
Abstract

“Even before the pandemic, children were missing recommended screenings, which hampered the early detection of delays/disabilities.”
Maria was 10 months old when her parents first noticed her development was different from her siblings. Maria was not yet starting to sit on the floor unsupported (i.e., without use of hands for support) like her brothers were by this same age. Maria attended a family in-home group setting 2 days a week, went to her Spanish-speaking grandmother’s house 2 days a week, and in her own home with a babysitter 1 day a week while both of her immigrant parents worked lower-paying jobs. Her parents shared their concerns about her development with Maria’s pediatrician and early childhood educator. Both professionals advised her family to “wait and see.” Maria did not get a screening. Her development in motor areas continued to follow an atypical pattern. Her gross and fine motor skills were slow to develop during toddlerhood and preschool years. Maria and her family were not connected with child development services. When Maria was at the end of her kindergarten year, she was referred for an evaluation because her kindergarten teacher had developmental concerns that were corroborated by Maria’s parents. Maria became eligible for special education services after an in-depth and comprehensive evaluation. By the time she got an individualized education program to meet her needs, Maria was in first grade.
Early detection is recommended so that early intervention can begin as soon as possible in the hope of improving developmental and behavioral outcomes for young children. American Academy of Pediatrics (AAP, 2020) recommends routine and periodic screenings. Routine screenings are also recommended by Division for Early Childhood of the Council for Exceptional Children (DEC Recommended Practices), across education, health, and social sectors. Developmental-behavioral screening is a quick look at what the child can do now. The girl in the vignette, Maria, did not receive regular screenings.
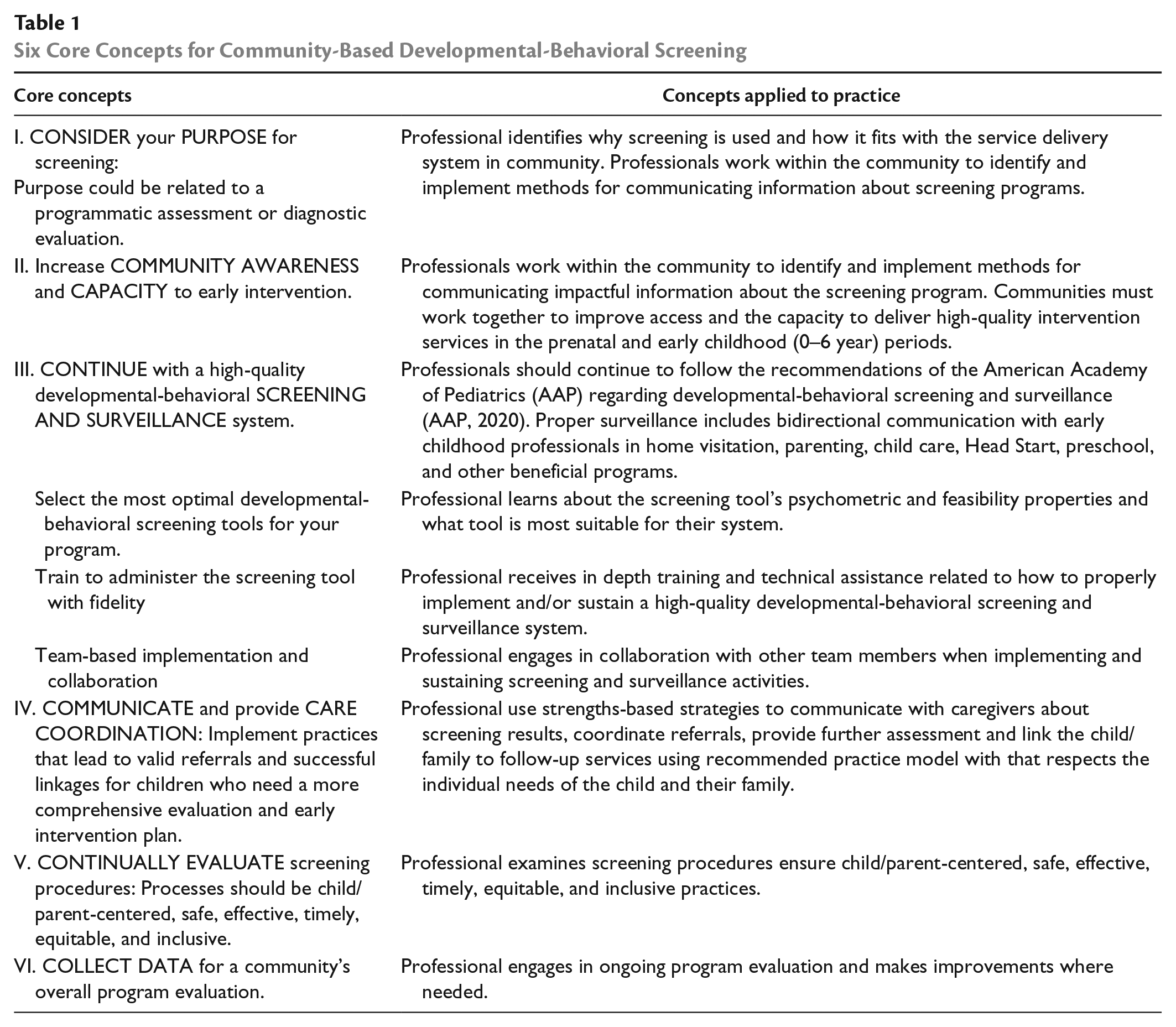
Maria showed early signs of developmental variation, but her special needs were not formally identified and addressed until many years later. Even before the pandemic, children were missing recommended screenings, which hampered the early detection of delays/disabilities (Bricker et al., 2013; Macy et al., 2014; Marks et al., 2015). States that receive Individuals with Disabilities and Education Act (IDEA) Part C funding for early intervention (EI) or early childhood special education (ECSE) services are required to provide free, universal screenings for young children (Macy, 2022). However, this will not be enough without emphasis on six core concepts or six “C”s (Table 1) surrounding inclusive and equitable screening: (a)
Six Core Concepts for Community-Based Developmental-Behavioral Screening
When there is a failure to swiftly detect an at-risk condition, developmental delay, other atypical milestone pattern, or disability, the benefits of connecting to community-based services may be compromised from the tyranny of time while brain plasticity diminishes. A child’s genes, neuroendocrine signals, and environment (e.g., parent–child interactions) are most interactive during early childhood period, when neural circuits display a heightened sensitivity in acquiring instructive and adaptive signals (Inguaggiato et al., 2017). A “wait and see” approach is incongruous with everything that we have learned about brain plasticity.
“When there is a failure to swiftly detect an at-risk condition, developmental delay, other atypical milestone pattern, or disability, the benefits of connecting to community-based services may be compromised from the tyranny of time while brain plasticity diminishes.” “When familiar caregivers have a concern about their child’s development, they need timely access to community-based services that are easy to navigate for a diverse group of families.”
In the vignette, barriers existed for Maria and her family. Families need reliable, accessible, and equitable developmental-behavioral screening in their community (Bricker et al., 2013). When familiar caregivers have a concern about their child’s development, they need timely access to community-based services that are easy to navigate for a diverse group of families. Solutions are needed to reach all children with developmental screening, and especially when cultural, language, parental trauma-related, and SES barriers exist. Children experiencing homelessness, a family with an income below poverty guidelines, and persons of color may experience barriers in accessing resources in their community. (Bricker et al., 2013; Iruka et al., 2022; Meurer et al., 2022).
Early identification and intervention programs may offer services with limited coverage, accessibility, scope, frequency, or intensity (Bricker et al., 2013). Identifying and connecting children at risk for developmental-behavioral problems to EI/ECSE services became even more challenging with the COVID-19 health crisis, which is related to worsening racial, gender, and income inequalities (Brodie et al., 2021). A new generation of young children born shortly before, during, or after global pandemic may be disadvantaged by a lack of developmental-behavioral screening early in life. States made many COVID-related changes to child assessments, such as no required assessments, fewer assessments over time, or replacing face-to-face with virtual assessments (Macy, 2022). In the State of Babies report, researchers described the following trends during the pandemic: (a) only one in three U.S. young children (33.8%) received a developmental screening and reported racial disparities, (b) children who are White (36.4%) were screened at higher rates compared with children of other races (Hispanic 31.1%, Black 27.5%, and Asian 26.2%), and (c) lower rates of screening in children with low-income families (29.0%) than higher / above low-income families (36.9%; Keating & Heinemeier, 2022). Just like Maria’s case, there are often multiple barriers to overcome in the early identification process for young children in the United States and many other countries. Six core concepts are reviewed to connect everyone who screens children across settings into a single unified system and ensuring that all parts of the system align and work seamlessly together (Bricker et al., 2013).
Core Concepts for Equitable and Inclusive Screening in Your Community
Consider Your Purpose with Screening
Maria and her parents would have benefited from professionals who had gained an understanding of early childhood screening and its impact on children and families (DEC RP—Assessment A1 and A7). The purpose of screening is to get a snapshot of the child’s developmental-behavioral performance in 10 to 20 min, not to make a diagnosis (Marks & LaRosa, 2012). Screening tools are primarily meant for children perceived to be asymptomatic but, they are also meant for those children deemed by developmental surveillance/monitoring to be “at-risk” (Marks & LaRosa, 2012). Under IDEA Part C, screening is at the state’s discretion and great variability exists in execution of screening between states. Therefore, underlying objective(s) for screening and service delivery should be understood by professionals in early child care, medical, social, and EI/ECSE settings.
“Six core concepts are reviewed to connect everyone who screens children across settings into a single unified system and ensuring that all parts of the system align and work seamlessly together.”

Community Awareness and Capacity for Early Intervention
Maria’s parents were unaware of the free developmental screening offered in their community. Increasing public awareness and accessibility to screenings and IDEA activities (DEC RP—Assessment A1 and A7) are critical for communities. Various forms of media can be used to inform the public about early identification and development-behavioral screening. U.S. public awareness campaign “Learn the Signs. Act Early” increased parent’s awareness and discussion about developmental milestones. While increasing awareness is a laudable goal, communities must also increase and improve access to EI/ECSE programs and other beneficial community services that are tailored to child and family needs (Marks et al., 2015). For example, Help Me Grow (https://helpmegrownational.org/) program can improve a community’s awareness level and capacity to link at-risk children/families with community services not covered by IDEA; however, this program is not yet available in all U.S. states.
Continue With Developmental-Behavioral Screening and Surveillance
Maria missed an opportunity for evidence-based screening in her early childhood years. Developmental screening may measure a single domain or multiple developmental domains, which could include socio-emotional skills and behaviors. Questionnaires are standardized and normed so comparisons can be made across a large and representative sample of the population. Screens have cut-off scores so interpretations can be made to determine if child’s development is typical, borderline, or atypical for their age when compared with normative data. Screens are brief as the objective is to get a snapshot of the child’s development and behavior.
“While increasing awareness is a laudable goal, communities must also increase and improve access to EI/ECSE programs and other beneficial services that are tailored to the child and family needs.”

A group screening strategy may include asking parents to complete a screening tool at home and return it later, having a professional assessor do group activities and screening for each child, or organizing a community screening fair. Another option is to use an individual-based tracking system as concerns arise. Program providers and/or family members can periodically measure an individual child in the developmental area(s) of concern. A monitoring system is an effective strategy when concerns arise, but the child’s results should ideally be conclusive enough to determine if a more comprehensive evaluation is needed.
“Screening and surveillance includes bidirectional communication.”
Selecting the Most Optimal Developmental-Behavioral Screening Tools
Maria’s educator and pediatrician could have had access to screening tools used for early detection. Professionals could have benefited from following RPs for early childhood screening (DEC RP—Assessment A1 and A7). It is important for professionals to have understanding about various measures and learn what different sources have found regarding a screening tool’s sensitivity (co-positivity) and specificity (co-negativity) (AAP, 2020; Marks & LaRosa, 2012). Carefully review developmental-behavioral screening instruments to critically determine their psychometric and feasibility properties. Certain screens have good psychometric properties, but many are not well supported by existing research. Appendix A and B can help to identify the most psychometrically sound and feasible tools.
“Equity and inclusivity could be embedded into professional development.”
A screen’s accuracy represents the ability to accurately identify children who have a condition (sensitivity) and rule out children who do not have a condition (specificity). Reliability is essentially the ability to reproduce a result consistently. Validity represents the degree to which accumulated evidence and theory supports interpretations of test scores (i.e., the ability of a screening tool to identify a condition is statistically compared with an appropriate and equivalent reference standard instrument[s] while accounting for different sources of bias). Feasibility characteristics are critically important for diverse community members. For example, useful screening tools may contain multiple language translations, accessible reading levels for a wider audience, and tools that come with expert guidance and how to interpret the screening tool’s results, including in families from diverse backgrounds. Screens with better feasible properties are more likely to be reliably administered and interpreted correctly, and link at risk children/families to further assessment or services within the community.
Train to Administer Screening With Fidelity
Equity and inclusivity could be embedded into professional development for pre-service and in-service practitioners. Professionals must be flexible enough to consider diverse needs in the community (e.g., reading the questions directly to parents with low literacy, using a sign language interpreter when the caregiver is deaf). For example, Maria’s providers could have been trained to provide clear communication in Spanish if preferred for Maria’s parents that EI services are free. Maria’s parents also needed reassurance that they did not need to be afraid or anxious about contacting an EI/ECSE agency. Immigrants may perceive an EI /ECSE agency as a government organization who might contact law enforcement authorities, which could result in Maria’s parents being deported back to their home country and possibly even separate Maria (a U.S. born child) from her parents. Empathetic and well-trained professionals are able to serve the families of young children with high-quality services that support and empower families.
“Family capacity-building practices may include strengthening existing parenting knowledge and skills that enhance parenting self-efficacy beliefs and practices.”
Professionals serving Maria could have used DEC RPs for guidance on how to supportively and reliably administer a screening (DEC RP—parent-friendly Assessment A2). Ongoing professional development can be obtained from national technical assistance programs, higher education institutions, expert training seminars, or screening user’s guides to sustain a high-quality system. Plan-Do-Study-Action (PDSA) cycles can improve the manner in which a parent-friendly screen is administrated and sustained.
Team-Based Implementation and Collaboration
An agreed-upon team-based approach (where each team member is assigned specific tasks) is often key to successful implementation (Bricker et al., 2013). At least one team member should be tasked with ensuring that higher risk families with language, cultural, literacy, or disability-related barriers get personalized support during the screening process. Avoid duplication of tasks as this may annoy or frustrate parents. Good communication is needed between caregivers, office or program staff, health care providers, EI/ECSE programs, and other community professionals.
Communication and Care Coordination
Maria’s family did not experience good communication or coordinated efforts when her parents first expressed concerns at 10 months old. Instead, a “wait and see” follow-up plan was recommended. There are many barriers faced by all families and especially diverse community members that may include but are not limited to language, implicit/explicit biases related to delays/disabilities, time, and necessities like transportation. Reducing language barriers increases optimal care coordination. Effective communication can help professionals make valid referrals and successful linkages for at-risk children (Bricker et al., 2013). Results should have been communicated to build Maria’s family’s capacity to successfully navigate referrals, and secure meaningful and culturally relevant services for their child and family (DEC RP—Family: F3). “Family capacity-building practices” could have supported and helped their family overcome referral barriers in locating services for their child during a stressful period (DEC RP—Family: F7). “Family capacity-building practices” may include strengthening existing parenting knowledge and skills that promote development of new parenting abilities that enhance parenting self-efficacy beliefs and practices (DEC RP—Family: F7). When screening, professionals must monitor their explicit and implicit bias by continuously reflecting on their practices (DEC RP—Assessment A2; DEC RP—Family: F7) to promote quality care coordination and communication for diverse members of community.
Decide on processes, strategies, and times that fit each family’s needs as well as team. Explore common goals. Avoid technical jargon. Consider culture and language needs. Recognize that some caregivers prefer a “sugar-coated” (non-alarmist) style of communication while others prefer “straight talk” when a problem is suspected. Establish positive rapport and use a strengths-based approach for verbal and written communication (Marks & Glascoe, 2010). For families with economic needs, communicate that families should not have to pay for a screening, evaluation, or EI/ECSE services as they are components of IDEA and fall under “Free and Appropriate Public Education” or FAPE. Ask parents to repeat the follow-up plan.
“Consider Plan-Study-Do-Action (PDSA) cycles to make the screening process more parent-centered, safe, effective, timely, equitable, and inclusive.”
Developmental-behavioral screening and care coordination through 2-1-1 (i.e., a call-in system where intake directs the participant to locate services) was effective in increasing the numbers of young children referred to and receiving EI/ECSE services for developmental delays or autism-specific concerns. Care coordination enhances communication among early child educators, EI/ECSE professionals, health care providers, and parents. About half of parents with children identified as needing further evaluation do not follow-up with referral. Practices, such as two-way consent forms, can facilitate timely referral and improve communication between professional groups. Care coordination is important because many EI/ECSE-referred children (who were positive/concerning on a developmental-behavioral screening tool) are subsequently deemed ineligible for EI/ECSE services. These “false positive” cases often have multiple psychosocial risk factors (e.g., limited parental education or income, parental adverse childhood experiences) and need other assistance not available through programs funded by IDEA. Effective coordination of community services has potential to improve education, health, and social outcomes (Bricker et al., 2013).
Continually Evaluate Screening and Follow-Up Procedures
Maria’s parents were not given opportunities to provide feedback to professionals regarding the early detection process. Cultural biases toward delays in child development and disability may exist. Barriers must be overcome to optimally serve ALL members of the community. Consider Plan-Study-Do-Action (PDSA) cycles to make the screening process more parent-centered, safe, effective, timely, equitable, and inclusive. Studying benefits, barriers, and harms of the early detection process may inform continuous improvements that can be made with screening practices (Glascoe & Marks, 2011). Consider planning to periodically elicit feedback from families and team members to improve practices (Bricker et al., 2013; Iruka et al., 2022). Ask families for information leading to better understanding that bridges diverse cultures and languages. Quality improvements may benefit the program, children, and families being supported at many steps throughout the screening and follow-up process.
PDSA cycles can ensure more equity and inclusion for all children. Evaluation of assessment and follow-up practices that are equitable for all children is needed and required in IDEA. To ensure inclusive practices, professionals should monitor explicit and implicit bias in screening procedures, tools, and practices (Division for Early Childhood [DEC], 2014; ZERO TO THREE, 2021). A screening referral database can be used to determine who has not followed through with a referral. Follow-up phone calls to parents (or health care providers) can help facilitate timely referrals. Partnering with organizations, such as Help Me Grow, a model that aims to promote collaboration across child-serving groups and collects and analyzes related data to evaluate ongoing efforts and identify gaps, can help evaluate ongoing practice and procedures. Reflective practices have been shown to improve early detection of developmental-behavioral concerns in young children in health care settings, including for minority groups.
“Children are much more likely to reach their full potential when community-based programs enact a system that is more patient/parent-centered, safe, effective, timely, equitable, and inclusive.”
Collect Data for Overall Program Evaluation
A mix of professionals and family cared for Maria in early years, but data were not actively monitored regarding Maria or the efficacy of her community’s early identification system. Professionals serving children and their families are encouraged to collect data on how a child is developing and notice concerns when applicable (DEC RP—Assessment A1 and A7). There is a dire need to shorten the time intervals between the EI/ECSE referral and a comprehensive evaluation as well as the time interval until a child receives a wide assortment of services.
“Data can be gathered on the percentage of children in a population receiving (a) screenings, (b) referrals, (c) evaluations, (d) EI/ECSE or other beneficial community services.”
System-wide engagement is needed to successfully implement equitable screening, evaluation, and inclusive services (Bagnato, 2007; Marks et al., 2015). Data can be gathered on the percentage of children in a population receiving, (a) screenings, (b) referrals, (c) evaluations, and (d) EI/ECSE or other beneficial community services. Tracking data can help evaluate a program, identify ongoing gaps, and identify strategies to improve a community-based program. Model examples that have been tracking data include: Connecticut’s Help Me Grow program, Delaware’s Department of Public Health, Oklahoma’s Reach Out and Read program, Help Me Grow Vermont, 211 LA County, and Oregon’s Coordinated Care Organization (Bricker et al., 2013).
Research generally supports periodically screening for developmental-behavioral problems in early years of a child’s life because there is a rapid progression in receptive language, expressive language, cognitive, fine motor, gross motor, and social-emotional skills. For example, evaluation of a centralized state or community organization (e.g., HMG) that helps at risk families learn about why, where, and when to get screened.
Earlier is better when it comes to detecting and addressing concerning variations in development or concerning medical and/or environmental risk factors. However, there are so many barriers for families of at-risk or delayed children (like Maria) to overcome, and thus, they deserve a community-based early identification delivery system that can meet their needs. Children are much more likely to reach their full potential when community-based programs enact a system that is more patient/parent-centered, safe, effective, timely, equitable, and inclusive. Therefore, we recommend: (1) considering your purpose with screening, (2) increasing awareness and capacity to IDEA EI/ECSE and other beneficial community services, (3) continuing to provide high-quality developmental-behavioral screening and surveillance, (4) communicating well as a team and providing care coordination, (5) continually evaluating screening / early detection procedures, and (6) collecting data for an overall program evaluation.
Footnotes
Appendix
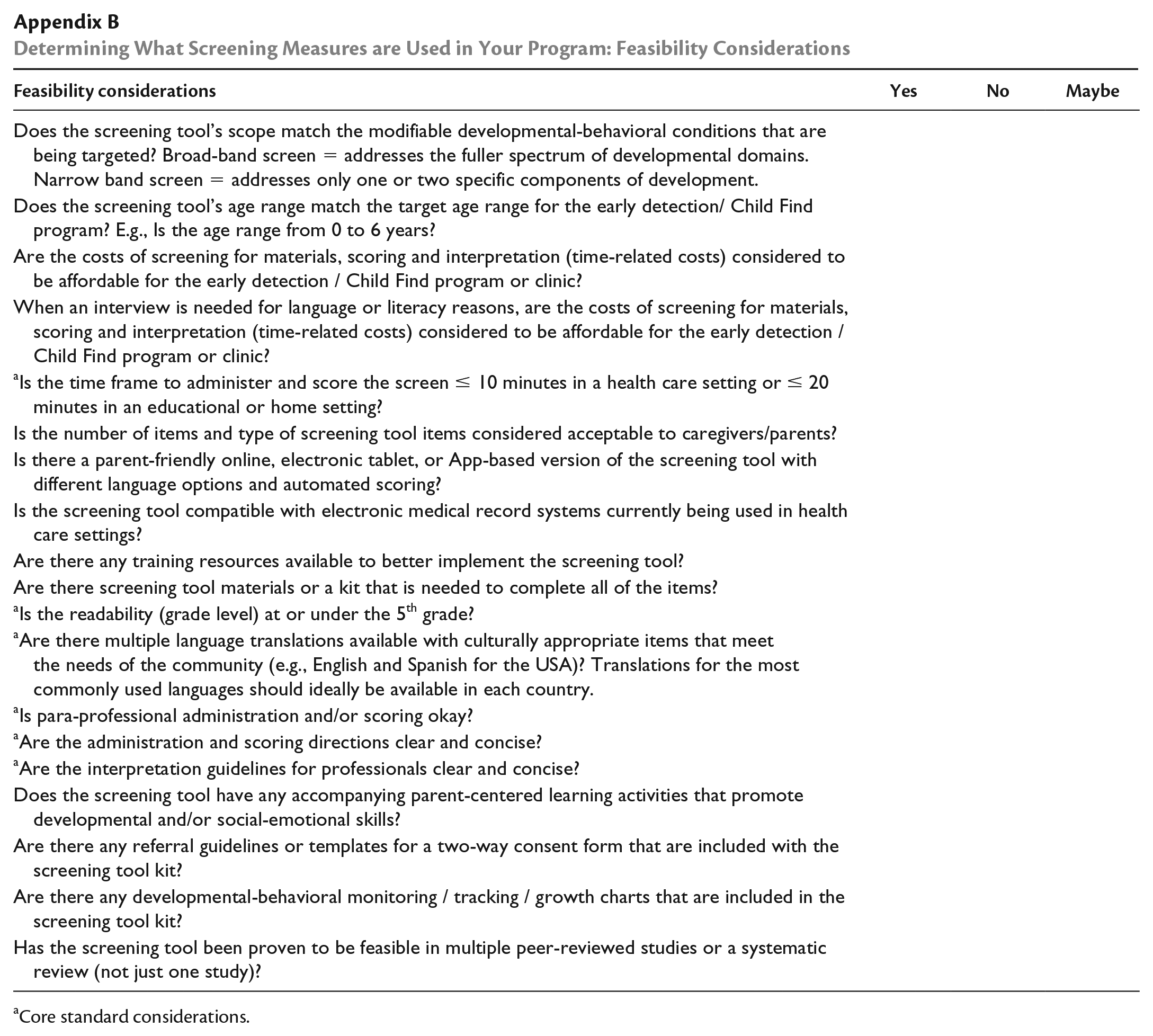
Determining What Screening Measures are Used in Your Program: Feasibility Considerations
| Feasibility considerations | Yes | No | Maybe |
|---|---|---|---|
| Does the screening tool’s scope match the modifiable developmental-behavioral conditions that are being targeted? Broad-band screen = addresses the fuller spectrum of developmental domains. Narrow band screen = addresses only one or two specific components of development. | |||
| Does the screening tool’s age range match the target age range for the early detection/ Child Find program? E.g., Is the age range from 0 to 6 years? | |||
| Are the costs of screening for materials, scoring and interpretation (time-related costs) considered to be affordable for the early detection / Child Find program or clinic? | |||
| When an interview is needed for language or literacy reasons, are the costs of screening for materials, scoring and interpretation (time-related costs) considered to be affordable for the early detection / Child Find program or clinic? | |||
|
a
Is the time frame to administer and score the screen |
|||
| Is the number of items and type of screening tool items considered acceptable to caregivers/parents? | |||
| Is there a parent-friendly online, electronic tablet, or App-based version of the screening tool with different language options and automated scoring? | |||
| Is the screening tool compatible with electronic medical record systems currently being used in health care settings? | |||
| Are there any training resources available to better implement the screening tool? | |||
| Are there screening tool materials or a kit that is needed to complete all of the items? | |||
| a Is the readability (grade level) at or under the 5th grade? | |||
| a Are there multiple language translations available with culturally appropriate items that meet the needs of the community (e.g., English and Spanish for the USA)? Translations for the most commonly used languages should ideally be available in each country. | |||
| a Is para-professional administration and/or scoring okay? | |||
| a Are the administration and scoring directions clear and concise? | |||
| a Are the interpretation guidelines for professionals clear and concise? | |||
| Does the screening tool have any accompanying parent-centered learning activities that promote developmental and/or social-emotional skills? | |||
| Are there any referral guidelines or templates for a two-way consent form that are included with the screening tool kit? | |||
| Are there any developmental-behavioral monitoring / tracking / growth charts that are included in the screening tool kit? | |||
| Has the screening tool been proven to be feasible in multiple peer-reviewed studies or a systematic review (not just one study)? |
Core standard considerations.
Author’s Note
You may reach Marisa Macy, PhD by email at
You may reach Kevin Marks, MD by email at