
Abstract
In managing a chronic illness, customers have the opportunity to play an active role in their healthcare—by cocreating value. For example, customers can adhere to medical advice, seek out information about their condition(s), manage their diet, and interact with family and friends. Moreover, across an extended treatment period, customers may dynamically adjust their level of value cocreation. In this study, we examine 307 healthcare customers receiving treatment for cancer, with 12 value cocreation activities tracked longitudinally over 4 survey waves. Using a hidden Markov model, we reveal three latent states of customer value cocreation: low, moderate, and high. We then determine which of the 12 value cocreation activities are most strongly associated with transitions among cocreation states. Finally, we show that transitioning to a cocreation state with a higher level of cocreation activity positively correlates with customer and marketing outcomes, including customer quality of life and satisfaction. Our findings show that an increase in six cocreation activities—actively sharing information, compliance with medical requirements, interacting with staff, maintaining a healthy diet, interacting with others who receive treatment, and maintaining a good physical appearance—yields positive gains for both customer and marketing outcomes. In contrast, an increase in emotion regulation negatively affects customer outcomes.
Keywords
Marketing can contribute substantially to the understanding and management of healthcare service experiences (Anderson et al. 2013; Berry and Bendapudi 2007; Chen et al. 2020). Chronic diseases such as cancer, diabetes, and heart disease are global challenges. As the leading causes of death and disability in the United States (CDC 2019) as well as other countries, they pose an enormous economic burden (Okediji, Salako, and Fatiregun 2017). For example, six in ten U.S. adults have a chronic disease, and four in ten have two or more chronic diseases (CDC 2019). It is estimated that by 2023 chronic disease will cost the U.S. economy more than $4.2 trillion annually in treatment expenditures and lost economic output (Bodenheimer, Chan, and Bennett 2009). Not surprisingly, reducing the systemwide burden of chronic disease is a key concern for healthcare organizations, policy makers, and governments. One-way healthcare providers can begin to reduce that burden is to facilitate the healthcare customer’s role in actively managing their own illness (Ahn et al. 2015). Indeed, customer proactivity for well-being in areas such as healthcare, financial, and education services is a top research priority for service marketing scholars (Ostrom et al. 2021).
Healthcare customers can contribute to their own health status by undertaking activities that aim to cocreate value with a focal healthcare service provider (Prahalad and Ramaswamy 2004). They can also draw on resources that extend well beyond the focal firm to cocreate that value (Arnould, Price, and Malshe 2006). These include activities undertaken with other healthcare service providers, such as complementary therapists; activities with private sources, such as family, friends, and other customers; and self-generated activities like emotion regulation (McColl-Kennedy et al. 2012; Sweeney, Danaher, and McColl-Kennedy 2015). The benefits of engaging customers in their own healthcare, and by extension value cocreation, 1 are potentially better health and well-being (Ahn et al. 2015) and higher levels of customer satisfaction (Vega-Vazquez, Revilla-Camacho, and Cossio-Silva 2013). However, healthcare customers may differ in their level of access, ability, and willingness to cocreate value (Laud et al. 2019; Stokburger-Sauer et al. 2016). Consequently, value cocreation may not always be appropriate for enhancing well-being.
Although marketing can play a fundamental role in improving customers’ well-being (Anderson and Ostrom 2015; Berry and Bendapudi 2007; Chen et al. 2020; Dagger and Sweeney 2006), the challenge for managers is motivating customers to undertake activities associated with value cocreation. That task is difficult, as health-related habits and routines can be firmly entrenched (Dellande, Gilly, and Graham 2004), and value cocreation generally requires substantial customer effort over a long period of time (Sweeney, Danaher, and McColl-Kennedy 2015). While previous research has investigated the activities customers engage in to cocreate value in healthcare (e.g., McColl-Kennedy et al. 2012; Sweeney, Danaher, and McColl-Kennedy 2015), three critical questions about the dynamics of customer value cocreation remain unanswered.
First, to what extent do value cocreation activities derive from customers’ underlying predisposition and motivation to cocreate—that is, their latent value cocreation state? We expect that healthcare customers vary in the range of cocreation activities they adopt and the intensity with which they undertake them—some might be high cocreators, while others are low cocreators. Second, is movement among latent value cocreation states fluid? For example, can customers migrate from a lower, less desirable state to a higher, more desirable one? If customers do transition between states, it is critical to identify (a) which value cocreation activities positively influence upward state transitions (or stabilize customers in a desirable state) and (b) which activities must be managed to avoid a downward transition in cocreation state. Indeed, partaking in some cocreation activities is not guaranteed to positively influence state transitions for all customers. Third, what effect do value cocreation state transitions have on important marketing (e.g., customer satisfaction) and customer (e.g., well-being) outcomes over time? Healthcare providers can enhance these outcomes by ensuring that a customer undertakes the right value cocreation activities at the right point in time.
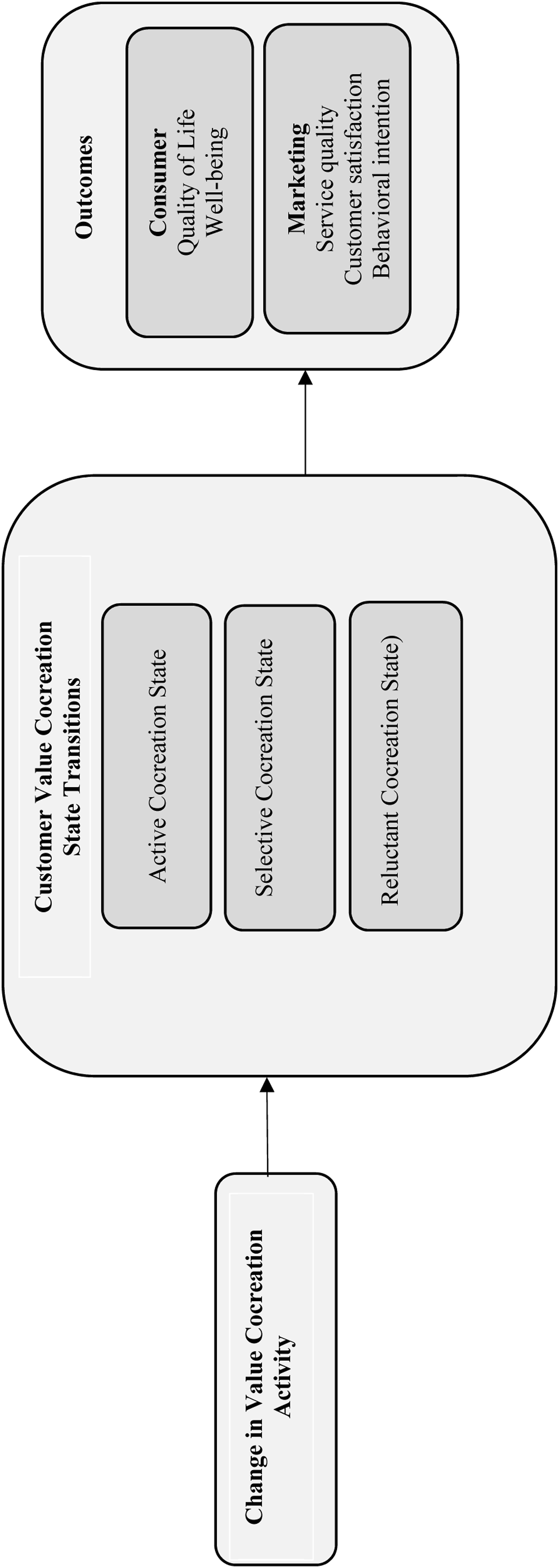
In addressing these questions, our study has three aims that we address with a novel empirical approach: (1) identify and characterize latent states of customer value cocreation, using a hidden Markov model; (2) investigate customer transitions among value cocreation states—and identify the activities associated with those transitions, using a multinomial logit model; and (3) examine the correlation between latent state transitions and changes in customer satisfaction, perceptions of service quality, behavioral intentions (e.g., treatment continuation), quality of life, and well-being (see Figure 1). To achieve our study aims, we undertake a longitudinal examination of healthcare experiences of patients with cancer, from their initial diagnosis through 12 months of care, across 4 survey waves. Customer value cocreation states, transitions, and key outcomes.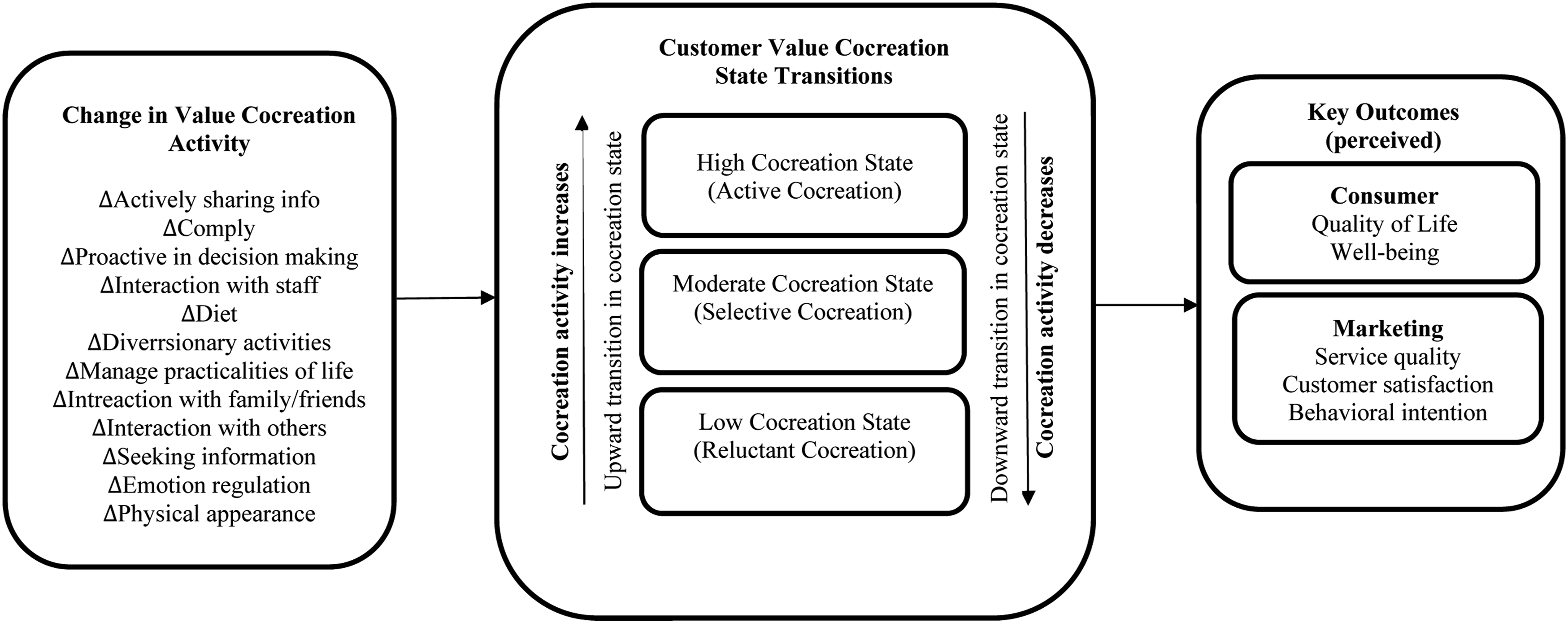
Using our hidden Markov model, we reveal three latent value cocreation states, corresponding to low, moderate, and high cocreation activity. Customers in the high state actively engage in a wide range of activities very intensively; the opposite occurs for customers in the low state, who are reluctant cocreators. Those in the moderate state selectively choose some activities and engage in them intensively. Customers in these states also vary in their psychological characteristics (e.g., self-efficacy, optimism, and locus of control), demographic characteristics (e.g., age and gender), and health status (e.g., comorbidity). We further show that changes in some cocreation activities are associated with an upward (positive), stabilizing, or downward (negative) transition in value cocreation states. Finally, we demonstrate that transitioning to a state with higher levels of cocreation activity positively correlates with increases in customer and marketing outcomes, such as customer satisfaction and well-being.
Customer Value Cocreation Theory
Value cocreation is an important concept not only in service research (Ostrom et al. 2015), but also in consumer behavior (e.g., Arnould, Price, and Malshe 2006) and, more broadly, in marketing (e.g., Epp and Price 2008). Value cocreation is central to service–dominant logic, which holds that value derives from an active process of integrating personal resources (e.g., knowledge, skills, and abilities) with resources of other actors in a service network (McColl-Kennedy et al. 2012; Vargo and Lusch 2016). Value cocreation highlights the benefits that can be obtained when customers, service providers, and parties beyond the customer–firm dyad, work to jointly cocreate value and outcomes. Customers can cocreate value with the focal firm and also with private sources, including the customer’s own personal knowledge and skillsets, and with social structures such as the self, family, peers, and other customers (Epp and Price 2008). Value also can be cocreated with market-facing sources, such as other firms or entities (e.g., complementary therapists), or even more broadly with community sources (Arnould et al. 2006).
Researchers who have studied service ecosystems and complex value networks with multiple actors (e.g., Beirao, Patricio, and Fisk 2017; Pinho et al. 2014) have conceptualized value cocreation from an actor perspective, using a combination of generic factors (such as resource access, resource-sharing, and resource recombination) that yield value cocreation outcomes. These studies largely take an organizational perspective. In the context of health, for example, studies have focused on better healthcare provision, cost and time savings, and healthcare decision-support management (Beirao, Patricio, and Fisk 2017; Pinho et al. 2014). While McColl-Kennedy et al. (2012) qualitatively investigated the potential effect of combinations of value cocreation activities through their concept of value cocreation styles, no research has empirically addressed the effects of integrating a range of value cocreation activities over time and from the perspective of a specific actor (such as the customer).
Furthermore, no research has examined the existence of latent customer value cocreation states or addressed the effect of changes in value cocreation activities on transitions among customer value cocreation states. Previous research (e.g., Sweeney et al., 2015) has treated cocreation as a static concept, but we posit that the extent to which customers undertake value cocreation activities evolves over time. In the early stages of treatment, customers may engage in a different “set” of activities, and to varying extents, than in later stages of treatment. Given that value cocreation activities are likely to dynamically affect outcomes such as customer satisfaction and well-being, we aim to offer the first insights into the effect of cocreation state transitions on business and customer outcomes. We do so through the application of an innovative empirical approach—applying a hidden Markov model and a multinomial logit model to study value cocreation state transitions. Finally, it is rare for studies to explicitly consider the customer’s role in value cocreation beyond the service setting itself, as we seek to do.
We adopt the definition that customer value cocreation is “the benefit realized from integration of resources through activities and interactions with collaborators in the customer’s service network” (McColl-Kennedy et al. 2012, p. 375). As this network can include the focal firm, as well as other market-facing and private sources, we offer the example of a healthcare customer diagnosed with cancer who attends a clinic to receive chemotherapy or radiation but who may also use the services of other providers such as a physical therapist or a nutritionist. In addition, such a customer may engage with family and friends, in diversionary activities, and in attending support groups (McColl-Kennedy et al. 2012; Sweeney, Danaher, and McColl-Kennedy 2015). In this way, we view healthcare customers as performing a range of value cocreation activities that extend well beyond interactions with the focal service provider but that still revolve around the customer’s cancer journey.
Drawing on the work of Sweeney, Danaher, and McColl-Kennedy (2015), who have developed a scale to assess the customer value cocreation activities that healthcare customers undertake in the context of chronic illness (e.g., cancer, heart disease, and diabetes), we examine 12 customer value cocreation activities relevant to the cancer service context of our study: actively sharing information, adherence to medical requirements, proactive involvement in decision-making, interaction with clinic staff, maintaining a healthy diet, diversionary activities, managing the practicalities of life, relationships with family and friends, interacting with others receiving treatment, seeking information, emotion regulation, and managing physical appearance. These activities, listed on the left side of Figure 1, include those undertaken with the focal provider and with other public and private sources.
Customer Value Cocreation Latent States
Although McColl-Kennedy et al. (2012) provide preliminary evidence that cancer patients cocreate value in different ways, we know little about the dynamic aspects of value cocreation across time. Some degree of cocreation activity in service delivery is inevitable, but customers have considerable discretion about the range of cocreation activities they may decide to adopt and the extent to which they engage in the activities (Claycomb, Lengnick-Hall, and Inks 2001). Early evidence appears in the involvement and customer participation literatures, which show that customers vary in their level of service/product participation and/or involvement (Cermak, File, and Prince 1994). More recently, Sweeney, Danaher, and McColl-Kennedy (2015) have shown that customer value cocreation takes place within the customer’s service network, moving beyond firm–customer service interactions, and that customers differ in the degree of effort they put into value cocreation.
Underpinning customers’ varying levels of cocreation activity (high, moderate, and low—as discussed earlier) is the concept of a latent state, an unobserved psychological disposition that elicits behavior (Netzer et al. 2017). In our study, being in a particular latent state depends on the range of cocreation activities they adopt and the intensity with which they undertake them, and also on a customer’s psychological traits, health status, and anticipation of future outcomes. For example, a patient with cancer who does not believe they can influence their health outcomes, and who has a poor medical prognosis, is likely to be in a state of low observed cocreation activity. Conversely, a patient who believes their behavior can influence their health outcomes, and who is advised that their prognosis is good, is more likely to be in a state of high observed cocreation activity:
Customers vary in the breadth of value cocreation activities they adopt, and the degree to which they undertake them, such that customers will range from low to high in their cocreation activity. The importance of customer value cocreation in healthcare is well recognized (Beirao, Patricio, and Fisk 2017; Sweeney, Danaher, and McColl-Kennedy 2015; Zhao, Wang, and Fan 2015). However, the fact that value cocreation evolves dynamically has largely been overlooked, even though prior research in other areas supports the notion of state transitions. For example, in the marketing literature, Zhang et al. (2016) find that customers transition through different relationship states and can migrate to a higher-performing, more desirable relationship state. Danaher, Sajtos, and Danaher (2020) further show that loyalty-program members transition between latent loyalty states, and that different reward categories and marketing effort are associated with these transitions. In the medical and economics literatures, Adena and Myck (2014) show that low wealth increases the likelihood that a healthy person will transition from better to poorer health, and Morefield et al. (2012) show that occupation influences health transitions, with blue-collar employment increasing the probability of transitioning from very good to bad health. Leveraging these studies, we predict that healthcare customers can and do transition among value cocreation states, and that activities associated with these transitions are state-dependent. That is, we expect that customer value cocreation activities differentially affect state transitions, such that some activities drive a positive upward transition between states, some stabilize customers in a particular state (good if they are in a desirable cocreation state, bad if they are in a less desirable state), and other activities cause a negative, downward transition (from a more desirable to a less desirable state).
Changes in customer value cocreation activities differentially influence transitions among low, moderate, and high customer value cocreation states.
Benefits of Customer Value Cocreation
An important benefit of customers’ ability to transition among cocreation states is that the states may be associated with important marketing and customer outcomes that relate to the care aspects of healthcare (but not necessarily, of course, to disease prognosis). Thus, we examine the effect of customer value cocreation transitions on perceptions of customer satisfaction, service quality, behavioral intentions (e.g., treatment adherence), quality of life, and well-being.
The literature reveals that customers who actively participate in service interactions are more satisfied with the service experience (Dellande et al. 2004; Gallan et al. 2013) and that the more effort customers put into value cocreation, the greater their level of satisfaction with the service (Sweeney, Danaher, and McColl-Kennedy 2015). Claycomb et al. (2001) surmise that customers who actively participate in cocreation are more likely to have their needs met, thereby increasing their likelihood of satisfaction. Similarly, and in terms of perceived service quality, research indicates that as customer participation increases, there is a corresponding increase in perceptions of service quality (Wang, Wang, and Zhao 2007). Bowen (1986) explains that as customers increase their level of involvement with a service provider, the provider gains the chance to shape customers’ perceptions and judgments about the firm. Finally, evidence suggests that increased customer participation is associated with positive post-purchase behavioral intentions (Cermak, File, and Prince 1994) and that the amount of effort customers put into value cocreation positively influences their behavioral intentions (Sweeney, Danaher, and McColl-Kennedy 2015).
Transitioning to a higher customer value cocreation state is positively associated with increased customer satisfaction, service quality perceptions, and behavioral intentions. In addition to these service marketing outcomes, managers can positively influence customers’ quality of life and well-being (Anderson et al. 2013; Sirgy and Lee 1996). We define quality of life as a broad-ranging concept affected by the individual’s physical health, psychological state, level of independence, social relationships, and their relationships to salient features of their environment (WHO 1995), and well-being as overall satisfaction and happiness with one’s life (Diener, Tamir, and Scollon 2006). These constructs, often used interchangeably in the literature, are clearly subjective, individual, and experimental (Upton and Upton 2015). Given that a basic tenet of healthcare is to maximize well-being (Sirgy and Lee 1996), we believe that customer value cocreation, viewed as the enhancement of customer benefit from the integration of resources, has the potential to positively shape customers’ lives (Finsterwalder et al. 2017). When customers are active cocreators of their own healthcare, they can influence their well-being outcomes:
Transitioning to a higher customer value cocreation state is positively associated with improved perceptions of well-being and quality of life.
Research Method
Chronic diseases are ongoing, generally incurable illnesses. As healthcare services for chronic disease are generally high touch, involving a high level of personal contact with customers, they provide a rich context to investigate the effect of value cocreation activities on state transitions. A chronic disease that has wide ranging implications for the health system is cancer, which we study for two reasons. First, cancer services unfold within an ecosystem that involves multiple parties and service encounters over time, thus enabling researchers to investigate the activities associated with state transitions. Second, customers need to undertake a range of activities to promote health and build psychological reserve—they interact with healthcare providers and systems, adhere to treatment protocols, and monitor and manage their illness (Wagner, Austin, and Korff 1996).
Data
Data were collected from customers of two private outpatient cancer clinics in Australia (all patients had private health insurance). Ethics approval was gained from the clinics, hospitals, and primary university involved in the study. Participants were assured that their involvement (or not) in the study would not compromise their medical care. At the conclusion of data collection all survey responses were anonymized. As cancer services and experiences unfold across time, we use a longitudinal survey design that obtains data from a panel of cancer patients over time. As the bulk of cancer treatment happens within a 12-month timeframe (e.g., diagnosis, chemotherapy, and radiation) we monitored customer value cocreation activities and outcomes at four time points—baseline (initial diagnosis), 3 months, 6 months, and 12 months post diagnosis.
These four time points were determined based on the goals of our study, the cocreation activities, and in consultation with oncologists, nurses, clinic management, and patients themselves. The data collection process involved a research nurse recruiting patients into the study. The research nurse worked with the clinic administration team to identify new patients ahead of their first appointment at the clinic. When these patients arrived at the clinic for their first appointment the nurse invited them to participate in the study. Questionnaires were then given to patients to complete at the clinic. Subsequent surveys were mailed to participants at 3, 6, and 12 months post the first survey period with a reply-paid envelope for return.
In total, 307 newly diagnosed patients were recruited into the study. Some 301 completed the survey at T1.
2
At T2, 190 respondents completed the survey, 174 at T3, and 153 at T4. At each time point a participant’s objective health data was collected, through the clinic. This is important because it allows us to control for health status in our analysis. Over the period of our study not all customers completed each survey wave. For instance, some customers completed only the initial survey at T1, or surveys at T1 and T2. One reason for this attrition is that 54 patients passed away at some point during the 12 months and so dropped out of our longitudinal study,
3
while others dropped out for reasons that are unknown to us, but not due to death. In addition, some respondents completed just a subset of the four possible surveys. For example, they may have completed T1, missed T2 but completed T3. We avoid limiting our study to just those completing surveys at each time point (T1, T2, T3, and T4) because a respondent completing all four waves is likely to be different to someone who drops out along the way, potentially biasing our model results. Therefore, we include all respondents, even those who passed away mid-study, or did not complete all four survey waves for some other reason(s). This results in
Measures
All value cocreation measures use 7-point Likert scales, where 1 represents “strongly disagree” and 7 represents “strongly agree.” Online Appendix A lists the scale items for the variables in our study, and reports the psychometric properties of these scales (using AMOSv25). All measurement models had good fit to the data with adequate levels of construct reliability, average variance extracted, and discriminant validity (Fornell and Larcker 1981).
As can be seen in Online Appendix A, healthcare customer value cocreation is measured using the 12 activities listed previously, with a scale adapted from Sweeney, Danaher, and McColl-Kennedy (2015). As this scale was developed in the context of chronic illness (diabetes, heart disease, and cancer) it is highly relevant to our study. For outcomes, quality of life is measured by a single item specifying a short time window (EORTC 2015), and well-being with a scale adapted from Fox (2004). The service marketing outcomes of service quality, customer satisfaction (Cronin, Brady, and Hult 2000) and behavioral intentions (Zeithaml, Berry, and Parasuraman 1996), and the individual traits of locus of control (Wallston, Stein, and Smith’s 1994), self-efficacy (Sherer et al. 1982), and optimism (Scheier and Carver 1985) are adapted from well-established scales.
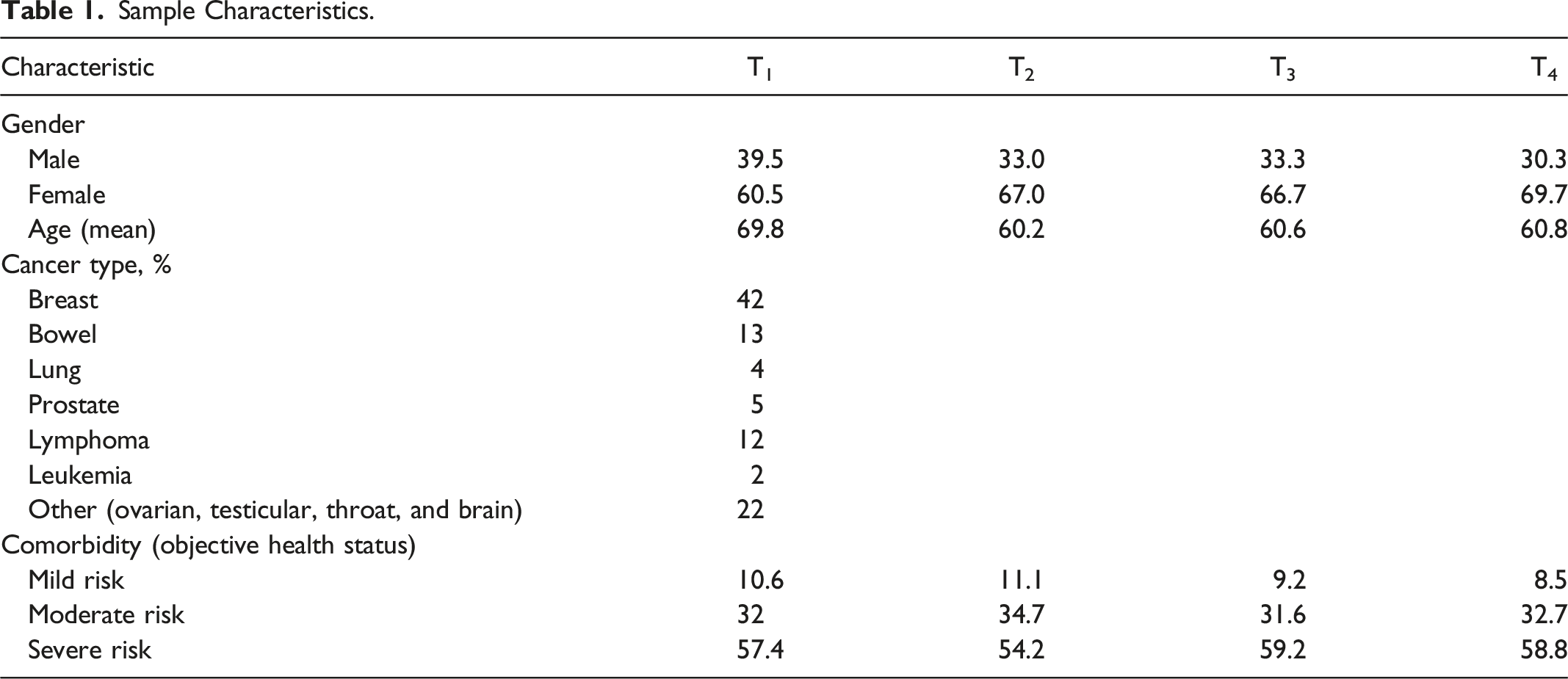
Sample Characteristics.
Given the mortality rate among the population, we construct variables designed to handle attrition, which is especially critical for studies in the context of chronic disease. As noted earlier, one reason for dropping out of the study is the death of a healthcare customer, so we have a binary variable to capture this event. We also have a number of instances where a customer did not complete all four waves of the study (and they did not pass away during the study). We therefore also construct a binary variable to indicate if a customer is a “non-completer.” 4 Finally, we have dummy variables to accommodate any effects due to the survey waves, with the baseline dummy being the first wave.
Model
The focus of our study is to examine the dynamic value cocreation activity that a healthcare customer engages in as they proceed through their lengthy treatment. While dynamic customer behavior can be modeled as a state-dependent process (Seetharaman 2004), such models do not capture two key elements we wish to investigate, namely, latent cocreation states and transitions (upward and downward) between these states. Given these requirements, we use a hidden Markov model (HMM) which allows researchers to infer latent states from observed cocreation behaviors and then study transitions between these states (Luo and Kumar 2013; Zhang et al. 2016). HMMs are particularly suited to longitudinal studies, where they have been used for self-assessed health status (e.g., Reus-Pons et al. 2018) and customer relationship states (e.g., Dwyer, Schurr, and Oh 1987; Luo and Kumar 2013; Zhang et al. 2016). Our study is the first to apply a HMM to reveal latent cocreation states for healthcare customers, and how they transition between these states over time.
As well as identifying the number and prevalence of latent states, HMMs estimate the “stickiness” or transience of each state via a transition matrix, which gives the probability of a customer remaining in the current state or moving to another state at each time period (Zhang et al. 2016). Hence, HMMs allow for the possibility of no transition, which is conceptually and practically relevant in our case because cocreation activities are often stable. Another valuable feature of a HMM is the ability to gauge the influence of covariates such as controls for attrition and noncompletion on transitions between latent states.
Suppose that at each survey period 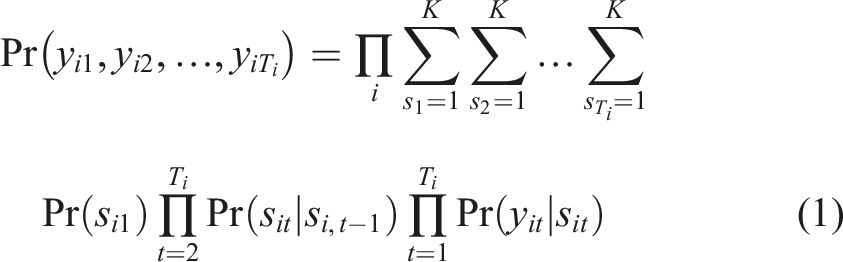
The product
We now generalize equation (1) to accommodate covariates that influence the initial state and the transition probabilities between states. 
The initial state variable
Results
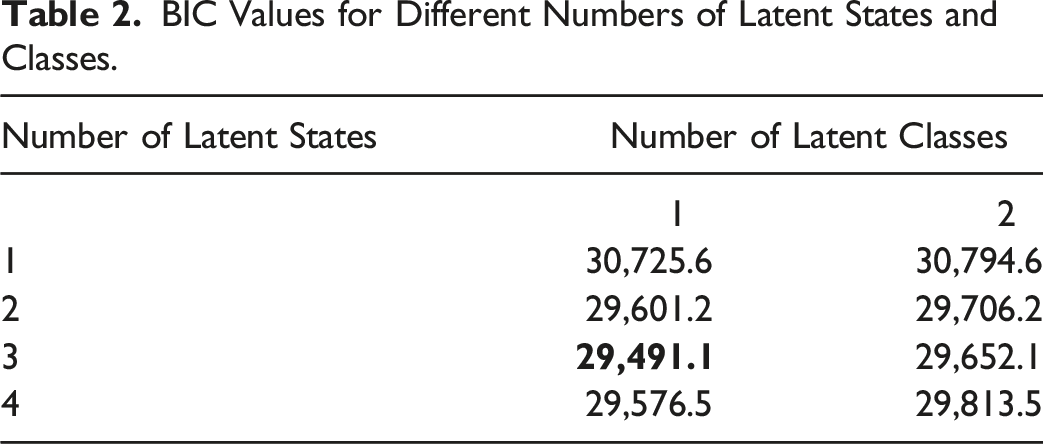
BIC Values for Different Numbers of Latent States and Classes.
Profiling the States
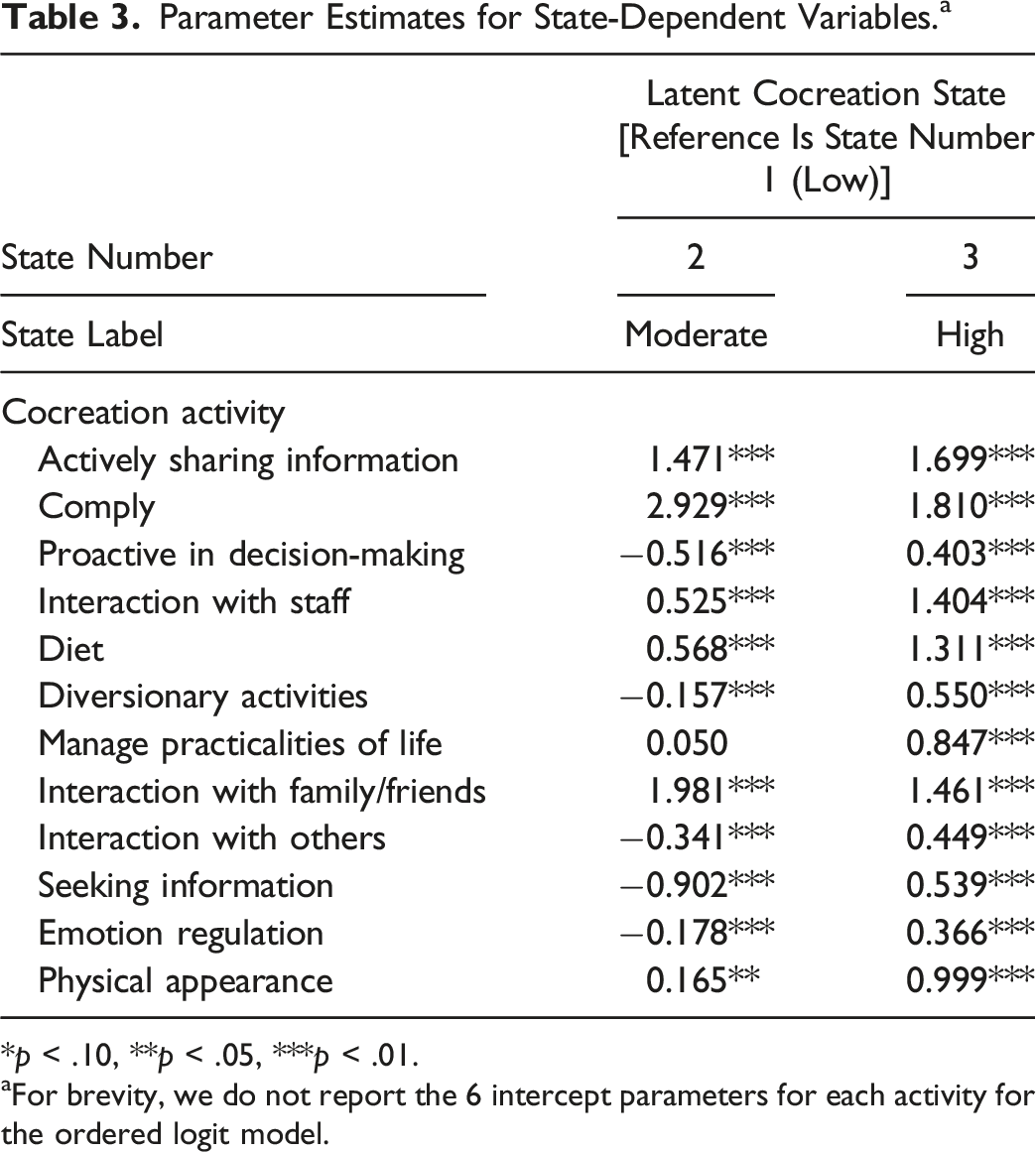
Parameter Estimates for State-Dependent Variables. a
*p < .10, **p < .05, ***p < .01.
aFor brevity, we do not report the 6 intercept parameters for each activity for the ordered logit model.
Looking across all the cocreation activities, we see that when customers are in state 2 they actively share information, comply with medical requirements, interact with staff, maintain a healthy diet, interact with friends and family, and put effort into maintaining their physical appearance. However, as evidenced by significant negative coefficients, those in state 2 engage significantly less than those in state 1 for a number of cocreation activities, such as being proactive in decision-making, undertaking diversionary activities, interacting with others, seeking information and emotion regulation, which are more effortful activities based on Sweeney, Danaher, and McColl-Kennedy’s (2015) scale. That is, customers in state 2 are very judicious in their uptake of the range of possible cocreation activities, embracing less effortful activities and selectively avoiding more effortful activities.
State 3 is straightforward because customers in this state have significant positive coefficients for all 12 cocreation activities. This means they engage in all cocreation activities consistently more than customers in state 1, and also more than those in state 2, apart from the activities of compliance and interacting with family and friends. Given these comparisons of cocreation activities across the states, we label cocreation states 1 through 3, respectively, as low (evidenced by reluctance to cocreate), moderate (evidenced by engaging in selective cocreation activities), and high (evidenced by highly active cocreation). Our findings provide support for H1 that customers vary in the breadth of cocreation activities they adopt and the degree to which they undertake them such that some customers will be high cocreators, some will be moderate cocreators, and others will be low cocreators. That is, there is more than one cocreation state.
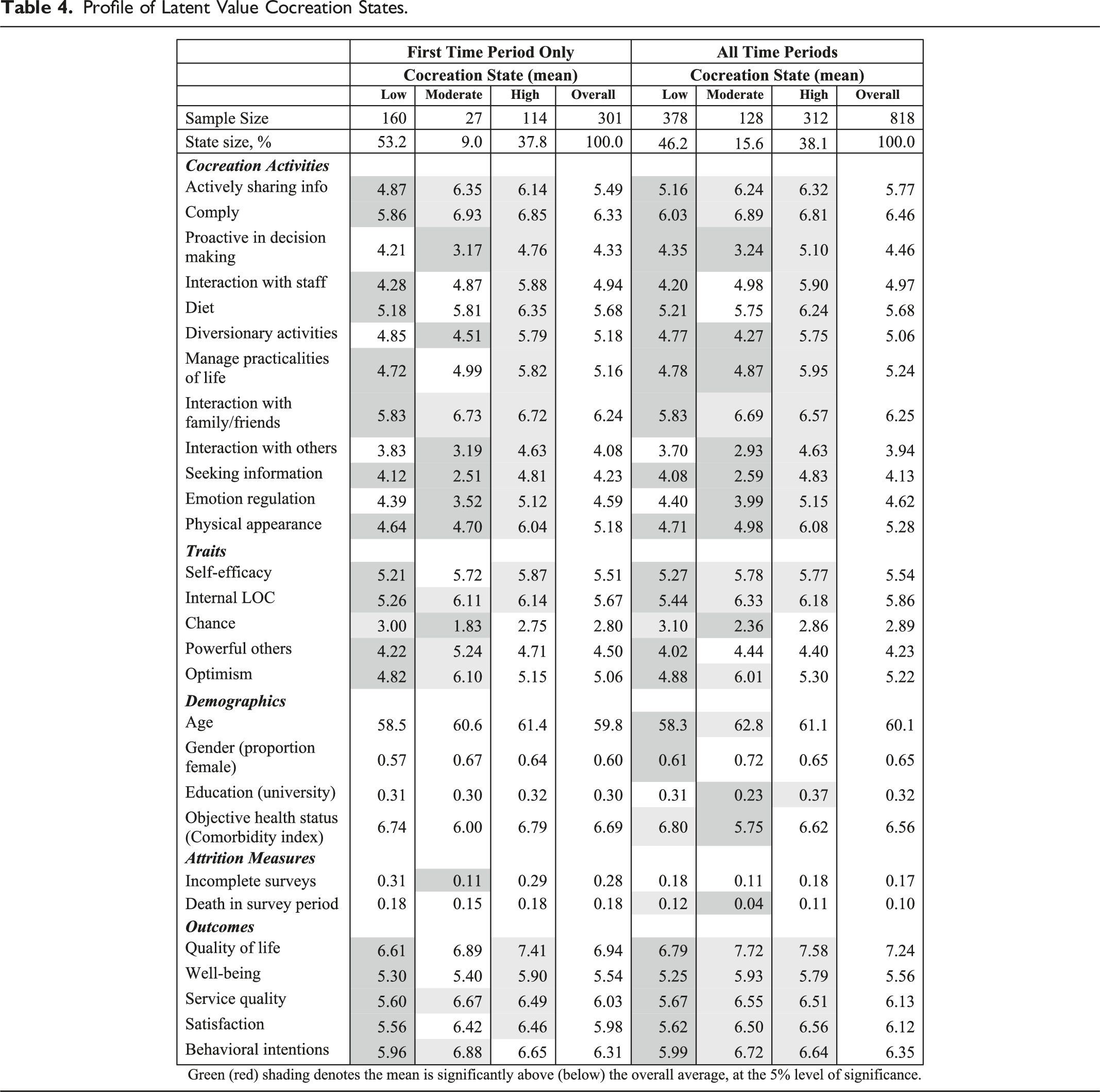
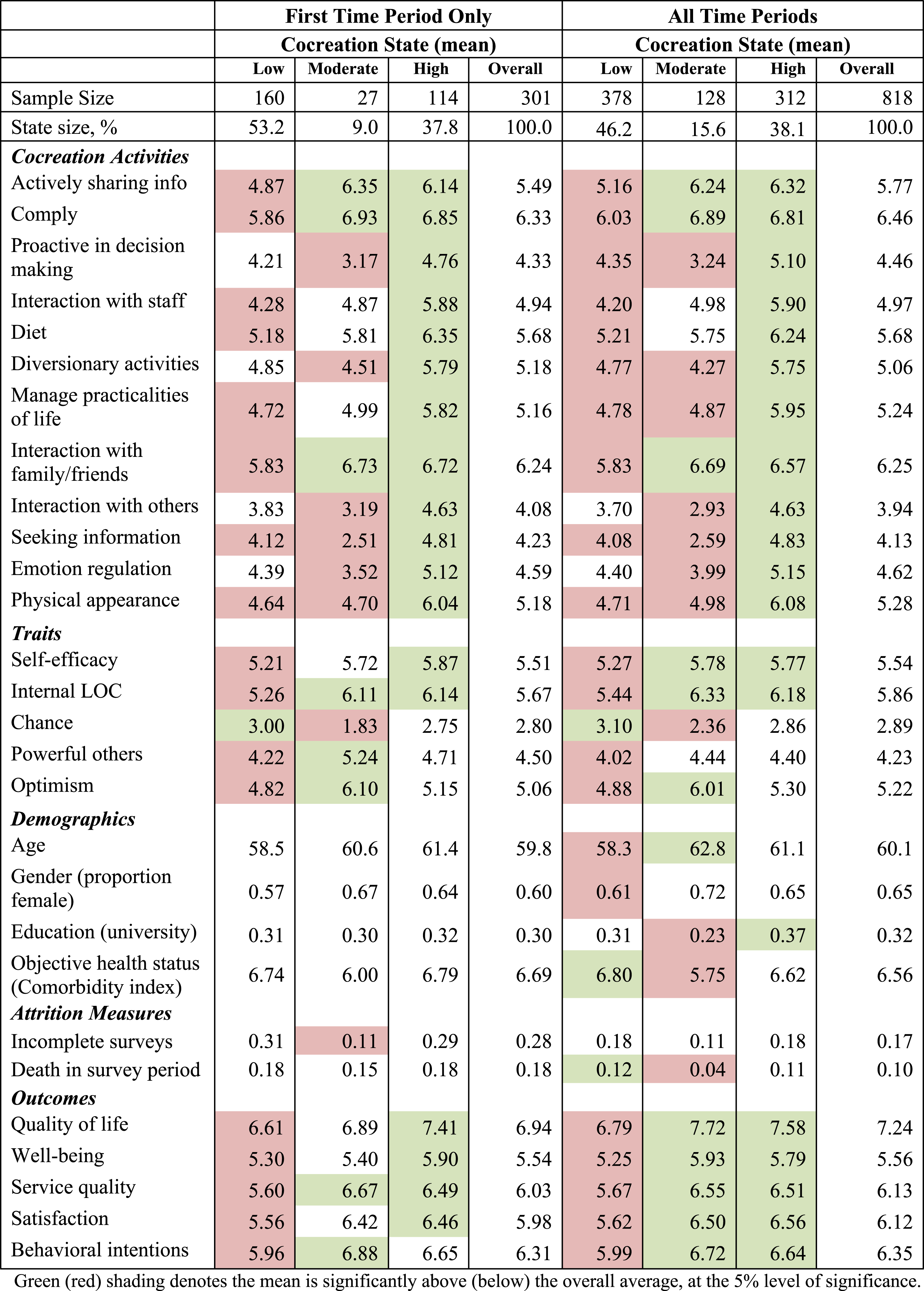
Profile of Latent Value Cocreation States.
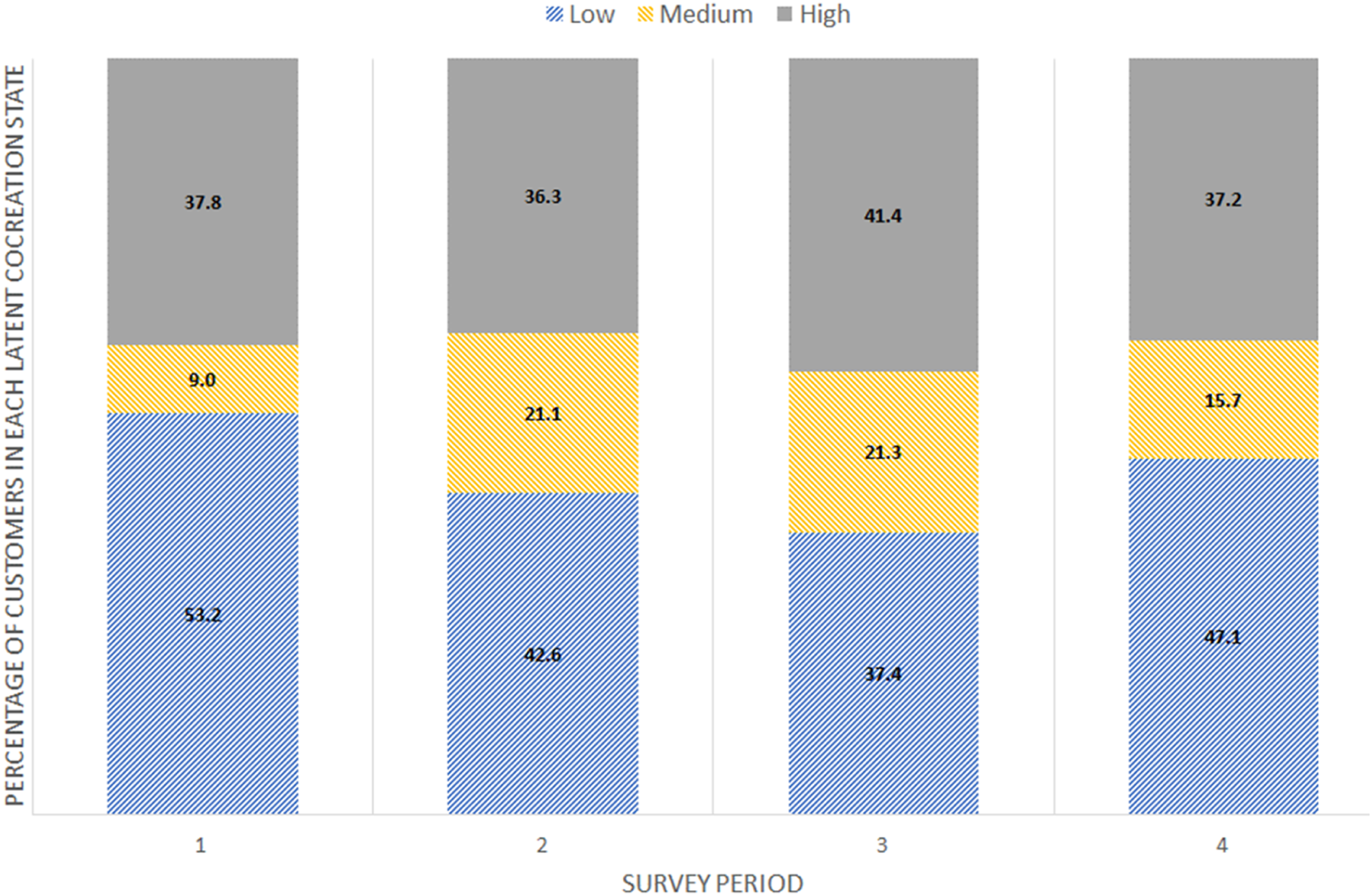
Percentage of customers in each cocreation state across survey periods.
Returning to Table 4, we compare each state’s mean for each measure against the overall mean using ANOVA. To aid and simplify the exposition of these many ANOVAs we color code the columns in Table 4. Red shading indicates a state’s mean is statistically significantly below the overall average at the 5% level of significance, while green shading indicates a state’s mean is above the overall average. The pattern for the 12 cocreation activities is broadly in line with Table 3: customers in the low cocreation state have most of their cocreation activity means significantly below the overall average; those in the moderate state have some means above average and some below; those in the high cocreation state have all cocreation activity means above average.
Turning attention to personality traits, those in the low cocreation state are below average on self-efficacy, internal locus of control, powerful others, and optimism, and above average on chance. In contrast, those in the moderate and high states rate themselves above average for internal locus of control and self-efficacy. Interestingly, those in the moderate state are the least likely to agree that their health status is affected by chance and the most likely to agree that their own actions and those of powerful others can influence their condition (e.g., internal and powerful other locus of control).
In the first time period there are no significant differences in customer demographics across the states. However, looking across all the time periods, the effects of attrition start to emerge, with relatively more men and more younger customers in the low cocreation state. Looking across all time periods, those in the low state have more comorbidities and a slightly higher death rate. In contrast, those in the moderate state have the lowest comorbidities and death rate.
The last five rows of Table 4 compare outcome measures across the states. Not surprisingly, across all time periods, those in the low state have significantly lower perceived outcomes for all five measures, while the reverse occurs for those in the moderate and high cocreation states. This provides some initial evidence that being in a moderate or high cocreation state has benefits for customer quality of life and well-being, as well as outcomes that are important to a service provider, such as customer satisfaction and behavioral intentions.
Transition Matrix
Transition Probabilities Between Latent Value Cocreation States.
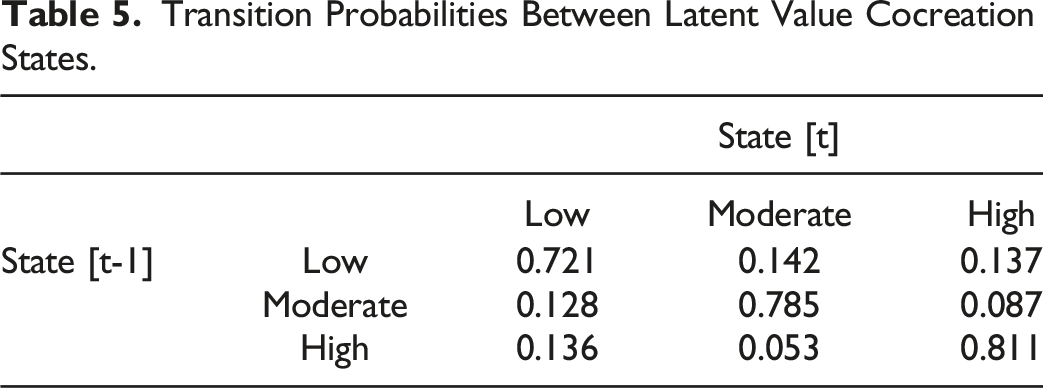
The transition matrix also provides insights into customer movement between two states. For instance, customers in a low cocreation state have probabilities of 0.142 and 0.137, respectively, of moving to the moderate and high cocreation states. Moreover, the transition probability between moderate and high cocreation states is 0.087, while the reverse transition has a lower probability (0.053), reinforcing the stickiness of the high cocreation state. There is also some notable movement from the moderate and high cocreation states down to the low cocreation state, as also seen in Figure 2. This is not necessarily a bad thing as some customers feel less need to maintain cocreation activities as their health improves during the recovery phase.
Activities Influencing Value Cocreation State Transitions
Zhang et al. (2016) investigate the influence of a number of factors on upward and downward migration in customer relationship states. We now undertake an analogous examination to that of Zhang et al. (2016) by utilizing the longitudinal nature of our data to look for situations where a customer transitions from their current state to a state with more (or less) cocreation activity. For example, Figure 2 shows that between the first and second survey waves the percentage of customers in the moderate cocreation state rises from 9.0% to 21.1%, but declines from 21.3% to 15.7% between the third and fourth survey waves. There are three possible ways a customer can upwardly increase their cocreation state, either by transitioning from low to moderate, low to high, or moderate to high. Across all the survey waves there are 50 instances of an upward state transition from one survey period to the next. To enable a change in cocreation state there must be a concomitant change in one or more of the 12 cocreation measures, and so a novel feature of this analysis is to reveal which changes in the 12 cocreation activities are most strongly associated with either an upward or downward transition in cocreation status.
To achieve this, we calculate the change in each of the cocreation activities at the individual level from one time period to the next, denoted as
Since
Estimated Coefficients for Multinomial Logit Model Relating Changes in Value Cocreation Activities to Changes in Latent Cocreation State. a
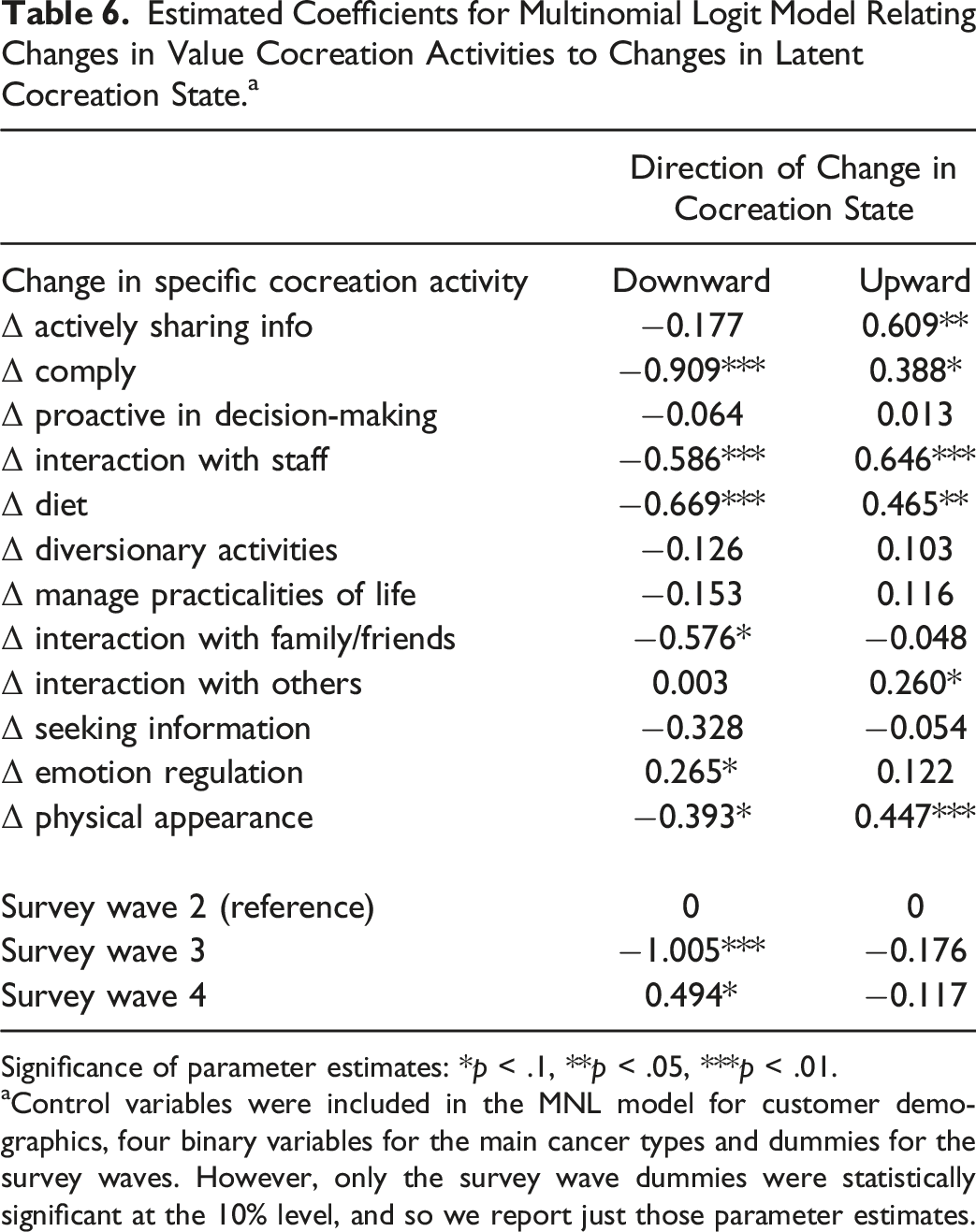
Significance of parameter estimates: *p < .1, **p < .05, ***p < .01.
aControl variables were included in the MNL model for customer demographics, four binary variables for the main cancer types and dummies for the survey waves. However, only the survey wave dummies were statistically significant at the 10% level, and so we report just those parameter estimates.
In sum, our findings support H2 which states that customer value cocreation activities differentially impact transitions between low, moderate, and high customer cocreation states. We find that positive increases in six distinct cocreation activities have the most influence on favorable changes in cocreation state. We now show how these upward and downward shifts in cocreation activities impact service marketing and customer outcomes.
Value Cocreation Activities, Marketing, and Customer Outcomes
Correlation Between State Changes and Outcome Measures.
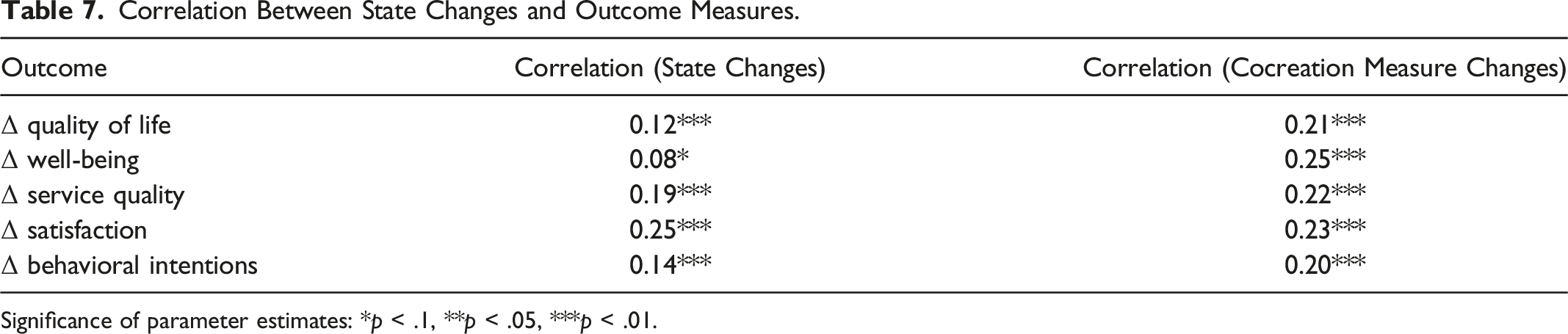
Significance of parameter estimates: *p < .1, **p < .05, ***p < .01.
Although not causal, the fact that we examine changes in outcomes and cocreation activities at the individual level does remove time-invariant effects such as differences among customers. Even after taking first differences, there remain meaningful correlations for cocreation state transitions and activities with key outcomes. The overall findings in Table 7 give indicative evidence that customers who choose to increase their cocreation activities subsequently perceive higher well-being and quality of life, while the reverse occurs for customers reducing their cocreation activities. Managers also benefit when their customers increase cocreation activities, because these customers report higher perceived levels of service quality, satisfaction, and behavioral intentions. Taken together, these findings support hypotheses H3a and H3b.
General Discussion
Our study offers several contributions - it profiles dynamic latent customer value cocreation states, examines transitions between these states, and links these transitions to important outcomes. In so doing, we offer a novel empirical approach that can be adopted by managers and future scholars to better understand the dynamics of customer value cocreation.
Profiling Low, Moderate, and High Value Cocreation States
Our study is the first to profile dynamic latent customer value cocreation states. In the low or “reluctant” cocreation state, we find that customers undertake a broad range of value cocreation activities but they do so with minimal intensity. As these customers have low self-efficacy and optimism they are less likely to believe they have the ability to attain a certain outcome, especially if progress is slow or difficult (Bandura 1977; Scheier and Carver 1992). Reluctant cocreators tend to believe that their health outcomes are determined by luck or chance (external locus of control), they do not believe their own actions or those of powerful others can influence outcomes. Reluctant cocreators tend to be slightly younger (<60) and male. Given evidence that men “under-use” medical services (White and Witty 2009) and are less likely to engage in medical decision-making (Arora and McHorney 2000), this bias aligns with their reluctance to engage deeply in cocreation. Healthwise, these customers have more health issues and a higher death rate, which presents a further challenge to value cocreation.
We find that customers in the moderate or “selective” cocreation state undertake a narrow range of cocreation activities but do so with high intensity. Customers in this state have high self-efficacy, optimism, and internal locus of control. They also believe in the influence of powerful others. Selective cocreators are confident in their capacity to attain a specific outcome and believe that their actions and those of powerful others can influence outcomes. This may explain their predilection for activities like compliance with medical advice and actively sharing information with medical staff. Selective cocreators tend to be slightly older (>60), with a lower education level. This dovetails with research that older and less educated patients are more likely to “blindly trust” medical care (Meyer, Ward, and Jiwa 2012; Rodriguez et al. 2013), and are less likely to engage in activities that are not directly associated with powerful others.
In the high or “active” cocreation state, customers undertake a broad range of activities, all with high intensity. These customers have high self-efficacy, optimism, and a strong internal locus of control. They believe that outcomes are influenced by their own choices and actions. Individuals with high internal locus of control typically try to master their environment (Keenan and McBain 1979), and are confident in their ability to undertake the behaviors necessary to influence outcomes (Bandura 1977). Consequently, active cocreators are willing to strive towards a goal even if the associated activities are challenging (e.g., proactive decision-making) or time consuming (e.g., managing diet, and appearance). Active cocreators are often highly educated. As educated patients have greater health literacy, seek out more information, ask more questions, and are more confident and assured in medical interactions (Street and Millay 2001; Arora and McHorney 2000), it is not surprising that customers in this state engage in a broad range of activities with intensity.
Value Cocreation State Transitions
As well as profiling value cocreation states, our study is the first to reveal the extent to which healthcare customers change latent cocreation states over the course time (see Figure 2), and estimate the probability that a customer will remain in their current cocreation state or transition states (see Tables 5 and 6). Indeed, we find that an increase in the specific cocreation activities of actively sharing information, compliance with medical requirements, interacting with staff, maintaining a healthy diet, interacting with others, and maintaining a good physical appearance are associated with an upward transition to a higher cocreation state. Further, with the exception of actively sharing information and interacting with others, an increase in these cocreation activities is associated with preventing a downward state transition, thus stabilizing a customer in a particular state, which is a desirable outcome for those in the selective or active states.
We also find that an increase in the activity of emotion regulation is associated with a downward state transition, which is an undesirable outcome. Emotion regulation reflects how customers modify their expressive behavior, including how they communicate information and emotions about their illness to others. As emotions run high in cancer services, it is not uncommon for customers to modify/regulate their expressive behavior to protect themselves and others. This can be problematic as high levels of emotion suppression are associated with increased emotional distress (Cordova et al. 2003).
Our findings are novel in that they highlight which value cocreation activities positively influence state transitions and/or stabilize customers in a desirable state, and which need to be managed to avoid a downward transition. The benefit of getting customers to undertake activities associated with positive state transitions is improved perceptions of service quality and customer satisfaction, positive behavioral intentions, and higher perceived quality of life and well-being for patients. Importantly, we find that even patients with a poor prognosis still engage in cocreation activities (as do those with a more favorable prognosis)— patients still want to live the best life they can, even if they have a life-limiting disease. Value cocreation thus represents an important strategy for healthcare services. However, we note that there are situations and customers for which value cocreation might not be appropriate, because they may not have the skill, ability, access, or willingness to cocreate.
Managerial Implications
Our study highlights the value cocreation activities that are associated with state transitions (see Table 6). For example, we find that managing one’s diet is associated with a positive state transition and also with stabilizing a customer in a more desirable state. Managers can use this knowledge to design information modules such as “nutrition for people living with cancer,” provide regular access to dietitians who can establish a nutritional plan for that patient, and encourage customers to ask questions and share information with their care team. While managing diet is a tangible cocreation activity where hands-on individual appointments or group workshops can be developed, the psycho-social/educational needs of cancer patients can also be addressed in a variety of ways. For instance, to help customers actively share information managers can develop tools such as medication tables/checklists, instigate pre-appointment questionnaires, and encourage patient symptom and question diary keeping. These initiatives can greatly increase the likelihood of customers sharing critical information.
Our findings also highlight that healthcare providers should be cognizant of a customer’s value cocreations state, as highlighted in Figure 3. We find that reluctant cocreators have the most to gain from value cocreation but they do not believe they have the ability to influence outcomes like well-being. To bolster confidence in undertaking value cocreation activities, healthcare providers need to strengthen self-efficacy and optimism, and foster an internal locus of control in reluctant cocreators. While psychological characteristics are relatively stable they are nonetheless malleable (Bandura 1977), with studies demonstrating that when self-efficacy and internal locus of control are strengthened, individuals are able to undertake difficult tasks with confidence (Bandura 1984), and are more likely to change their health behavior (Grembowski et al. 1993). Customer value cocreation state profiles and associated marketing strategies.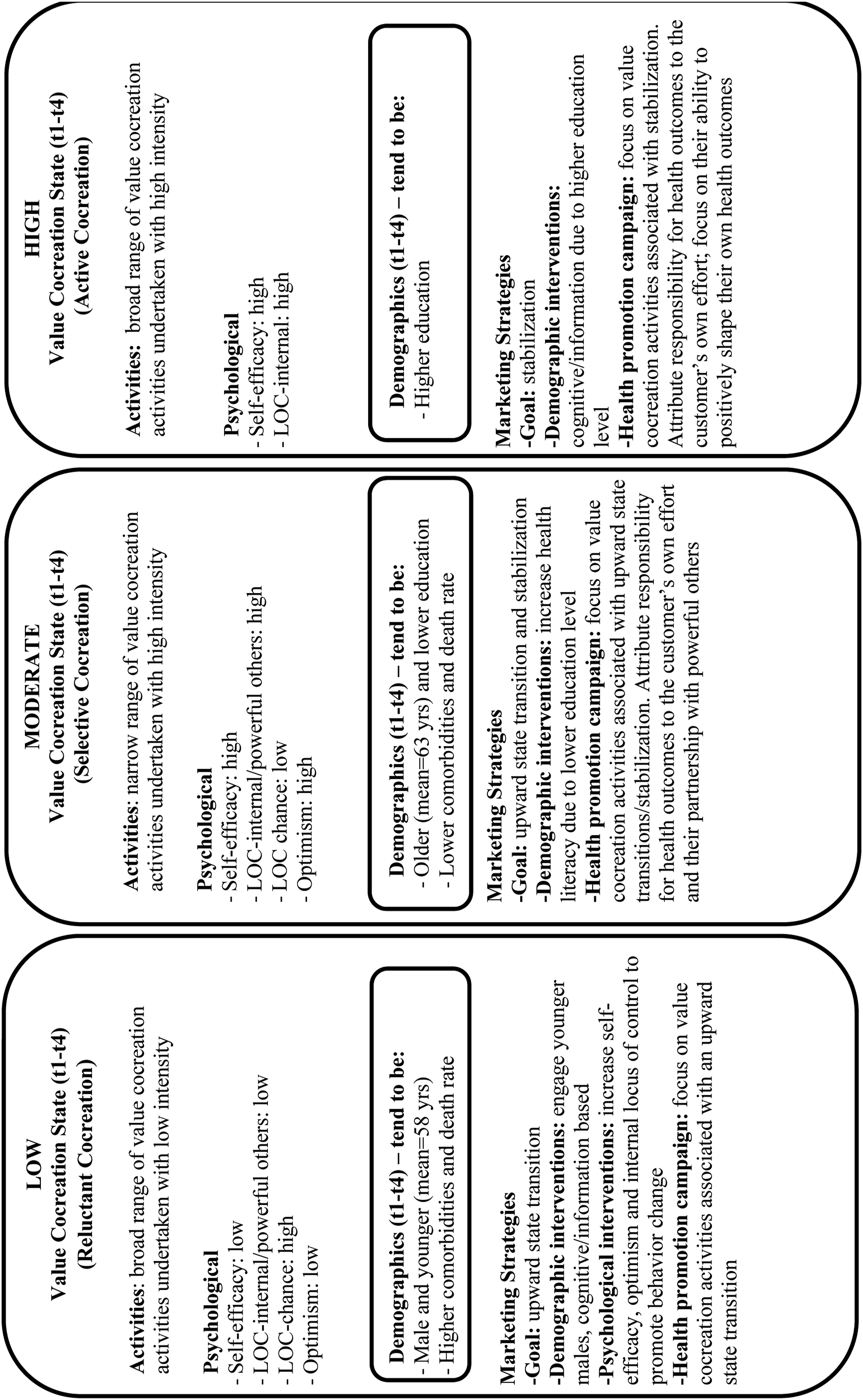
Selective cocreators are already in a desirable state; however, managers should aim to either retain customers in this state or transition them to the active cocreation state. We posit that customers in this state would benefit from health literacy programs as they tend to be older and have a lower education level. They would also benefit from engagement in the 6 cocreation activities that positively influence upward state transitions and the 5 activities that prevent slippage to a lower state (see Table 6). Selective cocreators have higher self-efficacy, greater optimism, and a strong internal locus of control. As they also believe that outcomes are governed by powerful others, attributing responsibility for outcomes like improved well-being to the customer’s partnership with powerful others (e.g., “Together You and Your Doctor Hold the Key to Your Well-being”) may be particularly effective when developing information materials for these customers.
As active cocreators are in the most desirable state, managers should aim to retain them in this state by preventing a downward transition. This can be achieved via the 5 cocreation activities in Table 6 that have significant negative coefficients. As active cocreators have a higher education level they may benefit from factual information around the process and benefit of undertaking certain cocreation activities. Given that increased emotion regulation is associated with a downward state transition, interventions can be designed to assist active cocreators in managing their emotions, particularly how they share information with others (selective cocreators would also benefit from this approach). As health information that is aligned with an individual’s locus of control is effective in influencing health behavior change (Williams-Piehota et al. 2004), focusing on an individual’s responsibility (e.g., “You Hold the Key to Your Well-being”) in maintaining their own health may also be effective for these customers.
Limitations and Further Research
As we study customer value cocreation within the Australian private healthcare sector, applying our finding to other localities or healthcare systems needs to be undertaken with caution. Our focus was also on individuals who accepted cancer treatment thus we do not offer insights on the relevance of value cocreation activities to non-users or service refusers. And while the cancers we studied can be considered chronic (as patients are monitored for recurrence and live with the late-effects of their treatment), not all cancers require long-term intervention or follow-up. While our study examines value cocreation activities across cancer types (and prognoses), a more nuanced approach examining differences between cancer types (e.g., breast versus skin cancer) may be insightful. We therefore encourage future researchers to consider value cocreation dynamics in different localities and healthcare systems, for users and non-users, and for specific cancer types.
As our study focuses on cancer services, we adopt the chronic health (viz., cancer) cocreation activities of Sweeney, Danaher, and McColl-Kennedy (2015). However, we recognize that there are other activities that could be included in our study. We encourage future researchers in healthcare to expand upon these activities and for those in other settings to explore the range of activities relevant to their context. Relatedly, considering additional germane variables like customer autonomy, competence, and health literacy, as well as firm variables, like communication channels, would be worthwhile, as would examining the effect of value cocreation activities on different aspects of perceived quality of life (e.g., social, emotional, physical, and economic functioning) and on firm outcomes like innovation or process efficiencies.
We additionally note that the timeframe and data collection points in our study were developed after consultation with medical experts (and patients). They mirror a typical cancer service experience, capturing diagnosis, treatment, and a post-treatment phase. However, we recognize that in our and other healthcare and service settings, a longer time horizon may provide additional insights. Indeed, a longer timeframe would allow researchers to study in greater detail the activities undertake beyond the medical clinic including other public and private facing activities.
Finally, a logical next step would be to examine the concept of cocreation transitions in other contexts using the innovative empirical approach outline in our study. In the healthcare sector, our findings and approach are relevant to a range of services such as cardiovascular, diabetes, asthma, arthritis, obesity, and mental health services. Our research is also pertinent to other services which are complex, interactive, and ongoing (e.g., education, financial planning, and personal services) where customer value cocreation is relevant and important to customer and marketing outcomes. We encourage future research to adopt our methodology to profile latent customer states (be they sustainable consumption, media usage states, or loyalty states), examine transitions between these states, and determine the effect of these transitions on important outcomes over time.
Supplemental Material
Supplemental Material - Dynamic Customer Value Cocreation in Healthcare
Supplemental Material for Dynamic Customer Value Cocreation in Healthcare by Tracey S. Danaher, Peter J. Danaher, Jillian C. Sweeney, and Janet R. McColl-Kennedy in Journal of Service Research
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Australian Research Council (LP0775220).
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.