
Abstract
Two 12-year-old cats were diagnosed with chronic kidney disease (CKD) based on physical examination, clinicopathologic data and, in one case, abdominal ultrasound findings. Approximately 1 year after the initial diagnosis of CKD both cats developed renal transitional cell carcinoma (TCC) — bilateral in one cat. Based on post-mortem examination, one cat had no evidence of metastasis and the other had metastasis to the large intestine, heart and lungs. This is the first report of de novo bilateral renal TCC in a cat, as well as the first report of renal TCC developing in cats with previous history of confirmed CKD.
Case Report
Chronic kidney disease (CKD) is common in cats and is observed with an increased frequency in aged cats. 1 In contrast to CKD, feline renal transitional cell carcinoma (TCC) is rare. 2 Humans with end-stage renal disease have an increased incidence of malignancy, including renal neoplasms. 3 In Asia and Western countries, the most common upper urinary tract cancer in patients on dialysis is TCC and renal cell carcinoma, respectively.4, 5 There have been no reports documenting the coincidence of CKD and malignancy in the veterinary literature. This case report describes two aged cats that were diagnosed with CKD and which subsequently developed renal TCC.
Case 1, a 12-year-old, castrated male, domestic shorthaircat was presented for evaluation of suspected CKD based on a history of polydipsia for several months and azotemia being detected on a routine serum biochemistry screening. On physical examination the cat was normally hydrated, had a body condition score of 2.5/5 and had bilaterally small kidneys on abdominal palpation. Azotemia superimposed on a minimally-concentrated urine sample was confirmed (Table 1). A fundic exam was unremarkable and abdominal ultrasound findings included bilaterally hyperechoic renal cortices and irregular kidney margins with decreased cortico-medullary definition. There was slight (0.2 cm) pelvic dilation of the left kidney with a linear hyperechoic shadowing structure within the renal pelvis (suspected nephrolith). A urine aerobic bacterial culture had no growth and a serum total thyroid hormone concentration (TT4) (21.3 nmol/l) was within the reference interval (10–45.5 nmol/l). Indirect systolic blood pressure measured by Doppler was 155 mmHg. Treatment recommendations included gradual transition over 14 days to a prescription renal diet (Hill’s prescription diet feline k/d). At recheck 17 days later, the azotemia was unchanged; International Renal Interest Society (IRIS) 6 CKD stage 2, non-proteinuric, borderline hypertensive CKD was diagnosed based on these findings. Benazepril (2.5 mg PO q24h) was started for borderline hypertension (165 mmHg). Two weeks later the cat represented with a 3-day history of vomiting and excessive grooming behavior. The skin on the cat’s medial forearms and ventral neck and thorax was erythematous and excoriated. Although no histopathology was performed, a drug reaction was suspected and the benazepril discontinued. Two weeks later the vomiting, erythema, and excoriations had resolved and Rubenal (Vetoquinol USA, Fort Worth, TX, USA) treatment (75 mg PO q12h) was started.
Clinicopathologic parameters case 1. Système International units with common units in square brackets

PCV = packed cell volume, CREA = creatinine, BUN = blood urea nitrogen, PHOS = serum phosphorous, USG = urine specific gravity, UP/C = urine protein to creatinine ratio, iBP = indirect Doppler blood pressure, TT4 = total thyroxine concentration, TX = treatment, ND = not determined.
Over the next 9 months, the CKD progressed to IRIS CKD stage 3 (non-proteinuric, borderline hypertensive), the cat lost weight and the body condition score decreased to 2.0/5. A follow-up TT4 was normal and an aerobic bacterial urine culture had no growth (Table 1). Approximately 1 year after the initial evaluation, the cat presented with anorexia and intermittent vomiting. Azotemia had markedly increased (Table 1); aerobic bacterial urine culture had no growth and systolic blood pressure was 150 mmHg. The kidneys were similar in size compared with the previous abdominal ultrasound (right kidney was 3.8 cm in length compared with the previously-measured 3.67 cm and the left kidney was 4.0 cm in length compared with the previously- measured 3.8 cm). The previously-noted hyperechoic cortices and the decreased cortico-medullary distinction appeared unchanged. The location and size of the previously-suspected left pelvic renolith was also unchanged. Two days of intravenous fluid therapy to replace deficits and provide maintenance needs failed to improve the azotemia and the owner elected euthanasia.
On post-mortem examination, grossly both kidneys had irregularly indented cortices; the left kidney measured 3.5 × 2.5 cm and the right kidney measured 3.5 × 2 cm (Figure 1). On histological examination, the pelves of both kidneys were lined by multiple layers of neoplastic transitional epithelial cells. Multiple foci of neoplastic cells extended into the renal medulla and cortex as solid sheets or nests of cells. Discrete islands of closely packed neoplastic cells had destroyed and replaced normal renal tissue and elicited marked desmoplasia in areas of tumor growth. The neoplastic cells had indistinct cell borders with a moderate amount of pale, eosinophilic cytoplasm. The nuclei were round with finely stippled chromatin and a single prominent nucleolus. There was marked anisocytosis and anisokaryosis with 14 mitotic figures in 10 random 400× fields. These neoplastic cells occasionally formed small pseudocysts filled with a small amount of necrotic debris (Figure 2). Within the renal parenchyma surrounding the neoplasm, the glomeruli were multifocally and globally shrunken and sclerotic, with marked thickening of Bowman’s capsule. There was marked degeneration, regeneration, tubular ectasia, loss of tubules and thickened tubular basement membranes, with occasional intratubular protein casts. The interstitium contained multifocal aggregates of lymphocytes and plasma cells admixed with moderate amount of interstitial fibrosis. There was no gross, or histologic, evidence of additional neoplasia within the urinary tract or other organs.

Case 1. The cortical surface of both kidneys had multiple indentations and the right kidney was shrunken. There was no gross evidence of neoplasm in both kidneys

Case 1. High magnification of kidney section showing characteristic neoplastic transitional epithelial cells with a pseudocyst (*) surrounded by abundant mucinous fibrous connective tissue (arrow heads)
Case 2, a 12-year-old, castrated male, domestic longhair cat was presented for evaluation of polydipsia/polyuria and weight loss of 3 months duration. Body condition score was judged to be 4.5/5 and the kidneys were small and firm on abdominal palpation; indirect systolic blood pressure was 140 mmHg. The total thyroid hormone concentration was within the reference interval at 36.3 nmol/l. The owner elected not to return for follow-up serum biochemistry, abdominal imaging and urine protein/creatinine ratio, which were scheduled for the following week. Treatment recommendations included gradual transition to a prescription renal diet. Four-and-a-half months later, the cat had lost 0.4 kg of body weight and serum creatinine and indirect systolic blood pressure had increased (2.6 mg/dl and 160 mmHg, respectively; IRIS 6 CKD stage 2 with borderline hypertension). Approximately 13 months after the initial evaluation for CKD, the cat presented collapsed with pale mucous membranes. Packed cell volume was 11% with a total protein of 9.0 gm/dl. The owner declined further diagnostics/treatment and the cat was euthanased.
On post-mortem examination, grossly both kidneys had irregularly indented cortices; the left kidney measured 3.5 × 2.5 cm and the right kidney measured 4 × 3 cm. The left kidney had a firm, white, subcapsular nodule measuring 1 × 2 cm (Figure 3). The serosa of the descending colon had a 0.5 × 0.3 cm firm, white nodule. All lung lobes had multifocal irregular firm, white nodules on cut surface. The heart contained pinpoint white nodules on the epicardium of the left ventricle and a 5.0 × 3.0 cm white nodule in the intraventricular septum which extended from the endocardium into the myocardium. On histologic examination, the left renal pelvis was lined by multiple layers of neoplastic transitional epithelial cells that extended into the renal parenchyma as multiple foci of neoplastic cell aggregates. The neoplastic cells had similar cellular morphology as described in case 1, with metastasis to serosa of the colon, lung and heart. The focal subcapsular nodule in the left kidney was microscopically consistent with TCC. Both kidneys had chronic degenerative changes, as described in case 1. There was no gross or histologic evidence of additional neoplasia within the lower urinary tract.

Case 2. The cortical surface of the left kidney had a focal subcapsular nodule (arrows) measuring 1 × 2 cm
Of the 21 reported cases of feline renal TCC, bilateral disease has been reported in one cat.2,7–11 In this cat, bilateral disease was believed to be caused by metastasis as there was also metastasis to other organs. 7 To our knowledge, case 1 described here is the first reported case of bilateral de novo renal TCC in a cat. The diagnosis of bilateral de novo renal TCC was made because of the absence of renal vascular invasion, as well as distant metastasis. In addition, both cases are the first reported to have well-documented physical and clinicopathologic evidence of CKD for approximately 1 year prior to the diagnosis of renal TCC.
Renal TCC arises from the renal pelvic urothelium and at the time of diagnosis has commonly metastasized to distant organs and invaded renal parenchyma and/or perirenal tissue.2, 8, 9 Feline renal TCC is rare, being reported in 3/4393 feline accessions (0.068%) in a necropsy review. 2 There is a paucity of clinical information regarding feline renal TCC, but clinical illness at the time of diagnosis is common. Clinical signs have included vomiting, anorexia and weight loss.9,10 Physical examination may included renomegaly2,8,9,11,12 and pain, but this is not invariably present, and renomegaly or gross deformation of the kidney may be mild. 7
Clinicopathologic parameters case 2. Système International units with common units in square brackets
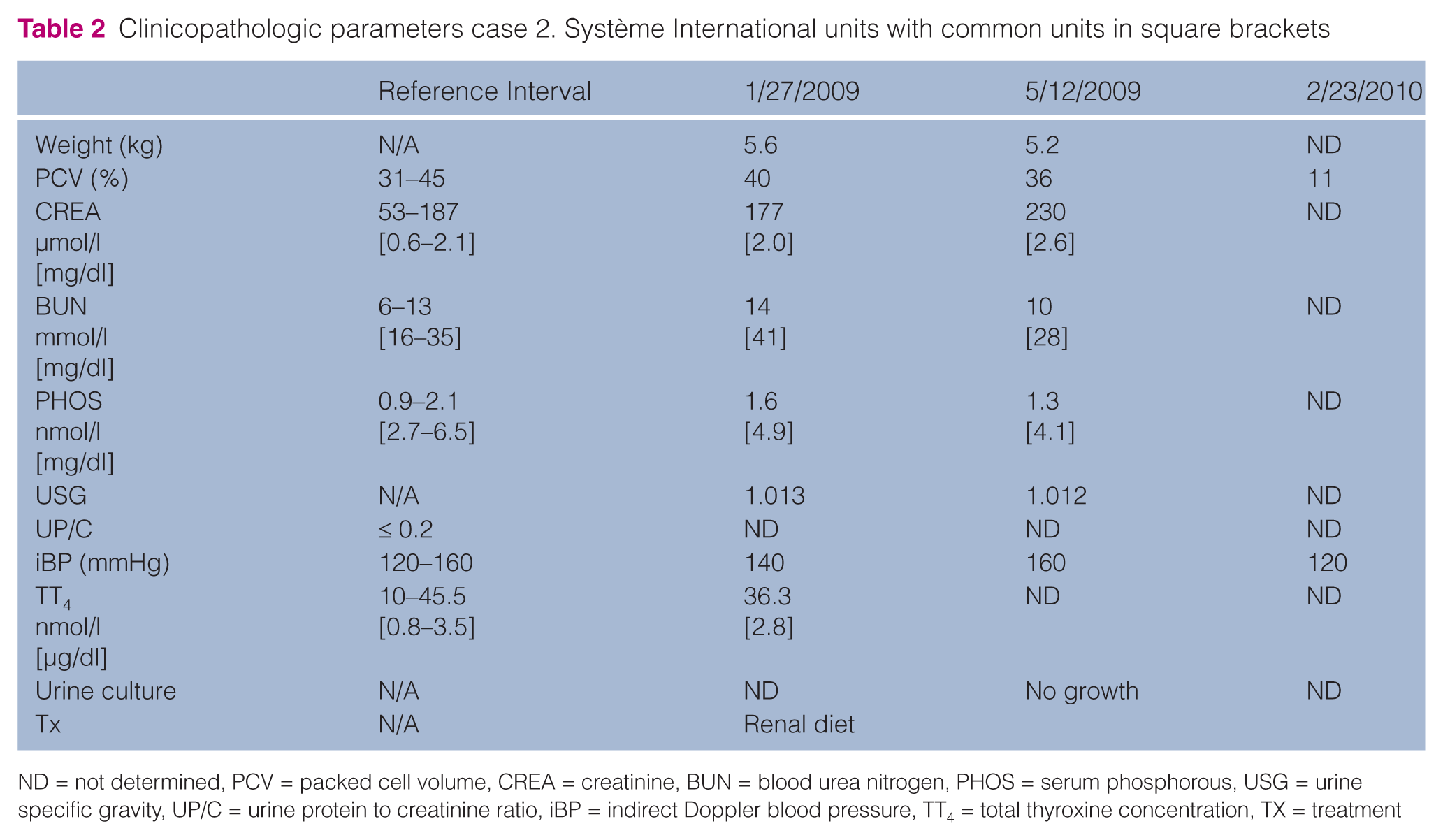
ND = not determined, PCV = packed cell volume, CREA = creatinine, BUN = blood urea nitrogen, PHOS = serum phosphorous, USG = urine specific gravity, UP/C = urine protein to creatinine ratio, iBP = indirect Doppler blood pressure, TT4 = total thyroxine concentration, TX = treatment
Most of the reported cases of feline renal TCC do not provide individual laboratory work or imaging findings, which precludes any presumptuous diagnosis of concurrent CKD, although azotemia, dilute urine and unilateral renal TCC has been reported in two cats.8,12 In the majority of cases, diagnosis was made post mortem and in the remaining cases survival after diagnosis was short.2, 7–10,11,12 The mean age of all reported cases of feline renal TCC, including the two cases reported here, is 10.4 years.8–10,11,12 Because both CKD and renal TCC primarily affect older cats, these two diseases may be coincidentally found in the same cat. Alternatively, CKD or the treatment of CKD may have led to the development of TCC. Humans with end-stage renal disease with and without renal transplant or hemodialysis have an increased incidence of malignancy, including renal neoplasms.3,13–15 Renal TCC is the most common upper urinary tract neoplasm in patients receiving dialysis in Taiwan, which is different than Western countries in which renal cell carcinoma is the most common.4,5 The increased risk for malignant cancer after renal transplant in people is likely caused by immunosuppression and compromised immunological surveillance in addition to genetic, environmental and viral factors.13,14,16 It has been postulated that immunosuppression of chronic uremia independent of renal transplant may also be partially responsible.17,18 Other known risk factors for upper urinary tract TCC in humans include analgesic abuse, the use of Chinese herb containing aristocholic acid (AA) and being a Chinese herbalist.19–21 In one study, Chinese herbalists had a standardized incidence ratio for upper urinary tract urothelial carcinomas of 4.25 (95% confidence interval 2.47–6.80). 21 It should be noted that only case 1 in this report was known to receive a Chinese herbal supplement, Rheum officinale, and this supplement is not known to contain AA or be a carcinogen. The incidence of malignant neoplasia in feline CKD compared withan aged-matched population without CKD remains unknown.
Feline CKD is a slowly progressive disease with long survival expected in IRIS 6 stages 1–3. 22 A major factor in morbidity, mortality, cost-of-treatment and patient quality-of-life is the occurrence of uremic crisis. During these intermittent episodes of clinical illness, cats commonly require parenteral fluid administration in addition to other supportive care. In many cases, an underlying cause to the acute decompensation is not found, although ascending urinary tract infections, acute ureteral obstruction or dehydration secondary to other disease are possible. Both cases presented here had an acute clinical decompensation presumed to be the result of renal TCC, although it is unknown if there was, in fact, worsening renal function in case 2.
The ante-mortem diagnosis of urothelial neoplasia arising from the renal pelvis may be difficult. This was illustrated in case 1 where neoplasia was not suspected, even after abdominal ultrasound had been performed. Irregular kidneys with decreased corticomedullary definition and mild pyelectasia were similar ultrasonographically at first diagnosis of CKD, and 1 year later immediately before the cat was euthanased. As previously mentioned, because renal TCC arises from the renal pelvis, renomegaly and drastic alteration to gross (ultrasonographic) renal conformation may be mild or absent. 7 The difficulty indetecting renal pelvic cancer has been recognized in human medicine where ‘meticulous sonographic evaluation of a hydronephrotic kidney, particularly in older patients, to avoid missing urothelial cancer’ is recommended. 23 In case 1, it is likely that the only means of definitive ante-mortem diagnosis would have been renal biopsy. As invasion into the renal cortex is common,2,8,9,10 routine ultrasound guided renal cortical biopsy may have been adequate. As neither cat was diagnosed ante-mortem, nor are there reports of the treatment of bilateral renal TCC or renal TCC in a cat with concurrent CKD, it remains unknown how ante-mortem diagnosis may have altered the outcome in these two cases.
The cases presented here are the first to report renal TCC and bilateral de novo renal TCC as a probable cause of acute decompensation in feline CKD. In an acute uremic crisis, in feline CKD, if azotemia does not improve with supportive care and the cause of uremic crisis remains undetermined after routine diagnostic investigation, renal TCC should be considered. Risk factors for feline renal TCC, including CKD, are unknown. Further investigation into the incidence of renal TCC and other malignant neoplasms as related to CKD and the treatment of CKD are warranted.
Footnotes
Acknowledgements
The authors would like to thank Dr Bawa Bhupinder for the images and the Kansas State Diagnostic Laboratory for their support. Both cases were seen at the Veterinary Medical Teaching Hospital, Kansas State University.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
Drs Hanzlicek and Grauer are involved in a clinical study funded by Vetoquinol, the maker of the herbal supplement, Rubenal, briefly discussed in this article.