
Abstract
The current study is the first to examine whether the positive effects of the School-Wide Positive Behavioral Interventions and Supports (SWPBIS) model, previously documented as effective in the school context, may generalize to the home context. Potential benefits for children and parents were investigated longitudinally. A randomly selected subsample of Norwegian students drawn from a larger dataset and considered at respectively low, moderate, and high risk of developing conduct problems was rated by their parents at five time points across four successive school years. Only the fourth graders were included in the analyses to follow a stable group of students over time. Data were analyzed using linear mixed models. The outcome variables examined were parent-rated problem behavior and social skills, monitoring, mental health, support to the child’s schooling, and school–home cooperation. The analyses revealed no significant benefits of SWPBIS in the home context, neither for the children nor the parents. Likewise, no differential effects for low-, moderate-, and high-risk groups were detected. To increase the odds of cross-domain effects of the SWPBIS model, the inclusion of additional intervention components to better inform, include, and support parents should be considered, particularly for parents of students with more severe behavior problems.
Research strongly suggests that universal school-wide prevention approaches significantly reduce children’s conduct problems and aggressive behavior (Bradshaw et al., 2010, 2012; Durlak et al., 2011; Mitchell et al., 2018). Among the most successful interventions is the School-Wide Positive Behavioral Interventions and Supports (SWPBIS) model. Several systematic reviews and meta-analyses (Chitiyo et al., 2012; Horner et al., 2010; Lee & Gage, 2020; Noltemeyer et al., 2018; Solomon et al., 2012) conclude that SWPBIS is a highly promising intervention model for the prevention of externalizing behavior problems among students, for improving the learning/classroom climate, and for improving safety in elementary and middle schools.
The SWPBIS model (called PALS in Norway) has also been evaluated in several longitudinal effectiveness studies, with encouraging outcomes for students, teachers, and schools (e.g., Borgen et al., 2021; Sørlie et al., 2016, 2018; Sørlie & Ogden, 2015). Positive effects have also been registered for an abbreviated version of the model (Sørlie et al., 2015). However, to the best of our knowledge, generalizability effects to the home environment have not been examined, neither in the Norwegian effectiveness studies nor in other SWPBIS studies. It is therefore unclear if the parents experience child behavioral improvements or other benefits from the school intervention. In most school-based intervention studies, teachers and students are the primary informants. Parent assessments are seldom included to identify potential child behavioral changes at home or changes in the parent’s situation. In the current study, we attempt to fill some of these knowledge gaps by examining if the SWPBIS model, as implemented in Norway, had any effect on parental reports of the family situation.
The School-Wide Positive Behavior Support Model
The SWPBIS model is a broadly implemented intervention worldwide, which aims to prevent moderate and serious student behavior problems (Michael et al., 2023). The main intention of the model is to replace reactive and punishment-oriented disciplinary approaches with one that promotes positive behavior support. The model was developed in the United States and Norway was the first European country to follow suit. Only surface changes were made to match the model to the Norwegian cultural and linguistic context (Sørlie & Ogden, 2015). The model is a multitiered, structured, yet flexible, approach to promote a safe and inclusive learning environment and to prevent and reduce antisocial behavior in students (Sprague & Walker, 2005). Social skills are added to the behavioral expectations taught (Gresham et al., 2001). The core intervention components are similar in the American and the Norwegian versions and include (a) positive relationships, (b) school-wide expectations as a few positively formulated rules and prosocial skills, (c) positive directions and instruction, and (d) positive behavior support including encouragement, recognition, and positive involvement.
The intervention model consists of three tiers of prevention and intervention: a universal, selected, and indicated tier. All interventions should be evidence-based and matched to the students’ needs. The universal Tier 1 interventions apply to all students in all school arenas, while selected interventions at Tier 2 are intended for the 10–15% of the students who do not benefit sufficiently from the universal interventions. The indicated interventions at Tier 3 are intended for the few students (1–4%) at high risk of conduct disorder. Based on individual needs and risk assessment, they are offered individually tailored and intensive interventions. The selected level has the same objectives as the universal but offers intensive small-group teaching for limited periods. The school model further relies on a team-structured organization and implementation, and each school appoints a team of five to six representatives, including parents and the principal, to make plans, train their colleagues in essential features of the intervention model and implementation structure, and routinely report on the outcomes and implementation fidelity at their school. To monitor the quality of the implementation (fidelity), the “Effective Behavior Support Self-Assessment Survey” (Sugai et al., 2009) or other fidelity measures should annually be completed by the teachers or implementation team. After completion, each school gets its their fidelity results in the form of easily understandable graphs.
The School-Wide Positive Behavior Support Model and Parents
In Norway, the SWPBIS model is implemented in the school setting with no pronounced intentions of changing either student behavior or parent behavior at home. Descriptions of the model contain little information about the goals, the specific content, and guidelines for school–home cooperation. Still, according to the Norwegian handbook, parents should be fully informed about the schools’ plan to implement the model, and their participation in the school’s implementation or leader team is recommended (Arnesen & Meek-Hansen, 2010). Moreover, general recommendations are made for extended school–home contact and collaboration when students require additional help and support. Although not included among the core components, teachers are encouraged to make home visits, and parents are asked to encourage their children to attend school, get to school on time, pay attention in lessons, and behave positively. The recommendations emphasize the importance of good school–home relationships, but there are few indications that this collaboration receives much attention. In the United States, efforts have been made to help schools integrate research-supported family engagement strategies more systematically into the tiered support system to get away from the often random and event-based strategies used in many schools (Garbacz et al., 2018; Weist et al., 2017).
To our knowledge, no studies have evaluated the extent to which the recommendations related to family engagement are implemented in practice. Neither did our review of the literature uncover any prior attempts to evaluate the potential crossover effects of the SWPBIS model to the home context nor any parent assessments of change. In this study, we thus aimed to investigate if there are any significant generalization effects of the SWPBIS model from school to home in Norway, and by that, contribute with research-based knowledge on how this school-wide prevention model might influence the parents’ situation and children’s behavior at home.
School-Based and Home-Based Interventions and Generalizability of Outcomes
Some children act out both at school and at home, but most structured intervention programs for the prevention and reduction of child conduct problems are carried out either at school or at home. They address parent and teacher assessments separately and most school-based programs only report on teacher and/or student assessments. For example, Wilson and Lipsey (2007) reported that 70% of the school-based studies assessing aggressive/disruptive behavior outcomes used teacher or self-report data, while only 2% used parent-reported data. To get an update on the situation, we searched for home-based and/or school-based intervention studies published after 2010 targeting children with conduct problems in which both parents and teachers were used as informants in the outcome analyses.
School-Based Interventions
The Families And School Together (FAST) is a multifamily, after-school program, mainly implemented in the school context for families having children with multiple risk factors (i.e., high-risk samples). According to a Cochrane systematic review, no generalizing effects from school to home were tested or found (Valentine et al., 2019). The Positive Alternative THinking Strategies (PATHS) program is a universal social competence classroom-based intervention that aims to reduce teacher-and parent-rated externalizing behavior. In addition to student activities in and outside the classroom context, materials for use with parents are included. The program has demonstrated cross-domain effects with significant reductions in teacher- and parent-rated aggressive behavior among preK and Grades 1-3 students (e.g., Malti et al., 2011). The Conjoint Behavioral Consultation (CBC) program is a family–school partnership model aiming at the promotion of teacher-rated behavioral competence and decreasing problem behavior in disruptive children (i.e., high-risk samples). In a randomized controlled trial (RCT) with 267 children in rural elementary schools, effects on parent competence in problem-solving were demonstrated for participants in the CBC group relative to the control group. However, different from program effects for children in urban elementary schools (e.g., Sheridan et al., 2013) nonsignificant effects were found for parent-rated child externalizing and internalizing behaviors (Sheridan & Wheeler, 2017). The school-based Anger Coping Program (ACP) is a cognitive-behavioral intervention relevant for children (from 7 years of age) and adolescents with clinical levels of conduct problems. It targets both children in the school context and their parents (Lochman et al., 2021). A comprehensive social-cognitive component aims to teach parents how to interact with their children. Included are also family communication and problem-solving to maintain positive relationships between parents and children. Impacts both on child aggression (rated by independent observers and parents) and on maternal depression, marital/partner conflict, and parent stress management have been examined. Outcome analyses have demonstrated generalization effects to the home environment for high-risk boys and their parents (e.g., Lochman & Lenhart, 1993). The Coping Power Universal program is an adaptation of the APC. It is a universal classroom-based program with no parenting components rather than a targeted program like the ACP (Muratori et al., 2019). The intervention was tested on 1,030 Italian fourth and fifth graders in 70 elementary classrooms. The focus on problem-solving and emotional regulation produced changes in the student’s behavior both in the classroom and at home. The effect sizes of parent ratings were small, however, compared to the moderate effect sizes of the teacher ratings. The Family–School Partnership (FSP) program was evaluated in a meta-analysis of 77 intervention studies (Smith et al., 2019). All studies examined outcome effects on child problem behavior both at home and at school. Although the meta-analysis concluded that the FSP program often resulted in improved student outcomes, none of them were observed in the home environment.
The review of research on school-based interventions targeting both home and school demonstrated mixed results. Some of the programs targeting high-risk children were effective, while others were not. Most effective among the targeted programs were school-based programs containing components that directly targeted the parents, particularly problem-solving skills, but also components that are often included in parenting programs like social skills, stress management, and emotion regulation. Moreover, two universal school programs which included parenting intervention components demonstrated crossover effects from school to home.
Home-Based Interventions
In the search for opposite generalization effects from home to school, we examined a selection of RCTs conducted on two parent training programs, Parent Management Training, the Oregon model (PMTO; Askeland et al., 2014) and Early Interventions for Children at Risk (EICR; Solholm et al., 2013). In an RCT on PMTO, teachers reported a higher level of social competence in the intervention group at postassessment compared to the comparison group (Ogden & Hagen, 2008) and in the 1-year follow-up study (Hagen et al., 2011). RCTs conducted on the EICR program showed no home-to-school generalization effects (Kjøbli et al., 2013; Kjøbli & Ogden, 2012). In conclusion, except for the crossover effect of social skills, there were no generalization effects from home to school when parent training programs were examined.
Research Questions
In the current study, the transfer of child behavioral changes from school to home was examined, as were benefits for parents after the implementation of the school-wide prevention model SWPBIS. The following research questions were formulated: (a) Are there significant differences in problem behavior and social skills at home among students respectively at low, moderate, or high risk of conduct problems when parent ratings from schools implementing the SWPBIS model are compared with parent ratings from control schools over 4 years and when demographic variables (i.e., student sex, parent education, family finances) are controlled for? (b) Following 4 years of implementation of the SWPBIS model and controlling for demographic variables, are there significant group differences in the parents’ perceived mental health, monitoring, school support of the child, and school–home collaboration?
Method
Participants
The current study is based on repeated parental questionnaire data derived from a longitudinal multicohort effectiveness study of the SWPBIS model in Norway. A stratified, matched, and randomly invited sample of 65 ordinary primary schools participated in the study among which 28 schools implemented the full SWPBIS model while 18 schools implemented an abbreviated version (Preventing Problem Behavior in School), and 20 schools maintained “Practices as Usual” (PAU; for details of design and recruitment procedure, see Sørlie and Ogden [2014]). The first assessment (T1, baseline) was conducted at the beginning of a new school year and close to the initiation of the SWPBIS model. The remaining assessments were carried out at the end of the following school years (T2-T5). Due to a lack of resources, only parent ratings from a part of the sample were possible to collect. Accordingly, based on the students’ T1 mean scores on the Teacher Report Form (TRF, Achenbach, 1991) externalization scale and Norwegian TRF norms (Larsson & Drugli, 2011; Lurie, 2006), we first divided all students into three risk groups (high, moderate, low). Next, a subgroup of 30% was randomly drawn, and their parents were asked to complete a questionnaire annually. The “select cases by random sample of cases” method in SPSS was used to randomly select students. The subgroup included 10% of all students considered at low risk of severe conduct problems (i.e., TRF Ext <4.99), 10% considered at moderate risk (TRF Ext between 5.0 and 10.99), and 10% considered at high risk (TRF Ext >11.0). The selection procedure implied an oversampling of the number of students in the high-risk group compared to the number of students in the moderate- and low-risk groups. The oversampling was done to gain statistical power to detect significant cross-contextual outcome differences. To enable tracking of a stable group of students, the current analyses were limited to the fourth graders (age 9 years) of the 30% subsample (n = 594 of total n = 2,138). These students were followed through seventh grade (age 12 years).
At T1, the analytical sample consisted of 219 low-risk students (36.8%), 178 moderate-risk students (30%), and 196 high-risk students (33%). They received either PAU (n = 160, 26.9%), the full (n = 252, 42.4%), or the abbreviated SWPBIS model (n = 182, 30.6%). Out of these, 345 were boys (58.1%) and most (n = 545, 91.7%) had Norwegian as their first language. Moreover, 25% (n = 149) received ongoing special education, 17.5% had been referred to the school educational services, and 10.6% had been referred to the child welfare or mental health services.
Most parents were between 31 and 40 years of age (60.5%) or between 41 and 50 years (35.1%), while only 2.8% and 1.2% were either younger than 30 or older than 50 years. Most had completed at least 3 years (41.9%) or 1 or 2 years (10.7%) at university or college. Only 6% reported primary school as their highest education, while 19.5% and 21.9% respectively stated that 1–2 and 3 years at high school were their highest educational level. As concerns the family economy, 1% reported that they often or every month could not afford food, medicines (1%), insurance (2.5%), furniture or household articles (6.3%), or paying for recreational activities or pleasures (5.9%).
There were mostly small (1-1.7%) differences between the subsample and the total sample, except that there were 3.8% more boys and 4.1% more students referred to child welfare or mental health services in the total sample. In addition, the main part of parents in the subsample were somewhat younger than in the total sample (7.9% more parents were 31–40 years old, and 6.4% fever were 41–50 years old).
Procedures
The parents were informed about the study and received a letter of consent written in Norwegian or in one of the four most frequently spoken foreign languages, English, Urdu, Somali, and Bosnian. The consent was signed and returned via the school. The parents who consented to participate in the study then completed a questionnaire which was returned at each assessment point via the Internet or the schools. To standardize the assessment procedure, written instructions were given. Every year, the contributing parents participated in a raffle for five gift cards worth 2,000 Norwegian Krone.
Measures
Problem Behavior
The primary outcome variable in the current study was parent ratings of the children’s behavior at home, which was assessed with a Norwegian translation of the 17-item Problem Behavior scale (Cronbach’s ɑ = .88, max–min score = 68–17) of the Social Skills Rating System (SSRS, Gresham & Elliott, 1990). The parents rated how often the child showed problem behaviors on a four-point scale (1 = Seldom/never, 4 = Very often). SSRS measures three subdimensions of problem behavior with six items each: externalizing (Cronbach’s ɑ = .80), internalizing (ɑ = .73), and hyperactivity (ɑ = .83). Only the total scores were used in the analyses. Item examples: “Acts sad or depressed,” “Argues/quarrels with others,” and “Doesn’t follow rules or instructions.”
Social Skills
The children’s social skills were measured with a Norwegian translation of the 38-item parent version (ɑ = .94, max–min score = 152–38) of SSRS (Gresham & Elliott, 1990; Ogden, 2003). The parents rated how often the children engaged in positive social behaviors (1 = Seldom/never, 4 = Very often). The SSRS parent version taps four social skills dimensions (10 items each): cooperation, assertion, self-control, and responsibility. The sum scores only were used in the analyses. Item examples: “Volunteers to help family members with household tasks” and “Speaks in an appropriate tone of voice at home.”
Mental Health
Parent’s self-ratings of symptoms of depression and anxiety were assessed by an 11-item scale (ɑ = .90) derived from the Hopkins Symptom Check List (HSLC-25; Derogatis et al., 1974; max–min score = 44–11). Item examples: “Constantly afraid or anxious” and “Easily angry/furious (temper outbursts).” Rating scale: 1 = Not bothered, 4 = Very bothered.
Monitoring
The parents’ knowledge of the child’s whereabouts, who they were with, and what they were doing during their spare time was assessed with an eight-item scale (α =. 82, max–min score = 32–8) from the Oregon Healthy Teen Survey (Oregon Health Authority, 2020). Item examples: “The child tells me openly and voluntarily about everything he/she is doing during leisure time” and “I almost always know where my child is when not at home.” Rating scale: 1 = Fits very well, 4 = Does not fit.
School Support
The parents’ support for their child’s school efforts was assessed with an eight-item parental assessment scale (α =. 85, max–min score = 32–8) from the Oregon Healthy Teen Survey (Oregon Health Authority, 2020). Item examples: “I have daily conversations with the child about what is going on at school” and “I often encourage the child to do well in school, but without demands.” Rating scale: 1 = Fits very poorly, 4= Fits very well.
School–Home Cooperation
The parents’ views on and experiences with the school–home collaborations were measured with 17 items using a 4-point rating scale (1 = Fits very poorly, 4= Fits very well). The scale was developed for this study (ɑ = .91, max–min score = 68–17). Item examples: “I have good contact with the child’s main teacher,” “I am frequently informed of the child’s educational plan (curriculum),” and “I feel that the teachers are interested in my suggestions and take my suggestions into account.”
Covariates
Covariates included in the analyses were student sex (girl, boy), parent self-reports on the family economic status, and education. Only the baseline scores of the covariates were used in the analyses. The perceived family economy was assessed with six items (ɑ = .85) from the Household Economics scale developed by Pearlin and Schooler (1978). Parent education was measured by the responding parent ticking off her/his highest completed education (1 = No or limited schooling, 6 = Minimum 3 years college or university education).
Analytic Approach
Data were analyzed using linear mixed models as implemented in the SPSS Mixed module. As a default model, a random intercept of students across repeated measures was specified. As T1 was used for the classification of risk groups, only T2–T5 measurements for the dependent variables were included in the outcome analyses. To isolate main and interactive effects, independent fixed variables were entered block-wise. Intervention effects would be demonstrated if two-way intervention group by time interaction terms were statistically significant. Moderation of intervention effects by risk group would be indicated by significant three-way interactions, controlling for main effects and relevant two-way interactions. Effects were adjusted for the T1 covariates parent education, family economy, and student sex and tested using Satterthwaite F-tests, with corrected degrees of freedom. Bonferonni correction was used to control for family-wise error rates across outcomes. As there were six outcomes, the nominal p-value was set to p < .00833. The categorical independent variables risk group and intervention group and their interactions were tested through simple contrasts against a reference category. For the risk group variable, low and medium risk was compared to the high-risk category. For the intervention group variable, the PAU and abbreviated condition were used as references. Two- and three-way interaction terms were specified through product terms of included main variables. Time was treated as a continuous variable and tested for linear effects. Differential effects of time were tested through the product term of simple contrasts and time, centered on T1.
As students came from different schools, potential random school-level effects (RSE) were assessed. In line with numerous other studies, we used the intraclass correlation (ICC) to guide modeling decisions about random effects. As a simple rule of thumb, a strong ICC of the school would support the inclusion of an RSE, at least to avoid biased standard errors. In contrast, an ICC close to zero would be an argument for excluding RSE from the random part of the analysis. Although the ICC provides a useful heuristic for making decisions about the inclusion of random effects, some note the need to also consider other sources of information. The impact of any given ICC varies as a function of cluster size (Huang, 2018; Peugh, 2010) and type of research question (Nezlek, 2008). It follows from the design effect (DEFF) formula (e.g., Peugh, 2010): DEFF = 1 + (nc − 1) × ICC, that the impact of sample clustering (schools) on sampling variance (DEFF) is a function of ICC and cluster size. A small ICC could give rise to a strong DEFF if the average cluster size is big (Huang, 2018).
All models were tested with RSE (three-level model: school–student–time) and without RSE (two-level model: student–time). The ICC of schools ranged between 0% for the school support and social skills variables and 6.6% for the home-school cooperation variable. Under the current average cluster size, the school-level ICC represented a DEFF ranging between 1.00 and 1.53 across outcomes. The ICC and DEFF indicated that the two-level model without RSE was an acceptable model specification in the present study.
Results
The presentation of results follows a logical order. Initially, means and standard deviations (raw scores) for each outcome variable across time points are shown in Table 1. We then present the main effects of time, risk group, and sex. Next, we present the interactive effects with an emphasis on intervention effects, particularly for groups considered at low, moderate, and high risk of conduct problems.
Means and Standard Deviations for the Parent-Rated Outcome Variables Across Assessments (T1 n = 594).
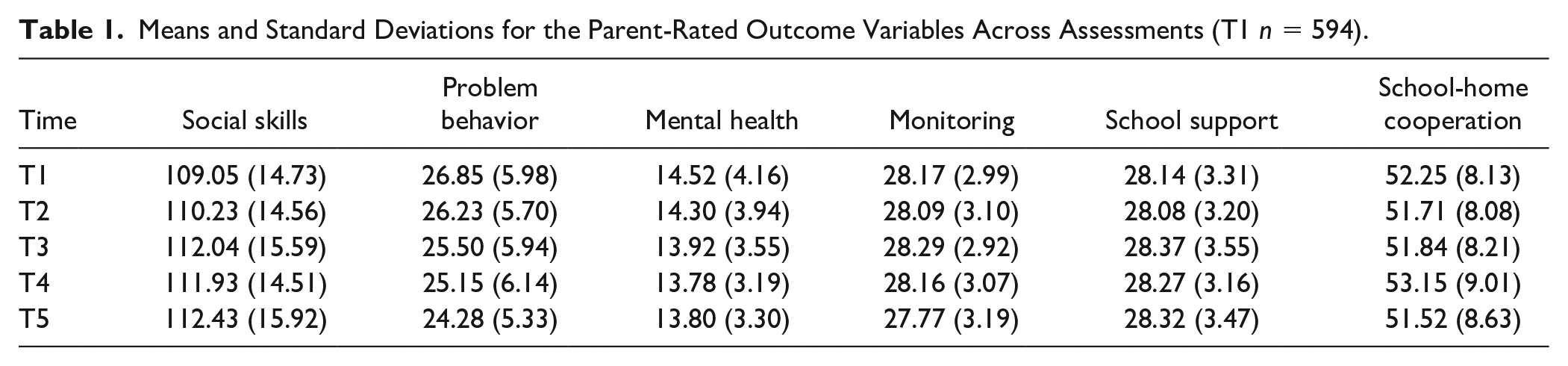
According to Table 1, the mean values and dispersion of the parent-rated variables were either stable or showed a marginal positive change across the school years. From fourth through seventh grade, the social skills scores slightly increased while the ratings of problem behavior in the home setting decreased. Despite the oversampling of students frequently showing problem behaviors in the school setting, the parents generally seemed to rate the children’s problem behavior in the home settings as relatively low (M = 24–26 of max-min = 68–17). Across studies and measures, Norwegian children are rated as having fewer problems than in other societies both by teachers and by parents (Jozefiak et al., 2012; Larsson & Drugli, 2011). The parents’ ratings of their mental health (anxiety and depression) were also in the lower range, while the self-ratings of their monitoring, support for their child’s school efforts, and collaboration with the school were in the higher range. In other words, the parents seemed to have a rather positive and stable perception of their children’s functioning as well as of their parental role.
Analysis of main and interactive longitudinal effects was conducted for each dependent variable (for details, see Online Supplemental Material Tables 2–7). The key findings are summarized in the following text. Information on the omnibus F-test for each independent variable is given. For further details about the specific contrasts, see the Online Supplemental Material tables.
Main Effects of Time
Statistically significant main effects of linear time were observed for problem behavior at home only, F(1, 636.60) = 1.36, p = .0000000032. The findings indicate that independent of being in the intervention groups or the control group, the children’s problem behavior in the home setting decreased over time. For social skills, mental health, parental monitoring, school-home cooperation, and parental school support, there were no significant main effects of linear time across the four school years. A test of deviation from linearity at two degrees of freedom was statistically significant for school-home collaboration but not for the other five outcomes.
Main Effects of Risk Group
Higher risk was associated with more problem behaviors, lower social skills, and less positive school-home cooperation. Statistically significant main effects of risk group were observed for problem behavior at home, F(2, 404.34) = 22.48, p = .000000000055, social skills, F(2, 401.31) = 13.96, p = .00000014, and school–home cooperation, F(2, 409.96) = 7.25, p = .000803881. For parental mental health, monitoring, and school support, there were no main effects of risk group.
Main Effects of Sex
According to the parents, there were no statistically significant main effects of sex, which indicate that boys and girls did not differ in their social and behavioral development over time. Likewise, being a parent to a boy or a girl did not seem to affect the parent ratings of their monitoring skills, ability to support the child’s schooling, or their evaluation of the school-home cooperation.
Intervention Group by Time Interaction
Group-by-time interaction effects were statistically nonsignificant for all outcomes, suggesting no evidence for intervention effects in the home setting across the period (i.e., neither for parental mental health, problem behavior, social skills, school support, and school collaboration nor for monitoring).
Moderation of Intervention Effects by Risk Group
Likewise, we found no statistically significant three-way intervention-by-time-by-risk group interaction effects, suggesting that there were no clear differences in the three risk groups’ (low, moderate, high) benefits of the SWPBIS model in the home context.
Other Interactions
For risk group-by-time, significant interactions were observed for problem behavior at home, F(2, 627.74) = 4.92, p = .007557297, but not for the other outcomes. This implies that the low-risk group showed a steady decline in problem behaviors over the school years, whereas the moderate- and high-risk groups changed less. To assess subgroup consistency, a saturated interaction including sex-by-time and sex-by-risk group was estimated. Risk group-by-sex interactions were observed for parent-rated social skills, F(2, 394.06) = 5 .41, p = .0048, indicating that the impact of risk group on social skills was stronger for boys than for girls. For the other outcomes, there was no significant interaction effects of sex.
To visualize differential development across risk groups, scores for each dependent variable were centered on the T1 grand mean score and standardized to the T1 standard deviation as shown in Figure 1. It was evident that the risk groups had similar trajectories across time, as indicated by the overlapping confidence intervals. The most striking aspect of Figure 1 is that the risk groups differed in their general outcome levels. Over time, the low-risk group maintained a lower level of problem behaviors and a higher level of social skills. The medium- and high-risk groups did not differ much. Except for problem behaviors at home, the differences between the groups over time were rather stable. The trajectories were in general linear, but with a few random deviations from linearity on single time points.
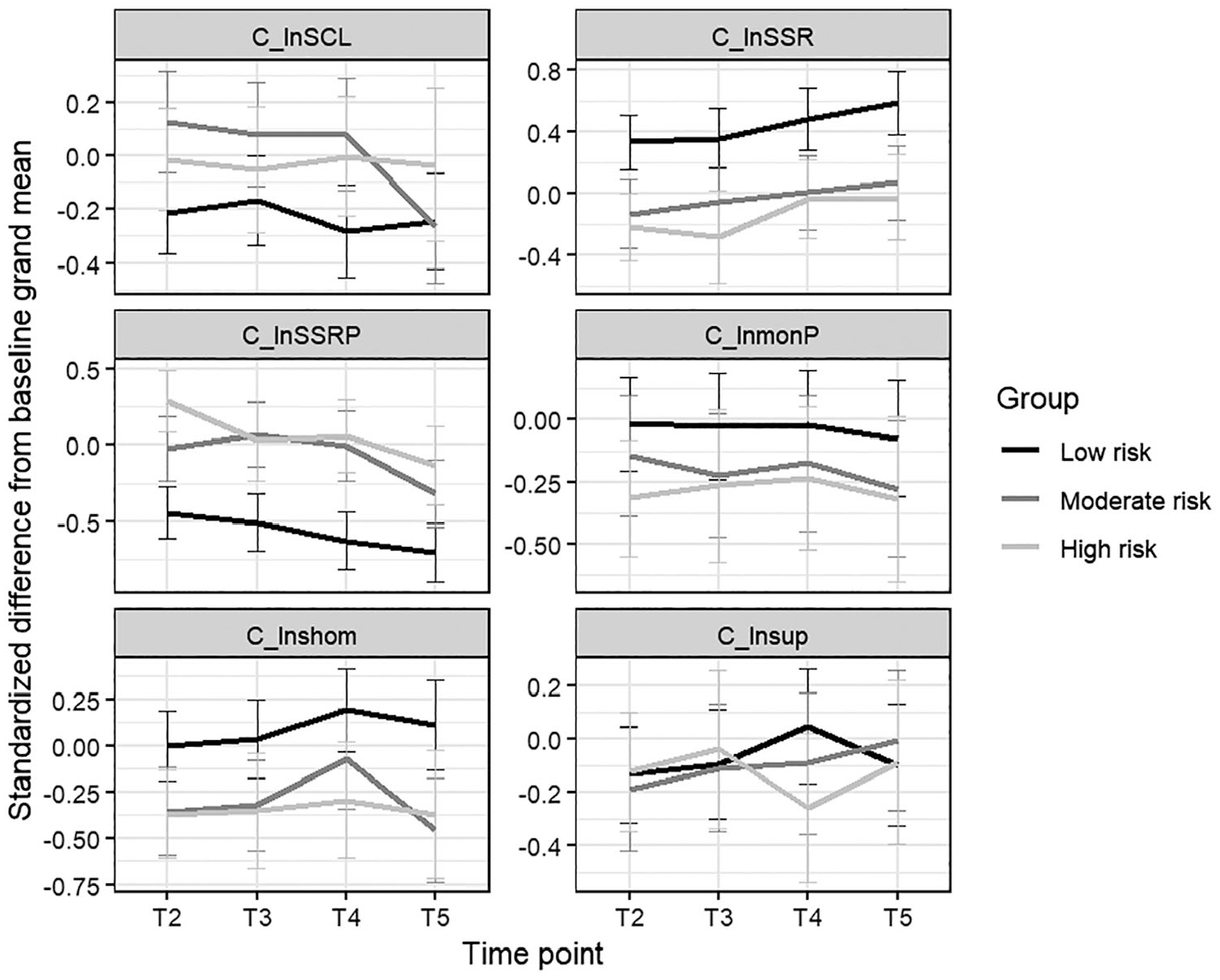
Differential Development Over Time Across Risk Groups and Outcome Variables.
Discussion
The present study examined whether the previously documented positive behavioral changes among students in schools implementing the SWPBIS model (Chitiyo et al., 2012; Lee & Gage, 2020; Noltemeyer et al., 2018; Sørlie et al., 2016; Sørlie & Ogden, 2015) may generalize to the home setting. We also examined whether parents may benefit from SWPBIS. Potential intervention effects in the home setting were investigated over a 4-year period in a randomly selected sample (n = 594) of students (fourth through seventh grade) considered at various levels of risk. No significant differences were detected between students in the intervention group attending SWPBIS schools and students in the control schools maintaining PAU. This should come as no surprise as the raw scores on both the primary and the secondary outcome variables were quite stable over time and leaning to the positive side rather than to the negative side. Evidently, there was little room for improvement in any of the groups. Parent ratings of social skills, monitoring, school support, and school-home collaboration remained in the high positive range, while conduct and mental health problems, despite low scores at baseline, were further reduced. These results generally suggest that the SWPBIS model had no significant impacts in the home setting, neither for students nor for parents. Likewise, we found no indications of differential intervention effects in the home setting for students considered at respectively low, moderate, or high risk of conduct problems. Accordingly, the previously documented positive effects of SWPBIS on high-risk students’ behavior in the school context (e.g., Borgen et al., 2021; Sørlie et al., 2018) did not seem to generalize to the home context.
The high-risk group was, however, rated by their parents as being less socially skilled, and the parents experienced the cooperation with the school as more conflictual and less satisfactory than other parents. The high-risk group was also rated across research conditions and time as showing more problem behavior in the home setting than students in the moderate- and low-risk groups. Accordingly, the parent ratings point in roughly the same direction as previous teacher ratings; students frequently showing problem behavior in school are rated as less socially and academically skilled (e.g., Hukkelberg et al., 2019; Kremer et al., 2016). Since the risk groups were selected based on teacher ratings, the parent ratings suggest that the high-risk group differs from other students in that they strive with multiple problems that are observable both at school and at home. The results also reflect this finding as parents of children frequently report that externalizing problems are often stressful and concerning. The correlations between teacher and parent ratings are usually moderate, in the region of 0.30 (Piquero et al., 2012). The parents’ assessments of the risk groups’ functioning may thus give rise to discrepancies among teachers and parents.
Independent of which research condition and risk group the students belonged to, the occurrence of problem behaviors in the home setting significantly decreased over the 4-year study period. Moreover, the study results revealed no significant sex differences in how boys and girls developed over time on any of the parent-rated outcome variables. The impact of risk group on social skills was, however, stronger for boys than for girls. The low-risk group’s problem behavior decreased more over the school years, compared to the moderate- and high-risk groups which changed less. Several studies, including twin studies, have found that externalizing problem behavior in typically developing children and youths shows strong stability over time, from childhood to early adulthood—for boys as well as for girls (e.g., Flouri et al., 2019; Hatoum et al., 2018). The decrease demonstrated in this study may be due to the increased social pressure children are exposed to when they misbehave, for instance from parents, relatives, and friends. According to social control theory, children who bond to family, friends, or school are more susceptible to the environment’s expectations and norm pressure, regardless of being exposed to any formal interventions (Schreck & Hirschi, 2009). Children who frequently demonstrate disruptive behavior may experience pressure proportional to the increase in such behavior. They are expected to comply with norms and values in their family and social network and are usually rewarded for doing so.
The findings from the current study join findings from other effectiveness studies that have failed to demonstrate cross-domain effects of school-based or home-based interventions such as the FAST program, the FSP program, and the PMTO program. The lack of indicative generalization effects for the SWPBIS model is perhaps disappointing but not surprising, in that most interventions that have documented effects both in the school and home setting are, unlike the SWPBIS model in Norway, characterized by an incorporation of specific components, strategies, and materials directly aimed at the parents such as the PATHS program, CBS program, and ACP. In this context, it should be noted that the SWPBIS model has a school-wide approach and does not have a stated goal of influencing the students’ behavior outside the school context or entail gains for parents. In most cases, preventing and reducing problem behavior in the school setting are perhaps sufficient. However, for those students showing externalizing behavior across contexts, it may seem that SWPBIS is insufficiently rigged, at least in Norway. In line with recent recommendations from researchers including Weist et al. (2017) and Garbacz et al. (2018), our findings indicate that the acceptance and effectiveness of the intervention model could benefit from a more clear and more specified approach to involve and support parents.
To our knowledge, this is the first study examining the potential effects of the SWPBIS model in the home context. Other strengths of the study include (a) the use of a randomly selected subsample from a large-scale effectiveness study with a sound design, (b) longitudinal data, and (c) the use of reliable and widely used instruments. However, the study may also have been hampered by some weaknesses. Although parents were seen as the most reliable informants of possible changes in the home setting, the validity of the study findings could have benefited from the inclusion of additional student ratings. A second limitation is that the sample may have been too small to detect minor changes in the home setting. Third, other factors than those we have accounted for in the analyses may have influenced the results (e.g., fidelity). Fourth, the children’s and parents’ problems as measured in the home setting may initially have been limited thus leaving little room for change. On this basis, the study results should be interpreted with caution.
Conclusions and Practical Implications
The results from this study indicate that there are few generalization effects from the SWPBIS model to the home context. It seems that parents rarely perceive or register any significant changes in their children’s behavior and social skills following the SWPBIS model. Likewise, they did not register any significant changes in their mental health, in the school–home collaboration, or in their monitoring and support of the children’s schooling. Neither were we able to detect any differential effects of SWPBIS in the home setting for students with varying risk status. However, before firm conclusions of the model’s generalizing effects to the home setting are drawn, the study results should be replicated in future studies.
Outcomes from the current as well as several previous evaluation studies indicate that children with conduct problems could benefit from a combination and integration of parenting and school-based intervention components. At the universal level, the results suggest a need for increased information and involvement of parents in general preventive work. At the selected level, there may be a need for extended contact and cooperation between school and home. More frequent contacts and increased communication could be integrated in the model like home visits, report cards, and phone calls. A short-term parenting program (three to five sessions) could also be delivered by the school health services or the municipal child and family services (Kjøbli & Ogden, 2012). Finally, at the indicated level, a full-scale parenting program could be recommended (Askeland et al., 2014). Parenting programs (e.g., PMTO) contain several of the components shown to be effective in previous school–home projects, including relationship building, problem-solving, good directions, skills encouragement, monitoring, and self-regulation. This intervention could be integrated with relational activities between parents and teachers, in which home and school coordinate their efforts, rather than working in isolation (Smith et al., 2019).
Supplemental Material
sj-docx-1-pbi-10.1177_10983007241312421 – Supplemental material for Are There Generalization Effects to the Home Context From the School-Wide Positive Behavioral Interventions and Supports (SWPBIS) Model?
Supplemental material, sj-docx-1-pbi-10.1177_10983007241312421 for Are There Generalization Effects to the Home Context From the School-Wide Positive Behavioral Interventions and Supports (SWPBIS) Model? by Mari-Anne Sørlie, Terje Ogden and Torbjørn Torsheim in Journal of Positive Behavior Interventions
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by the Norwegian Center for Child Behavioral Development and in part by a grant from the Norwegian Directorate for Education and Training. The standards of the regional Committee for Medical and Health Research Ethics (REK South-East) and of the Norwegian Social Science Data Services were followed throughout the conduct of the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.