
Abstract
Transformative Service Research (TSR) highlights the fundamental importance of resource integration for consumer well-being. However, recent research suggests that resource integration can be problematic and imperfect, particularly for vulnerable consumers with complex and ongoing resource requirements. Such vulnerable consumers may face transition challenges and end up in an uncertain “in-between” experience of liminality, where the linkage to resource integration remains under-researched. In response to recent service prioritization challenges, we explore how vulnerable actors experience liminality and resource integration in service systems. The vulnerable actors highlighted in this study are parents in families of children with life-long conditions (e.g., autism spectrum disorder/ASD and Down syndrome). We reveal a new form of liminality as a persistent, relational phenomenon that interdependent vulnerable actors with ongoing complex resource needs collectively experienced within service systems. Further, we identify the dynamics of persistent liminality as Precipitating, Subsisting, and Resisting. Finally, in line with TSR, we shed light on the resource constraints that decrease the well-being of vulnerable consumers. We also identify implications for theory, practice, and future research.
My favorite line out of any movie would be “just keep swimming” from “Finding Nemo.” Because that’s what you do, when you have a special needs child, that’s what life is. You don’t know what next week is going to bring (Margaret, parent of 12-year-old boy with ASD).
Introduction
Consumers’ well-being is significantly impacted by the service systems with which they interact to cocreate value (Anderson et al. 2013). Systemic views of value cocreation, underpinned by service-dominant (SD) logic (e.g., Vargo and Lusch 2016), define value as attainable outcomes “realized from the integration of resources through activities and interactions with collaborators in the customer’s service network” (McColl-Kennedy et al. 2012, p. 370). These discourses related to systemic value cocreation and research integration are founded on several normative assumptions. First, actors (including consumers, families, managers, organizations, and politicians) have unlimited agency and abilities to identify, acquire and integrate resources to cocreate value-in-use within service systems (Ng, Sweeney, and Plewa 2019). Second, there is a tacit assumption that resource integration creates value for beneficiaries (Karpen and Kleinaltenkamp 2019). Third, service systems are viewed as self-adjusting and resource-replenishing (Lusch and Vargo 2014), offering access to self- and/or system-generating resources.
However, a small but growing corpus of studies has begun to problematize and critique this overly optimistic view of systemic value cocreation (see Echeverri and Skålén 2021). In tandem, service scholars are calling for further research on resource constraints to improve service system flexibility to meet consumers’ changing needs (Ostrom et al. 2021). Whereas early work emphasizes actors’ misuse of resources as deterring value cocreation (Plé and Cáseres 2010), Plé (2016) characterizes unsuccessful resource integration, namely, resource misintegration, as a systemic phenomenon which occurs when one or more actors do not or cannot access, use or integrate resources in ways that are congruent with the other actors and/or institutions involved in value cocreation. This may occur, for example, when there is a mismatch between resource demand and supply or when actor needs are intense, uncertain and/or stressful (Dauphin et al. 2020).
Resource integration becomes particularly contested in situations where actors may not have equal agency or skills to engage in it (Kelleher et al. 2020). This is a notable risk for those in the weakest positions in society, vulnerable consumers for whom the implications and consequences of resource integration challenges are likely to be the most significant. Transformative Service Research (TSR) highlights the need to study vulnerable consumers embedded in service systems (Anderson et al. 2013), emphasizing the importance of resources for consumer well-being outcomes. Such concerns are echoed in a recent prioritization of service challenges (Field et al. 2021) that exhorts service scholars to address the inequities that concern vulnerable citizens and to reduce barriers to service access and utilization. It is important to note that vulnerability is not necessarily a fixed attribute but rather “a state of powerlessness […] an imbalance in marketplace interactions which arises from the interaction of individual states, individual characteristics, and external conditions within a context where consumption goals may be hindered” (Baker et al. 2005, p. 134). Vulnerable consumers may therefore include those who are experiencing vulnerability through market or societal exclusion, marginalization or through diminished agency, such as people who are financially insecure, less educated, who are mentally or physically ill, whose needs are complex and difficult to meet. Vulnerable consumers also include secondary vulnerable consumers, whose position is derived from their close ties to a person in a primary vulnerable position (Pavia and Mason 2014). The experience of one such group, namely, parents of children with ongoing and complex additional needs, is characterized by liminality (Ryan and Runswick-Cole 2008).
Whereas liminality refers to “a state or process which is betwixt-and-between” and often occurs as part of social transition processes such as growing up, moving house, divorcing, or losing loved ones (Turner 1979, p. 465), families may end up living with permanent liminality i.e., long-term transitions that lack an anticipated end (Appau, Ozanne, and Klein 2020). In the case of children who have ongoing and complex additional needs, with no opportunity to transition into independent adulthood, such enduring liminality may severely impact parents and families who are unable to exit from this liminal state. They and their children remain trapped in an unending state of uncertainty and precarity. This observation served as the starting point for studying enduring liminality. Moreover, despite its importance, the dialectic between liminality and resource integration remains under-researched. A deeper understanding of the interplay between resource integration and liminality contributes to TSR by shedding light on vulnerable consumers’ experiences of assessing and integrating resources. It would also help organizations devise strategies to better support families with complex and ongoing resource requirements.
In line with such critical perspectives, our study aims to explore how families experience liminality and resource (mis)integration in service systems. Our focus is on complex service systems comprising multiple actors, interactions, and actor interdependencies (Pinho et al. 2014) including healthcare and, by association, education. Such human-centered service systems (Breidbach et al. 2016) are highly dependent on human actor orchestration to cocreate value, posing further complexity. Drawing on the experiences of vulnerable actors embedded in family systems, parents of neuro-divergent children e.g., those with autism spectrum disorder (ASD) or genetic conditions such as Down syndrome, our findings reveal how parents and families experience persistent liminality and resource (mis)integration.
Our contributions are three-fold. First, we reveal persistent liminality as a dynamic, relational, and unending cycle of evolving and recursive transitioning, which is collectively experienced by interdependent and vulnerable actors bound by uncertain, ongoing, and complex resource requirements. This form of liminality keeps shifting and changing, which makes it challenging and exhausting for the parents as there is no resolution. Rather than resulting from a predefined individual transitional process, we build on Appau, Ozanne, and Klein’s (2020) incorporation of both individual and social dimensions to reflect how liminality is experienced by actors in relation to others connected through social relations. Second, we reveal how persistent liminality is experienced as the interplay between family caregiving realities and resource (mis)integration and comprises three dynamics—Precipitating, Subsisting, and Resisting—that explicate how persistent liminality emerges and is sustained in interactions between vulnerable consumers and service systems. Third, in line with TSR, we shed light on the resource constraints within maladaptive service systems that decrease the well-being of vulnerable consumers and that accentuate and sustain resource misintegration and persistent liminality. Together, these findings advance knowledge of the relationship between vulnerable consumers’ experiences of liminality and resource integration.
We structure our paper as follows. We begin by tracing the theoretical origins of liminality to reflect its emergence as a central characteristic of parents’/families’ everyday experiences in service systems. Next, we discuss resource integration and its corollary, resource misintegration, in service systems. We then detail our empirical study and present our findings, concluding with contributions, implications, and avenues for future research.
Liminality and Resource Integration in Service Systems
Liminality in Service Systems
Liminality has its anthropological origins in the work of Van Gennep (1909/1960), who studied various rites of passage in primitive societies. These encompassed three phases—separation (pre-liminal), transition (liminal), and incorporation (post-liminal)—each characterized by changes in social structure, actor agency and position, and impacting identity (c.f. Andrews and Roberts, 2015). Extending Van Gennep’s work beyond the anthropological sphere, Turner (1979) defined liminality as “a state or process which is betwixt-and-between the normal, day-to-day, cultural and social states and processes” (p. 465). The liminal period is an indeterminate time and state where the present ceases to exist for the actor (also referred to as luminar) and is characterized by experiences of uncertainty regarding the future.
Although liminality is characteristically contingent and temporary, paradoxically, it can become permanent in certain instances (Appau, Ozanne, and Klein 2020) where transition is impossible or unsuccessful (Murphy and McDowell 2019). To characterize such an enduring form of liminality, Appau, Ozanne, and Klein (2020, p. 167) propose the term permanent liminality, which describes “transitions that can span years and even a lifetime with no anticipated end.” Permanent liminality comprises a social space “when a temporary suspension of the normal, everyday, taken-for-granted state of affairs becomes permanent” (Szakolczai 2009, p. 233). Murphy and McDowell (2019) explore permanent liminality in settings affected by ongoing conflict and identify how transitional processes can become trapped. Similarly, Appau, Ozanne, and Klein (2020) evidence how permanent liminality follows the demarcated stages of Van Gennep’s rites of passage when endless cycles of separation and incorporation continuously repeat as individuals experience becoming members of the Pentecostal church. However, they do not examine the circumstances and mechanisms whereby separation occurs but no reincorporation happens. In such a case, permanent liminality is characterized as an enduring state of stasis without desired transition, a form of temporal entrapment. Exploring food insecurity experiences, Moraes et al. (2021) identify liminality as non-linear and persistent involving a cyclical reliance on supplementary food services. Within healthcare, Nakata et al. (2019) explore how liminality characterizes the journey for patients suffering from chronic illness, who oscillate between treatment compliance and non-compliance over the long term. In the context of ASD, Ryan and Runswick-Cole (2008) argue that liminality is underlined through a lack of appreciation of the skills, expertise, and resources that mothers (need to) acquire, suggesting that resource integration may play a role in accentuating liminality.
Although the predominant scholarly focus to date has been on the indeterminate (liminal) state within which actors find themselves or the associated outcomes, a deeper interrogation of the nature and dynamics of liminal experiences remains lacking. This lacuna is highlighted by Söderlund and Borg (2018, p. 15), who call for a deeper understanding of “how individuals view the liminal experience and how it is perceived when it unfolds and what tensions are involved.” Entering or remaining in a liminal state is, above all, an experience fraught with danger, as the actors may potentially lose their identity and status without them being replaced (Andrews and Roberts, 2015). Some may become luminars and experience paradoxical identities and psychological risks (Ladge, Clair, and Greenberg 2012), resulting in a suspension in time of normal life and prior structures. Whereas luminars may find themselves physically and socially marginalized, others may conversely experience communitas involving a positive collective experience of liminality (Turner 1982). Although research on permanent liminality has advanced the understanding of an enduring liminal state, little is known regarding the dynamics of liminality in terms of its temporal and processual aspects and how it evolves and is experienced over extended time-periods. In complex service systems, such as healthcare, involving multiple actors, interactions and actor interdependencies (Pinho et al. 2014), and, more particularly, within multiple intersecting service systems, exiting a liminal state may be particularly difficult. Actors must often navigate complex resource integration challenges to cocreate value on behalf of dependent others (Kelleher et al. 2020). Hence, of particular interest is the interrelationship between liminality and resource integration that may have a substantial impact on value cocreation and well-being outcomes, particularly in cases of actor vulnerability.
Resource Integration in Service Systems
Over the past two decades, systemic perspectives of value cocreation have received increasing interest, in tandem with the ongoing scholarly engagement with SD logic. Service systems are defined as “relatively self-contained, self-adjusting systems of resource-integrating actors connected by shared institutional arrangements and mutual value creation through service exchange” (Lusch and Vargo 2014, p. 161). Bruce et al. (2019, p. 182) suggest that resource integration is a “process consisting of activities to assemble, master, and optimize resources, to plan and fine-tune usage events in real-time, and to reflect upon previous activities,” positioning customers and other actors as overseers of value cocreation. Within the systemic perspective, all economic and social actors are viewed as willing and able resource integrators (Lusch and Vargo 2014; Vargo and Lusch 2016). Central to the definitions of resource integration is the characterization of resources as “anything an actor can draw on for support” (Vargo and Lusch 2019, p. 740).
Within the SD logic discourse, several studies build on assumptions of uninhibited actor agency and the ample self-generation of resources through recursive resource integration (Ng, Sweeney, and Plewa 2019; Sweeney, Danaher, and McColl-Kenedy 2015). Applying the principles of problematization (Alvesson and Sandberg 2011), we question the assumptions that service systems always can or will self-adapt to meet actors’ resource requirements and that all actors have access to the resources that they need within service systems. A growing corpus of studies on value co-destruction and resource misintegration (for review, see Echeverri and Skålén 2021) suggest, for example, that actors face several challenges in identifying, accessing, securing, or integrating the resources that they need, but empirical research outlining why and in which contexts this occurs is largely absent. These problematic resource integration challenges have been attributed to many factors, including service providers who may fail to provide necessary resources or fulfill their value proposition (Smith 2013), power relations between actors (Echeverri and Skålén 2021; Mustak and Plé 2020) and multiple actors’ diverging value perceptions that lead to conflict and failure to realize value for all (Cabiddu, Moreno, and Sebastiano 2019; Laamanen and Skålén 2015; Skålén, Aal, and Edvardsson 2015). Building on Plé (2016), Laud et al. (2019) present a typology of resource misintegration manifestations and explain their causes. These include lack of resources, blocked access, lack of understanding, incapacity or disagreement over how to integrate resources, along with deceptive, negligent, excessive, or coercive integration of resources. Further, Dauphin et al. (2020) propose that resource misintegration may be attributable to a mismatch between resource demand and supply or when actor needs are intense, uncertain, and/or stressful. Despite these advancements, Echeverri (2021, p. 104) criticizes extant resource integration discourses for their inability to uncover “what really matters to actors” owing to an overarching focus on the static resource integration organizing and coordinating mechanisms.
Within healthcare and social care service systems, successful resource integration requires feedback from interactions between actors and institutions to correctly identify actors’ intended actions and desired resources to realize their goals. Although patients are themselves responsible for many of their well-being outcomes (Azzari et al. 2021), medical interventions requiring adherence and compliance often fail because service providers do not adequately account for or accommodate how customers integrate resources (Spanjol et al. 2015). In other cases, faced with prolonged illness and resource challenges, patients become surrogate healthcare workers, requiring job-crafting efforts (c.f. Azzari et al. 2021). Exploring caregiver role and identity, Gummerus et al. (2021) show that caregivers often shoulder a greater responsibility than intended for resource integration to ensure the well-being of their loved one(s). Moreover, if patients or their caregivers cannot access experts within service systems or do not align with the institutional arrangements of healthcare service providers (or vice versa) (Karpen and Kleinaltenkamp 2019), they will fail in their role as resource integrators, resulting in negative well-being outcomes (Anderson et al. 2016). The healthcare and social care literature therefore diverges from the SD logic literature in highlighting that actors as opposed to systems are adaptive and self-adjusting by developing resource integration strategies to counter or navigate resource misintegration.
Returning to Lusch and Vargo’s (2014) assumptions that all actors are able and willing resource integrators, it would appear that in the absence of ongoing, optimal resource integration, actors are left in a state of “betwixt-and-between”: that is, experiencing liminality. This important dialectic between liminality and resource integration in service systems has not yet been addressed. We will next turn to our method and findings, which address the calls to study how vulnerable actors experience resource integration inequities (Field et al. 2021).
Method
Research Design and Context
A participatory approach, involving both academic and non-academic actors, was adopted to increase the societal and transformative impact of the research and to mitigate potential harm relating to the research process (Davis and Ozanne 2019). The empirical study aimed to explore how actors (parents of children, adolescents, and young adults with additional needs, particularly ASD and Down syndrome) experienced resource integration and liminality in complex service systems. These parents are actors in family systems where the children’s needs for resources are complex, long term, and difficult to resolve and are embedded in interconnected service systems. The research was undertaken in Finland and Ireland. Acknowledging the differences between the public healthcare service systems servicing families with ASD and Down syndrome in both countries, families face similar challenges in accessing and securing resources to meet their needs, which are related to both the complexity of the children’s conditions and the complexity of the service systems with multiple actors, interactions, and interdependencies (Pinho et al. 2014).
The Irish public healthcare system is highly fragmented, comprising a range of primary and secondary care services incorporating pediatricians, occupational therapists, psychiatrists, psychologists, and speech and language therapists. It is also dependent on effective co-operation between various healthcare service providers and other core services such as education (e.g., children’s day-care, early learning centers and schools), child welfare, and other social and community services. Indeed, one study of ASD public healthcare services in Ireland highlights several key barriers to accessing services, including ineffective interdisciplinary/interagency collaboration, a lack of clear pathway to services, lack of standardized care delivery, inadequate evidence-based practice and appropriate intervention, inadequate information and support for families, lack of training among health professionals as well as inadequate forward planning of transitions from diagnosis through school age to adulthood (Health Services Executive 2017). The Finnish system is equally complex, and persons with ASD fall within different legislation frameworks depending on whether they are intellectually disabled. As described on the City of Helsinki (2021) webpage, “The majority of people with an autism spectrum disorder will receive their services from other service providers than those specifically intended for people with an autism spectrum disorder.” In Finland, individuals with ASD and their families experience several barriers to their inclusion in society (Wallace, Guldberg, and Bailey 2019).
We characterize the Irish and Finnish public health sectors as complex service systems involving multiple actors, interactions, and interdependencies (Pinho et al. 2014). Furthermore, as human-centered service systems, they rely on human actors to orchestrate value cocreation (Breidbach et al. 2016), which can entail significant challenges in accessing resources including health services, personnel, and supports. Their complexity is further heightened through their interrelationships with other closely linked services, such as education and related child services, as well as their dependence on private (fee-paying) services that are often engaged to compensate for failures in the public system. Although a range of national, regional, and local government and voluntary bodies in Ireland and Finland has been established to advocate for families and people with ASD and Down syndrome and to offer additional services and support, they are limited in resources and scale. The first and second authors contacted three such organizations: a regional support unit representing families with ASD in Ireland [Irish Organization A], a national body representing and advocating for families with children with ASD and representing 3400 members [Finnish Organization A] and a national organization representing families with Down syndrome and its local branches with over 3500 members [Irish Organization B]. In line with the participatory approach adopted, representatives from all three organizations were consulted before finalizing the research question, design as well as the final analysis. The study was then submitted to the institutions of the first and second authors for parallel ethical approval.
Data Collection
Interview participants.
Following Stokes (2006), during the interviews, the first and second authors invited participants to reflect on, make sense of and share their experiences of living with and caring for a child with additional needs/abilities and accessing healthcare and other services. Using a loosely structured interview protocol (Appendix A), every effort was made to solicit participants’ narratives, perspectives, and worldviews, as opposed to imposing a framework or structure by the researchers. A flexible approach was adopted so that interviews flowed in a conversational style, where participants were put at ease and felt free to raise questions and concerns throughout, allowing new insights and trajectories to freely emerge (Denzin and Lincoln 2017). Following some initial questions that explored participants’ family situations and caregiving and parenting practices with respect to the child/adolescent/young adult with additional needs, participants were invited to reflect on how they experienced caring for their child (in some cases, multiple children) and how this impacted the child/ren, them as parents and other family members. We then probed how such experiences varied and were impacted by actors, resources, and/or the overall service system(s) over time.
Throughout the interviews, participant sensemaking and reflection were facilitated through sensitive and timely probing, active listening, and the effective use of silence. In addition, interviewers noted in field notes their reflections and emotions after each interview, as well as their own emergent sensemaking. Both interviewers systematically debriefed the research team following each interview to collectively gather immediate insights and to strengthen the quality and trustworthiness of the data in real time (McMahon and Winch 2018). The third author acted as a “critical friend” at these debriefings by probing and questioning the emergent interpretations. The debriefings acted as an informal support within the team to counterbalance the emotional work involved in conducting research on a sensitive topic while also enabling professional detachment and full attention to the deeply personal experiences that the participants were sharing (Dickson-Swift et al. 2009).
Data Analysis
Following each interview, the interview recordings and field notes were transcribed. In addition, the Finnish interviews were translated into English to enable individual and then group coding by each of the three authors. Our qualitative study followed a hermeneutic approach (e.g., Thompson, Pollio, and Locander 1994), wherein analysis and interpretation entailed a back-and-forth movement between data and theory (Spiggle 1994). Specifically, we employed a three-stage coding process, with each team member initially coding the data independently. Following Gioia, Corley, and Hamilton (2012), we first employed open coding to label the raw data shared by participants as well as the first and second authors’ reflections. During this stage, liminality emerged as the sensitizing lens through which subsequent coding took place, including references to an unresolved state, feelings of being unable to move forward, uncertainty regarding diagnosis and care and fear regarding an unpredictable future. Then, we conducted axial coding with thematic analysis, which resulted in second-order constructs. The concepts related to the challenges around the condition and diagnosis evolved into a second-order theme Evolving Condition and Care Dilemmas, whereas resource-scoping challenges became a second-order theme Resource Obscurity. Finally, we continued to condense and abstract the themes, focusing more on theoretical development, until we derived the aggregate dimensions of Precipitating, Subsisting, and Resisting that reflect the dynamics of persistent liminality linked to the interplay between Family Caregiving Realities and Resource (Mis)Integration. The more in-depth analysis process and data structure are reported in Appendix B. Before finalization, member checks were conducted to ensure trustworthiness and congruence between the research team explanations and participants’ sensemaking of their experience and situations.
Findings
Overview
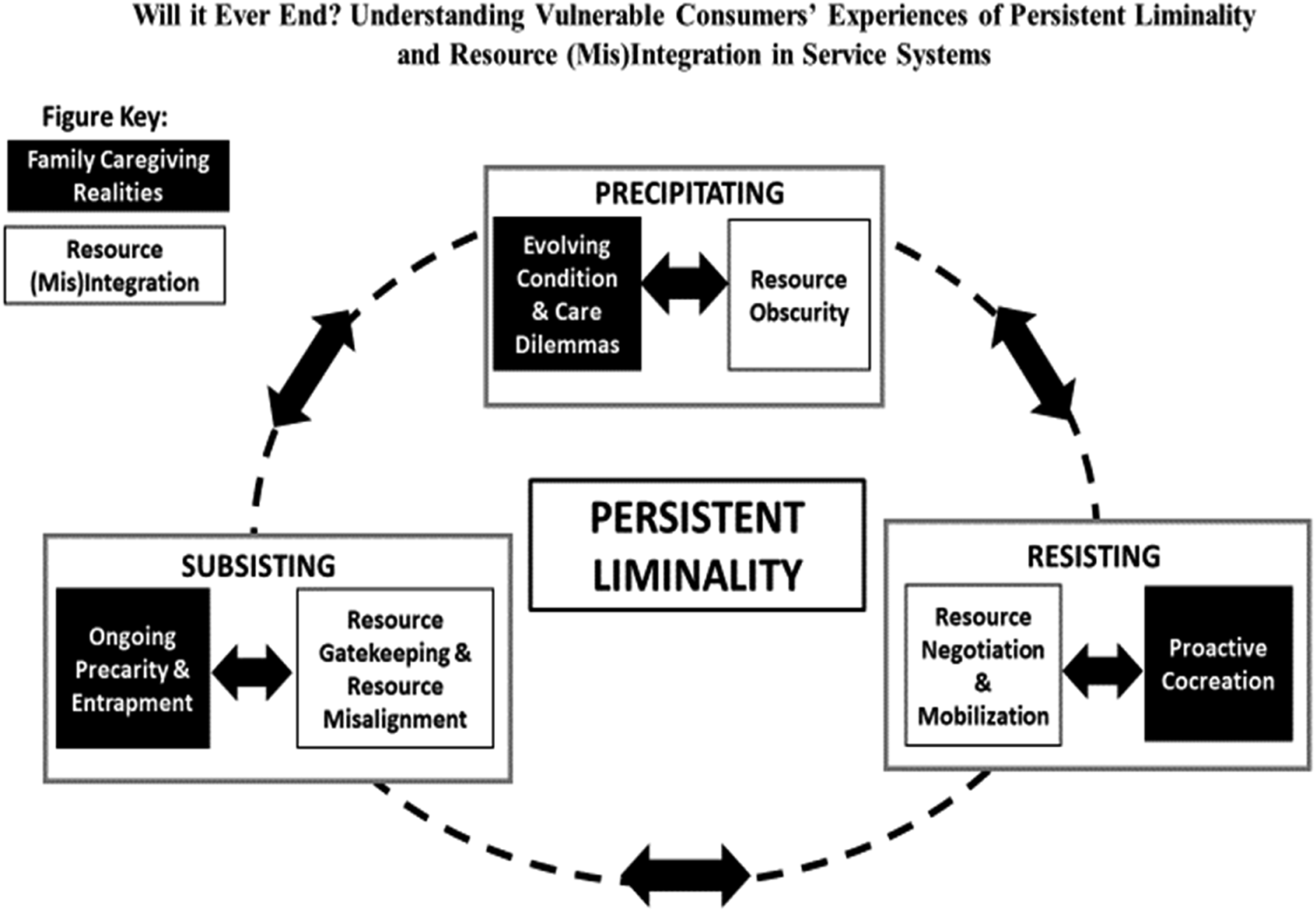
Through an iterative process of data analysis and theoretical interpretation, we developed our conceptualization: Vulnerable Consumers' Experiences of Persistent Liminality and Resource (Mis)Integration (Figure 1). Vulnerable consumers' experiences of persistent liminality and resource (mis)integration.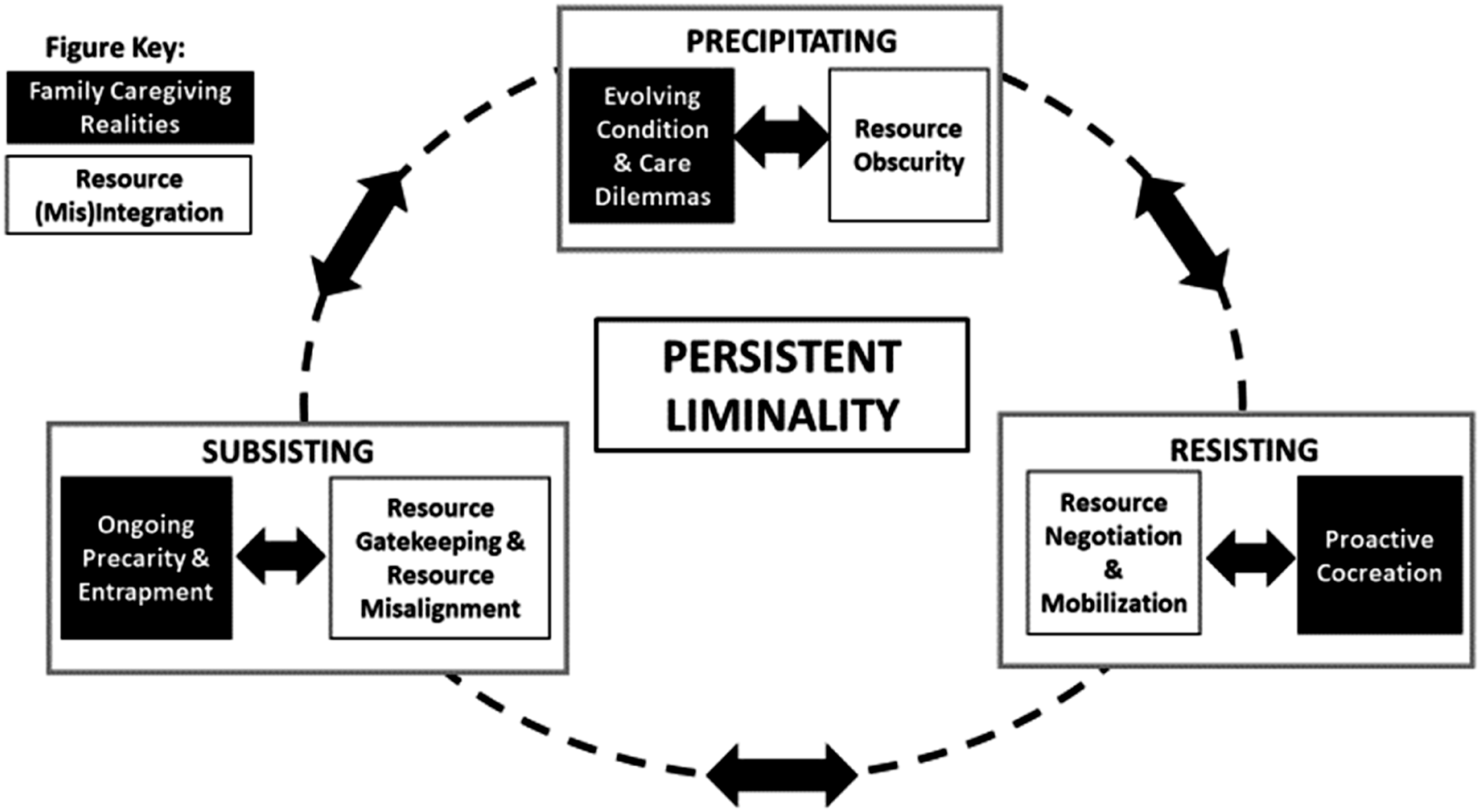
We define Persistent Liminality as a dynamic, relational, and unending cycle of evolving and recursive transitioning, which is collectively experienced by interdependent and, in our case, vulnerable actors bound by uncertain, ongoing, and complex resource requirements. This form of liminality keeps shifting and changing, which makes it challenging and exhausting for the parents as there is no resolution. Our findings advance previous conceptualizations of liminality by illuminating and evidencing its evolving, challenging and enduring characteristics. In our study, Persistent Liminality emerged where children with complex and ongoing additional needs, who experienced resource misintegration, were unable to transition to independent adults and their parents, as caregivers, were unable to move forward.
The enduring nature of persistent liminality was reflected in parents posing soul-searching question such as “will this ever change?” (Anna) or expressing that their life had been put on hold: “I want to have a life. I want a life back” (Sinead), whereas the relational nature of liminality emerged through reflections on how the child’s condition affected the whole family and others beyond: “we were at a real crisis point in our family” (Bernadette) and “I backed away from my family; I backed away from my friends. That’s what it does to you” (Gary).
Following deeper thematic analysis, persistent liminality manifested in our data as three dynamics, which we term Precipitating, Subsisting, and Resisting. Specifically, persistent liminality and each of its three dynamics emerged from the interplay between and caregiving complexities (Family Caregiving Realities) and resource integration challenges (Resource (Mis)Integration), which are enduring and recursive. This combination resulted in a wicked problem that was challenging to deal with and resolve.
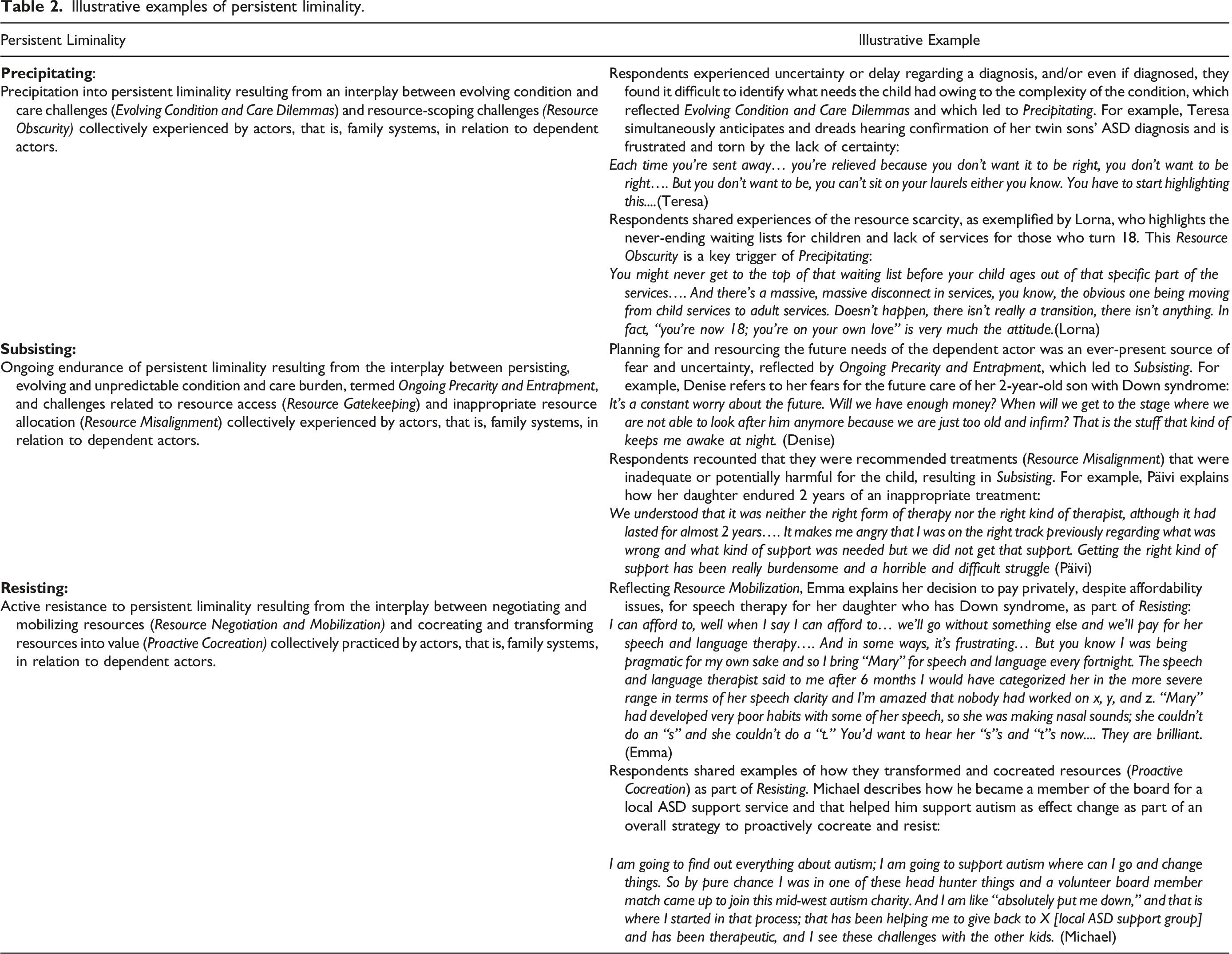
Illustrative examples of persistent liminality.
Precipitating
Precipitating reflects the interplay between the complex and changing condition and care needs of the children, captured by Evolving Condition and Care Dilemmas, and the difficulty in identifying resources to fulfill the needs of their children along with where and how to access them, that is, Resource Obscurity. This was accompanied by parents’ realization that the requirement for ongoing resources and their replenishment would be life-long and shifting. As the children’s conditions evolved, so did their needs for support, resulting in the continuous requirement to find new solutions which accentuated persistent liminality.
Evolving Condition and Care Dilemmas—Resource Obscurity
Precipitating first manifested at the initial diagnosis stage or when early symptoms emerged. For many, the “not knowing and the fear of it [the condition]” (Teresa), along with the gradual realization that their children’s ongoing conditions would restrict the life of the caregiver and the child, precipitated a trajectory fraught with uncertainty and unpredictability. As the complex condition and care needs evolved, it became clear to the families that the liminality remained unresolved. As Sinead reflected, As he (son) has grown older, we’ve just seen deficit after deficit after deficit. And it’s things like every time you get something settled, every time you figure something out and you learn how to deal with that, another piece of the puzzle disappears, and you have to figure that out (Sinead).
Liminality similarly emerged through the unfulfilled dreams for their children and the life that they could have led. Parents expressed sadness and fear when the full realization of a future with significantly different expectations, worries, and concerns regarding their children’s long-term health and happiness began to sink in. In Frank’s case, following the years of coming to terms with his son’s condition, his aspirations for his son faded and he was bereft: …It was like a death in the family…my aspirations for my super star soccer player and all that, all went out the window and you had to restart everything so that the first six years of your life [as a parent]…of his life is gone. (Frank)
Maladjustment was also experienced by the children who sometimes rejected or denied their own condition and, as reflected by Margaret’s son, shunned the services that they might benefit from, further triggering unresolved feelings within the family: … he’s very aware and he doesn’t like being autistic. … And he’s not silly; he knows he’s, he knows himself like…he is now pushing the autism away…he says he’s “not too sure about the [ASD] social clubs.” It actually broke my heart to hear him say it. He said “you know other autistic children make me feel uncomfortable.” (Margaret)
The unpredictability of the future illness trajectory and uncertainty regarding access to opportunities for their children were experienced as constant sources of fear and risk, further reflecting an unending state of liminality. This uncertainty was underpinned by parental efforts to learn about and understand their children’s diagnoses, the future challenges that their children might face as well as their future care needs, including their educational needs. Lorna predicted challenges regarding where and when her child will be allowed to access high school: I don’t know where secondary school is going to be and when we’re going to be there. (Lorna)
Beyond educational needs, care dilemmas comprised parents’ difficulties in defining which challenges formed part of normal child development and which ones stemmed from the children’s additional needs. Parents also experienced uncertainty regarding their role and responsibility in relation to their children’s behavior and what they could do to help their children cope better. As Päivi explains, parents often felt that they had to defend their child’s eventual misbehavior to others, such as teachers, family members, or friends, reflecting the relational nature of liminality: One must keep explaining and defending [the child and his/her misbehavior] – the child has these diagnoses that in part explain the behavior, but one does keep thinking what one could have done differently. (Päivi)
Besides educational and health-related challenges, children and particularly teenagers, while growing up, often faced challenges in fostering social relationships, necessitating parents to act as arbitrators when engaging with others. Families’ situations were further exacerbated when their children’s needs were unmet due to challenges in identifying appropriate resources. We term this Resource Obscurity. It was difficult for parents to know which services their children needed and were entitled to, where and from which institutions the services could be accessed, and whether the actual services received were optimal. Although nominally a wide range of services, therapies, treatments, providers and agencies were available within the healthcare system, participants highlighted the obscurity of such resources and reported significant challenges regarding scoping and devising the appropriate care plans for their children. The formal healthcare service system frequently did not fully recognize ASD as a condition when compared with more visible, physical conditions, even though it often entailed severe symptoms and long-term challenges. This meant that the available resources remained obscure. [ASD] is not considered a disability [by the public healthcare system in Finland] but rather a characteristic and not a developmental disability. However, there are so many challenges. They [children with ASD] kind of fall between the cracks. (Helena)
Resource obscurity in the form of service system unresponsiveness was further reflected in the references to the “bureaucracy and the red tape” (Paula) and the feeling of being “sent around in a circle” (Margaret) or being told that “there is nothing wrong with that child” (Paula). When parents finally received an appointment for their child with a health or educational specialist, there was further obscurity in acknowledging the condition, the diagnosis and/or as identifying and coordinating appropriate treatments and supports across intersecting service systems. Sinead described the harrowing case of her 11-year-old son who had severe attention deficit hyperactivity disorder (ADHD) and autism and who suffered from suicidal ideation. She recounted how she was advised by the psychiatrist within the mental healthcare service system to “tell him to get over it” and to inform the school or educational systems “to ignore it, that he was only doing it for attention.” This was met with shock and disbelief by the school principal, who was supportive but who lacked the specialized knowledge and resources to cater for her son’s complex needs. …. She [psychiatrist] told me to send my child to school and tell him get over himself. And she told me that if he talked about killing himself, tell the school to ignore it, that he was just doing it for attention. Now I went and spoke to the principal of his school at the time; he was 11 years of age. And I said to her “this is what I’ve been told,” and she just went “oh my God”; she said, “you never ever ignore a child that says they want to kill themselves.” (Sinead)
Resource obscurity was evident in other cases too in terms of gross inconsistencies in identifying the needs of the child and identifying necessary resources. Bernadette describes the challenges she has experienced in gaining recognition for her son’s severe ASD, oppositional defiant disorder (ODD) and pathological demand avoidance (PDA) condition alongside the inability of the various child mental health and social/family and police services to identify solutions that would meet his complex psychological needs. The ongoing resource obscurity and failure of the healthcare systems to recognize or treat PDA and the aggressive behavior means that the family finds themselves in an unending liminal state. I’ve been ringing the people that you know you think are the ones that should care. And yet you end up kind of having to do it all yourself and find your way yourself; I mean the first time I mentioned PDA [pathological demand avoidance], I’m told it’s not a clinical diagnosis. So I put it aside; I was told, “that’s something that’s just made up,” but it’s not. It’s around since the ‘80s; it is recognized; it’s something that will help J [son], but I had to discover that myself. (Bernadette)
Their experience of liminality was further accentuated by the fear that the son would be transferred to criminal services once he turns 12 owing to the obscurity of the appropriate resources within the intersecting service systems to meet his complex needs: We had a police liaison, a juvenile liaison officer, come out…to try to talk to him. Social services, I spoke to them, again there wasn’t anything anybody could do…. My concern is his future; this is a child who is getting bigger, and he’s so aggressive… and I suppose the outlook isn’t great…. I think it is a social welfare issue right now but that once he’s over 12, it’s criminal. It is, it gets very serious…life is going to be very, very hard for him. (Bernadette)
For families and specifically parents, who initially held hopes and dreams for a healthy child and a future filled with excitement and positivity, their lives were irreversibly disrupted. The evolving nature of the child’s condition and care needs implies that there is no moving forward, rather an ongoing accommodation of complex dilemmas and challenges with no reintegration possible. The resultant impact on family well-being is significant, accentuating vulnerability, and leading to long-term physical, psychological, social, and economic outcomes.
Subsisting
Subsisting emerged from the Ongoing Precarity and the resulting experiences of Entrapment, when parents were faced with the unceasing challenges of resource access, expertise and support (Resource Gatekeeping) and inappropriate resource allocation (Resource Misalignment). In such cases, families could only subsist or endure persistent liminality, lacking the agency, capacity, or energy to transition beyond it or to actively counter it.
Ongoing Precarity and Entrapment—Resource Gatekeeping and Resource Misalignment
Susbsisting reflected a state of value stasis (rather than value cocreation), of being stuck despite parents’ best efforts to secure resources or remaining stuck even when partial or inadequate resources were secured. Feelings of ongoing precarity and entrapment were further complicated by the case-specific nature of the children’s condition involving differing levels of cognitive abilities and developmental and health concerns. Reflecting the persistent nature of her liminality and struggle to get by, Maria likened this to a “continual grieving process, where parents were constantly and acutely impacted by the limitations that the children’s conditions placed on the children and the parents. As Maria recounted: He has the diagnosis, and it is very clear that he has it [ASD], but perhaps just it’s, it has become a continuous grieving process; it’s not like you lose something once, but rather it is this reminder of everything that restricts my life and even more his life, so it is this continual process, not like all the time compare what others are doing and what he does not do, but rather try to be happy over his advancements. (Maria)
Restricted resource access coupled with the inadequacy of resources and supports forced parents to prioritize their children’s care over their own needs and to commit themselves to a lifetime of caregiving. For many, the “path was laid out” (Denise), and many were “stuck” (Sinead), often unable to take control of their lives “we don’t know where we are going” (Frank) and unable to move forward or to plan a future with any kind of determinacy. The example of Teresa below reflected the experience of several parents who had to give up their jobs to pursue caregiving due to being excluded from the service system. In Teresa’s case, her autistic twin sons were refused access to the childcare system, forcing her to become their full-time caregiver: I’m probably going to be a caregiver for the rest of my life…. I was very angry that I had to give up my job because there’s no crèche [children’s day-care center] that will take a child with a disability. I was forced into being the full-time caregiver. You kind of lose that sense of yourself. (Teresa)
Teresa’s comment “you kind of lose that sense of yourself” signals how her sense of disconnection and entrapment ensued. This shows how liminality could lead to a dilution of one’s self-identity: not being the same as it was before but lacking an acceptable alternative. Such perceived changes to self-identity and role were shared by many respondents and clearly reflect the impact of liminality on identity.
There was also a stark realization that ongoing precarity and entrapment would continue into the next generation, where other siblings would be forced into caregiving, reflecting how persistent liminality may temporally and relationally expand. Mary feared that her two other children would be tasked with caring for their younger sister with Down syndrome in the future, where their roles would change from being siblings to “new caregivers”: As I said, the fear is of the burden that she may possibly be on them rather than how they would integrate into her life I suppose…them having to take over from us as caregivers rather than her being a sibling as part of their lives. I suppose it’s just that fear: are they going to be the new carers rather than siblings? (Mary)
Parents’ and families’ experiences of persistent liminality were further reflected in cases where their adult children continued to be on medication, draw on “adult services” and were unable to live independently. This was described by Paula, whose eldest son (22) suffered from ASD and other forms of anxiety and who continued living at home: He was a late diagnosis at age 14… He’s on Prozac; he’s medicated. He’s under adult services now, so we attend X Mental Health services. He sees the psychiatrist and the occupational therapist to help him. (Paula)
Alongside experiences of ongoing precarity and entrapment, parents’ situations were exacerbated by restrictive access to services, expertise, and appropriate supports, which we term Resource Gatekeeping. Obtaining an initial diagnosis, which was a prerequisite for accessing specific resources and services, was the first major challenge faced by parents: It kind of feels like it is a criterion for disability services or an alibi for not having to offer any benefits or services because the child does not have a disability diagnosis. (Helena)
Others, such as Sinead, felt that the resource gatekeeping was caused by the service system being stretched over its limits and lacking sufficient resources: And I think part of it is the services are over-stretched. They can’t take on anymore, so they’ve made a decision that anyone with autism is not their responsibility and it’s somebody else who has to deal with it. (Sinead)
Paula described how her negotiations with several agencies within the Irish healthcare system to access counseling services for her son were overshadowed by resource constraints. When they start discussing it around the table, you’re getting nowhere. When you ask for something, you get the response: “we’ve so many children on our books.” They throw you scraps; you’re meant to be grateful. “We’ve given him six sessions last year” and you’re like: “Yeah, but they were six generalized sessions about something that isn’t specific to what he needs.” Things like actual counselling for the child?? There doesn’t appear to be any such thing. Apparently, nobody can offer those services. (Paula)
Despite Paula’s informed understanding of her child’s needs, the lack of access to and appropriateness of the resources and services on offer underlined the level of resource gatekeeping, where parents such as Paula were expected to be “grateful” for the “scraps” they received from an inadequate, inflexible, and ostensibly uncaring system. Denise, in turn, recounted how she had to delay her son, who suffers from Down syndrome, in starting school due to his developmental issues but highlights that the early education system does not easily adapt to this: But there is always a worry, you know, like he was due to start preschool this year. I wanted to hold him back a year – the state doesn’t make that easy, as I had to go to this whole big rigmarole of applying to the state for exemption for the second year. And it comes with so much stress because then you have to get the letters from your therapists basically telling you how behind your child is…he has a big [medical] file; it’s that big, it’s just crazy…. (Denise)
A particularly sinister form of resource gatekeeping was experienced where families were, owing to their child’s behavioral challenges, “put down” (Teresa), “laughed at” (Bernadette) or judged as “bad parents” (Lilli) or a “hypochondriac mother” (Lorna). Such gaslighting by service providers exacerbated the already difficult limbo in which parents and their children subsisted. As a mother of an 18-year-old daughter with Asperger (now medically recognized as part of ASD), Lilli recounted how child protection services were alerted as they awaited a diagnosis for their child. This represented not only a failure of the health and social care systems but also an inappropriate engagement of governmental resources linked to the child welfare and protection service system: Child welfare stepped in, and we said the whole time that we wanted Asperger (a form of ASD) tests. We wanted Asperger expertise…. Then we got to the adolescent psychiatry…. We had thought that we were undergoing the Asperger tests during the 9 months because there had been all kinds of check-ups…. The doctor told me that we would never get the tests… because we are bad parents. (Lilli)
As reflected by Lilli’s poignant case, families were excluded from some systems (health and social care), they were almost involuntarily entrapped by other systems (child welfare system) and were prejudged as bad parents. There was nothing parents could do to remove this stigmatizing label or to negate the judgmental attitudes toward them. This resource gatekeeping further entrapped, stigmatized, and excluded them from the very service systems (e.g., healthcare and education) that they were so dependent on, sustaining their experiences of persistent liminality.
In certain instances where access to resources was possible, the actual resources delivered proved to be unsuitable, resulting in years of inappropriate treatments that were inadequate or potentially harmful for the child. We term this Resource Misalignment, namely, the inadequacy, inflexibility, and maladaptivity of resources necessary to meet actors’ ongoing complex needs. The disability support system servicing families of children with ASD was called out for their lack of professionalism as well as for their dereliction of duty of care to participants like Helena: This service system is impossible. It causes hatred and powerlessness. Can it really be like this? Families seek help anywhere they can, just anywhere. This group [children with ASD] is nobody’s concern. (Helena)
Resource misalignment was further reflected by Bernadette, who actively participated in and paid for multiple private service supports for her child with ASD, PDA, and ODD. Bernadette found that they had failed to help him: “he didn’t have the skills to collaborate...we couldn’t go anywhere.” As a result, she and her son were trapped at home. There was also a strong sense that institutions within the healthcare system operated in a disjointed way, with disconnects between private and public healthcare systems particularly evident. Teresa highlighted how a costly diagnosis obtained through the private healthcare system was not officially accepted by the public one. As a result, Teresa and her child had to endure a lengthy wait for a public health assessment: Everyone will tell you: you can pay privately; you can pay a fortune, but nobody will believe your private report. And they’ll kind of say, oh you’re being the panicky mother and you know anyone can pay for a diagnosis…. (Teresa)
In summary, Subsisting highlights the failings of multiple and clearly disjointed service systems exacerbated and sustained the ongoing precarity and entrapment that was collectively experienced within families. Feeling trapped in this enduring liminality and unable to plan for the future directly affected families’ sense of agency and control of their lives, resulting in negative well-being outcomes and further exacerbating their vulnerability.
Resisting
Resisting reflects families’ efforts to resist persistent liminality through negotiating and mobilizing resources (termed Resource Negotiation and Mobilization) and to cocreate and transform resources to address their needs (termed Proactive Cocreation). Specifically, families sought to mitigate the impact of persistent liminality through ongoing resource negotiation and mobilization, and, in doing so, actively coproduced resources and cocreated value to compensate for resource absence, inadequacy, and misalignment.
Proactive Cocreation—Resource Negotiation and Mobilization
Resisting and the associated strategies employed by participants represent active rather than passive responses to the challenges posed by persistent liminality. Participants recounted the numerous strategies that they employed to secure resources, including negotiating, lobbying, fighting, and advocating on behalf of their child with complex additional needs. Some described their battles with various systems as a “tooth and nail fight,” necessitating significant time and effort. Michael, a father of three sons with ASD, described being treated as an “exception” within a rigid, fragmented healthcare system: But the damn system should be easier, it’s not…you are an exception to the system rather than feeling that there is an open door where you go through and go how do I do this. It’s the tooth and nail fight…. (Michael)
In contrast, Paula described how she “play[s] the game” to ensure that she and her child can remain on good terms and work with the health experts and institutions who ultimately decided on resources allocation. She also however describes herself “as a fighter” who used her knowledge and skills to put a “case together” to lobby agencies “to do [their] jobs” and negotiate for additional services within the child protection and welfare system for her son “who deserves more”: It took me more than three years to bring Tusla [child and family agency] in, and I’m good to put my case together. I’m a fighter and I still had to do that for my son. And put ourselves out there, all our vulnerabilities on the table, but you will now do your jobs because he deserves more. (Paula)
Clearly, parents like Paula recognized the importance of leveraging their skills and employing system navigation strategies over extended periods to secure resources on behalf of their children: And they will wipe their hands of him when he turns 16 in terms of education. And the same will be said about that special school that he’s enrolled until he’s 18…but theoretically, they will not be obligated to help him when he turns 16. Which is why I’m pushing this now…he’s 14 and a half, if you get me. (Paula)
Paula describes how her son risked being excluded from his “special school” when he turns 16, which is why she was “pushing this now.” Such Proactive Cocreation was evident from the forward-looking approach to lobbying that she adopted, years in advance, to secure continued specialized education for her son until he reached 18. Ulla, in turn, revealed how she consciously concealed that her daughter had ASD when applying for a vocational school so as not to put her chances of being admitted in jeopardy: I did not want to disclose that she has ASD because then they start questioning whether this is the right place for her, that she should go [elsewhere], but then we had to tell that it’s not just panic attacks…then she got kicked out of there; they said we will put you on hold. (Ulla)
Hence, parents’ resisting may, as a last resort, even take counterproductive forms such as trying to hide the child’s additional needs. Ulla’s daughter, who since reaching adulthood (18), has tried accessing several different vocational schools but has failed to complete any training and continues to live at home with her parents.
Others too spoke of fighting for resources, “There’s a fight for every single thing you know” (Teresa), but also recognized the importance of prioritizing certain resources and services above others for their children. Teresa explained how she learnt to “pick my battles.” She prioritized fighting for her twin autistic boys to remain in a children’s day-care center and to secure the right for them to remain in the “mainstream” (general) education system as opposed to being segregated in special needs care facilities: Everything was about getting them into mainstream…. I pick my battles; that’s why I fought for the crèche…back then it was all about mainstream and that was my chance to keep my foot in the door with mainstream…. (Teresa)
Such negotiation by Teresa to secure and transform resources reflected Proactive Cocreation that were of immediate and longer-term value to her sons.
To cocreate value for their three sons with ASD, Michael described his strategy to “work the problem, work the problem” alongside his wife Lorna, who viewed herself as “an enabler,” constantly negotiating and mobilizing resources to meet the complex and diverse care needs of their sons. They collectively work like “a mini company” or a “project team” to secure resources for their children: …and it is just the grind of, well, “I can take this call here and if you do that drop, I will do this pick up” amongst all the other stuff. Then you have got all the form-filling and the fighting with the bureaucracy stuff on top of that as a stressor point…so I think we work very well as a project team…we are a very good team in terms of the task orienting but…it’s a case of we continually having to put ourselves back from being just almost like a mini company versus being a married couple. (Michael)
Others similarly became focused on “finding a solution” (Gary). Despite their best efforts to negotiate resources within the public healthcare system, in response to continued resource neglect/absence, exclusion, or misalignment, some parents felt compelled to pay for resources through private health providers, reflected by Sinead’s comment: “I can’t get the services that I need for my child, so I have to pay privately.” This, we argue, reflected resource mobilization, albeit outside the public healthcare service system, where parents actively resist persistent liminality by paying for necessary services.
Parents also mobilized resources through sharing information and doing research through becoming a member of self-help, parent network, and community support groups. Gary, who is widowed and is the sole carer for his son with ASD and two other children, describes how he is often the only male carer actively sharing and seeking support from those in similar caring situations. …and that’s why I go onto those [support] groups on Facebook because they know what it feels like…they know what it’s like when your child has a meltdown…and what you’re going through…. I get great comfort and support there…. And I’m often the only man…or the only one who posts or shares, it’s full of women, mammies…who are carers, not dads like me. (Gary)
Despite the persistent liminality, others felt impelled to advocate for those worse affected, reflected by participants like Bernadette: I need to talk more about this, advocate more, show where the flaws are in the system and show that support is needed for families that are struggling…. It needs to be said; it needs to be heard. (Bernadette)
Even if this did not necessarily grant them access to resources, parents felt that it gave them a mission, which somewhat alleviated their experiences of liminality. Some parents went a step further and volunteered (e.g., Margaret, Michael, and Lorna) or worked with ASD voluntary support services (e.g., Emma) and Down syndrome charities (e.g., Denise) to collectively advocate for their children’s needs with government organizations and policymakers.
In summary, Resisting permitted families to supplement, cocreate, and transform resources to create value for their children with additional needs. In this regard, it can be perceived as an active and positive response to the challenges of persistent liminality caused by resource misintegration and was to mitigate vulnerability.
Discussion
This study responds to calls for research on the nature and temporal duration of liminality (Söderlund and Borg 2018) and the importance of reducing barriers to resource integration for vulnerable consumers (Field et al. 2021) while also advancing the growing body of work investigating resource integration challenges (Varman et al. 2022). Our study makes three contributions to understanding how families experience and navigate resource (mis)integration and persistent liminality in service systems.
Our first contribution sheds light on vulnerable consumers’ experiences of persistent liminality. Our study reveals how parents experienced persistent liminality as an unpredictable, burdensome, and unending cycle of effort to meet their child’s complex resource needs and to secure their child’s future, with little assurance of positive outcomes for the child and other family members, where love, hope, and perseverance carried the families forward. Building on both traditional conceptualizations (Turner 1979; Van Gennep 1909/1960) and recent perspectives that have revealed permanent forms of liminality (Appau, Ozanne, and Klein 2020; Murphy and McDowell 2019; Nakata et al. 2019), we evidence how liminality evolves and persists within families who were unable to transition due to the complex needs of the child combined with resource challenges. Whereas recent research suggests that liminality may become permanent, that is, an enduring state of stasis without desired transition (Appau, Ozanne, and Klein 2020; Murphy and McDowell 2019; Nakata et al. 2019), our findings reveal persistent liminality as a dynamic, relational, and unending cycle of evolving and recursive transitioning, which is collectively experienced by interdependent actors in service systems. The relational aspect of liminality is revealed through actor interdependence, where persistent liminality is experienced by actors connected through social relations both within the family (i.e., the child with additional needs, parents and other family members) and in interactions within the service systems more broadly (i.e., family actors and service providers).
Persistent liminality not only endures for the life of the caregiver but may also continue into the next generation (i.e., siblings as future caregivers). This extends the traditional view on liminality as an individual, linear, static, and transitional process with demarcated starting and ending points (Van Gennep 1909/1960). It also builds on recent research on the liminal experiences of the individual patient (Nakata et al. 2019), the disabled child and parent dyad (Ryan and Runswick-Cole 2008) and the in/dividual divide (Appau, Ozanne, and Klein 2020). We bring forth how the complexity of care needs, coupled with the obscurity of resources, result in a dynamic liminality that persists and is re-activated as the children grow and their care needs evolve. Hence, neither the children nor their parents can transition from dependence to independence but rather experience continuously evolving persistent liminality. Trapped in persistent liminality, and unable to plan or control their lives or futures, these already vulnerable actors endure diminished agency which in turn inhibits their ability to integrate resources to cocreate value (Lusch and Vargo, 2014). Liminality, particularly if it persists, we argue, diminishes consumer agency (e.g., Sewell, 1992) and well-being and is thus a central area of concern in TSR.
Second, building on our previous contribution, we identify three dynamics of persistent liminality that form a cycle of transitioning: Precipitating, Subsisting, and Resisting. They constitute the continuous interplay between unpredictable conditions and complex care needs and resource integration challenges and opportunities. These dynamics shed light on the interrelationship between persistent liminality and resource integration in service systems, reflecting an evolution within the liminality experience (albeit one without an end). Through Precipitating, we reveal the precursors or triggers of persistent liminality that continuously recur within complex service systems. Precipitating, although characterized as dynamic, may also temporally, if briefly, entail a state of stability, which is quickly eroded when care needs evolve (e.g., due to children growing, new health issues arising or educational or social contexts changing). Subsisting reflects the everyday struggles of living with and enduring persistent liminality and entails families’ interactions with service systems. Resisting, in turn, is the families’ active resistance to persistent liminality, where actors proactively cocreate value. Our study importantly connects persistent liminality and its three dynamics to the interplay between condition and care complexities and resource integration challenges and thus foregrounds it as a wicked problem that is perpetual and recursive.
Whereas recent service research presents both positive (e.g., Sweeney et al. 2015) and negative perspectives on customer effort (e.g., Azzari et al. 2021), our study advances knowledge by revealing the nature and outcomes of resource integration efforts of vulnerable actors as they navigate the Precipitating, Subsisting, and Resisting dynamics of persistent liminality. Service providers seemed to collude with the under-resourcing of intersecting health and social care systems, knowing that parents will, due to love, struggle (Subsisting) and advocate (Resisting) to alleviate the gaps in care. In addition to accessing, adapting, or customizing existing resources (Akaka et al. 2012), vulnerable actors, as unpaid and unsupported social and healthcare workers, become the reluctant resources vital to keeping the system going over time. We therefore extend the work of Kelleher et al. (2020) that illustrates how caregivers as service orchestrators employ brokering strategies with health and social care providers. Our study highlights how service systems complicate brokering by hindering access to both public and private resources that are distributed by different actors.
Third, in line with TSR, we shed light on the resource constraints within maladaptive service systems, caused by systems’ failure to adequately supply and replenish the necessary resources, which accentuate and sustain resource misintegration and persistent liminality, and decrease the well-being of vulnerable consumers. By addressing calls to identify resource constraints in service systems for vulnerable consumers and their broader effects on society (Field et al. 2021), we add to the understanding of consumer vulnerability as a key concern of TSR. Our findings highlight the negative impact of resource constraints on vulnerability (Anderson et al. 2016). Moreover, they foreground maladaptive systems involving resource misintegration (Laud et al. 2019; Plé 2016) and significant system-wide deficiencies and challenges (Ostrom et al. 2021) that lead to persistent liminality and diminish consumer well-being. Our research focuses on vulnerable actors who can neither access the resources they need for themselves or for their families nor avail of the resources that are available, partially due to inadequate or inflexible service systems. Our study therefore counters earlier work on service systems that assumes their dynamic and self-adjusting nature (Vargo and Lusch 2016), suggesting that service systems transform and adapt in the face of adversity (Berry et al. 2020) and generate resources to meet actors’ resource requirements, which leads to value cocreation (Ng, Sweeney, and Plewa 2019). Our findings reveal instead that these assumptions may not apply within public service systems owing to service system misintegration coupled with actors’ complex and evolving (care) needs.
We identify two sets of emergent resource misintegration phenomena that underlie resource constraints. Resource Obscurity in service systems not only leads to negative value outcomes but also limits the very opportunity for resource integration. Resource integration may also fail due to Resource Gatekeeping and Resource Misalignment, which extends recent studies that have linked resource configuration challenges to the ongoing practice alignment and misalignment within service systems (Echeverri and Skålén 2021). Hence, the root cause seems to be an inability rather than unwillingness to adapt that is caused by resource constraints and systemic inflexibility inherent in (public) service systems owing to fixed resources or the lack of coordination. Due to the often intersecting and disjointed nature of healthcare, social and education service systems, actors face additional inabilities and failures in meeting their resource needs. This resonates with Azzari et al. (2021), who highlight how patients and their families, through responsibilization, must learn to job-craft to ensure well-being outcomes. Although such efforts involve hard work and perseverance, our study shows that they may or may not lead to mutually benefitting value cocreation, as SD logic would argue. We therefore contribute to service research by increasing understanding of the nature and impact of systemic and structural maladaptivity alongside the adaptive and self-adjusting capacity of actors.
On a broader level, our results deepen the understanding presented by Varman et al. (2022), who show how traditional service systems are conceptualized as market-based service systems comprising calculative and competitive market conventions, which may lead to negative outcomes. These in turn trigger actors to create alternative service systems based on civic conventions and regimes of agape or solidarity and love (Varman et al. 2022). This represents an additional onerous and problematic burden on parents who already struggle to care for their children with additional needs. It also accentuates the vulnerability of children whose parents lack the capacity to engage in proactive cocreation due to, for example, financial constraints, conflicting needs of family members or mental health issues. Such challenges relating to the adverse power dynamics facing actors have received scant attention in SD logic resource integration discourses. Our study therefore empirically and conceptually addresses the critique (Laamanen and Skålén 2015; Mustak and Plé 2020; Skålén et al. 2015) of SD logic’s overly optimistic and unproblematized perspective of resource integration. Notably, our findings lay blame with problematic system structures, particularly resource constraints, rather than intentional action by individual actors or power displays.
Together, these findings shed light on the heretofore under-researched relationship between resource integration and liminality experiences. Although resource (mis)integration does not directly cause persistent liminality, combined with family caregiving realities, it triggers, sustains, and alleviates persistent liminality. Hence, from a TSR perspective, resource availability, quality, and equality are important goals across public and private service systems in helping to alleviate liminality even if impossible to counter it fully. Our study shows that despite valiantly resisting through proactive cocreation and resource negotiation and mobilization, our parental actors as part of the family collective ultimately failed to exit persistent liminality. This was due to the enduring and evolving precarity of their children’s condition and complex care needs combined with ongoing resource integration challenges imposed by the complex service system. Even the most effortful and creative resisting strategies failed to resolve such significant and complex challenges.
Managerial Implications
This study unveils how parents and families of children with ongoing and complex additional needs experience service systems and reveals important shortcomings that necessitate focused managerial attention. Service providers should acknowledge that persistent liminality is an enduring, unpredictable, and burdensome cycle that diminishes vulnerable consumers’ well-being. While parents in our study often sensed the emerging challenges facing their child (Precipitating), their concerns were often dismissed or downplayed and the challenges in identifying appropriate resources (Resource Obscurity) represented a major obstacle. Indeed, specialist service providers themselves had difficulty recognizing the causes and conditions underlying the child’s cognitive or behavioral challenges which inhibited resource integration. A clear implication is the provision of education and training to those working with children (both medical staff but also educators, social workers, and support staff) to facilitate identification of the condition early on. Such programs could include creating easily memorizable acronyms to support diagnosing (alike FAST for stroke), videos portraying typical behaviors, and information on gender differences as girls are particularly adept at masking their social challenges and remain undiagnosed (Hull, Petrides, and Mandy 2020). As a further concern, non-white ASD people may be even more vulnerable to issues such as police violence and institutional racism as their actions may be potentially misconstrued as anti-social behavior and result in mistreatment (Giwa Onaiwu 2020). This highlights the need to train police, firefighters, security officers, and other staff who are responsible for public safety.
Another implication for managers stems from the high resource demands that complex conditions bring, coupled with the isolation of parents as caregivers. Reflected in Subsisting and Resisting, parents exerted significant efforts to access resources, secure a future for their child and lead a somewhat normal family life. It is therefore imperative that service providers are equipped with specialized skills, adequate time, and genuine empathy to proactively work with the parents to design and implement appropriate child-specific care and developmental plans. To alleviate parents’ feelings of isolation, it would be useful to offer dedicated supports such as face-to-face peer network groups, online discussion forums and websites with easily digestible content for the extended family, who would be better equipped to support the child, parents, and siblings. This would broaden the available resources, and perhaps improve well-being through stronger relational ties.
Our findings also revealed that even though an omnichannel experience may be available to some, it is still not the case for all. Managers should therefore prioritize the provision of an integrated and holistic service involving both single and central touchpoints that effectively manage the responsibility for all actors and the servicing of their needs. Managers could also draw on the tools provided by service design to craft better integrated service pathways and to identify bottlenecks that decrease consumer well-being. This would facilitate the much-needed orchestration of services across interconnected systems.
Moreover, our study foregrounds the ongoing, severe resource integration challenges faced by vulnerable consumers and highlights their interrelationship to liminality. In cases such as this where needs are complex and evolving, services need to be customized and reassessed on a regular basis and adapted over time. As this is likely to be labor-intensive, time-consuming, and costly, navigating budget restraints and managing with insufficient resources is a universal challenge that must be appropriately and effectively resolved. Although governments could be ultimately blamed for the bureaucracy and under-resourcing of public healthcare systems, it is often private healthcare providers which profit from servicing otherwise unmet needs, ultimately masking and sustaining the failures in the public service system. We therefore argue for an appropriate alternative to the discriminatory two-tiered system emanating from the dependence on private providers who profit from resource gaps in the public system.
As the global staffing (WHO 2023) and budget crisis in care has shown, resources are scarce and not likely to be abundant in the foreseeable future. One possible solution is shifting emphasis from short to long-term impact to influence the use of scarce resources. While costly in the short-run, were resources allocated to early diagnosis and interventions to support children and families, they might lead to considerable savings in the long-run, helping to reduce developmental delays and mitigating against exclusion from education and work and mental health issues. Investigating the work opportunities and income potential for both parents and, where possible, children might also significantly impact economically. Supporting parents and children to avail of and continue in appropriate and sustainable work pays off financially. Hence, an important policy implication is to arrange longitudinal interventions around life and work opportunities for parent and children and measure their well-being and financial outcomes over time.
We believe that the managerial relevance of our findings by far extends the studied context and is likely to apply to similar cases involving consumer vulnerability where solutions are challenging and outcomes unpredictable. Examples entail children’s mental health, criminal behavior, and drug abuse affect the lives of both the children and their loved ones over the long term. Extending beyond the private versus public healthcare context, the challenges around resource provision and integration are even more acute in service systems where power disparities exist. These may include education, banking, pensions, and insurance as evident in countries where private systems are often perceived as superior and accessible only to those who can afford to pay. Other power disparities are evident within base of the pyramid markets or service systems that are overstretched by actor resource demands and in times of worldwide shortages owing to famine, environmental destruction through natural disasters, trade embargos, or wars. This is particularly prevalent in the case of non-renewable natural resources or when emergency accommodation demands exceed supply for those fleeing war and disasters.
Finally, in terms of public policy implications, it is important to challenge the mindset among some stakeholders and within society more broadly that children with these conditions will no longer need care or support once they reach adulthood. Given the often life-long nature and impact of these conditions, long-term strategic planning and coordination is required by government bodies, state-run service institutions, private service providers, and service orchestrators to assist families to plan for the longer-term welfare of their children. This should involve the coordination of various service systems (including health and social care, education, taxation, and welfare systems) to assist caregivers and families in planning for the education, development and work opportunities of children as well as their ongoing healthcare/social care needs over the life-long care journey. Although we highlight the criticality of providing resources to family caregivers, it is vitally important that they do not become the buttress or stop gap for resources and supports that should be serviced from within the healthcare system itself. It is therefore important that “family caregivers are seen not just as resources but also as partners who need information, training, and supportive services” (Berry et al. 2022, p. 13).
Avenues for Further Research
An important avenue for research is the nature and impact of persistent liminality in service systems in general and particularly those which are complex. In contemporary societies, transitions may take on a more enduring nature, which emphasizes the relevance and pervasiveness of persistent liminality. Examples include gig workers, expats or involuntary “career temps” (Garsten 1999) or those trapped in zero-hours contracts with inadequate financial or economic resources to progress, that is, buy a house or start a family. There are also other contemporary settings where persistent liminality might help to explain the experiences of individuals, such as NEETs (young people who are neither employed nor at work or training), those waiting to adopt or to undergo infertility treatments or those burdened by problem debt or costly loan restructuring.
Future research might also fruitfully examine how resource obscurity impacts value cocreation to inform policy on how to improve resource supply and allocation particularly in service systems, particularly those more complex, to meet actors’ ongoing and evolving needs over time. This is important not only during times of ongoing resource scarcity, as in the context studied, but also following abrupt disruptions to service systems, such as those caused by war or natural disasters, which may be enduring. Vulnerable consumers, including the poor, the undocumented or those who are members of ethnic, gender and language minorities, may be particularly affected in these situations. A fruitful avenue of research would be to explore agency and the associated power dynamics and disparities between actors and service providers/institutions and to compare resource access (in)adequacy and alignment across systems and countries. This would expose large discrepancies between countries/systems in relation to access and quality of private and public healthcare, social care, and education. It would also highlight systems that provide universal healthcare access for all, regardless of means. Furthermore, such research would facilitate the exploration of experiences of resource (in)adequacy amongst and within populations, including using quality of life and well-being measures. The unfair allocation of resources in unsustainable service systems, such as fast fashion, single-use plastic, and excessive air travel, along with systems where resources are in short supply, such as food deserts in major urban centers may also be a future focus. Somewhat surprisingly, the study of misalignment in relation to institutions and institutional arrangements and the resulting negative impact on value cocreation have received scant attention from service scholars to date. This research is even more timely given that numerous complex service systems across nations remain under-resourced and ineffectively managed, reflected by those (education, healthcare, and social care) explored in this study.
Supplemental Material
Supplemental Material - It Never Ends: Vulnerable Consumers’ Experiences of Persistent Liminality and Resource (Mis)Integration
Supplemental Material for It Never Ends: Vulnerable Consumers’ Experiences of Persistent Liminality and Resource (Mis)Integration by Deirdre O’Loughlin, Johanna Gummerus, and Carol Kelleher in Journal of Service Research
Supplemental Material
Supplemental Material - It Never Ends: Vulnerable Consumers’ Experiences of Persistent Liminality and Resource (Mis)Integration
Supplemental Material for It Never Ends: Vulnerable Consumers’ Experiences of Persistent Liminality and Resource (Mis)Integration by Deirdre O’Loughlin, Johanna Gummerus, and Carol Kelleher in Journal of Service Research
Supplemental Material
Supplemental Material - It Never Ends: Vulnerable Consumers’ Experiences of Persistent Liminality and Resource (Mis)Integration
Supplemental Material for It Never Ends: Vulnerable Consumers’ Experiences of Persistent Liminality and Resource (Mis)Integration by Deirdre O’Loughlin, Johanna Gummerus, and Carol Kelleher in Journal of Service Research
Footnotes
Acknowledgments
The authors would like to acknowledge the participants who shared their stories and the organizations representing ASD and Down syndrome in Ireland and Finland which supported the research study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by CERS, Centre for Relationship Marketing and Service Management, Hanken School of Economics, Finland.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.