
Abstract
Where historically justice and behavioral health professionals have functioned independently in systems that often collide, the ability to provide community behavioral health training to justice involved professionals may lead to enhanced public safety and decreases in incarcerations. This study evaluated the impact of the Mental Health First Aid program completed by 85 justice professionals. Study participants completed a questionnaire before and after the training to assess the impact on knowledge, attitudes, and beliefs. Findings suggest the training reduced stigmatizing attitudes and improved participants’recognition of mental health disorders, self-confidence in providing help, and intent to help. The results of this study provide preliminary evidence supportive of justice communities investing in the Mental Health First Aid training consistent with the International Chiefs of Police Association’s commitment to the “One Mind Campaign” to ensure that justice professionals have the skills to safely and responsibly meet the needs of people with mental illness
Collisions frequently occur at the intersection of mental health and criminal justice, with tragic and sometimes fatal consequences. Nearly half (44%) of individuals incarcerated in U.S. jails have a history of a mental health conditions (Bronson and Berzofsky, 2017), and those with serious mental illness have a 60% five-year re-arrest rate when released from correctional facilities (Torrey et al., 2017). However, despite frequent encounters, law enforcement and corrections officers are often inadequately trained to respond to persons with mental illness (PwMI) (Morgan and Miles-Johnson, 2022).
Whether responding to a suicide attempt or a report of a disorderly person, police officers are often the first to arrive to crises involving PwMI (Vermeer et al., 2020). Called “streetcorner psychiatrists” by some (Watson and Angell, 2013), police officers often prescribe the fates of PwMI, influencing whether they receive proper treatment, are left to continue to manage their current situation on their own, or are cycled through the criminal justice system (Watson et al., 2008). Approximately one in 10 calls that officers respond to involve PwMI (Lord & Bjerregard, 2014), and police spend more time responding to these calls than they do on assaults, burglaries, and traffic incidents combined (Cordner, 2006).
Caused by misconceptions that often stem from a lack of mental health education, many people hold stereotypes and prejudices regarding mental illnesses. Link et al. (1999) found the public tends to desire social distance from individuals depicted with symptoms of mental illness in vignettes, as well as perceive them as disproportionately dangerous compared with any real threat posed. Unfortunately, justice-involved professionals are not immune to these stigmatized beliefs. In fact, recent evidence suggests that police hold more stigmatizing views towards PwMI than other community members (Tartaro et al., 2023). As an officer’s actions regarding use of force are influenced by a suspect’s demeanor (Farrell, 2022), this consideration of stigma is especially relevant to police work, and it is even more of a concern today. Americans were found to be twice as likely to perceive people with schizophrenia as violent in 2018 than they did in the 1996 (Pescosolido et al., 2021). However, police interactions are actually more likely to be dangerous for the PwMI than for the officers (Cordner, 2006). While mental illness was only attributed to one out every 42 fatal assaults on police officers in the United States between 1993 and 2002 (Cordner, 2006), PwMI die in approximately one of every four fatal police interactions (Saleh et al., 2018) and are 16 times more likely to be killed in a police encounter than the general population (Fuller et al., 2015). When police officers perceive PwMI as a threat and have limited or no training on how to peacefully defuse these types of crises, they may resort to undue force, or in other cases, “mercy bookings” in order to maintain the safety of themselves and/or others (Smith et al., 2022). This greatly contributes to the critical issue that PwMI represent a disproportionately large fraction of the jail and prison populations (Bronson and Berzofsky, 2017). In America, there are three times more severely mentally ill people in jails and prisons than in hospitals. In Arizona, one of the worst states for access to mental health care, the ratio balloons to almost 10 times more (Torrey et al., 2010).
However, since mental healthcare is clearly not the focus of jails and prisons, the corrections system is incapable of providing adequate support and treatment to these individuals. For individuals suffering from serious mental illness (SMI), detention facilities are especially chaotic and disorienting environments (Roth, 2018). Once incarcerated, individuals with SMI are often left untreated and are at an increased risk of becoming victims of assault, staying incarcerated longer, becoming repeat offenders, being sent to solitary confinement, and attempting suicide (Bronson and Berzofsky, 2017; Torrey et al., 2010). Considering that this frequent incarceration of PwMI is inimical to the health and safety of both staff and all incarcerated individuals, mental health training in all areas of the criminal justice system is paramount.
Despite their regular contact with civilians with mental health disorders, many justice-involved professionals receive limited - if any - training on how to handle these types of situations (Morgan and Miles-Johnson, 2022). In fact, both police (Morgan and Miles-Johnson, 2022) and correctional officers (Lavoie et al., 2006) report their lack of sufficient training in this area as a critical problem, as PwMI may not respond well to traditional protocol (Morgan and Miles-Johnson, 2022). Law enforcement officials (Morgan and Miles-Johnson, 2022) and detention staff (Lavoie et al., 2006) have advocated for additional training in this area so they can safely and constructively handle situations involving PwMI.
Literature Review
Existing Programs
Many police departments have partially addressed the unique needs of responding to mental health crises by implementing a Crisis Intervention Team (CIT) consisting of officers who are trained and knowledgeable in identifying and communicating with PwMI. This extensive 40-h CIT training model is often considered the gold standard for preparing police officers to respond to situations involving PwMI. CIT programs have been shown to improve police knowledge, confidence, and attitudes (Compton et al., 2011; Nick et al., 2022). Evidence also suggests CIT-certified officers directed more PwMI to mental health services than did officers without CIT certification (Bratina et al., 2020). However, the training is expensive and requires more of the department’s resources as officers must be off the streets for a week to complete the 40-h CIT training (Compton et al., 2011) which can be particularly problematic for small departments. For these reasons, not all officers are CIT certified and most departments have a goal of certifying 20–25% of officers in CIT (typically consisting of those who volunteer to complete the training) (Compton et al., 2011). In addition, CIT programs are easier to adopt in larger, urban areas than smaller, rural ones (Rogers et al., 2019), so only around 15–17% of total police agencies had implemented CIT as of 2019 (Rogers et al., 2019). Even in departments where CIT teams have been assembled, police dispatchers are not always able to discern from information provided whether a crisis is going to involve someone with mental health conditions (Wood et al., 2021; Mitchell et al., 2022), and the number of officers who are CIT-certified is necessarily limited by police time and resources (Rogers et al., 2019). Thus, calls involving a person with a mental health disorder are not always immediately responded to by a CIT-certified officer.
Other programs have also emerged to assist law enforcement officials in responding to mental health crises. Some programs are based upon the collaboration of justice-involved professionals and trained peer support specialists, such as the R.E.A.L. Program in Lincoln, Nevada (Magdanz, n. d.). Started in 2011, this effort opened a pathway in which police officers, community corrections officers, and local human service providers can refer individuals with mental health and/or substance use conditions to a trained (mental health) professional with lived experience who provides ongoing support and resources. Program data suggests its effectiveness in outreach, community support, and improved quality of life for PwMI (Magdanz, n. d.). Another approach that is being widely implemented due to an increasing evidence base is dispatching 24/7 mobile crisis intervention teams consisting of mental health professionals to accompany police officers on mental health related calls, or to provide alternatives to law enforcement (Kirst et al., 2015). The CAHOOTS program in Eugene, Oregon was one of the first mobile crisis programs of this kind and is estimated by the Eugene Police Crime Analysis Unit (2020) to have diverted between 5-8% of 911 calls that police officers would have otherwise responded to. Inspired by these positive outcomes, similar programs have been established, such as the Crisis Response Network’s work in Arizona linking crisis hotlines and police calls to mobile crisis teams. Similar programs are now in Denver, Colorado and Olympia, Washington (Waters, 2021).
Although CIT and mobile crisis programs are often successful at preventing tragic situations, people will inevitably fall through the cracks due to limited capacity and/or education of officers (Waters, 2021). Furthermore, officials who work in other areas of the criminal justice system (such as corrections) are not typically trained in CIT and do not have access to mobile crisis teams, leaving a critical gap in training and highlighting the need for some form of mental health training for all justice-involved professionals.
A Potential Complementary Approach: Mental Health First Aid Training
Given that individuals experiencing mental illness and substance use disorders often have more contact with the criminal justice system than others (Hoch et al., 2009), the better prepared officers and staff are to respond effectively and appropriately to an individual presenting with a mental illness, the more likely the interaction will be positive (Reamer, 2022). As such, the International Association of Chiefs of Police supports the “One Mind” pledge with a goal of training and certifying 100% of sworn police officers in mental health awareness courses. This involves providing CIT training to a minimum of 20% of sworn officers and Mental Health First Aid (MHFA) 1 training to the remaining 80% of officers. The goal of MHFA “is to prevent tragedies, decrease the need for arrests and incarcerations for people with mental illness, reduce repeat detentions and help police officers connect with appropriate resources that can help” (Brooks, 2018). During MHFA training, officers are trained to intervene during a mental health crisis by recognizing the symptoms of mental illness, engaging with the individual in crisis, deescalating the incident, and connecting the individual to needed care. And yet, while there is significant momentum and funding behind the 8-h Mental Health First Aid training generally and the One Mind Campaign specifically, to date there are zero evidence-based assessments of the MHFA in the justice community. An evidence-based evaluation with this specific population of justice professionals is an essential first step towards the development of evidence informed policies regarding training for justice professionals and the appropriate allocation of limited resources.
Mental Health First Aid Training for Justice-Involved Professionals
In 2014, $15 million in the United States Substance Abuse and Mental Health Services Administration (SAMHSA) budget was dedicated to expand Mental Health First Aid training for first responders (Young, 2015), and a modified version of MHFA training for Public Safety (MHFA-PS) personnel was created. Due to the special circumstances that public safety officials may encounter, the public safety version of the MHFA course provides officers with skills to effectively and safely handle situations involving people with mental health conditions. Additionally, it focuses on improving public safety officers’ abilities to recognize psychosis, substance abuse, co-occurring disorders, depression, anxiety, traumatic brain injury, autism spectrum disorders, and excited delirium (Young, 2015).
While police departments in places like Rhode Island, Pennsylvania, and Hoonah, Alaska piloted the MHFA-PS program (Gibb, 2014), there is still no peer-reviewed research available on the effectiveness of these programs. However, in Massachusetts, Young (2015) compared officers who took a brief 1-h mental health course with officers who were given a 12-h Massachusetts Municipal Basic Recruit Officer Course Mental Health Training, which combines elements of both MHFA training and Crisis Intervention Team (CIT) training. The research on this course demonstrates that it improves self-efficacy and confidence while reducing stigmatizing attitudes towards PwMI. Although this training is partially derived from MHFA training, it is not exactly the same. Therefore, the outcomes of this study are not necessarily generalizable to MHFA training. Nonetheless, the results of this research show promising implications for MHFA courses in the criminal justice community.
Knowledge and Recognition of the Problem
In order to effectively help people in mental health crises, it is imperative to first be capable of recognizing the problem. For this reason, the first topic taught in the MHFA course revolves around improving participants’ knowledge and literacy of mental health disorders. They learn an encompassing definition and description of what mental health problems are, prevalence rates, the professionals that can provide help to these individuals, and the treatments that are available. The participants are also provided with information about common types of mental illnesses - such as substance abuse problems, psychotic disorders, depression, anxiety disorders, and eating disorders (Kelly et al., 2009). Numerous studies on MHFA training have demonstrated significant improvements in knowledge and identification of mental health problems, (Wong et al., 2017; Morawska et al., 2013) and these outcomes were shown by Hart et al. (2012) to be maintained after 6 months.
Attitudes Towards People with Mental Illnesses
Partially due to a lack of knowledge and understanding, the general population often holds negative attitudes and perceptions about PwMI. For instance, many believe that this population is generally less capable of recovery (Barry et al., 2013), perceive them as more unpredictable and violent (Pescosolido et al., 2021; Link et al., 1999), and consequently desire more social distance from PwMI (Link et al., 1999). Arrests and misdemeanors exacerbate this problem. Thus, the focus on the reduction of stigma is especially critical for people working in the criminal justice system, where instinctive reactions can be potentially dangerous (Watson et al., 2008). For law enforcement officers, this stigma not only impacts how they interact with PwMI, but it also influences how these civilians perceive and respond to officers. A person treated with respect and empathy by a police officer may see that officer as less threatening and therefore react more calmly. In order to reduce stigmatizing beliefs, the MHFA course encourages participants to reflect on their beliefs towards PwMI, learn prevalence rates, and become trained on other stigma-reducing exercises (Young, 2015). These exercises appear to have a significant impact. The MHFA program has primarily been shown to reduce stigmatizing attitudes for both general and specific populations and professions (Bond et al., 2015; Hart et al., 2012; Jorm et al., 2010).
Self-Confidence in Providing Help
When dealing with a mental health crisis, a first responder’s self-confidence in his or her ability to help is vital. Studies have demonstrated that police officers lack confidence or self-efficacy when interacting PwMI (Morgan and Miles-Johnson, 2022). Without proper training, law enforcement officials may feel that they are incapable of properly handling the situation, causing them to be uncomfortable, to panic, or to resort to methods that they believe ensure the safety of themselves or others (i.e., arrests or violence) (Borum, 2000). In addition, this may lead them to respond to mental health crises less frequently (Young, 2015). By providing skills, resources, and a basic and memorable 5-step plan for responding to these crises, MHFA training has demonstrated significant effectiveness in boosting the confidence of participants (Svensson and Hansson, 2017).
Helping Others and Themselves
Evidence suggests that MHFA training is effective in improving mental health first aid intentions (Aakre et al., 2016). The helping behaviors most commonly reported include encouraging professional help and listening to the person (Jorm et al., 2010), which are both crucial components of the action plan that MHFA training is based upon. In addition to training participants to help others in a crisis, some research has demonstrated that the MHFA program has positive effects on the mental health of the participants themselves (Kitchener and Jorm, 2004). Considering police officers are more susceptible to developing posttraumatic stress disorder (PTSD) (Kates, 2008) and have high prevalence rates of depression (Lawson et al., 2012), this training may be especially beneficial. For this reason, self-care is particularly emphasized as part of the MHFA for Public Safety course (Gibb, 2014).
There is clearly a need for training and effective policies to enable criminal justice professionals to quickly identify, deescalate, and divert those with mental illness from correctional institutions toward professional community mental health providers. There have been over 100 studies evaluating the Mental Health First Aid Training including school personnel, faith-based organizations, hospitals and nursing home staff, families, and teens; however, to date, the authors are unaware of any evaluations that examine the use of the Mental Health First Aid Training with justice professionals. Current estimates show that there are more than 10,000 police officers, corrections officers, and other public safety professionals who have completed the MHFA training yet no studies that examines whether Mental Health First Aid changes officer’s knowledge, attitudes, and beliefs towards PwMI and leads to officers appropriately identifying, de-escalating, and referring individuals to mental health care as appropriate. This study is a first step in examining the unique contribution of Mental Health First Aid training for justice professionals. The purpose of this research is to evaluate the effectiveness of the Mental Health First Aid Training on increasing knowledge and skills to connect PwMI to appropriate health services, thus diverting these individuals from the criminal justice system.
Theoretical Framework
A central reason for the widespread adoption of the MHFA courses is that they are simple and short, yet they teach widely applicable life-saving skills. MHFA trainers use the acronym ALGEE to teach participants an easily remembered action plan for helping people experiencing a mental health crisis. ALGEE stands for Approach the person, assess for risk or harm, listen non-judgmentally, give reassurance and information, encourage appropriate professional help, and encourage self-help and other support strategies. However, in the American version of MHFA, the first step “approach the person” is not taught. The information and strategies taught in each of these first aid steps are presented as key to improving helping behaviors, self-confidence, and knowledge while also reducing stigma.
Created by Anthony Jorm and Betty Kitchner in Australia in 2001 to prepare the general public to assist people experiencing a mental health crisis, the eight-hour Mental Health First Aid training program has expanded beyond national borders to reach people in over 14 countries (Jorm and Kitchener, 2011). The training is now intended for the general population and several versions have been created for specific groups so that people of all ages, cultural backgrounds, and professions can more effectively utilize MHFA to help those around them in crisis. The effectiveness of the MHFA training has been evaluated within a variety of different populations including youth (Kelly et al., 2011), elderly care staff (Svensson and Hansson, 2017), Aboriginal and Torres Strait Islanders (Armstrong et al., 2017), pharmacists, (Kirschbaum et al., 2016) nursing and medical students (Bond et al., 2015) and university Residential Assistants (Thombs et al., 2015). Within several countries, and for both the general public and specific groups, research has consistently demonstrated the MHFA program’s effectiveness in improving recognition and knowledge of mental health disorders, self-confidence in providing help to someone with mental health problems, increasing helping behaviors, all while reducing stigmatizing attitudes (Jorm and Kitchener, 2011).
Current Study
Overall, research on MHFA training has demonstrated the program’s effectiveness in improving participants’ self-confidence in providing help, identification of mental health disorders, helping behaviors, and attitudes towards PwMI. However, 50 of the 60 evaluation studies on MHFA include Kitchener and Jorm, the creators of MHFA, as authors or co-authors. This highlights the need for independent evaluators to assess the MHFA course in order to inform decisions regarding the investment of Mental Health First Aid on a wide scale, especially for justice professionals. Additionally, no peer-reviewed studies have been published on the effectiveness of MHFA training specifically for justice-involved professionals. Thus, the purpose of the current study is to determine how MHFA training impacts the knowledge, behaviors, and beliefs of participants who work in the criminal justice system.
Hypotheses
Based upon prior research and theory, it is hypothesized that justice professionals who complete the Mental Health First Aid Workshop will be more likely to report: (H1) greater awareness and recognition of mental illness, (H2) less stigma toward individuals presenting with mental health issues, (H3) increased confidence in their ability to utilize a variety of communication techniques meant to deescalate encounters with individuals presenting with mental health issues, and (H4) more willingness to work collaboratively with the health system to engage presenting individuals in the health system versus the criminal justice system
Methods
Design
This experiment used a one-group pretest/posttest design, with all participants receiving training in Mental Health First Aid (MHFA). Thus, the MHFA training course acted as the independent variable. The dependent variables that were measured included recognition of mental health disorders, attitudes towards PwMI, increased self-confidence in providing help, and an improvement in self-reported ability to appropriately help PwMI. Variables such as the length of the course, instructor, course content, and survey questions were controlled for via the study design and remained constant throughout the study.
Setting
Five separate MHFA training sessions were conducted in a northern Arizona city, where the population consists of a little over 70,000 people. The training was provided at a local police department on five separate training dates over an 8-month period.
Participants
Demographics of training participants (N = 85).
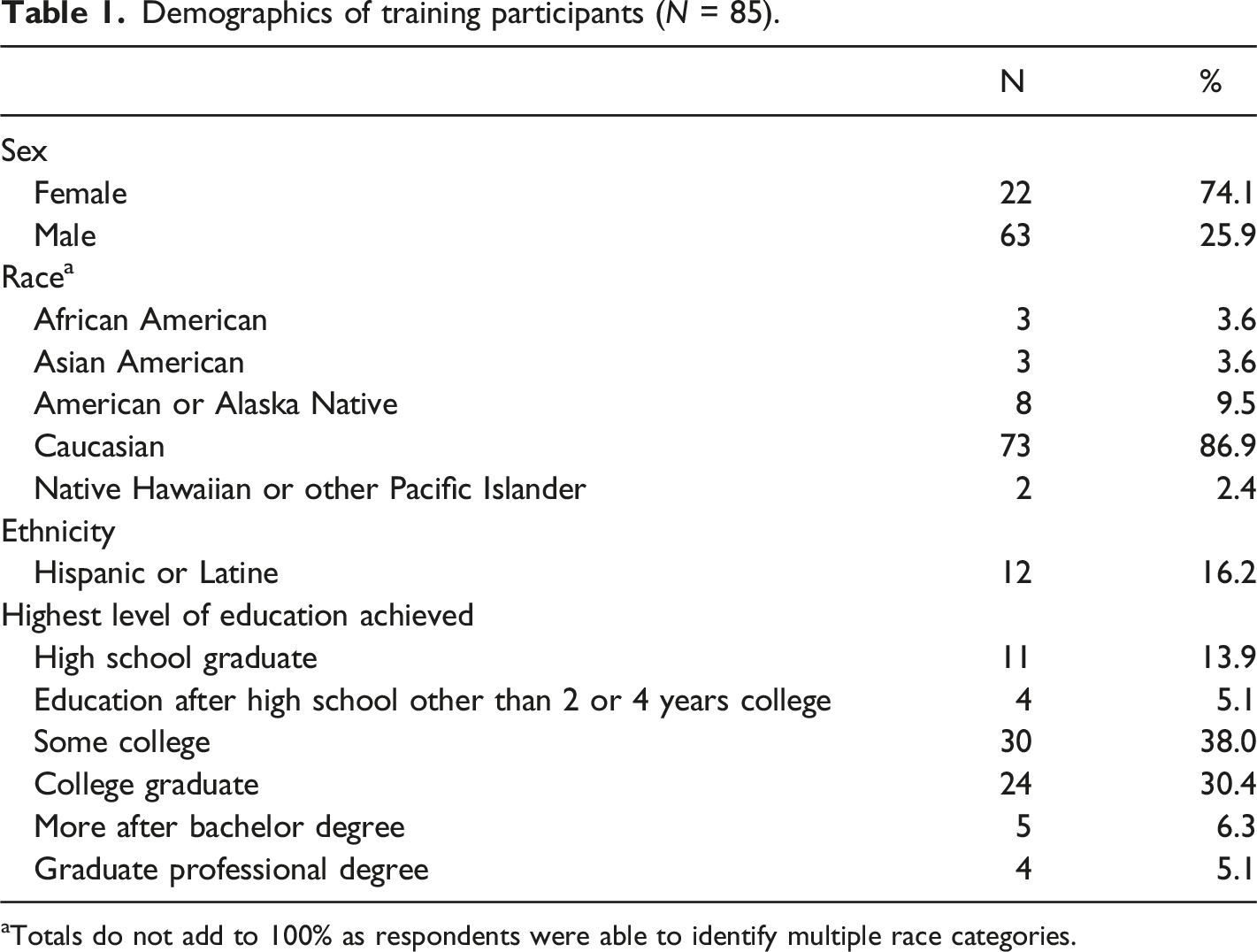
aTotals do not add to 100% as respondents were able to identify multiple race categories.
The most common reasons participants reported for attending the training were (1) because the participant believed the training to be important in helping them do a better job (N = 27) and (2) their attendance was mandated (N = 14). Fifty-three percent of the participants reported prior mental health training. Of these participants who indicated having prior mental health training, 36% reported having already completed the intensive 40-h Crisis Intervention Training (CIT) course. A vast majority of the participants (82%) indicated that they had contact with someone with a mental health condition during the past 6 months, while 9% reported not having any contact, and 6% of the participants did not know whether they had.
Measurements
The pretest and posttest surveys completed by trainees used the same standard outcome measures found in other MHFA studies (Aakre et al., 2016). The survey, designed by Kitchener and Jorm, is designed to measure participants’ mental health knowledge, recognition of depression or schizophrenia, self-confidence in providing help, mental health first aid intentions, and attitudes towards PwMI. In addition, respondents were asked about their socio-demographic characteristics, why they were interested in the course, self-reported history of mental health problems in the respondent or their family, contact with PwMI in the past 6 months, and if any help was offered by the participant.
In the survey, participants were randomly assigned vignettes depicting a person with either schizophrenia or depression. The study was intentionally designed so that trainees received the same scenario at both the pre-training and post-training conditions consistent with prior evaluations. These vignettes were used in other MHFA studies and are based on DSM-IV and ICD-10 diagnostic criteria for major depression and schizophrenia. The two scenarios depicted below were used to guide questions asked throughout the survey.
The depression vignette was as follows: John is 30 years old. He has been feeling unusually sad and miserable for the last few weeks. Even though he is tired all the time, he has trouble sleeping nearly every night. John doesn't feel like eating and has lost weight. He can't keep his mind on his work and puts off making any decisions. Even day-to-day tasks seem too much for him. This has come to the attention of John's boss who is concerned about his lowered productivity.
The schizophrenia vignette was as follows: John is 24 and lives at home with his parents. He has had a few temporary jobs since finishing school but is now unemployed. Over the last six months he has stopped seeing his friends and has begun locking himself in his bedroom and refusing to eat with the family or to have a bath. His parents also hear him walking about his bedroom at night while they are in bed. Even though they know he is alone, they have heard him shouting and arguing as if someone else is there. When they try to encourage him to do more things, he whispers that he won't leave home because he is being spied upon by the neighbor. They do not believe he is taking drugs because he never sees anyone or goes anywhere.
Recognition of Depression and Schizophrenia
After being presented with one of the vignettes, participants were asked the open-ended question: “what, if anything, is wrong with John?” Responses including ‘depressed’, ‘depression,’ ‘affective disorder’ or ‘mood disorder’ signified a correct identification of the problem depicted in the vignette according to a professional consensus. For the schizophrenia vignette, responses including ‘schizophrenia’, ‘schizoaffective disorder’, or ‘psychosis’ were identified as correct.
Attitudes Towards People with Mental Health Conditions
(a) Social Distance was measured using questions adapted from the validated attitudinal Social Distance Scale (SDS) (Link et al., 1999). Participants were asked how willing they would be to interact with John in five different circumstances. The social distance items included: Move next door to John; Spend an evening socializing with John; Make friends with John; Have John start working closely with you on a job; Have John marry into your family. These were rated on a scale from one to 4 (1 being “definitely willing” and four being “definitely unwilling”). Responses were summed for a total score ranging from 5 – 20 with higher average summed scores suggesting greater social distance. (b) Personal Stigma towards mental illness items were adapted from the validated Depression Stigma Scale (DSS) (Griffiths et al., 2008). Participants were asked whether they endorsed the following negative statements about PwMI: (1) People with a problem like John’s could snap out of it if they wanted; (2) A problem like John’s is a sign of personal weakness; (3) John’s problem is not a real medical illness; (4) People with a problem like John’s are dangerous; (5) It is best to avoid people with a problem like John’s so that you don’t develop this problem; (6) People with a problem like John’s are unpredictable; and (7) If I had a problem like John’s I would not tell anyone. These questions were rated on a 5-point Likert scale ranging from strongly disagree (coded = 1) to strongly agree (coded = 5). Responses were summed for a total score ranging from 7 to 35 with higher average summed scores suggesting greater stigma.
Self-Confidence in Providing Help to Someone with a Mental Illness
To assess confidence in providing help to an individual with a mental illness, participants were asked: “How confident would you be in your ability to help John?” They responded on a 5-point Likert scale ranging from ‘not at all’ (coded as 1) to ‘extremely’ (coded as 5).
Mental Health First Aid Intentions: Helping Others and Self
Using the vignettes, trainees were asked to describe how they would interact with the individual. Using an open-ended question, participants were asked: “Imagine John is someone you have known for a long time and care about. You want to help him. What would you do?” These responses are coded according to the ALGEE action plan, which is a major component of the MHFA course. ALGEE is an easily remembered acronym that stands for Assess and Assist with any crisis; Listen non-judgmentally; Give support and information; Encourage appropriate professional help; and encourage other supports receive. According to the official MHFA coding system, participants received 0–2 points per component of the ALGEE plan for a maximum total of 10 points. Based on the quality of the answer, 0 points were allocated for “no mention or inadequate response,” one point was given for a “superficial response without details,” and two points were provided if the answer contained “specific details or actions.”
Beliefs About Treatments and Interventions
In the survey, participants rated a list of people, treatments and actions that might be used by the person depicted in the vignette. They were asked: ‘if John was to seek help from any of the following people, is it likely to be “helpful”, “harmful,” “neither” or “don’t know” for his problem? Participant responses were compared to the consensus of professionals in the field. The professional consensus demonstrated that GPs, psychiatrists, clinical psychologists, counseling, antidepressants, and cognitive behavior therapy are all helpful for depression. Based on the number of interventions that participants selected as ‘helpful’, the scoring for the depression vignette thus ranged from 0–6. For the schizophrenia vignette, the professional consensus showed that GPs, psychiatrists, clinical psychologists, antipsychotics and admission to a ward are helpful. The scoring for the schizophrenia version also ranged from 0–5, based on the interventions that participants selected as helpful. In order to maintain equal scoring, these scores were converted into percentages.
Procedure
Ethical clearance for this study was received in accordance with the Institutional Review Board guidelines at Northern Arizona University. A certified MHFA instructor taught the course on five separate occasions. Hand-written surveys were administered to a total of 85 participants prior to each training session. Trainees then completed the 8-h MHFA course over two consecutive days. At the culmination of the training, participants filled out a posttest survey. To maintain anonymity, participants were asked to put the last four digits of their social security number on both the pre-test and post-test so they could be matched.
Results
Analysis
Differences Between Pre versus Post Test Results on Four Hypothesized Outcomes.
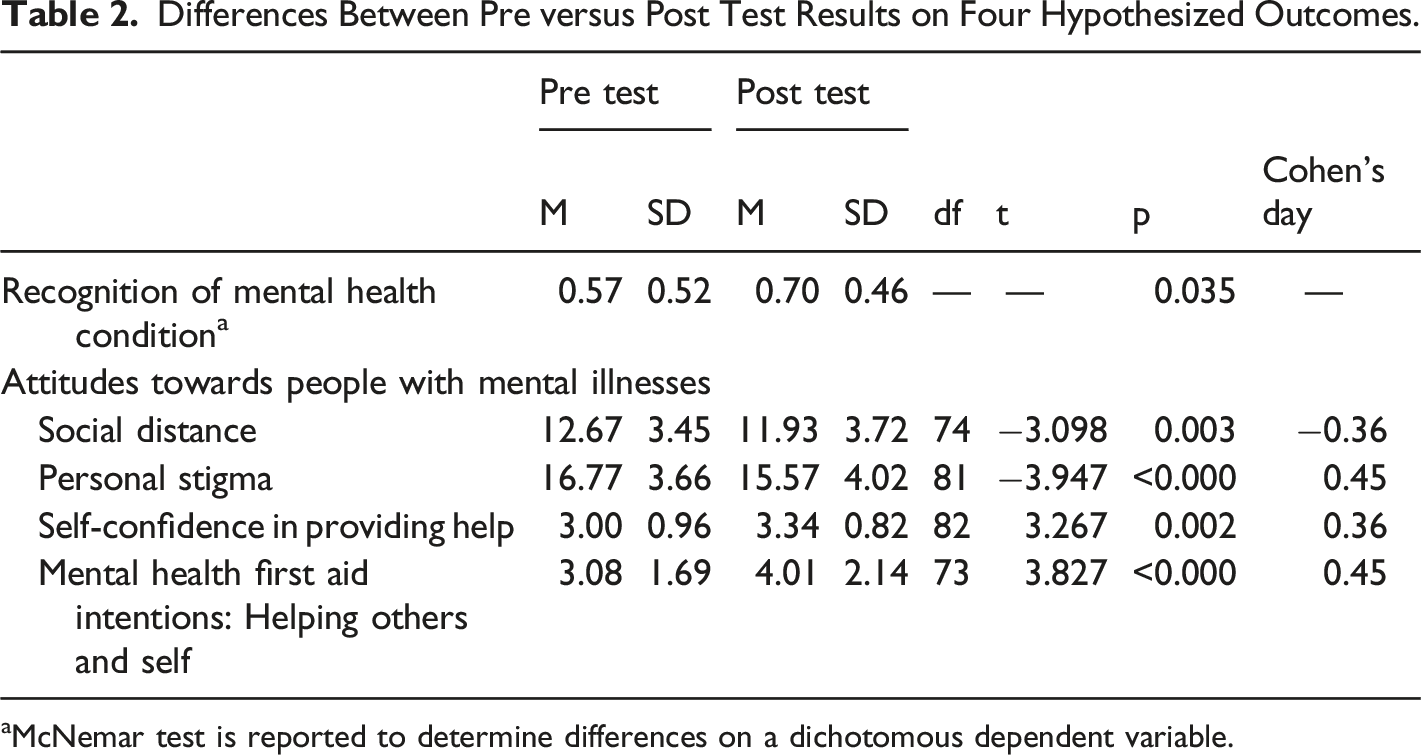
aMcNemar test is reported to determine differences on a dichotomous dependent variable.
Hypothesis 1: Recognition of Depression or Schizophrenia in a Vignette
The first hypothesis predicted that participants would exhibit significant improvements in the accurate identification of the mental health disorder (schizophrenia or depression) presented in the vignettes after completing the MHFA training. To assess whether pre-training (M = 0.57, SD = 0.52) and post-training recognition means (M = 0.70, SD = 0.46) were different, a McNemar test was performed. The McNemar test is used to determine if there are differences on a dichotomous dependent variable (recognition of mental health condition) between two related groups (pre and post tests). The proportion of respondents able to correctly identify an individual presenting with depression or schizophrenia increased from the pretest value of 57%–70% at the posttest following the training. This is a statistically significant difference, p = 0.035. These results imply that MHFA training does improve participants’ ability to recognize and correctly identify whether the person in the vignette is suffering from depression or schizophrenia.
Hypothesis 2: Attitudes Towards People with Mental Illnesses
The prediction that participants will report significant decreases in average social distance and stigma after the MHFA training was assessed using a paired samples t-test. Mean social distance and stigma scores in the pretest and posttest conditions were compared.
There was a significant difference in the means for the pre-training condition (M = 12.67, SD = 3.45) and the post-training conditions (M = 11.83, SD = 3.72); t (74) = −3.098, p < 0.003. Cohen’s d was estimated at −0.36, which is a small/medium effect based on Cohen’s (1992) guidelines. As such, the mean in the posttest condition was significantly lower than the mean in the pretest condition, indicating that MHFA training does appear to improve the justice professionals’ knowledge on attitudes towards an individual experiencing a mental health issue.
The mean in the posttest conditions (M = 15.57, SD = 4.02) was significantly lower than the mean in the pretest conditions (M = 16.77, SD = 3.66); t (81) = −3.947, p < 0.000. Cohen’s d was estimated at 0.45, which is a medium effect based on Cohen’s (1992) guidelines. According to these results, MHFA training does appear to improve justice professionals’ attitudes towards PwMI. Specifically, both attitudes towards desiring social distance from individuals with a mental illness and personal stigma towards individuals with a mental illness decreased after completing the course.
Hypothesis 3: Self-Confidence in Providing Help
In the third hypothesis, it was predicted that justice professionals would report significantly more self-confidence in their abilities to help an individual with a mental illness after completing the MHFA course. To test whether pre-training (M = 3.00, SD = 0.96) and post-training self-confidence means (M = 3.34, SD = 0.82) were equal, another paired samples t-test was performed. The assumption of normality was considered satisfied as skewness and kurtosis levels were estimated at 0.191 and 0.347, respectively, which is less than the maximum allowable values for a t-test. Two outliers were detected that were more than 1.5 box-lengths from the edge of the box in a boxplot. Inspection of the two cases did not reveal them to be extreme and they were kept in for the final analysis. The null hypothesis of equal means for the pretest and posttest conditions was rejected; t (82) = 3.267, p < 0.002. Thus, the post-training mean was significantly higher than the pre-training mean. Cohen’s d was estimated at 0.36, which is a small/medium effect according to Cohen’s (1992) guidelines. These results suggest that MHFA training does increase self-confidence in providing help after completion of the MHFA course for the justice professionals who completed the training.
Hypothesis 4: Mental Health First Aid Intentions: Helping Others and Self
It was hypothesized that trainees’ knowledge on how to appropriately help the person suffering from a mental health problem in the vignette would significantly increase after completion of the MHFA training. A paired samples t-test was conducted to compare average ALGEE helping behaviors reported in the pretest and posttest conditions. Before conducting the analysis, the assumption of normally distributed difference scores was investigated. This assumption was considered satisfied as skewness and kurtosis levels were estimated at 0.71 and 0.62, respectively, which is less than the maximum allowable values for a t-test. One outlier was detected that was more than 1.5 box-lengths from the edge of the box in a boxpolot. Inspection of the value did not reveal it to be extreme and the respondent was kept in the analysis. There was a significant difference in the means for the pre-training condition (M = 3.08, SD = 1.69) and the post-training conditions (M = 4.01, SD = 2.14); t (73) = 3.827, p < 0.000. Cohen’s d was estimated at 0.45, which is a medium effect based on Cohen’s (1992) guidelines. The mean in the posttest condition was significantly higher than the mean in the pretest condition, indicating that the MHFA training did appear to improve justice professionals’ knowledge on how to provide appropriate help to an individual experiencing a mental health problem.
Discussion
The purpose of this study was to examine the effectiveness of Mental Health First Aid training in preparing those who work as justice-involved professionals to effectively respond to PwMI. It was hypothesized that after completing the MHFA training course, participants would demonstrate significant improvements in self-confidence providing help, recognition of mental health disorders and how they are treated, knowledge of professional forms of help, and attitudes towards PwMI. As detailed below, the results of this study supported each of these hypotheses.
Knowledge and recognition of mental health problems
The ability to understand and identify mental illness is instrumental to effectively responding to PwMI. Ninety-seven (97) percent of the respondents indicated the individual depicted in the scenario needed help at the pre-test and 98% indicated the individual needed help at the post-test. This is not a significant increase; however, given that the percentage of respondents identifying the need for help was already so high at the pre-training condition, a significant increase would not be expected. Consistent with prior research on the effectiveness of the MHFA course (Wong et al., 2017; Morawska et al., 2013), the current study found significant improvements in the knowledge required to recognize depression or schizophrenia in the vignette after completing the MHFA training, an important first step in understanding how to appropriately interact and deescalate a potentially volatile situation.
Attitudes towards people with depression or schizophrenia
It is especially necessary to reduce the presence of stigma in people who have power over PwMI and frequently interact with them. For officers in charge of public safety and individuals who work in the jails, stigmatizing attitudes may cause them to respond with violence, arrests, or harsher punishments (Watson et al., 2008). Prior research has shown the MHFA training is effective in reducing stigmatizing attitudes both in the general public and also within specific populations and professions (Bond et al., 2015; Hart et al., 2012; Hart et al., 2018; Jorm et al., 2010). Similarly, this study found a statistically significant decrease in attitudes consistent with social distance and stigma towards PwMI after completion of the course. This suggests that MHFA training may lead justice professionals to be more willing to interact with PwMI and endorse fewer negative beliefs about this population.
Self-confidence in providing help
Trainees’ confidence in their abilities to provide help to someone suffering from a mental health problem is essential. This is especially true for police officers and other justice professionals, who have reported a lack of confidence or self-efficacy when interacting with PwMI (Morgan and& Miles-Johnson, 2022). Similar to prior research that examined the impact of MHFA trainings (Svensson and& Hansson, 2017), this present study found a significant increase in average reported self-confidence in providing aid to someone suffering from a mental health problem.
Mental health first aid intentions: Helping others and self
Previous literature has demonstrated that MHFA training is effective in improving mental health first aid intentions (Aakre et al., 2016), as seen in participants addressing more components of the ALGEE action plan after completing the course. The five-steps include: (1) Assess for risk of suicide or harm, (2) Listen nonjudgmentally, (3) Give reassurance and information, (4) Encourage appropriate professional help, (5) Encourage self-help and other support strategies. These findings were corroborated by the results in the present study.
Limitations
This study was designed to assess improvements for justice professionals in knowledge, attitudes, and beliefs towards PwMI. One major limitation to the design of this study is that these results are based entirely on self-reported data and theoretical helping behaviors in response to hypothetical scenarios. In reality, participants may react much differently when they are faced with an actual mental health crisis in the field. While assessing the impact of the 8-h MHFA training via pre-post tests is an appropriate and necessary first step to assessing the impact of the training for justice-involved professionals, it is necessary to see whether results are maintained long-term. Thus, designing a study and collecting data allowing for follow ups that actually evaluate the impact of the training on behavior and experiences in the field is a necessary next step in examining the impact of the MHFA training outside of a classroom setting.
This research is also not generalizable to any specific population or type of job within the criminal justice system. Several types of staff working in the criminal legal system attended the training, including detention staff, administrative specialists at the jail, cooks at the jail, officers from the local police department, and deputies from the county sheriff’s department. In addition, there may be ceiling effects due to the fact that 42 out of 80 of the participants (53%) reported that they already had prior mental health training. Furthermore, 36 of those 42 participants had already completed an intensive 40-h Crisis Intervention Training (CIT). Since many trainees already had extensive knowledge about mental health, MHFA training likely only reinforced skills taught in CIT training, so limited improvements may have been detected.
Finally, this research is unable to definitively claim that MHFA training caused the changes observed from the pretest to the posttest condition. In order to align with the police department’s goal of training 100% of their officers in Mental Health First Aid, this study did not have a control group. Thus, it is susceptible to threats to internal validity.
Policy implications
Recognizing the limitations inherent in the study design and the lack of a long term follow-up that allows for assessment of changes in behavior for justice-involved individuals, the results of this study provide evidence supportive of justice communities investing in the Mental Health First Aid training, consistent with the International Chiefs of Police Association’s commitment to the “One Mind Campaign” to ensure that criminal justice professionals have the skills to safely and responsibly respond to calls that involve PwMI. These results indicate that the implementation of the MHFA program could improve criminal justice professionals’ responses to people suffering from mental illnesses. Knowledge, attitudes, beliefs, and hypothetical helping behaviors are important to examine; however, it is also necessary to evaluate actual changes in behavior and identify obstacles to effectively implementing ALGEE strategies while actually in the field. Considering the critical overlap between the mental health and the criminal justice systems, this study concludes that more research on MHFA training with justice professionals is necessary as is future research that examines changes in behaviors beyond self-reported knowledge, attitudes, and beliefs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.