
Abstract
Clinical approach
Monoparetic cats are frequently presented to their veterinarian with the main complaint being lameness. A good knowledge of the motor and sensory innervation of the thoracic and pelvic limb is essential for the diagnosis of neurological causes of lameness or monoparesis (see box below and Table 1).
Spinal cord segments, muscles and cutaneous sensory fields for peripheral nerves of the thoracic and pelvic limbs

The spinal cord segments in brackets contribute to limb innervation in some, but not all, cats
Orthopaedic and neurological examination
A detailed orthopaedic examination should be performed before embarking on the neurological examination. The femoral pulse, as well as colour and temperature of the foot pads, should be checked to evaluate for possible thromboembolism. Each joint, ligament, tendon and bone should be carefully assessed for evidence of pain, restricted range of motion, instability and swelling. For a more detailed discussion of the orthopaedic examination in cats, readers are referred to an accompanying article in this special issue by Kerwin. 1
Is the cat lame or monoparetic?
Strictly speaking, lameness describes abnormal function of a limb or a gait change, caused by a resistance to pain or discomfort. A mechanical lameness relates to a non-painful, abnormal gait due to altered anatomy or range of motion in joints. Lameness often presents as a short stride on the affected limb and long stride on the contralateral limb, and is usually associated with pain from orthopaedic disease. Additionally, it can be associated with nervous system dysfunction referred to as nerve root signature (referred pain down a limb, causing lameness, resulting from entrapment of a spinal nerve, which is usually due to a lateralised disc extrusion or nerve root tumour).
Monoparesis is defined as a loss of ability to support weight (lower motor neuron [LMN] disease) or inability to generate a gait (upper motor neuron [UMN] disease). The term paresis implies that some voluntary movement is still present, as compared with paralysis which refers to a more severe paresis with complete (-plegia) loss of voluntary movement. Monoparesis/plegia is usually caused by a lesion of the LMN innervating the affected limb; very lateralised lesions caudal to the T2 spinal cord segment can also result in pelvic limb monoparesis.
Lameness of neurological origin usually arises from a lesion affecting spinal cord segments C6–T2 for the thoracic limb and L4–S1 for the pelvic limb.
Once orthopaedic causes have been ruled out clinically, the clinician should focus on the neurological examination. Although a complete neurological evaluation is preferable, the all-too-common fractious nature of our feline patients makes this a challenging task. A more targeted neurological examination of a lame or monoparetic cat is often more practical, with particular attention being paid to assessment of gait, postural reactions, segmental spinal reflexes (flexor withdrawal and extensor tone) and muscle mass/symmetry.
Gait evaluation
Gait evaluation should allow differentiation of lameness from monoparesis, as well as UMN monoparesis from LMN monoparesis.
Lameness of neurological origin usually arises from a lesion affecting the spinal nerve (eg, lateralised disc or tumour) at the level of intumescences (ie, spinal cord segments C6–T2 for the thoracic limb and L4–S1 for the pelvic limb). Cats with a brachial plexus tumour can also present with lameness early in the course of the disease before a more typical monoparesis develops later on. LMN paresis manifests as degrees of difficulty in supporting weight, producing a gait abnormality varying from a short stride to collapse of the limb whenever weight is placed on it. UMN paresis causes a delay in the onset of protraction, which is the swing phase of the gait.
Postural reactions
The postural reactions evaluate the cat’s awareness of the precise position and movements of parts of its body (especially the limbs), as well as the cat’s ability to generate movement in the part tested. Paw positioning can be very difficult to assess in cats. Hopping, wheelbarrowing and tactile placing are the preferred postural reaction tests in feline patients (Figure 1). 2 The primary aim of testing these postural reactions is to detect any subtle deficits that were not obvious on gait evaluation. Identification of postural reaction deficits in limb(s) other than the limb showing lameness/monoparesis could indicate the presence of a spinal cord lesion or a polyneuropathy. Differentiation between these two disease locations can be made by evaluation of spinal reflexes and muscle tone/mass.

Paw position testing can be very difficult to assess in cats. The hopping response is, therefore, the preferred postural reaction test in feline patients
Spinal reflexes, extensor tone and muscle mass/symmetry
Each limb muscle should be palpated to detect any focal muscle atrophy. Such findings could indicate disease in the spinal cord intumescence (spinal cord segments C6–T2 and L4–S1), nerve root or peripheral nerve that innervates the muscle, or could be related to disuse atrophy associated with an orthopaedic condition. Following gait and postural reaction evaluation, examination of the spinal reflexes helps to narrow down the lesion localisation by testing the integrity of the C6–T2 and L4–S1 intumescences, the peripheral nerves (respective segmental sensory and motor nerves), and the muscle innervated (Table 1). Although many spinal reflexes are described in the literature, most of them are difficult to perform and interpret in cats. For each limb, the flexor and extensor function should be evaluated (Figure 2).
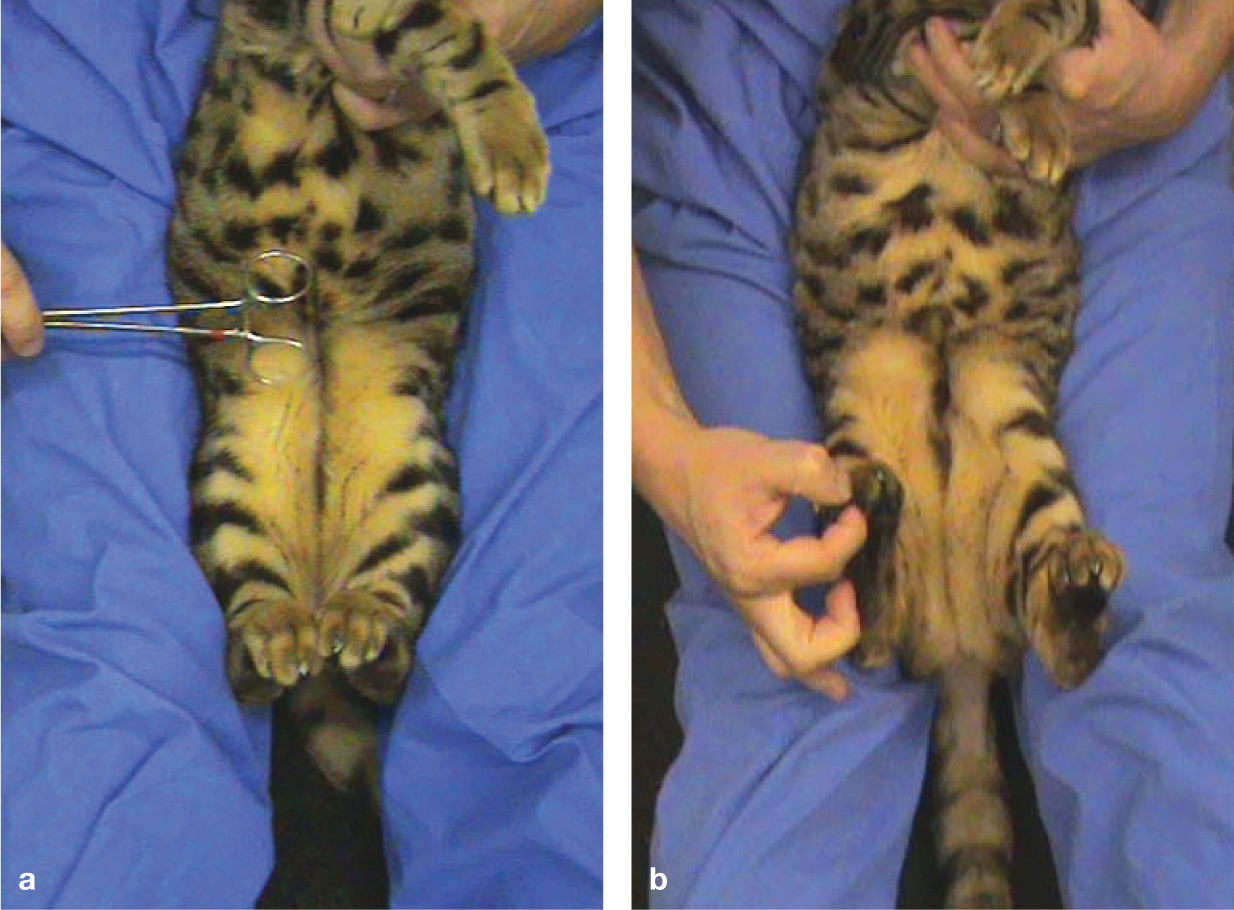
Spinal reflex evaluation in cats is best performed with the animal supported in dorsal recumbency between the thighs of the examiner. Although many spinal reflexes are described, the most reliable ones in cats are the patellar reflex (a) and withdrawal reflex (b). Evaluation of extensor tone in the pelvic limb can be used as a control in cats with ambiguous patellar reflexes as it involves the same neuroanatomical components
The flexor system is evaluated via the withdrawal reflex. In the thoracic limb, the withdrawal reflex evaluates the integrity of the C6–T2 spinal cord segments (and associated nerve roots), brachial plexus, peripheral nerves (radial, axillary, musculocutaneous, median and ulnar) and the muscle innervated. In the pelvic limb, this reflex evaluates the integrity of the L4–S1 spinal cord segments (and associated nerve roots), the femoral and sciatic nerves, and the muscle innervated.
The extensor system is evaluated by assessing the extensor tone in the limb. The ability to support weight on the tested limb is determined while the contralateral limb is lifted off the ground. In the thoracic limb, this tests mainly the radial nerve (elbow, carpus and digits extension via triceps and extensor carpi radialis innervation) and associated spinal cord segments (C7–T2). In the pelvic limbs, this tests mainly the femoral nerve (stifle extension via quadriceps group contraction) and tibial nerve (hock extension via gastrocnemius contraction), and associated spinal cord segments (L4–L6 and L6–S2, respectively).
Cutaneous sensory testing
A dermatome is an area of skin that corresponds to a specific nerve root and spinal cord segment. Areas of decreased or absent cutaneous pain perception may aid in identification of specific peripheral nerves, nerve roots and spinal cord segments involved in the disease process. Cutaneous sensation is evaluated by pinching the skin with a haemostat. The response elicited may be a behavioural response or a withdrawal reflex. The presence of either response indicates functional integrity of the particular sensory nerve tested (Table 1 and Figure 3).

Cutaneous autonomous zones in cats. Diagram reproduced with permission from ‘Small animal neurological emergencies’, eds Platt SR and Garosi LS, Manson Publishing (In press 2012)
Other neurological findings
In a cat presenting with thoracic limb monoparesis, the presence of ipsilateral complete or partial Horner’s syndrome (ie, sympathetic dysfunction limited to miosis, without obvious protrusion of the third eyelid, enophthalmia or ptosis of the upper eyelid) and/or loss of the ipsilateral cutaneous trunci reflex may help to further localise the lesion to the T1–T3 and/or C8–T2 spinal cord segments and associated nerve roots, respectively (Figure 4).

Traumatic avulsion of the left brachial plexus in a 2-year-old domestic shorthair cat following a road traffic accident. In addition to the severe monoparesis, this cat shows ipsilateral Horner’s syndrome (miosis and enophthalmia) as a result of damage to the preganglionic sympathetic nerve supply to the eye that runs alongside the ventral roots and proximal spinal nerves that form the brachial plexus
Neurodiagnostic investigations
Having established the neuroanatomical source of a particular problem (spinal cord, plexus or peripheral nerve[s]), further investigations can be considered to refine/narrow down the list of differential diagnoses (see later). 2
Electrodiagnostics
Electromyography (EMG) can be helpful to support neurological involvement, particularly in cases of occult lameness where an orthopaedic cause cannot be identified. Spontaneous electrical activity (positive sharp waves, fibrillation potentials) often develops in denervated muscles 5–7 days after the nerve injury has occurred (Figure 5). EMG alone does not differentiate primary muscular disease from peripheral nerve disease, although the former would be a very unusual cause of monoparesis or neurological lameness.
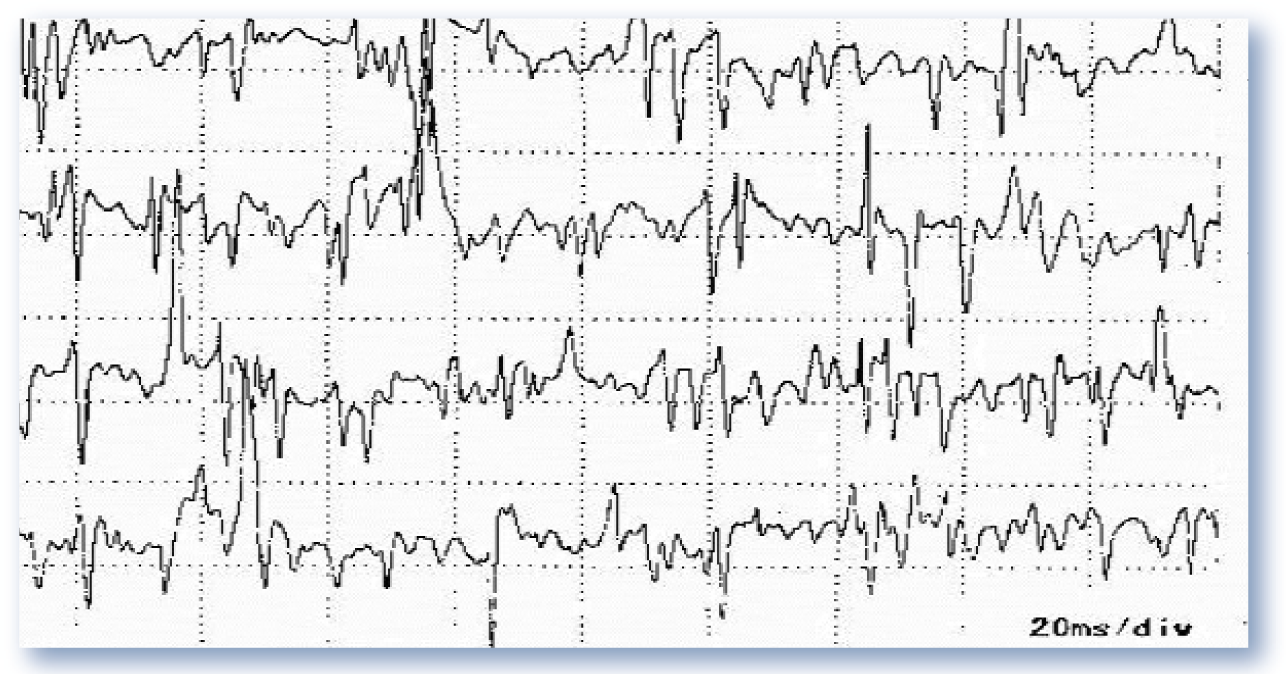
EMG is used to identify denervated muscles and to identify and characterise myopathies. It can be particularly useful for differentiating disuse from a neurogenic cause of muscle atrophy in a cat with lameness/monoparesis. A normal relaxed muscle is electrically silent (flat trace on recording) except in the end-plate region. Around 5–7 days after a peripheral motor nerve lesion, denervated muscle fibres exhibit spontaneous depolarisations, such as represented on this electromyogram, in the form of fibrillation potentials and positive sharp waves
Nerve conduction studies can be used to assess specific spinal nerves. Serial nerve conduction studies can give helpful prognostic information during the recovery phase of a traumatic peripheral nerve injury. F-waves and cord dorsum potentials can give information on ventral and dorsal nerve roots, respectively. 3
Imaging
Although many imaging modalities can be used to evaluate spinal cord integrity, magnetic resonance imaging (MRI) is the most sensitive and specific. Furthermore, MRI is the imaging modality of choice for nerve root, plexus and proximal (at least) peripheral nerve lesions (Figure 6). 4 Imaging of more distal peripheral nerve lesions can be more challenging. In the case of brachial plexus trauma, MRI of the affected plexus may provide information on the degree of nerve and associated soft tissue trauma. However, signal changes indicating an enlarged brachial plexus or peripheral nerve on MRI are rarely characteristic of a specific disease process (ie, inflammatory, infectious or neoplastic).Tissue biopsy using ultrasound-guided percutaneous needle sampling or surgical exploration is, therefore, necessary to enable histological diagnosis. 4

MRI of the lumbar spine in a cat with right pelvic limb weakness caused by L4–L5 disc extrusion. (A) On the sagittal view, the L4–L5 intervertebral disc (arrowhead) is dehydrated and has extruded, causing marked spinal cord compression (arrow). As well as involving extrusion of disc material (arrow), which appears midline on the transverse view of the caudal part of L4 (B), there is also secondary haemorrhage (arrow) at the level of the L4–L5 foramen (C). This affects femoral nerve function and the ability to support weight, as was observed in the right pelvic limb of this cat. Courtesy of Francois Liebel, Davies Veterinary Specialists
VITAMIN D mnemonic
Cerebrospinal fluid analysis
Cerebrospinal fluid (CSF) collection and analysis is useful to exclude inflammatory CNS disease. Collection distal to the site of the suspected lesion (ie, lumbar collection at L6–L7) is more likely to reveal changes. Nerve root compression or tumour may result in increased CSF protein levels; inflammatory/ infectious processes involving the nerve root may also result in increased CSF protein, and/or increased nucleated cell count. 4
Common neurological causes of lameness
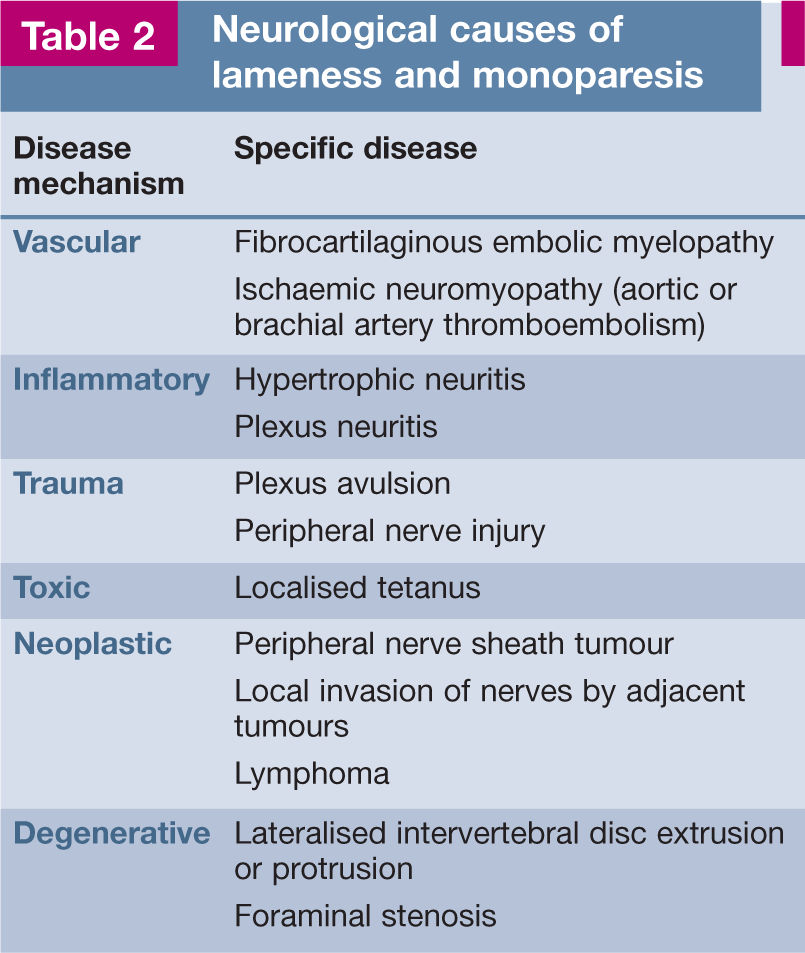
Determination of a list of differential diagnoses should be directed entirely by the neuroanatomical diagnosis (spinal cord, plexus or peripheral nerve[s]), and is essential in choosing and interpreting any diagnostic tests. The differentials list can be developed by taking into account elements such as history of trauma, mode of onset (peracute, acute, subacute or chronic) and pattern of development of the condition. Disease processes that affect the nervous system are traditionally classified using the ‘VITAMIN D’ mnemonic (see box and Table 2). Each category has a typical signalment, onset and progression. 2
Neurological causes of lameness and monoparesis
Vascular disease
Fibrocartilaginous embolic myelopathy
Fibrocartilaginous embolic myelopathy (FCEM) is a syndrome of acute spinal cord infarction caused by embolisation of fibrocartilage material. Histopathological evaluation is necessary to establish a definitive diagnosis as other conditions (even if rare) can also cause spinal cord infarction (ie, neoplastic emboli, parasitic embolism, septic emboli associated with bacterial endocarditis or other infection). FCEM should be suspected in cats with acute, and then non-progressive, signs of a focal myelopathy.5,6
Being a non-compressive spinal cord disease, affected cats are classically non-painful on palpation/manipulation of the spine. Emboli can occur anywhere in the spinal cord, so LMN or UMN signs can be observed. Unilateral infarctions affecting the grey matter of spinal cord segments C6–T2 or L4–S2, or the white matter of spinal cord segments T3–L3, may cause acute monoparesis of the thoracic (C6–T2) or pelvic limbs (T3–L3 or L4–S2). MRI is the diagnostic modality of choice (Figure 7).

Dorsal (A) and transverse (B) T2-weighted images of the lumbar spine of a cat with peracute onset of severe monoparesis of the right pelvic limb. Focal intramedullary hyperintensity confined to the right side of the spinal cord can be seen on the transverse image (arrowhead) at the level of the caudal part of L5 and on the dorsal image (arrow). These findings and history are suggestive of fibrocartilaginous embolic myelopathy
Treatment of FCEM is essentially conservative and based on supportive care and physiotherapy. The prognosis for functional recovery is usually good, though some cats experience persistent deficits (especially in the case of intumescence involvement and LMN signs). Cats with absent nociception (deep pain perception) have a guarded to poor outcome.
Ischaemic neuromyopathy
Ischaemic neuromyopathy occurs in cats with cardiomyopathy (especially hypertrophic cardiomyopathy), subsequent to thrombosis of the caudal aorta or its main branches. Arterial thromboembolism also occurs as a complication of hyperthyroidism and neoplasia. 7 Abyssinian, Birman, Ragdoll and male cats were overrepresented in one study. 8 The origin of the embolus is usually a thrombus attached to an endocardial surface. The most common site of occlusion is the aortic trifurcation. Other sites of embolism, such as the brachial artery, have also been reported. 9 The ischaemia is produced by vasoconstriction of collateral circulation induced by serotonin and thromboxane A2 from platelets trapped in the thrombus.
Clinical signs are typically acute and include paresis/paraplegia, with cold extremities, weak or absent femoral pulses, firm painful muscles and loss of nociception. In most cats, thromboembolism will affect both pelvic limbs, although a single limb (thoracic or pelvic) can be embolised. The nail beds are cyanotic and fail to bleed when cut. Tachypnoea and hypothermia were seen as additional clinical findings in 91% and 66%, respectively, of 127 cats in one study. 8
Common biochemical abnormalities in the acute phase include hyperglycaemia, azotaemia and abnormally high serum concentrations of muscle enzymes. 8 Diagnosis can be confirmed by aortography or Doppler ultrasonography of the aorta and its main branches. Thoracic radiography, echocardiography and electrocardiography are indicated to investigate the possibility of an underlying heart disease.
In the acute phase, treatment mainly relies on supportive care and management of the underlying heart disease, where appropriate. Use of thrombolytic agents such as tissue plasminogen activator (t-PA) or streptokinase has been advocated, although there is as yet no controlled study that shows that such treatment offers a significantly better outcome than no treatment. Aspirin and low-molecular weight heparin have been suggested for thromboprophylaxis.8,10 No significant difference was found in survival or recurrence rate between cats receiving high-dose aspirin (≤ 40 mg/cat q72h) and cats receiving low-dose aspirin (5 mg/cat q72h). 8 Adverse effects were less frequent and milder for the lower dosage. 8 Long-term mortality is primarily attributable to the severe underlying cardiac disease. A review of 100 cases reported an average long-term survival of 11.5 months in the 37% of cases that survived the initial thromboembolic episode. The remaining cases either died (28%) or were euthanased (35%). 11
Inflammatory disease
Hypertrophic neuritis
In people, hypertrophic neuritis is a rare tumour-like, chronic inflammatory, focal or multifocal, mainly demyelinating neuropathy, of unknown origin. 12 Areas of Schwann cell proliferation (‘onion bulb’ formation), as a result of repeated episodes of demyelination and remyelination, are the hallmark of this condition. 12 Response to corticosteroid treatment is usually variable between individuals and overall the prognosis is poor.
Clinical signs, MRI and pathological findings in a cat with bilateral hypertrophic neuritis of the brachial plexus have been described (Figure 8). 4
In most cats, thromboembolism, and subsequent ischaemic neuromyopathy, will affect both pelvic limbs, although a single limb (thoracic or pelvic) can be embolised.

Brachial plexus neuritis with bilateral nerve root swelling in a 9-year-old Burmese cat. (A) Transverse T1-weighted post-contrast magnetic resonance image at the level of C5–6 shows bilateral enlargement and homogeneous contrast uptake of the brachial plexi. The post-mortem specimen (B) shows the swollen nerves (arrowheads) supplying both brachial plexi
Traumatic disease
Brachial plexus avulsion
Common causes of nerve injury in cats include road traffic accidents (RTAs), gunshot wounds, bites, lacerations, stretching, fractures and iatrogenic damage from surgical procedures or injection injuries. Three types of nerve damage are distinguished depending on the degree of structural damage: neurapraxia (transient physiological conduction block of nerve transmission in the absence of structural damage); axonotmesis (disruption of the axons with the endoneurial and Schwann cell sheaths remaining intact); and neurotmesis (complete severance of all structures of the nerve). Axonotmesis and neurotmesis are followed by Wallerian degeneration and both carry a guarded to poor prognosis.
Avulsion of the nerve roots forming the brachial plexus, as a result of an RTA or fall from a height, is the most common traumatic neuropathy in the cat. The damage occurs at the level of the spinal roots where resistance to stretch is less than that of peripheral nerves due to the lack of perineurium. 13
Neurological signs associated with brachial plexus avulsion depend on which nerve roots are affected:
Many cats with brachial plexus avulsion will also present with ipsilateral Horner’s syndrome and/or loss of the cutaneous trunci reflex.
EMG can help to determine the extent of muscle denervation and confirm the distribution of nerve injury, although changes may not be seen for 5–7 days after the injury. Serial evaluation of radial nerve motor conduction velocity has been suggested as a useful prognostic indicator, with early decreased conduction velocity indicating a poor prognosis. 14
Treatment of brachial plexus injury is conservative and mainly centres on aggressive physiotherapy. Pancarpal arthrodesis, to prevent carpal collapse secondary to loss of radial nerve function, is rarely appropriate as in most cases elbow function is also absent. The prognosis is good for cats with cranial brachial plexus avulsion that retain the ability to bear weight and have intact cutaneous sensation. Cats with complete or caudal brachial plexus avulsion have a guarded to poor prognosis, especially if cutaneous sensation has been lost. If no improvement is seen during the first 2 months, recovery is considered unlikely. Amputation is recommended in these cases, especially if complications such as self-mutilation from paraesthesia, joint contractures or trophic ulcers develop. Gabapentin (10–20 mg/kg PO q8–12h) can be considered to control neuropathic pain if self-mutilation is seen.
Radial nerve injury
Radial nerve paralysis is not synonymous with brachial plexus avulsion, as is sometimes incorrectly assumed. The radial nerve can be injured proximally by fractures of the first rib or distally by humeral fractures. Lesions of the radial nerve affect the cat’s ability to extend the carpus. If the lesion occurs proximally in the radial nerve, the elbow may be held more ventrally than normal. The limb may be carried off the ground with the elbow flexed if the musculocutaneous nerve is intact. Diagnosis is usually made on clinical grounds.
Radial nerve paralysis is not synonymous with brachial plexus avulsion, as is sometimes incorrectly assumed.
Treatment is conservative in most cases and based on aggressive physiotherapy. Other treatment options for permanent neurological impairment include arthrodesis, muscle relocation and amputation. The prognosis for cats with distal lesions depends on the severity of the neural injury: neurapraxia is seen most commonly, and most cases recover within 1–2 months; neurotmesis leads to complete loss of cutaneous sensation over the cranial antebrachium and foot, and carries a poor prognosis.
Sciatic nerve injury
Sciatic nerve injury is a reported complication of femoral or pelvic fractures, and may also be caused by impingement from a femoral intramedullary pin, acetabular fracture stabilisation or intramuscular injections in the caudal thigh. Clinical signs include lameness or monoparesis, with a dropped hock and knuckling of the digits, as well as severe pain in the case of an intramedullary pin- or fracture-related injury. The limb is still able to support weight because the quadriceps muscle is functioning. There may be associated sensory analgesia, which is detected on the lateral, dorsal and plantar surfaces of the foot. The prognosis depends on the underlying cause and severity of the nerve injury. Loss of nociception in the digits innervated by the sciatic nerve indicates a poor prognosis. Loss of sciatic nerve function post-surgical intervention, such as fracture reduction, may be an indication to repeat surgery to address the nerve injury. Failure to recover sensory or motor function after 3 months is associated with a poor prognosis, and limb amputation may be required.
Femoral nerve injury
Femoral nerve injury is less common than sciatic nerve injury as the nerve is well protected within the sublumbar musculature. Potential causes include trauma, retroperitoneal abscess, haematoma and neoplasia. Dysfunction of the femoral nerve causes monoparesis and severe gait abnormalities. The patient cannot bear weight on the affected limb and carries it flexed; stifle extension and patellar reflex are lost; neurogenic atrophy of the quadriceps muscle rapidly develops; and cutaneous sensation to the medial aspect of the limb and medial digit may be lost. Diagnosis is based on history and clinical signs. Treatment is mainly supportive and the prognosis is generally guarded. If no improvement is seen in 4–6 months, recovery is unlikely and amputation of the affected limb should be considered.
Toxic disease
Tetanus
Although cats are supposedly resistant to the effects of the Clostridium tetani exotoxin, several cases of tetanus have been reported. Signs can be limited to a single limb (eg, following a distal limb injury), causing monoparesis associated with extensor rigidity.15,16 The diagnosis is presumptive and based on the presence of classic clinical signs. Treatment is directed at controlling the infection (surgical wound debridement if a wound can be found, metronidazole 10 mg/kg PO q12h), neutralising the toxin (tetanus antitoxin 100–1000 U/kg IV), and relieving the spasticity (CRI diazepam 0.2–0.5 mg/kg/h or midazolam 0.2–0.3 mg/kg/h IV).
Neoplastic disease
Peripheral nerve tumours
Tumours of the spinal nerves, including the brachial plexus, are much less common in the cat than the dog. Most of the peripheral nerve tumours in dogs are anaplastic and histological identification of the cell of origin (Schwann cell, perineurial cell or fibroblast) is usually not possible. The term malignant peripheral nerve sheath tumour (MPNST) has, therefore, been suggested. 13 MPNSTs most commonly develop from spinal roots or other peripheral nerves. 13 In dogs, these tumours frequently arise in the caudal and cranial thoracic nerve roots, and slowly spread proximally and distally. 13 In the cat, peripheral nerve tumours are more often cases of lymphoma, with only sporadic cases of MPNST having been recorded.17,18 The latter tumour type can also occur in the skin, subcutis and/or mucous membrane. 18
Most cats with peripheral nerve tumours present with a chronic progressive, unilateral forelimb lameness and muscle atrophy. Occasionally, the tumour may be palpable and in some cases may extend proximally through an intervertebral foramen to compress the spinal cord, which may lead to pelvic limb paresis. 19 Ipsilateral Horner’s syndrome may be seen if the cranial thoracic nerve roots are affected by the tumour itself or if there is cord compression at this point. 20
A number of modalities have been described to help in the diagnosis of these tumours. Survey radiography is often unremarkable. Ultrasonography may be helpful in recognising large nerve sheath tumours. Myelography is only useful when there is vertebral canal involvement. EMG is indicated to differentiate neurological from orthopaedic causes of lameness and/or muscle atrophy. Imaging techniques such as CT and MRI are preferred to assist with early diagnosis (Figure 9); when peripheral nerve enlargement is identified, differential diagnoses should include idiopathic (suspected immune-mediated) neuritis, infectious neuritis, 21 metabolic disease 22 and neoplastic neuropathy.23,24
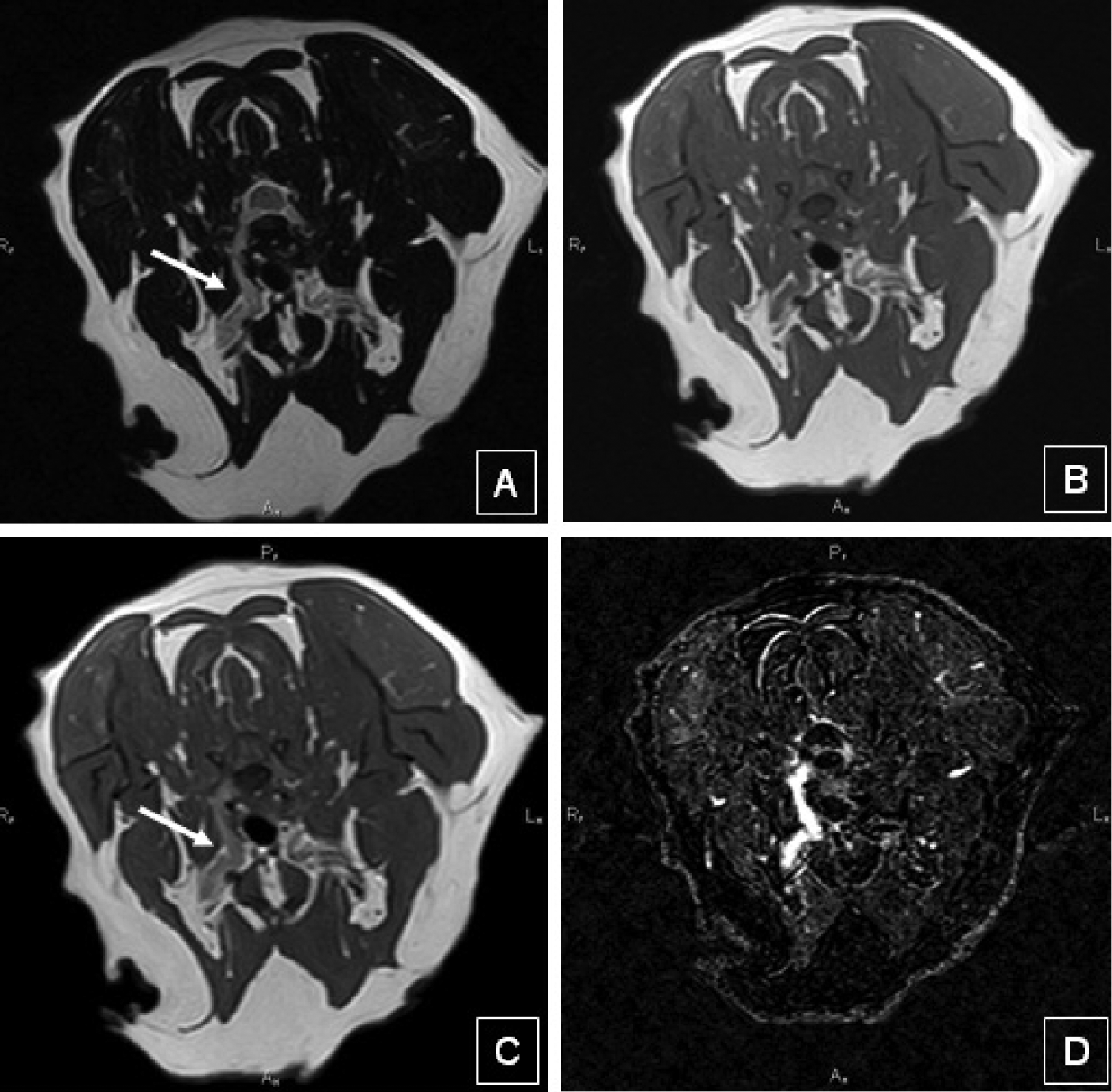
Transverse T2-weighted (A), T1-weighted pre- (B) and post-contrast (C), and subtraction image (D) of a right-sided brachial plexus tumour in a 10-year-old domestic shorthair cat with progressive right thoracic limb monoparesis. Although the tumour is not visible on the T1 image pre-contrast, the post-contrast study and the T2 image clearly show enlargement of the brachial plexus on the right (arrow)
Tumours within the brachial plexus or peripheral nerves are treated with local excision or by amputation of the affected limb. The prognosis for cats with peripheral nerve tumours overall is poor and the recurrence rate after surgery is high.
Brachial plexus lymphoma
Although lymphoma is considered to be the most common secondary tumour of the peripheral nerves, only a small number of cats with lymphoma involving the brachial plexus have been described (Figure 10).23–26 The optimum treatment (radiotherapy, chemotherapy and/or amputation) for cats with lymphoma involving the brachial plexus is unclear and the prognosis is, therefore, unknown.

High power view of a cytospun CSF sample from a cat with progressive right thoracic limb paresis caused by brachial plexus lymphoma. Three lymphoid cells are visible: at the top is a small mature lymphocyte; below are two larger intermediate neoplastic lymphocytes that have irregular, deeply basophilic cytoplasm surrounding a circular nucleus with irregularly clumped chromatin and prominent, variably sized and positioned multiple nucleoli. (x100, May-Grunwald-Giemsa.) Courtesy of Roger Powell, PTDS Veterinary Diagnostics
Key points
Monoparetic cats are frequently presented for veterinary investigation with the main complaint being lameness.
A good knowledge of the motor and sensory innervation of the thoracic and pelvic limb is essential in the diagnosis of neurological causes of lameness or monoparesis.
With a lame or monoparetic cat, attention should focus on assessment of gait, postural reactions, segmental spinal reflexes (flexor withdrawal and extensor tone) and muscle mass/symmetry.
Electromyography is helpful in some cases to support neurological involvement, particularly in cats with occult lameness where an orthopaedic cause cannot be identified.
MRI is the imaging modality of choice for nerve root, plexus and proximalperipheral nerve lesions. Imaging of more distal peripheral nerve lesions can be more challenging.
Footnotes
Funding
The author received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this review article.
Conflict of interest
The author declares that there is no conflict of interest.