the five normal bladder samples showed any COX-2 expression. However, COX-2 was over-expressed in the majority of our TCC cases (2/7; 71%), which was notably higher than previously documented (37%). 35 The level of expression was low (<1%), similar to that for feline oral squamous cell carcinoma using the same methodology. 41 In the month prior to the biopsies being collected, three of the cats found to be COX-2-positive and one of the cats found to be COX-2-negative had received meloxicam. These numbers are too small to be able to say whether or not meloxicam affected COX-2 staining.
The survival time for the meloxicam-treated cats was longer in COX-2-negative cats compared with COX-2-positive cats. Confirmation of this unexpected finding would require a larger study. If, however, this finding is supported by future studies, it might indicate that the potentially beneficial effects of this NSAID may not be mediated by COX-2-regulated mechanisms. Indeed, other anti-neoplastic mechanisms of NSAIDs have been proposed, including the induction of apoptosis, interference with cell-cycle progression, stimulation of immune surveillance and reduction of carcinogen activation or anti-angiogenic effects.42,43
In conclusion, we present the details of 11 cats with TCC affecting the urinary bladder, their clinical presentation and diagnostic findings, and their clinical outcome following treatment with meloxicam (plus or minus bladder surgery). The cats had a MST of 311 days which suggests that meloxicam may have a role to play in the palliative management of TCC in the urinary bladder of the cat
Footnotes
Acknowledgements
The authors would like to thank Ron Lowe, Andrea Harvey, Bridget O’Farrell, Geraldine Hale (NationWide Laboratories), Caroline Allen, Claire Devitt, Jeremy Hopkins, Elliot Beattie, Robina Logan and Andy Armitage who provided case material for this report. Thanks also to Richard Mellanby and Jodi Miller for their technical support.
Funding
We would like to thank both The University of Edinburgh Development Trust and The Animal Health Trust for funding the immunohistochemistry.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.
Accepted: 22 February 2012