
Abstract
Autistic adults who require significant support need an adapted living environment. In this study, we co-constructed, with the staff of a Canadian residential setting for autistic individuals, the PBIS-Residential setting for Autistic Adults (PBIS-RA) model, based on the five core components of the original system-wide PBIS model. We then sought to evaluate its implementation by identifying barriers, facilitators, and fidelity. Using a case analysis design, we collected data through field notes, PBIS-RA committee work, meeting minutes, staff interviews, and observations. We analyzed data using multiple modalities, such as coding interviews and analytical workshops, to understand the factors influencing organizational implementation of PBIS-RA, based on the Consolidated Framework for Implementation Research (CFIR). Our results identify the necessary adaptations for PBIS-RA to meet the unique needs of autistic adults in this residential setting. We highlight the specific elements that affected the implementation of the PBIS-RA, such as the expertise and motivation of key actors, the around-the-clock schedule, the high staff turnover, the complexity of the model, and the challenge of engaging all staff members. These findings contribute to a better understanding of adapting the PBIS model in a residential setting for autistic individuals and provide valuable insights to guide future implementation efforts.
Positive behavior intervention support (PBIS) is an evidence-based and widely implemented approach created in the mid-1980s (R. H. Horner et al., 1990). Many definitions of PBIS exist, but for the purposes of this paper, we will refer to R. H. Horner et al. (2017) who describe PBIS as a framework for selecting and implementing evidence-based practices within a multi-tiered continuum of behavioral supports that result in social, emotional, and academic success for all individuals. PBIS may be applied at the level of the individual and the level of larger systems (e.g., families, classrooms, schools). PBIS has become common in school settings, and many studies support its efficacy (Center on PBIS, 2020). In recent years, researchers and clinicians have begun implementing PBIS in other contexts such as juvenile justice facilities (McDaniel et al., 2014; Sprague et al., 2013) or childcare centers (Ai et al., 2022), as evidence suggests that the positive effects of PBIS extend beyond schools. This expansion has led proponents of PBIS to adapt the model to these clienteles. Varying clinical contexts have also produced new challenges for PBIS implementation given its complexity (Cohen et al., 2007; Tobin et al., 2012).
PBIS has been used with autistic individuals in schools (Crosland & Dunlap, 2012; Goh & Bambara, 2012), family (Blair et al., 2011; Lucyshyn et al., 2007; Singh et al., 2021), or in work environments (Schall, 2010). Autism 1 is a neurodevelopmental condition characterized by a qualitative impairment in social communication and interaction, and by restricted, repetitive, and stereotyped behaviors (American Psychiatric Association, 2022). Autistic people may also experience peculiarities in sensory input processing and exhibit impairments in adaptive functioning (Ray-Subramanian et al., 2011; Takarae et al., 2016) and intellectual functioning (Charman et al., 2011). The clinical picture becomes more complex as autistic people age. Adults have the same support needs as younger people (e.g., language development, occupational therapy, socialization, education, health care), but also have needs related to access to occupation, independence, and housing. A proportion of autistic adults require substantial support throughout their lives and need a residential environment that provides professional support.
Our research team partnered with a Foundation whose mission is “to create long-term, adapted living environments for autistic people aged 21 and over with an intellectual disability (ID).” The Foundation built a residence designed for autistic individuals and asked our research team to propose an evidence-based intervention approach to create an environment where residents could develop their potential and autonomy. We proposed the PBIS approach as it could provide a structured, positive atmosphere. We chose to conduct this project through co-construction, an approach defined as an equal partnership between the research team and a non-academic organization, that encompasses all phases of the project from design to analysis (L. K. Horner, 2016). Co-construction ensures the relevance and applicability of our findings, enriches understanding through diverse perspectives, and increases stakeholder engagement.
Few studies exist on the effects of PBIS on the adult autistic population. Two studies have evaluated the effects of PBIS in a residential context. McGill et al. (2018) showed that PBIS implementation in a residential setting for autistic and intellectually impaired adults reduced challenging behaviors. Lubar (2018) found that direct care workers who worked with clients with heterogeneous diagnoses, such as brain injury, mental health, and autism, experienced higher levels of self-efficacy. However, no difference was found in their incidence of burnout. Both studies focused on PBIS effects without evaluating the implementation quality. Bosco et al. (2019) evaluated the implementation of PBIS in community services for adults with ID. They reported staff appreciation for PBIS and its potential impact on challenging behaviors, but they also identified challenges such as staff turnover and the high level of resources required (Bosco et al., 2019).
To contextualize results, increase generalizability, and guide future implementation, experts recommend evaluating implementation before analyzing a program’s effects (Durlak & DuPre, 2008; Gottfredson et al., 2015). Implementation outcomes, such as acceptability, adoption, feasibility, sustainability, and fidelity are essential for a program to have the desired effect (Proctor et al., 2011). The Consolidated Framework for Implementation Research (CFIR) is one of many theoretical approaches used to understand implementation successes or failures of interventions in organizations (Nilsen, 2015). CFIR describes the type of determinants that may act as barriers and facilitators to innovation in a health services organization, emphasizing the role of internal and external contexts (Damschroder et al., 2009, 2022; Nilsen, 2015). This framework has also recently been used in autism research to explore the implementation of a patient navigation tool for accessing services (Broder-Fingert et al., 2018), the training of coaches to support parents (Mirenda et al., 2022), a transition to adulthood program (Kuhn et al., 2022), and a parent-mediated autism intervention (Carruthers et al., 2022).
As such, we considered it essential to document adaptations to the PBIS model for autistic adults with significant support needs and explore implementation issues considering this organization’s specific challenges (around-the-clock schedule, staff turnover, diversity of resident clinical profiles), before measuring the effect of the PBIS-RA model on the residents. For this study, our objectives were to (1) adapt the PBIS model to a residential setting for autistic adults with ID and evaluate its implementation by (2) identifying barriers to and facilitators of implementation, and (3) assessing the fidelity of implementation.
Method
Our research project design is a case analysis (Miles et al., 2014) of the PBIS-RA adaptation and implementation in a residence for autistic adults. Our data come from several sources, allowing for their triangulation during analysis (Patton, 2015): field notes of the research team during the project; the PBIS-RA committee’s work and meetings documentation; interviews with the staff; analytical workshops to discuss observations and reflections of the research and clinical teams; and observation of the staff’s work.
Participants
As this project was the result of a close collaboration and prolonged engagement between the residence clinical team and the research team, we consider each actor to be a research participant. The research team, all non-disabled women, consisted of three university professors: MMD (researchers’ initials are used for conciseness) is trained in psychoeducation and has been a clinician and researcher working with autistic individuals for the past 10 years; MA has extensive training in PBIS and has participated in the development, implementation, and evaluation of PBIS programs in daycare, residential settings, and schools with an autistic population; and VM is the parent of an autistic teenager and has multidisciplinary training in psychoeducation, management, and program evaluation. The team also included a PhD student (MH) with clinical expertise working with autistic children and adults in school and residential settings, as well as a post-doctoral student (IP) trained in psychoeducation with 9 years of research and clinical experience in autism. The Residence team included: the head of research and development (R&D), trained in social work, psychology, and autism intervention with 14 years of experience; and two clinical managers first hired as staff members. Finally, 24 women and 2 men staff members participated in the study (n = 26). Half of the employees were college educated (50%), 19% had an undergraduate university degree, and the rest were divided between high school, postgraduate, or another level of education. Employees had an average of 7 years of experience working with autistic individuals (0–24 years).
The Foundation partially funded this research through a non-profit national research organization (MITACS). As such, the researchers maintained their independence throughout the study and are fully responsible for the final analysis. Residential staff who participated in this research signed a consent form explaining the goal of the project and confirming that they could refuse to participate without consequences. The Research Ethics Committee of the Ministry of Health and Social Care approved this project (CCER21-22-04), which we conducted in accordance with the Canadian Tri-Council Policy Statement on Ethical Conduct for Research Involving Humans.
Setting
Our research setting was a newly constructed residence for 16 autistic adults with ID, which opened in 2021. The Residence is divided into four units of four individual quarters plus a shared living room and bathroom. Residents also have access to various common indoor and outdoor areas. The staff, present at all times, includes special educators, direct support workers, overnight support workers, a cook, and the head of R&D. The operating costs of the Residence are covered by the public health and social services network, with additional funding provided by the Foundation. The local public health and social care organization remains responsible for client follow-up and can provide specialized professional interventions if needed. Still, the Residence provides support to residents above what is typically seen in such settings.
Procedures and Timeline
The first step of our project was the creation of a PBIS-RA committee to collaborate with the research team (see Appendix A, online supplemental material). The purpose of this committee was (a) to adapt the original PBIS model to the context of the Residence and to the clientele’s needs; (b) to plan and support the implementation of the PBIS-RA using a template “agenda” created for this purpose (see Appendix B, online supplemental material); and (c) to sustain the PBIS-RA program at the Residence over the long term. The committee consisted of eight volunteer staff members who worked in a variety of roles (e.g., special educators and personal care workers) on both day and evening shifts. The meetings took place during shift changeover time every 2 weeks. Committee members also rotated, with some staff replacing others as implementation progressed.
Members of the research team (MA, VM, and MH) provided an 8-hour in-person training to the staff at the beginning of the project. Staff members who joined in the following months completed an online training course, created by the research team, which included 11 modules on each component of the PBIS-RA model. Over 8 months (between June 2021 and January 2022), the research team and committee members collaboratively built the adapted PBIS-RA model. During this period, the graduate students (MH and IP) facilitated 26 meetings of the PBIS-RA committee. The main topics were determination of the Residence values, development of the behavioral matrix, creation of visual supports, explicit teaching and promotion of expected behaviors, development of the reinforcement system, and development and implementation of the dedicated information system (Explorateur). The research team facilitated five additional committee meetings until September 2022. Thereafter, PBIS-RA committee held meetings every 2–4 weeks, for a total of 17 meetings. A member of the research team reviewed the agenda after each meeting and provided support when needed.
In February 2022, the behavioral matrix was displayed, and staff started applying the PBIS-RA model by teaching behavioral expectations and reinforcing expected behaviors. Still, the co-construction and implementation process was iterative, and each component could be revised. Delays arose in implementing the Explorateur component. In addition, the quality of the data entered in the system revealed a lack of understanding by staff of the concepts of antecedents, behaviors, and consequences (ABC). The research team created an impromptu training on the ABC sequence and the type of information needed to derive the function of the behaviors. A total of 27 individuals were trained, consisting of the attendants and educators in service at that time. The 27 employees were organized into subgroups with similar training needs, and the training sessions took place between January 1, 2023, and May 1, 2023. Throughout this project, the head of R&D and the research team also held several additional meetings as needed to monitor implementation progress or solve issues.
This co-construction process ensured that the proposed adaptations were directly related to the real needs of the clinical environment, and were therefore age, culturally, and contextually appropriate. The results of Objective 1 are the outcomes of this process.
Framework
We chose to use the CFIR, a pragmatic meta-theoretical framework that explores “the dynamic, multi-level, transient nature of implementation in specific contexts” of evidence-based practice in health care services or other areas of professional practice (Damschroder et al., 2009; Nilsen, 2015). This framework considers the organizational implementation of the PBIS-RA, from the selection of the model by the organization, to the allocation of the resources for the project, to the daily use of the model by the staff. The CFIR considers five major domains identified in the literature as influencing implementation outcomes (Damschroder et al., 2022; Proctor et al., 2011). The innovation domain considers, among other things, the evidence base, the advantages of the innovation over current or alternative solutions, its adaptability, and its cost. The inner-setting domain considers constructs such as the structural and cultural characteristics of the organization, the attitude toward change, and readiness for implementation. The outer setting domain looks at the influence of determinants outside the organization such as incentives, stakeholder policies, and regulations. The individual domain refers to the attitude and behavior of individuals in the organization, from the high-level leaders to the personnel delivering the innovation, including the innovation recipients. Finally, the implementation process domain includes the assessments of context and needs, implementation planning, engagement, and reflection on progress and experiences (Damschroder et al., 2009, 2022). We selected the CFIR after reviewing our data and considering various frameworks related to implementation (Nilsen, 2015). The CFIR was aligned with our research questions, addressed both organizational and individual levels of change, and captured the organizational and wider social context (Chambers, 2014).
Measures
To achieve Objective 2 (“identify barriers to and facilitators of implementation”), we developed a semi-structured interview outline for employees to address their perception of the implementation process. A master’s degree research assistant, not previously involved in the co-construction and implementation of the model, conducted 24 video interviews with the residence staff between November 2022 and April 2023, representing about 88.8% of total staff (see Appendix C, online supplemental material). We also developed a discussion outline based on CFIR’s main components to guide two analytical workshops (see data analysis section).
To address Objective 3 (“assess the fidelity of implementation”), we used the Preschool-Wide Evaluation Tool (PreSET; Steed & Pomerleau, 2012). This tool assesses universal program-wide PBIS implementation in early childhood. The PreSET is divided into two sections: a 15- to 20-minute interview with the program administrator and a 15- to 20-minute observation period. To our knowledge, no other assessment exists to evaluate the fidelity of PBIS implementation in residential settings. Therefore, the PreSET was translated into French and adapted to the residential setting. For example, the structured activities usually observed in the initial PreSET (ex: snack time) were adapted to a meal observation with the residents. The adapted PreSET was administered by a trained professional, who was not involved in the other steps of the project and had 5 years of experience using this tool.
Data Analysis
The analysis method for Objective 1 consisted of organizing and comparing documentation to map out the adapted PBIS-RA model against the components of the setting-wide PBIS (SW-PBIS) model (Simonsen et al., 2011).
For Objective 2, we recorded and transcribed staff interviews using Trint software (Trint, 2022). Two research assistants, with checks by one researcher, coded the interviews with first-level descriptive and protocol codes based on a preliminary list drawn up from the scientific literature and our research objectives (Miles et al., 2014). We added additional codes as they emerged from our analysis. For this study, we analyzed the codes addressing barriers and facilitators of the implementation of the PBIS-RA. Members of the research team (MMD, VM, IP, MH) held a 3-hour analytical workshop to discuss their field notes, documents, experiences, and coded staff interviews. The second analytical workshop with the research team, the Residence team (the head of R&D, the Residence general manager, and the person responsible for programming and clinical activities) was recorded for detailed notetaking. The CFIR constructs guided the discussion during both workshops and allowed us to identify factors that influenced the implementation of the PBIS-RA, as well as the direction and extent of that influence, including the interplay between factors. In discussing our data, we actively sought out disconfirming evidence and alternative explanations to foster a shared understanding, while remaining open to different perceptions (Patton, 2015). For both workshops, one researcher (VM) and a research assistant took detailed notes. These data were used to develop a thick description of the events, allowing for a reflexive posture as researchers and research participants (Patton, 2015). The research team re-examined the synthesis of both workshops, comparing with employees’ interview and looking for corroborating, inconsistent, and conflicting findings (Miles et al., 2014) to arrive at a final interpretation of the essential factors related to the implementation outcomes of PBIS-RA in the Residence.
For Objective 3, the professional applied the scoring procedure of the PreSET tool (Steed & Pomerleau, 2012) and commented on the elements specific to this environment. Finally, the comments of the head of R&D on the final manuscript served as a member check procedure to assess the confirmability of our interpretations (Lincoln & Guba, 1985). She did not identify any factual errors or discrepancies between our conclusions and her understanding of, or her experience implementing the SCP-RA, thereby strengthening our confidence in the validity of our interpretations.
Results
Objective 1. Components of Our Adapted PBIS-RA Model Compared to the Original Five Core Components of PBIS
This section presents the PBIS-RA model we developed with the PBIS-RA committee. Consistent with other writings on implementing PBIS models in alternative settings (Simonsen et al., 2011), we first present the five core components of the setting-wide PBIS (SWPBIS) model, then the additional components to adapt the model to autistic adults living in the Residence.
Core Component 1: A Clearly Stated Purpose and Approach for SWPBIS
The PBIS-RA model relies on the commitment of management and staff to implement it. The Foundation opted for PBIS because this model was consistent with its mission and its values of respect, commitment, self-determination, and innovation. The members of the PBIS-RA committee chose three values for the Residence: respect, commitment, and self-determination.
Core Component 2: A Few Positively Stated Behavioral Expectations
We determined behavioral expectations by creating a matrix of expected behaviors. Each value was translated into explicit behavioral expectations for each living area. Through these behavioral expectations, we aimed to foster a living environment that would support everyone’s potential while promoting a positive cohabitation. The behavioral expectations were designed to respect the residential context. In total, the matrix contains 77 expected behaviors divided across 12 living areas: Hallways and staircases (3), Activity room (6), Locker room (5), Large living room (7), Gym (7), Dining room (8), Small living rooms (8), Bedrooms (7), Bathrooms (7), Pool and spa area (8), Backyard (5), and Laundry room (3). Three additional behaviors are applicable in all settings; Appendix D (online supplemental material) shows an excerpt from the matrix.
Core Component 3: Procedures for Directly Teaching These Behavioral Expectations
We developed lesson plans to teach the behaviors listed in the behavioral matrix. We taught each behavior using explicit teaching (Bissonnette et al., 2016): (a) explain the behavioral expectation, (b) model the behavior, (c) practice the behavior (adapting the prompting and support to the resident’s needs), and (d) reinforce behavior and promote generalization. We created visual aids in the form of pictograms illustrating steps of expected behaviors to support learning (with varying levels of adaptive and intellectual functioning). To facilitate explicit teaching, the head of R&D created groups of residents sharing the same support needs for learning new behaviors. Teaching took place one living area at a time, starting with places where expectations were simpler (e.g., walking in the hallway) and ending with places where expectations were more complex (e.g., washing clothes in the laundry room).
Core Component 4: A Continuum of Strategies for Positively Reinforcing Displays of These Behavioral Expectations
The PBIS-RA committee opted for a three-level reinforcing model adapted to the Residence: individual, unit, and whole residence. Residents’ behaviors were randomly reinforced with PBIS coupons paired with a specific social reinforcer. Once a week, residents exchanged their coupons for items in the residence’s Rewards Store. Given the variable characteristics of the residents, the price of the items was individualized to ensure that every resident had access to them. These items included sensory objects, desired objects (e.g., pencils and stickers), special hygiene items, and a list of privileges (e.g., choosing the dessert of the day). The other two levels of reinforcement relied on interdependent group contingencies (Collins et al., 2019), in which reinforcers are delivered when the group meets a criterion. Besides coupons, residents earned points for their unit in the form of marbles accumulated in a see-through container. Once a unit reached its goal, its members won a reward activity. Finally, each time a unit reached its marble goal, the residents placed a large ball in a transparent cylinder corresponding to a goal for the whole residence. When the cylinder became full, the Residence held a special activity involving all residents. This continuum of strategies required knowledge of both residents’ interests and abilities. Thus, the “promotion of expected behaviors” component differed from the usual PBIS in its level of individualization and its concrete nature (e.g., transparent marble jars) to facilitate residents’ understanding.
Core Component 5: A Continuum of System-Wide Consequences for Noncompliance
We did not develop consequences for noncompliance as opposed to what is done in school settings (i.e., suspension and expulsion) as this is not appropriate for adults or alternative settings (Simonsen et al., 2011). We therefore opted for a positive behavioral perspective to manage challenging behaviors: the individual exhibiting such behavior is perceived as having a problem (not as being the problem), which implies that employees can help the resident find solutions. In this view, the challenging behavior expresses as an unmet need, and the individual is supported in expressing this need in a prosocial way. To this end, we set up an information system (Explorateur) to collect data on challenging behaviors with the aim of understanding their function and guiding interventions. We trained employees to use Explorateur and fill in descriptive analysis grids (antecedents, behaviors, consequences). Given the staff’s varying familiarity in completing such grids, a member of the research team evaluated a few copies of the grids to provide feedback. The grids were regularly analyzed during clinical meetings facilitated by the Residence general manager and the head of R&D. This way of managing challenging behaviors is consistent with the National Institute for Health and Care Excellence Guidelines (NICE, 2018), which recommend fully understanding developmental difficulties and challenging behaviors before proposing solutions.
Additional Components Co-Constructed With the PBIS Committee
Additional Component 1: Autism and the Needs of Autistic Adults
We added this component to ensure that staff had a sufficient knowledge and understanding of the adult autistic clientele and their daily needs.
Additional Component 2: Quality of Life and a Positive Approach
Given the context of a residential setting, we added this component to sensitize the staff to the notion of quality of life for autistic adults. We discussed the physical, psychological, social, and environmental dimensions of quality of life (Sáez-Suanes & Álvarez-Couto, 2022). To illustrate the concept, we provided examples of how to promote the quality of life for autistic people (e.g., providing them with responses adapted to their needs, ensuring consistency between the actors in the environment, offering them access to occupations adapted to their level of development and interests).
Additional Component 3: Involvement of Family
Maintaining relationships between residents and their families, as well as fostering communication between the Residence and residents’ families, was an important goal of the Foundation. We added a component on information for families and their involvement in the life of the Residence. Residents’ families were also invited to an information session on the PBIS-RA model, facilitated by the research team (MH and IP), in the presence of the head of R&D where parents had the opportunity to ask questions about the model and its implementation. Staff communicated with families via email, phone, or Class Dojo, a mobile application that allows users to send messages and photos. The frequency of communications, along with the involvement of parents, was individualized, as some residents were previously living with their family and others had been living in another residential setting.
Additional Component 4: Organization of the Physical Environment and Programming
The Residence was built specifically for the Foundation by architects based on a university report outlining the design principles for an autism-friendly environment. Creating a home atmosphere (i.e., making residents feel at home) and a physical structure supporting resident functioning were deemed important. The Residence general manager developed the programming with the aim of balancing free time, structured activities, and housekeeping tasks. The organization of physical space and time supports the functioning of autistic individuals (Mesibov et al., 2012) and corresponds to a universal intervention in a response-to-intervention model (Fox et al., 2010).
Objective 2: Barriers to and Facilitators of PBIS-RA Organizational Implementation
Our analysis led to the identification of elements that influenced the organizational implementation process of the PBIS-RA in all domains of the CFIR framework. Indeed, elements of the outer setting (OS) and the inner setting (IS) of the organization, the innovation characteristics (IN), the individuals (IND), and the implementation process (PR) contributed either to facilitate or impede the implementation of the model (see Figure 1; see Appendix E, online supplemental material for detailed descriptions).
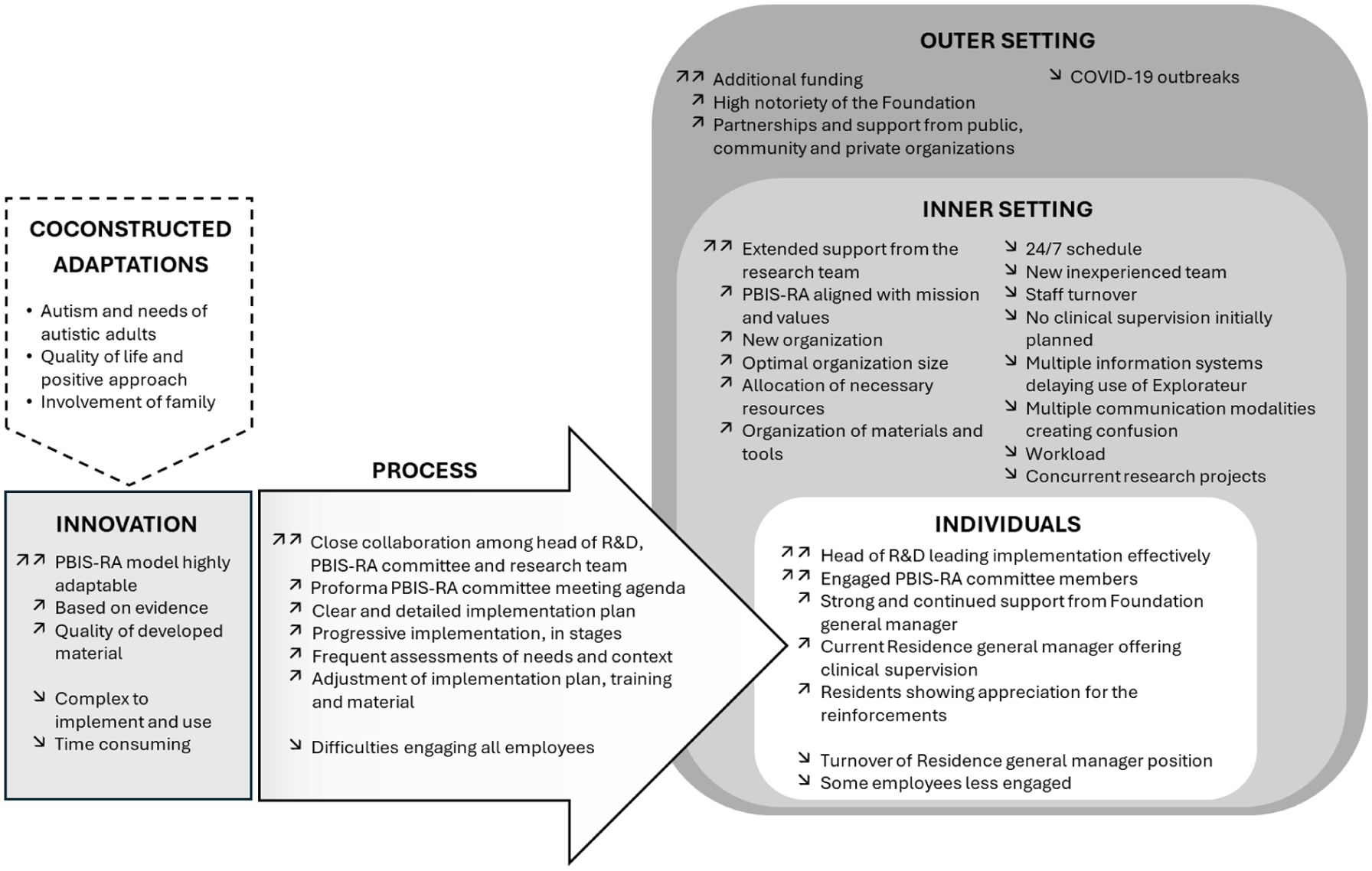
CFIR Elements Facilitating or Impeding the Implementation of PBIS-RA.
Facilitators of Implementation
Many factors supported the implementation of PBIS-RA. First, the Foundation was created by high-profile entertainers of the local cultural scene (OS) wanting to develop an innovative residence model supported by research (IS). The Foundation’s notoriety helped enlist the support from governmental decision makers, the regional health and social services authorities, local businesses and organizations, and major donors toward this innovation (OS). The research team considered the additional funding, above the usual funding for housing resources for this clientele, essential to support the implementation of the PBIS-RA (OS). However, during the workshop, the Residence team, indicated that without this additional funding, implementation would have been possible, but more difficult.
The Foundation’s management team selected the PBIS because of its evidence base (IN), even if certain advocacy groups considered it controversial, as noted by the Residence team. Both the research and Residence team, during the workshops, considered the adaptability of the PBIS model an essential factor that explains the success of the implementation, as each component of the model was adapted to the Residence (IN). The quality of the co-constructed material was also a factor contributing to the implementation according to the staff (IN): “We have all the tools necessary to apply the matrix. The behaviors that are displayed everywhere, so even if, let’s say, I didn’t remember one of the expected behaviors. It’s here” (participant E12).
The head of R&D, as implementation lead (IND), played an essential role: she coordinated efforts, provided clinical leadership, and effectively managed the implementation process. Her prior experience enabled her to offer expert support on the PBIS-RA model. She also received a strong mandate and ongoing support from the Foundation’s General manager (IND) as well as the necessary resources for the project (IS). Another essential element facilitating the implementation was the rigorous and structured work of the engaged PBIS-RA committee members (IND). Their work offset the negative effects of turnover in the Residence general manager position during the project. The PBIS-RA committee also relied on the long-term support of the research team (IS). The collaboration between the implementation lead and the research team was harmonious, based on trust fostered by previous collaborations (PR).
A clear and concrete implementation plan was adopted, then regularly revised to adapt to unforeseen events or other priorities (PR). The team carried out implementation progressively in stages, for example, by teaching expected behaviors one living area at a time (PR). The team also made many adjustments to meet the organization’s needs, such as retraining some staff members, simplifying the reinforcement strategies, and impromptu data collection to adjust the implementation process or understand hesitations about the model (PR). This also led to the creation of online training for new employees because of staff turnover.
The context of a new organization was a facilitating factor for implementing the PBIS-RA according to the Residence team, as there were no prior habits to change. The organization was large enough to provide structure and administrative support while still allowing for easy communication and momentum for the implementation (IS). Residence staff seem to have mobilized around the Foundation’s values of respect, commitment, and self-determination integrated into the PBIS-RA model (IS). The current Residence general manager reinforced the motivation of the staff toward the model by demonstrating the positive changes associated with it, including during her supervisory meetings with the staff (IND). Also, residents showed their appreciation for the reinforcements they received (IND). Finally, the reorganization of the materials and the rooms helped remind residents of expected behaviors, and coupons were placed in employees’ fanny packs for easy access when reinforcing expected behaviors (IS).
Barriers to Implementation
Turnover in the Residence general manager position was a barrier to implementation. In addition, the first two general managers were indifferent or did not embrace the model, which demotivated the PBIS-RA committee and certain employees (IND). As this was a new organization, the team was young, with no cohesion, and some employees had little experience with the autistic clientele (IS). The around-the-clock schedule also added challenges because the staff had to be replaced when participating in initial training or PBIS-RA committee meetings. High staff turnover also meant planning training for sixteen new employees over the course of the project (IS). Multiple information systems, some imposed by the public health and social services network, led to delayed implementation and reduced the use of Explorateur (IS). The Residence team workshop found that the cumulation of multiple communication modalities, such as email, clinical information systems, shift changes discussion, complicated communication on the PBIS-RA (IS).
PBIS-RA implementation may also have been stunted by employees’ involvement in other research projects in the Residence, or simply because of their workload: “The moments when we’re more like in the action, and we’re busier, doing it, then, sometimes we forget about it” (participant 20; I). Moreover, committee meetings and all non-essential activities were suspended during COVID-19 outbreaks (OS).
Both the research and Residence team deemed the PBIS-RA complex to implement. Many small but necessary tasks were needed to create the material. The Residence team felt, during the workshop, that the model was time-consuming, because it needed to be done every day, all day, by all staff. Staff echoed this: “There is a lot going on here. We’re overwhelmed. But I think we need to take the time to do it more” (participant E07). They also conveyed that using the model required extensive support from the PBIS-RA committee to develop their knowledge (IN; IND). According to the Residence team during the workshop, this makes the model costly, as it involved a lot of staff time (IN).
A major barrier to the implementation process was engaging the staff beyond members of the PBIS-RA committee. Initial training and communication proved insufficient (PR). This was particularly challenging when the first Residence general managers did not provide clinical supervision. As such, a gap emerged between the members of the PBIS-RA committee who adhered to the model and employees who used it either infrequently or not at all: “Not everyone applies it in the same way, or with the same rigor. That’s why, sometimes. . . you know, residents don’t necessarily follow” (Participant 19; IND). Some even questioned residents’ understanding of the expected behaviors and the reinforcement strategies (IND).
Objective 3. Fidelity of Implementation
The PreSET was conducted 1 year after the beginning of the PBIS-RA implementation. A score of 70% implementation fidelity was achieved, which is considered excellent for a residential setting implementation of just under 2 years. We would expect to see between 40% and 60% for this timeline, as stated by the original PreSET (Steed & Pomerleau, 2012; see Appendix F, online supplemental material). Specifically, the components “expectations defined” and “monitoring and decision-making” scored the highest. This means that the program had three positively stated expectations applicable to the residents, which were posted publicly throughout the Residence with visual supports and relevant appropriate behaviors for different settings and activities. The Explorateur information system was used daily to document residents’ occurrences of challenging behavior and a clinical team regularly reviewed this data.
The lowest scoring components were “behavioral expectations taught” and “program support” Both results showed that despite having clearly stated behavioral expectations in the program, the staff was not incorporating them into everyday routines and activities. Also, though daily schedules were posted in the Residence, the staff did not refer to them, yet visual cues can enhance autistic residents’ participation in everyday activities. The research team made recommendations to the Residence to address the PreSET scores and help the clinical team make improvements.
Discussion and Conclusion
This study aimed to describe the co-construction and implementation of a PBIS model adapted to a residential setting for autistic adults with ID. We used a case analysis design, combining multiple information sources, to adapt a PBIS model, to identify factors explaining the implementation process of the PBIS-RA model, and to evaluate the fidelity of its implementation.
The new components added to the original five core components of the PBIS, and the co-construction process with the PBIS-RA committee, ensured that the adaptations were specific to the residential setting and its residents. The adaptability of the model was a main factor in the success of the implementation. To engage the management and the staff toward the model, it was crucial for the leadership team, employees, and researchers to adapt the model to the residents’ traits, the organization’s values, and the Residence’s operational features. Still, the complexity of the model, including the resources and cost associated with its implementation and maintenance, suggest the importance of a continued active PBIS-RA committee and support from high- and mid-level managers. The importance of resources needed for the delivery of PBIS was also mentioned by Bosco and colleagues (2019). PBIS-RA depends on the daily involvement of all staff to apply strategies and activities. For this reason, training is a challenge due to staff turnover (Bosco et al., 2019), as this industry has an annual turnover rate between 24% and 70% annually (Bogenschutz et al., 2014). For this reason, we developed an online training on PBIS-RA that was added to the onboarding of new employees in the residence.
McDaniel et al. (2014) also examined the barriers and facilitators to system-wide PBIS implementation in an alternative education system. They found that obtaining staff buy-in was difficult because of the additional work involved in what was perceived as a top-down approach to implementation. This points to the importance of the internal context of the organization and the attitudes and behaviors of its leaders when implementing a PBIS model. They also mentioned that data collecting, analyzing, and implementing the model was initially difficult. In our study, the delayed implementation of the Explorateur information system also contributed to difficulties in using data for decision-making regarding challenging behaviors.
The CFIR provided a useful framework to observe key elements that explain implementation success and possible challenges. It led to the identification of less-obvious factors, such as the role of external organizations for support, collaboration or funding, or the role of organizational characteristics, such as the around-the-clock schedule, the multiple communication modalities, as well as well-known factors such as the influence of the Residence general managers. The PreSET also allowed the research team to assess implementation fidelity with a validated tool, albeit one not specifically designed for a residential setting. This assessment, made by a professional uninvolved with the project or research team, added valuable information to our case analysis.
The strengths of the study lie in the multiplication of information sources and the pooling of these data. Triangulating data enabled us to paint a nuanced picture of our case study. Each stakeholder group offered a complementary perspective. The staff revealed practical elements that influenced the implementation of the model, the management team addressed mostly internal issues, and the research team identified several aspects of the external context. While anchored in a specific setting, this case study thus provides lessons for other residential settings in implementing interventions based in the everyday practice of the personnel. Finally, our results contribute to the advancement of knowledge by adapting the SWPBIS model to a residential setting for autistic people with ID for the first time and implementing it with a high level of fidelity. Studying factors influencing the organizational implementation of the PBIS system also provides useful lessons for similar clinical settings.
One limit of the study is that the PreSET tool used to assess implementation fidelity was not adapted to the residential environment nor the PBIS-RA model. As a result, only the five core components were evaluated. Other components added to meet the clientele’s needs were not evaluated, resulting in an incomplete portrait of the model’s implementation. A second limitation is that we did not investigate residents’ appreciation and perception of the PBIS-RA model. This is an important aspect as staff who were less engaged with the model expressed doubts about the resident’s understanding of reinforcer delivered. Moreover, we did not measure the impact of PBIS-RA on the occurrence of challenging behaviors. Finally, as this is a case study, the transferability of our results might be limited, yet our in-depth descriptions allow for usability of our findings in other contexts (Miles et al., 2014).
Replication studies are needed to examine the adaptation and implementation of PBIS-RA and to explore variations associated with different autistic adult clientele, residential settings, organizational modalities, staff, or external factors. The next step would also be to comprehensively evaluate the effects of the PBIS-RA model, on both resident behavior and staff’s well-being. A tool specifically adapted to the autistic adult residential context should also be developed to more accurately assess implementation fidelity, considering the particularities of this clinical setting. As well, using a tool such as the Performance Diagnostic Checklist—Human Services (PDC-HS) could provide a better understanding of failure of employees to implement PBIS-RA activities (Brand et al., 2022). Finally, future studies should include residents’ appreciation and perception of the model.
Supplemental Material
sj-docx-1-pbi-10.1177_10983007251389270 – Supplemental material for Co-construction of a Positive Behavior Interventions and Supports Model in a Residential Care Setting for Autistic Adults: Exploring Implementation Barriers and Facilitators
Supplemental material, sj-docx-1-pbi-10.1177_10983007251389270 for Co-construction of a Positive Behavior Interventions and Supports Model in a Residential Care Setting for Autistic Adults: Exploring Implementation Barriers and Facilitators by Marie-Michèle Dufour, Valérie Martin, Isabelle Préfontaine, Mélissa Hogan and Malena Argumedes in Journal of Positive Behavior Interventions
Footnotes
Funding
This research project was supported by a grant (# IT25505) from MITACS—Accélération to the last author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.