
Abstract
In the global world, service cultures interact. The co-shaping interaction of local and global service cultures is a form of glocalization. In China, interaction between traditional Chinese medicine (TCM) and Western medicine (WM) has produced glocalized versions of both services. Through analysis of customers’ experience of healthcare service in southwestern China, this paper addresses two research questions: What distinctive cultural resources do informants associate with WM and TCM? And how do tensions emerge in the contrast between customers’ expected and experienced cultural resources in glocalized healthcare service? The resource integration construct provides theoretical language to analyze customers’ service experiences in glocalized service cultures. One theoretical contribution resulting from this analysis is showing that culturally specific resources embedded in service systems emerge phenomenologically through resource integration in customers’ experiences. A second theoretical contribution resulting from this analysis is demonstrating how the mix of culturally specific resources from two glocalized services causes tensions and effects how experience is interpreted and valued. The article’s managerial contribution is a four-step culture-comparative resource framework. The framework can help managers identify tensions in customer expectations and experiences in glocalized service and identify needed changes to facilitate customers’ positive service experiences.
I have visited the TCM [traditional Chinese medicine] hospitals several times. I expected I could get relaxed feelings in TCM but I was disappointed. They are called TCM hospitals, but the buildings and facilities are quite like WM [Western medicine] hospitals. And actually, in these TCM hospitals, WM is the dominant and TCM is only account for a small part of the business. I felt the same discomforts and anxieties as I was in WM hospitals. The air inside was full of the odor of disinfectants. People were crowded and hustling. The noises of screaming, crying and shouting made me feel sick. There were no cultural decorations as I expected, for example, calligraphy works and ancient paintings. The white and dull walls made me feel trapped. Doctors appeared quite busy, irritated and even fierce …. I even felt upset to ask them questions. (Dang, 54, Male)
Service experiences, that is, customers’ subjective interpretations of direct and indirect interactions with the service and service provider (Bitner 1992; Lemon and Verhoef 2016), are individually determined, based on service expectations. The epigraph illustrates that customers’ service expectations are culturally complex and multi-dimensional (Kabadayi et al. 2019). For example, Dang associates WM hospitals with discomfort, feels entrapped by white walls, misses cultural decorations, and experiences fear induced by doctors’ expressions. In a world of global marketing, service experience is increasingly embedded in the interplay of global and local service cultures (Cayla and Bhatnagar 2017; Korsmeyer 2016), which creates glocalized service cultures. In practice, this means that a customer may experience service via overlapping and interpenetrating service systems. From a cultural resource perspective, customers’ expectations and resulting experiences will derive from glocalized systems of meaning. We postulate that customers, such as Dang above, may experience tensions when their expectations clash with their experiences of culturally specific resources associated with glocalized service cultures.
Prior research in service-dominant logic (S-D logic) identifies a research gap and a need for analyses that focus on the impact of culture in service experiences as the epigraph illustrates (Akaka, Vargo and Schau 2015; Wilden et al. 2017). To date, service research has not focused on glocalization of services and customers’ service and resource expectations and experiences. Thus, it is essential to understand the tensions, such as those mentioned in the epigraph, emerging in service when expected cultural resources do not align with experienced ones. The purpose of this paper is to analyze resources that customers associate with WM and TCM service, and the emerging tensions between expected and experienced resources they integrate in service. Chinese government policies have shaped both Western medicine (WM) and traditional Chinese medicine (TCM) resulting in the glocalization of both service cultures. We use TCM and WM to refer to these glocalized service cultures, and not to the TCM of pre-Western influence and WM as practiced in the West now or in the past.
The resource integration construct (Bruce et al., 2019; Constantin & Lusch, 1994), which we elaborate in the next section, provides theoretical language to analyze customers’ service experiences in such glocalized service cultures. With the focus on customers’ experiences of culturally specific resources, this paper employs a holistic definition of culture as a repertoire of shared operant (immaterial) and operand (material) resources mobilized in particular social situations and relationships to guide action and interpretation of experience (Arnould and Thompson 2005). This study addresses two research questions. Given the call to address the impact of culture on service experience, we ask: What distinctive cultural resources do informants associate with WM and TCM? And given the evidence discussed below for tensions in service experience when providers and customers’ cultural backgrounds differ, we ask: how do tensions emerge in the contrast between customers’ expected and experienced cultural resources in glocalized healthcare service?
The paper next provides a theoretical review of resources in customers’ expectations and experiences, followed by discussion of the interplay of global and local service cultures that creates glocalized sociocultural contexts. This paper employs sociological definitions of glocalization (Robertson 1992) to conceptualize glocalized service culture as the unique interpenetration and process of co-shaping of local and global service cultures. Next, we discuss cultural resources in S-D logic and customers’ phenomenological experiences of them (Gill et al. 2010). From there, we move on to a discussion of the context of the study and our phenomenological methodology.
In the discussion, we return to the theoretical and managerial implications of the paper. One theoretical contribution responds to recent calls in service research to understand how resources emerge (Koskela-Huotari, Edvardsson and Tronvoll 2018) and how they are combined in services (Bruce et al., 2019). In our phenomenological perspective, culturally specific resources are not objective things with determinant effects that exist a priori; instead, they emerge in customers’ experiences where they may or may not align with their expectations.
A second theoretical contribution is to demonstrate how the mix of culturally specific resources from two glocalized services causes tensions in customers’ service experiences. Expectations for certain cultural resources that align with TCM conflict with service experiences of resources that align more closely with WM. These tensions, rather than under performance on service quality dimensions as in older service research, give rise to consumer anxiety and negative evaluations of their experiences.
The study’s managerial contribution is a four-step culture-comparative resource framework to identify culturally specific resources mobilized in glocalized service. The culture-comparative framework moves beyond merely adding, subtracting or measuring discrete elements of glocalized service to better facilitate customers’ positive service experiences. Finally, we open future resource avenues to study culturally specific resources, tensions between customers’ expectations and experiences, and how to manage them.
Theoretical Background
In this study, we adopt the perspective that service experience is foundational to business (Lusch and Vargo 2006). But, as human experience including service experience is shaped by cultural context (Korsmeyer 2016), we first elaborate our theoretical understanding of cultural resources and customers’ experiences of these resources based on the phenomenological approach, followed by our enabling perspective on sociocultural glocalization.
Culturally Specific Resources in Customers’ Expectations and Experiences
Resource integration refers to activating, assembling and combining firm and customer resources in a specific context such as in service, which produces meaningful actions, experiences, and outcomes (Bruce et al., 2019). This resource-based view of service experience derives from Penrose (1959) who considers the firm as a collection of productive resources. Resource-advantage theory subsequently proposed that a resource is anything that enables a firm to produce a market offering (Hunt and Morgan 2004). Following the Service-Dominant logic (S-D logic) framework, resources can be categorized into operand or operant resources. Operand resources are tangible, such as tools and products. Operant resources are intangible human resources, such as interaction styles, skills, explicit, and tacit knowledge, including cultural knowledge (Constantin and Lusch 1994). For firms, some operant resources are strategic, relational assets that defend firms from competitors, bind suppliers to them, and enable firms to realize customers’ preferences in improved market offerings (Madhavaram and Hunt 2008). As such, operant resources are of necessity situationally variable.
S-D logic emphasizes that operant resources provide the competitive edge in service and raise the question of “how to apply collective skills, experiences and knowledge (operant resources)” for the benefit of customers (Vargo and Lusch 2017, 52). Dynamic operant resources (e.g., knowledge, skills, and interaction styles) act on operand (tangible, material) resources, through which operant resources are expressed (Jaakkola, Helkkula and Aarikka-Stenroos 2015; Lusch and Vargo 2006). Of course, resources pertinent to service vary across service types, for example, banking versus adventure tourism, but also we contend across cultures.
One pertinent axiom of S-D logic is that “all economic and social actors are resource integrators,” who combine diverse resources to co-create value (Vargo and Lusch 2016, 18). Thus, this axiom posits that not only the firm, but also customers (and other relevant actors) integrate both operant and operand resources to co-create service experience (Bruce et al., 2019; Vargo & Lusch, 2008). In line with the S-D logic perspective, we state that products and materials are vehicles of service; the value of resources derives from conscious or unconscious experience of them (Schembri 2006). Until recently, service research has not focused on resources specific to given cultures although tourism service research has recognized their significance (Chronis, Arnould and Hampton 2012). Still, a few service researchers have acknowledged the need for empirical studies of service culture. Thus, Akaka et al. (2015) and Wilden et al. (2017) call for research that contributes to understanding the integration of symbolic, material and social resources in service experience.
This paper integrates two perspectives in analyzing resource integration. First, we take the phenomenological approach to resource integration that foregrounds customers’ subjective expectations and experiences of culturally specific resource integration. Customers’ prior experiences [of resources] foreground specific expectations they apply in new contexts, and channel current experiences, as well as merge with remembered past experiences (Helkkula, Kelleher and Pihlström 2012). At the same time, phenomenological experiences are shaped by cultural contexts. Pelto and Pelto (1975) argue that individuals’ expectations and experiences make up a “cultural pool”; insofar as culture is learned, individuals are the locus of culture, conceived of as a shared operant resource. Consequently, in order to study experience of resources holistically, Pelto and Pelto (1975) support analysis of the interplay between the meso-level of shared operant resources and individual level expectations and experiences that incorporate such operant resources. Therefore, it is important to connect individual, subjective expectations and experiences of resources to the meso-level understanding of the culturally specific operant resources.
Second, we understand resource integration as “emergent” (Clayton 2006) when customers, service providers, and other actors integrate resources within a service to co-create experience. Customers’ expectations and experiences of culturally specific resources emerge in service, where, as previous service research shows, the integration of materials, knowledge, interactions, signs, and other resources generate customers’ service experiences (Chronis, et al. 2012; Hamed, El-Bassiouny and Ternès 2019). This positions resources (interaction styles, practices, materials, symbols, and signs) as collective, emergent phenomena that both shape experiences and which people integrate to give sense to experiences (Bruce et al., 2019). For example, material such as medicines becomes an operand resource when integrated with other resources through specific experiential interactions (Bruce et al., 2019).
Despite recent interest in customers’ subjective service experiences, service research has paid little attention to distinctive cultural resources in service expectations and experiences, and how they emerge in interaction styles, practices, signs, and symbols (Bendapudi and Leone 2003; Spanjol et al. 2015). One exception is a study in consumer research, which shows how evoking alternative Western or Chinese cultural healthcare resources influenced customers’ service expectations (Wang, Keh and Bolton 2010). This study provided inspiration to investigate the effects of culturally specific resources on customers’ service expectations and experiences.
According to the holistic understanding of culture as a dynamic set of shared operant resources people draw upon to act and to make sense of experience (Arnould and Thompson 2005, 2018), customers may negotiate overlapping and sometimes even conflicting resources (systems of interactions, materials, signs, and symbols) to make sense of their experiences and achieve their purposes in particular social situations (Arnould and Thompson 2018). As customers’ expectations and experiences of culturally specific resources are subjective, a customer’s expectations may not align with experiences of resources and this misalignment may cause tensions in experience.
We follow Lupton (2012)’s influential text that frames WM as the culturally distinctive meanings, discourses, practices (operant resources), and technologies (operand resources) that accumulate around Western medicine and customers’ understandings (operant resources) of their bodies, health, and illness status in Western countries (see also Mattingly and Garro 2000)). Thus, customers’ healthcare service expectations and experiences integrate knowledge, relational, material, and symbolic resources, which are similarly embedded in doctors’, nurses’, and pharmacists’ medical practices and informed by medical service culture (Lupton 2012). At the same time, customers’ microsocial contexts (e.g., family, class, ethnicity, gender, and culture) and differential resource endowments also condition prior and current healthcare experience. In this way, ethnic minority patients’ complaints about inadequate respect or communication (Chalmers and Omer-Hashi 2002; Degni et al. 2014; Gould and Gould 2003), or their non-compliance with healthcare guidance (Gamble 1997), may reflect discrepancies in operant resource endowments among actors in healthcare (Main 2016).
Sociocultural Glocalization
The specific focus of this study is resources that customers integrate in glocalized service and the emerging tensions that arise between expected and experienced resources. Glocalization theory offers a perspective to improve understanding of the reciprocal impact of cultural contexts and service experiences insufficiently examined in previous research. Glocalization theory highlights the limitations of the Hofstedian concept of homogeneous national cultures (Arnould and Thompson 2005). But what is glocalization in service? Examining the intensifying global circulation of financial, technological, ideational, commercial, material, imagistic resources, and the like, Robertson (1992) adopted the term glocalization to theorize processes where “the global [culture] always become localized, and the local [culture], globalized” (p.161). Robertson (1992)’s theoretical framework does not predict that outside-in global marketing flows increase cultural homogeneity, in contrast to some formulations (Ritzer 2003). Instead, the global circulation of commercial formats, products, and images produces diverse glocalized outcomes (Ger and Belk 1996). Insofar as glocalization fuses elements from different global and local cultural schema, then “the interpenetration of the global and the local [actually] results in unique outcomes in different geographic areas” (Ritzer and Dean 2011, 159). Glocalization theory predicts that global flows create cultural hybrids. Glocalized consumption hybrids sometimes give people new means of representing their own culture (Ger and Belk 1996).
Glocalization also produces hybridized service forms. For example, according to Kjeldgaard and Östberg (2007), Scandinavia exhibits a hybrid café service culture; it is a glocalized service rather than a “Starbuckified coffee culture” to use Thompson and Arsel (2004)’s term. Similarly, Askegaard and Eckhardt (2012) describe the uptake of commercial yoga service in India as a glocalized hybrid, a “transformative compromise.”
Little service research has examined distinctive cultural or glocalized resources in service expectations and experiences manifest in interaction styles, practices, signs, and symbols, and how they emerge in service (Bendapudi and Leone 2003). Nevertheless, one key study showed priming subjects with alternative Western or Chinese cultural healthcare schemas (an operant resource) employing simple cues significantly influenced customers’ service preferences for TCM versus WM (Wang et al. 2010).
Similarly, little glocalization research has examined tensions in customers’ expectations and experiences of service. Some exceptions from previous research have documented that glocalization of service can induce conflict because of conflicting cultural resources associated with the service. For example, one study showed that English language proficiency (an operant resource) became a source of discrimination impacting both positive and negative employee experiences in India’s glocalized interpersonal services (Cayla and Bhatnagar 2017). But this research did not examine customer service experience with these linguistic resources. Similarly, the diffusion of glocalized yoga services in the US market has been tension-ridden, for example, to this day teaching yoga is forbidden in Alabama schools because of perceived conflicts between yoga and Christian dogma (Coskuner-Balli and Ertimur 2016). However, this research is silent on the impact of these public conflicts on customer service experiences.
Glocalization theory thus offers a perspective to improve understanding of the reciprocal impact of cultural contexts, integration of culturally specific resources, and service experiences insufficiently examined in previous service research (Jaakkola et al. 2015). Kabadayi et al. (2019)’s recognition of service experience’s complexity and its multi-dimensionality leads us to this investigation of service expectations and experiences in the glocalized healthcare service systems that emerged simultaneously in China. We claim that resource integration in glocalized service is important to customer experiences as customers integrate culturally specific resources when setting expectations and evaluating service. In this study, the resource integration construct gives us language to examine how expectations for certain materials, knowledge, practices, and interactions (and other resources) that align with TCM may conflict with experiences of differing materials, practices, and interactions (and other resources) that align with WM. Next, we discuss context and method before turning to the empirical study of how customers experience culturally specific resources in glocalized WM and TCM service.
Context and Method
Glocalization always occurs in specific, culturally distinctive contexts, locations, and times. This study’s context is healthcare service, where managing customers’ experiences is of utmost importance (Berry 2019). Healthcare service in contemporary Southwestern China offers a culturally distinct location for the study of customers’ glocalized service experiences. That is because China is unique in institutionalizing medical pluralism, that is, two medical cultures in its official healthcare system (Hsu 2008).
TCM is a legacy of several thousand-years’ of medical philosophy and a foundation in Taoist and Confucian thought (Chen and Xu 2003; ShenNong 2003). Meantime, Jesuit missionaries brought a version of WM to China in the 17th century, but it flourished only as the efficacy of germ-based treatment developed in the 19th century. In the mid-20th century (1957–1964), government intentionally standardized and institutionalized TCM notably by suppressing its spiritual elements, and integrating some WM elements (Taylor 2005; Hsu 2008). This government driven process drove the integration of TCM with an imported WM system into what we call glocalized TCM (TCM integrated with WM elements) and glocalized WM (WM as practiced in China). Therefore, this integration of biomedical and local medical systems is a government supported glocalization process of TCM and WM. In this way, it is useful to think of contemporary glocalized TCM as an invented tradition (Hsu 2008, a hybrid product of intentional glocalization.
The People’s Republic of China’s government invests in R&D of TCM through the application of scientific principles (Hsu 2008). WM is practiced in parallel to TCM. For example, “about 90% of the general hospitals have TCM departments” and “almost all of the TCM hospitals are practicing WM as well as TCM” (Xu and Yang 2009, 136). Many Chinese have positive attitudes toward TCM with regards to disease prevention, health promotion, and chronic disease (Lv et al. 2020). The total number of TCM outpatient visits is almost 1.3 billion per year, which is about one third of the total outpatient visits in China (Xu and Yang 2009). Meanwhile, WM is favored for acute medical conditions (Lam 2001; Xu and Yang 2009). “Expensive new drugs and technologies are expected to work” by Chinese consumers (Hesketh et al. 2012, 2), which is perhaps indicative of unrealistic expectations of WM.
Methodology
S-D logic emphasizes that experiences are phenomenologically interpreted (Vargo and Lusch 2008). Customers expect and experience reality of a resource only within their interpretation of the experience via the integration of culturally specific, operant (immaterial) and operand (material) resources (Creswell and Poth 2017). Accordingly, the study adopts the phenomenological approach to study customers’ subjective expectations and experiences of culturally specific resource integration. The aim is to bring to light and make sense of the lived meaning of customers’ expectations and experiences (Van Manen 2014).
Sociology, education, and health research often makes use of phenomenological inquiry (Creswell and Poth 2017). In service research, Shostack (1977) already called for research on experiences, and studies have increasingly been interested in lived experiences (Witell, Holmlund and Gustafsson 2020). Service research has conducted empirical analyses of customers’ phenomenological experiences (Harris et al. 2010). Vargo and Lusch (2008) further stimulated this approach by defining value as uniquely and phenomenologically (experientially) determined by the customer (or any other beneficiary) (Jaakkola et al. 2015).
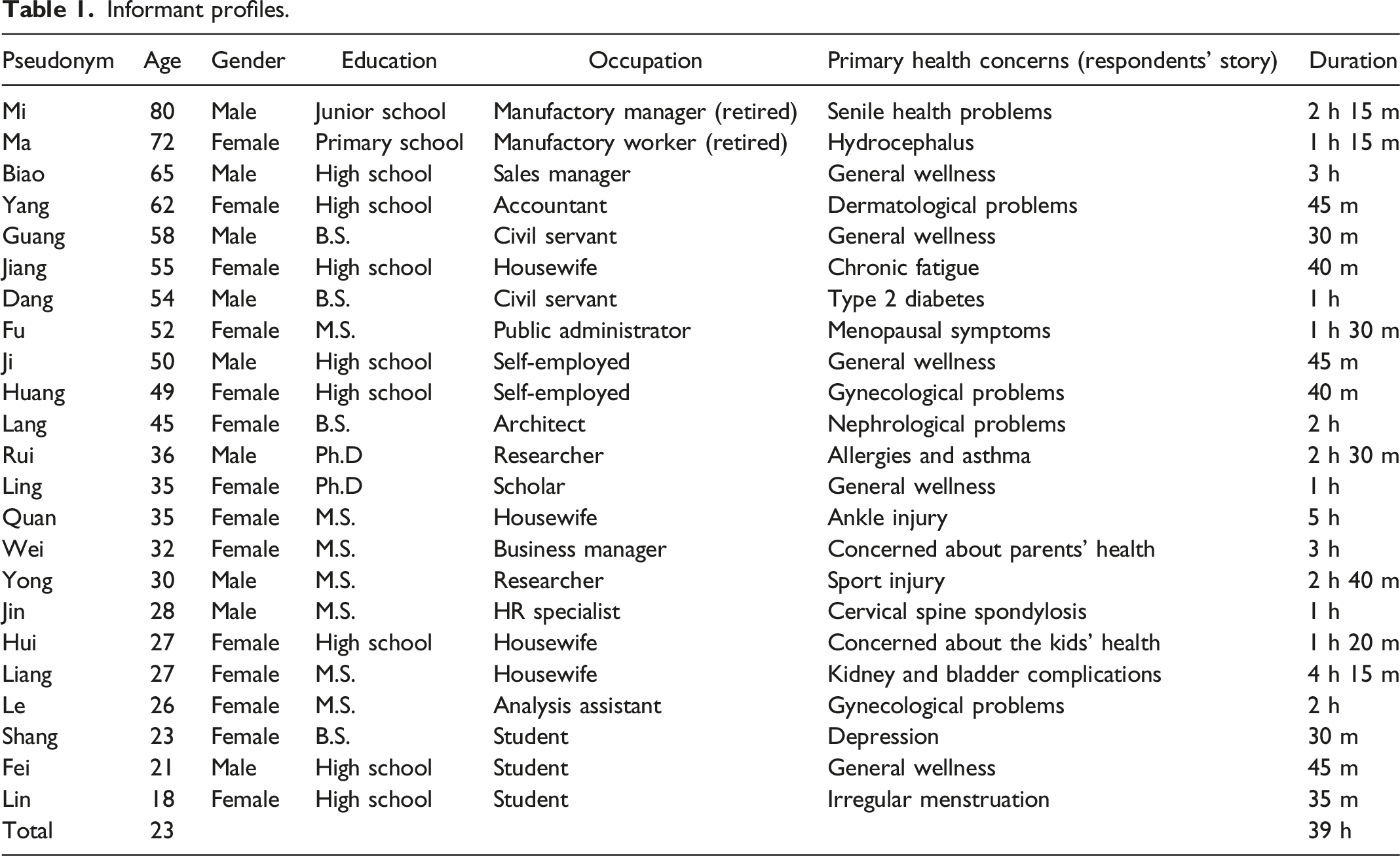
Data Collection
Informant profiles.
Analysis
The heart of qualitative research is data interpretation, which means making sense of, and learning from the data, which requires “both creative and critical faculties in making carefully considered judgments about what is meaningful in the patterns, themes, and categories generated by analysis” (Creswell and Poth 2017, 194). In analysis, phenomenological research focuses on “what” the individuals have experienced and “how” they have experienced it (Moustakas 1994). We followed data analysis steps recommended for phenomenological research (amended from Creswell and Poth (2017): organizing data files; close repeated reading of transcripts, adding margin notes, and forming initial codes; reducing codes into themes of expectations and experiences; making a textural description—what happened; developing a structural description—“how the phenomenon was experienced”; developing statements of significance; grouping statements into meaningful units; and finally developing the theoretical, composite “essence” of customers’ expectations and experiences of culturally specific resource integration.
Findings
This paper poses two research questions: What distinctive cultural resources do informants associate with WM and TCM? And how do tensions emerge in the contrast between customers’ expected and experienced cultural resources in glocalized healthcare service? As these two questions are so intertwined, we discuss them together, organized around resources, with the tensions’ discussion subsumed within the presentation. For purposes of exposition, the culturally distinctive resources are divided into three categories: 1) medical philosophies; 2) interaction styles; and 3) material, signs, and symbols. The first two are operant cultural resources, the latter operand cultural resources. These categories are based on differences between expected and experienced resources. The combination and application of these cultural resources in service either align or misalign (Peters et al. 2014). The misalignments between expected and experienced resources in TCM and WM provoked the tensions between them.
Tensions among cultural resources.
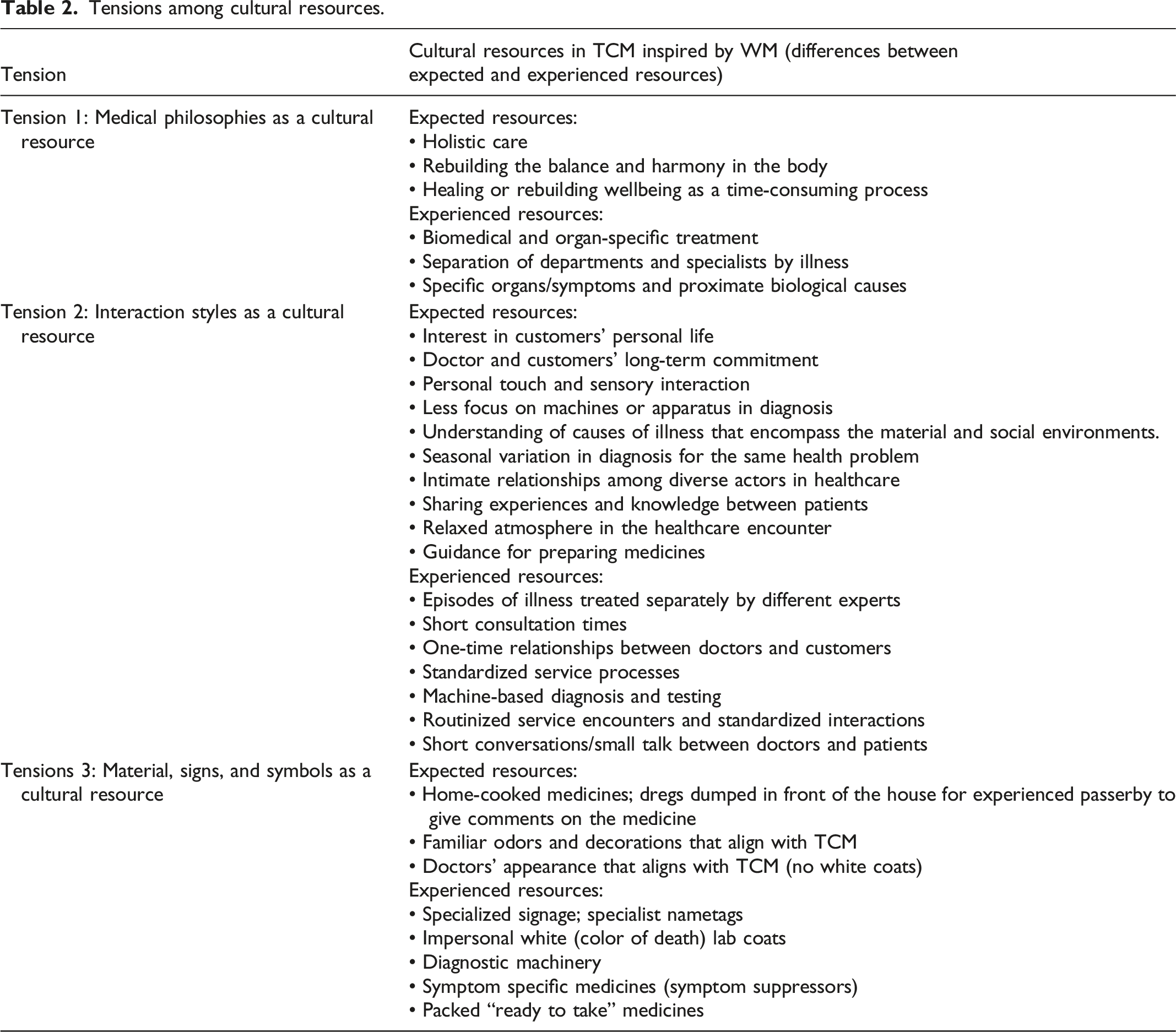
Tension 1: Medical Philosophies as a Cultural Resource
The dominant tension findings reveal is rooted in the discrepant epidemiologies or medical philosophies, an operant cultural resource, upon which the two service cultures are based. WM represents itself as an empirical, scientific, value-free system although of course, it is value-laden (Daly 2005; Knaapen 2014). Contemporary Chinese regard TCM as a value-laden cultural heritage, not just as a medical service (Qiu 2007). The evidence-based biomedical WM model links physical symptoms with determinant biological causes and outcomes (Daly 2005; Knaapen 2014). TCM attends holistically to balances/imbalances in elements and energetic flows within the body, the customers’ life stage, and lifestyle to address illnesses’ root causes (Hsu 2008; Xu and Yang 2009). Customers’ reports emphasize the differences in philosophy between WM and TCM.
First, we contrast the two service systems. In this excerpt, Lin experiences WM service. The service seeks to cure a biomedical symptom with a biomedical material resource, hormones. She contrasts this experience with the holistic treatment she received from the TCM physician in which her life circumstances entered into diagnosis.
I had tried different WMs for my irregular menstruation, targeting the function of womb and ovary or adjusting the hormone. I felt ok when I took the medicine. The symptom appeared again if I stopped taking the medicines for a period of time… The old TCM doctor was not just concerned irregular menstruation, but also asking about my study life. He said his medicine could help to improve my qi and blood flow and asks me not to give much pressure to myself. (Lin, 18, female)
Thus, Lin claims the WM medicine suppresses symptoms but does so only episodically; it treats but does not cure. By contrast, the TCM doctor foregrounds entirely different material and knowledge resources, qi energy and lifestyle, respectively. Lin suggests this “old” approach cures the underlying cause of illness. Lin’s association of glocalized WM with episodic, symptom-based treatment is consistent with previous research on Chinese consumers’ expectations for WM (Lam 2001; Xu and Yang 2009).
By contrast, Quan describes an experience of a holistic, personalized treatment, acupuncture, given by a TCM doctor. In her account, acupuncture helps to “open the channels and smooth the flow of qi of my whole body,” unlike WM that only targets the injury.
…he did not only insert the needles in the [injured] ankle area, but also in other parts of my body, leg, hip…While arranging needles, he explained to me the holism idea in acupuncture practice….I think he fitted entirely into my impression and expectation to an authentic TCM doctor… (Quan, 35, Female)
Like Western medicines, the acupuncture needles are a material resource but embedded in a culturally distinct epidemiology. The doctor represents the needles as vehicles for delivering holistic, personalized care. In this way, the needles and their use come to symbolize “TCM values and culture” to Quan. As in previous research (Wang et al. 2010), these two excerpts show customers recognize different cultural resources in medical service.
Second, while glocalized WM and glocalized TCM service experiences represent different philosophies, our informants express concern that the perceived “westernization” of the contemporary TCM service compromises holistic treatment itself. This is where tension emerges, as for example: Today’s TCM has been westernized. …The treatment and prescription are almost disease based and organ based. Doctors prescribe for the disease or symptom without considering the holistic health. The consultations time is quite short and TCM doctors’ practices become efficiency oriented now. Extremely pursuing the efficiency, they don’t drain their brain to create the therapies by themselves based on the patient’ patterns anymore but rely on the patent prescriptions that are symptoms based. (Ma, 72, Female)
Informants experience that the TCM doctors increasingly offer a standardized, efficiency focused, “symptom-based prescription” and they decreasingly invest “themselves,” in creating patient-centered, holistic therapies. Previous medical research has noted this tension between the expectation or desire for high level care and commodified episodic care as a source of increasing dissatisfaction with Chinese healthcare workers (Tucker et al. 2015). We note a shift from treatments emergent from resource integration practices between specific practitioners and specific customers based in TCM philosophy to an “efficiency oriented,” evidence-based resource integration practice based in WM philosophy. While our informants have recourse to both WM and TCM, they form discrepant interpretations of their experiences (Wang et al. 2010). Next, we will elaborate more specific tensions that the customers experience with the culturally based resources in healthcare service.
Tension 2: Interaction Styles as a Cultural Resource
Seiders et al. (2015) characterize interaction in provider–customer healthcare interactions as giving expert advice, creating provider–customer relationships, clarifying expectations, and motivating customers to become engaged with the service. Service research shows that interpersonal interaction between the healthcare provider and the customer plays an important role in reaching desired health outcomes (Dagger and Sweeney 2007; McColl-Kennedy et al. 2017). One of the benefits of adopting a cultural resource perspective on interaction is to identify how varying expectations and experiences of interaction influence customer experience.
The tension between episodic treatment and instant cure versus persistent engagement and continuous care relates to the duration of interaction and engagement between the customer and service provider (Messinger-Rapport 2004)
Well, in my mind, opposite to WM, the authentic TCM service is not to cure the illness immediately. For me, its effect is incrementally created in a long-term process. In TCM, doctors, patients, and other people including patients’ family should cooperate to pursue the mutual goals. Doctors should follow patients’ conditions and continuously provide diagnoses, treatments, and advices based on the changes. Patients should take great patience and persistence to engage in following the treatment plan, changing the lifestyles, and cultivating healthy habit for long-term benefits.... I will strongly feel proud of myself if my engagement brings good results to my life. (Ling, 35, Female)
As Ling’s comments suggest, persistent engagement versus episodic treatment is related to the tension between medical philosophies focused on holistic health versus episodic disease treatment. Holistic treatment requires integration of knowledge (operant) resources: comprehensive interaction and diagnosis of “patient patterns” with significant long-term investments of resources. TCM doctors should “cooperate” integrating knowledge resources to pursue “mutual goals,” evidently jointly determined. In the expected, historical TCM cultural frame temporal resources are integrated: long-term service interaction and doctor–customer commitment is needed. As Ling describes above, not just customers, but also their families (social resources), should actively commit themselves with “patience and persistence.” In following treatments, skills and knowledge resources are integrated: adjusting “lifestyles and cultivating” habits to balance the body, mind, and spirit.
Our data suggest that lack of consistency in interpersonal interaction is tied to experiences of short-lived results from the episodic WM care. Consistent with our informants’ experience, Berry et al. (2020) critique the overemphasis on treatment over healing in WM culture. A young woman’s narrative expresses a belief that “westernized” TCM pursues temporal “efficiency.” For example, Le says: I didn’t feel the pain shortly after I took the medicine. I guess it was kind of pain killer. The pain came back after several course” (Le, 26, female).
As described in the above excerpts and those presented below, medicine in China seems to have moved toward the classic case-based WM model in which doctors diagnose and prescribe based on epidemiological standards and patients comply. Ironically, collaboration, co-creation, and holistic care have become more common elements in Western medical practice (McColl-Kennedy et al. 2012).
Service research has acknowledged that short consultation times and lack of continuity of care create a threat to the patient–clinician interaction (Berry et al. 2020). Biao experiences this absence of continuity in the TCM culture.
It is hard to find good and cultured TCM doctors in this WM dominant age, let alone getting long-term relationship with TCM doctors. These years, I notice that many senior TCM doctors are often traveling to DY (a place where Biao lives) and see patients on a volunteer basis. It is a very good thing. I have been served in several free clinic events. But the thing is that the [TCM] visiting doctors only come one or two times per year or even only one time for the whole life. It is hard to get continuous service. In TCM, continuity and persistence are the essential for healing…. If you change the TCM doctor all the time, different types of treatments are mixed and you will find it hard to commit yourself into one. It will cause chaos to your health. (Biao, 65, Male)
Implicit in this description is an overall change in healthcare delivery in this “WM dominant age.” Consistent with a WM approach, medical care has been removed from community and relocated to medical centers (Xu and Yang 2009). Moreover, episodic treatment and inconsistency in service relationships characterize an impersonal, evidence-based approach to resource integration in healthcare. According to Biao, it seems the value associated with care is diminished in TCM as “it is hard to commit yourself” into a course of treatment “when different types of treatment are mixed.” Biao refers not just to mixing WM and TCM, but TCM itself. Historical TCM relied on consistent resource integration between persons, a TCM practitioner and a patient, and perhaps her family. Since different TCM doctors might prescribe different patterns of treatment depending upon which imbalances they thought to be primary within the body, mixing practitioners was discouraged.
The tension between standardization vs. patient-centered care relates to the intimacy of interaction
Patient-centered care is emphasized in historical TCM and increasingly the aim of WM medicine in some Western countries (Danaher and Gallan 2016; McColl-Kennedy et al. 2012). However, the Chinese informants experience that patient-centered care is hard to come by as TCM doctors’ service focuses on rapid treatment rather than learning about patients’ personal lives (Tucker et al. 2015). Both younger and elderly informants experience tensions when the TCM practice does not follow the historical TCM focus on customized, patient-centered care. For example, Liang wished to share knowledge, including her “terrible relationship” with her mother-in-law within a TCM service interaction.
I thought it was important for the doctor [TCM doctor] to become informed about my status, so I told her about my feelings and my daily life, including my terrible relationship with my mother-in-law. The doctor seemed very impatient and stopped the conversation, criticizing that “the reason you come here is your disease. My duty is to cure your disease. I don’t have time to listen to your story.” I felt very embarrassed (尴尬, gan ga) and disappointed (失望, shi wang) at that moment. (Liang, 27, Female)
Liang approached the service experience dialogically, that is, expecting the doctor “to become informed about my status” as in TCM and to allocate temporal resources to this activity. She shares social relationship information because she expects this information to be integrated into treatment. But operating in terms of a glocalized service model, the doctor rejects this invitation to dialog, limiting the focus to Liang’s physical symptoms and a “cure” for her disease, citing her own busy schedule.
We also notice Liang experienced a diminution in emotional resources, feeling “embarrassed and disappointed” she says. She suffered a loss of face from the doctor’s rejection. In sum, expectations of a communicative integration of resources are thwarted and the glocalized service is negatively valued relative to Lian’s culturally hybrid service expectations.
Tension 3: Material, Signs, and Symbols as a Cultural Resource
Customers’ experiences of tensions in material, signs, and symbols as a cultural resource relate to differences between those used in WM and TCM. While signs and symbols in service have been studied from the communication perspective, such as people’s experiences of hospitals (Hamed et al. 2019; Vigolo et al. 2020) or telehealth (Isautier et al. 2020), the cultural aspects are less discussed. Tourism service research has paid more attention to cultural aspects of materials, signs, and symbols (Chronis et al. 2012). For example, these researchers recognize that artefacts, signs, and symbols often encode both explicit and hidden meanings that provide cues for appropriate expectations and for making sense of service experiences.
The tension between device and laboratory tests vs. human touch and harmony in diagnosis relates to how much the diagnosis is based on personal touch and sensing. In this study, human touch refers to human interaction that creates experience of physical touch or interpersonal interaction (Berry 2019). Sensory experience is understudied in marketing as in the social sciences generally. Still, research shows that human touch is a culturally variable resource (Midorikawa and Niitsuma 2018) and that sensory cues affect product experience (Krishna and Morrin 2008). Studies in WM healthcare show that the use of human touch improves customer experience and health outcomes (Hyde and Boaden 2008). Before the 1950s, TCM diagnosis was based almost entirely on personal touch and sensing (Hesketh and Zhu 1997; Xu and Yang 2009). In fact, inspection, listening, smelling, inquiring, and palpation (pulse) are the key diagnostic practices in TCM (TCM 2009). But the evidence-based WM model emphasizes technical diagnosis (Daly 2005; Knaapen 2014). In China, both WM and TCM strongly embed service interaction in diagnostic material devices and standardized laboratory tests.
Informants experience little humane interaction and sharing in WM treatment. In contrast, they claim that human touch is foundational to authentic TCM diagnostic practices. The presence or absence of small gestures may prime expectations of this TCM element in healthcare (Wang et al. 2010), such as “The TCM doctor’s wife gave me a glass of warm water and also invited me to sit down” (Fei, 21, male). Ma (72) has experiences of TCM from earlier years, and contrasts at length the human warmth she associates with historical TCM service and the coldness in the WM service. There were no machines or well-advanced apparatus supporting diagnosis, and the diagnosis purely depended on Langzhongs’ experience and judgement and it was based on human to human interaction - not human to machines that in WM service only produces coldness (冷冰冰, leng bing bing). I could feel the body warmth and emotional warmth from Chen Langzhong when he diagnosed me by looking, listening-smelling, asking, touching and pulse/palpation. (Ma, 72, Female)
Ma suggests specific elements of diagnostic practice that produced particular resources (TCM 2009) and also induced emotional responses in customers. In this text, Ma refers to warmth and coldness, which in historical Chinese epidemiology are not merely ambient conditions but refer to bodily resources with health implications. Too much of one resource or the other induces a lack of harmony.
The cultural tension that emerged from our analysis is that because of the reliance on diagnostic testing, informants’ experience being treated as a medical “case” by emotionless “robots” (metaphors of practitioners) in WM hospitals and clinics. Informants’ narratives reveal that TCM service also favor machine-based diagnosis versus human touch to integrate knowledge resources. In Fu’s case, a doctor employs diagnostic tests consistent with WM practice, although he also engages in a “quick” physical palpation consistent with historical TCM. Fu continues, I learn that the introduction of WM diagnosis technology can increase the precision and efficiency in TCM diagnosis. But I just don’t like to be treated in such a cultureless way. And I really doubt whether it could bring more accurate diagnosis, since … patients’ lifestyles and personal information…are important in TCM diagnosis and only can be extracted by conversation… After I went back to the doctor with the results, he reviewed the results, gave some comments and prescribed to me. It looks very efficient but cultureless. …After a quick palpation and observation, he wrote on a form and then finally talked to me. He told me to do B ultrasound, blood test, and a few of other tests that I thought would only be provided by WM doctors. I noticed that what the doctor told me was almost the same with what he told to other patients and what he did for me was almost the same with how he treated other patients. (Fu, 52, Female)
Fu indicates the doctor implicitly rejects the legitimacy of human touch as a knowledge resource and instead relies on technology and laboratory tests. Her statement that he “didn’t respond to me too much,” suggests she expected a “conversation” that is interaction concerning the context of her illness. Her remark that “what the doctor told me and others was almost the same…” is consistent with an impersonal standardized evidence-based approach to medicine but inconsistent with expectations for personalized interaction and treatment in historical TCM.
The tension between a clinical vs. harmonious environment refers to a holistic evaluation of the sensory cues in the healthcare environment. Service research acknowledges that the service environment and its many elements (e.g., odors) affect customers’ service experiences (Girard et al. 2019). On the other hand, unfamiliar odors, décor, clinical attire, and other material elements of the service environment can detract from customer experience. The material environments, colors and odors typical of historical TCM, are different in glocalized TCM. Some informants assert that the site of TCM service (e.g., TCM clinics) should be a place of peace, producing harmony. Referring back to the opening quote of the paper, informants experienced both WM hospitals and TCM medical sites with their functionalist design, for example, dull, white walls, the absence of calligraphy, as anxiety producing (the lack of expected material, signs and symbols, the noise, and the emotional outpourings of other patients). Now, all the WM and TCM doctors wear white coats. In the hospital, I cannot distinguish TCM doctors from WM doctors. I don’t think TCM doctors should wear the white coats. It is not fit to TCM’s culture. White and black are two inauspicious colors. They are the color of mourning and associated with death and used predominantly in funerals in Chinese culture. So I feel quite upset when I face the doctors with white coats. It is horrible to visit TCM doctors. (Hui, 27, Female)
Pleasantness, safety, and convenience of the physical environment diminish stress (Parish, Berry and Lam 2008). By contrast, from this excerpt, we see that the presence of some and the absence of other material resources increase customers’ tension. Examples of problematic resources in the TCM clinics include white coats and white walls that may evoke associations of death and mourning; the odor of disinfectant; and the absence of artwork, not to mention patient screams, for example. Various aspects of the doctors’ demeanor, for example, “always wearing frowns,” also produce a conflict between expectations of the “relaxed” TCM experience and “hustling” reality that is “horrible.” To sum it up, excerpts indicate that elements of both the non-human and human resources available in the TCM hospitals conflict with informants’ expectations based on historical TCM cultural schemas for practice and interpretation.
The tension between standardized pre-packed medicines vs. personalized medicine once again evokes a foundational cultural tension between epidemiologies. Historically, TCM medicines were customized to the practitioner’s diagnosis, the customer’s problems including social context, and season. A doctor explains this three-way interaction between three resources to Huang: the efficacy of medicine, the customer’s body, and the ambient environment. An excerpt drawn from a TCM treatment encounter expresses the expectation for personalized and contextual medicine based on mutual sense-making: I also noticed that for the same problem, doctor Xue gave me different types of prescriptions at different times. I asked the doctor ‘why you prescribed X herb with X mg last time but this time you gave me X herb with a double amount? Did you make a mistake?’ He explained to me that my body status was changing and the season was changing so that my body can handle more X herb right now, and my problems could be solved quickly with this amount of X. You see, the treatment is quite contextualized. I doubt that if I go to WM doctors, they will always give same medicines for this symptom. I like to visit this TCM doctor. (Huang, 49, Female)
From a cultural resource perspective whether in WM or historical TCM practice, medicine is linked to a distinctive system of meaning. According to TCM theory, five elements (gold, wood, water, fire, and soil) construct the body (Jia, Zhao and Liang 2009). If someone is diagnosed with a relative lack of gold, two TCM doctors may give different prescriptions (Hui-Chu et al. 2012). One might supplement gold; the other might seek to diminish the presence of the other four elements. Mixing courses of treatment could be dangerous. If someone has multiple problems, the prescriptions given by different doctors may focus on different priorities depending upon which problem is thought to be the major one. In other words, resource integration in the TCM system is contingent rather than formulaic. Treatment consistency relies on ongoing personalized diagnosis rather than universalizing standards.
TCM prescriptions were not only patient specific historically, but medicine preparation and decocting methods varied in time and circumstance as Ma indicates in this excerpt: “But now many patent medicines have been prescribed and consumed just based on symptoms without any differentiation in seasons and time” (Ma, 72, female). Informants like Ma doubt the precision, accuracy, and effectiveness of “westernized” medicine that reflects the standardization built into Western pharmaceutical knowledge. She says, I also notice that the bags that are used by the TCM institutes to pack the decoction are quite similar without any personal information and labels. Most of the decoctions are in a same color, dark brown. So I think there must be a high risk of mistakenly mixing the medicine bags belonging to different patients or treating different diseases (Ma, 72, female).
Thus, standardized Chinese patent medicines as Ma describes them thus seem to represent a hybrid, glocalized product. They are neither customized to the patient’s circumstances as in historical TCM, nor fast acting, acute symptomatic treatments as in WM. Similarly, Ma also draws attention to devaluing of customers’ knowledge as customers role in preparing their “modernized” medicines is reduced relative to historical TCM medicines. TCM institutes provide the service of decocting medicines with big machines to industrially process and extract the medicines and pack the soup with sealed bags. So the patients don’t need to cook the medicine by themselves every day. They just need to take a bag of soup, warm it, cut the bag and drink it. It is very convenient. But I think the effect of medicines must be diminished. According to TCM the herb mixture needs to be decocted with cultured and subtle (讲究的, jiang jiu) methods for the effect. The herbs should be put into the pot orderly according to their natures, and the duration and degree of heating need to be controlled in a right way (Ma, 72 female).
As one of our more elderly informants, Ma’s text reveals first-hand experience of practice with traditional Chinese medical remedies. Medicines should be prepared “every day”; differentiated with regard to season and time; ingredients should be added in an “orderly” fashion; and time and temperature need to be controlled. In criticizing the uniform color of industrially processed Chinese medicines, she also indicates that color is a sensory indicator that differentiates one decoction from another. She experiences the uniform color as potentially misleading and “without any personal information.” These medicines frustrate sense-making. Finally, and this is key, the customer or her caregivers (e.g., family members) should take an active and knowledgeable role in the preparation of medicine. Through decoction, which is clearly both a resource integrating and sense-making practice, historically TCM customers literally integrated material resources employed in their overall healthcare. Although like Fu above, Ma recounts that the glocalized medicines are “convenient” or time saving, but they disempower the customer and her family from participation in treatment. Glocalization of medicines implies a “compliant” treatment recipient as in WM historically (Trostle 1988).
Standardization has been one of the aims in globalized marketing (Kotler 1986) as well as in evidence-based medicine. Standardization in evidence-based medicine aims to reinforce reassurance and certainty (Daly 2005; Knaapen 2014). However, customers’ experiences of standardization in TCM and WM produce tensions, not certainty and reassurance.
To summarize, the culturally distinct interaction styles and material cultural resources are empirically observable in informants’ narrative accounts of experiential tensions. Customers’ experiences of specific resources (medical philosophies, interaction styles, materials, signs, and symbols) match or conflict with their service expectations. Although they are discussed separately above, caregivers and patients assemble and combine the culturally distinct interaction styles and materials, signs, and symbols to produce customers’ holistic service experiences. As we have argued, incompatibilities and tensions between these resources’ underlying cultural meanings lead to tensions between service expectations and experiences. It is also implicit that glocalization is a process that changes with time. Older customers refer to their earlier experiences when TCM was still less inspired by WM.
Discussion
The focus of this study is how the integration of cultural resources may create conflict in customers’ service experiences. Responding to calls in recent service research, the analysis shows how resources emerge as they “are not static and scarce but becoming and contextual” (Koskela-Huotari et al. 2018, 384) and are combined in service (Bruce et al., 2019). Furthermore, building on previous research (Edvardsson and Tronvoll 2013), the paper shows that these specific cultural resources emerge and are integrated in service system relationships. In addition, this article complements meso-level approaches to experience as it takes a phenomenological approach to customers’ experiences of culturally specific resources. Overall, this study replies to the call for theorizing the impact of cultural context on service experiences (Akaka et al. 2015; Wilden et al. 2017).
This study provides more specific guidance organized around the general concepts of operand and operant resources for facilitating positive customer experiences than the calls for “respect” or “better communications” articulated in the healthcare literature. It shows that cultural resource integration leads to (dis)satisfaction with respect to expectations versus service experiences in Chinese healthcare. It may be that cultural resource mismatches similar to those found here would help explain unsatisfactory service experiences among ethnic minority and immigrant healthcare customers that are frequently attributed to disrespect or poor communication (Degni et al. 2014; Gould and Gould 2003; Main 2016). We expand on these contributions below.
Culturally Specific Resources Emerge in Customers’ Experiences
The first theoretical contribution of this article is to show that while culturally specific resources of service are embedded in service systems, their salience emerges through resource integration in customers’ experiences. Our perspective on culturally specific resources builds on prior research in S-D logic, citing Peters et al. (2014), that resources “are not, they become” and emerge out of the interaction of people, materials (operand resources), and culture (operant resources). Thus, a material artefact like a white lab coat or a packet of pre-prepared herbal medicine is not a resource “per se,” it emerges as a specific kind of resource when it is used and experienced within a service. Further, a new material (operand) resource, can affect the perceived “supply” of an intangible (operant) resource (Vargo, Akaka and Wieland 2020), as when diagnostic machinery renders TCM diagnosis more time efficient, but less interpersonally rewarding. The reverse may also be true as when scientific knowledge (operant resource) certifies the active agent in TCM herbal concoctions (operand resource) (Zhang et al. 2019).
Past service research, and especially S-D logic, has emphasized the phenomenological approach to customers’ value experiences. Similarly, in applying the phenomenological approach, we emphasize that from a customer’s perspective, the cultural specificity of resources emerges as customers make sense of resources within specific service experiences; thus, a pre-packaged herbal remedy conflicts with a cultural rendering of a “traditional” herbal remedy in a Chinese service context. Or the presence of a white coat conflicts with the image of a doctor in a TCM clinic but not in a WM clinic. The emergent approach to resource integration adopted here contrasts with a script-based approach to service. The script-based approach suggests interaction styles, material, signs, symbols etc. are resources “per se” for service even if customers do not use, lack experience of a specific resource, or resist it (Victorino et al. 2012).
Understanding of culturally specific resources as an experience responds to a call to investigate cultural context in service research empirically (Akaka et al. 2015) and builds on the discussion of value as customers’ subjective sense-making in a service context (Helkkula et al. 2012; Patrício et al. 2011). Service research has not generally identified how culture affects focal phenomena in service, even if the value of a cultural approach in medical service was recognized long ago (Kleinman, Eisenberg and Good 1978). Thus, according to our study, even if every customer individually calls upon culturally specific resources in deriving value from experience, the cultural context is “located in collective representations,” (Shweder and Levine 1984) as part of a heterogeneous “cultural pool” of resources (Pelto and Pelto 1975). This merging of meso and phenomenological perspectives helps bring culturally specific resource use to the center of analysis and demonstrates resources’ role in understanding culturally distinctive service experiences, that is, why some customers react negatively to the “same” service as a result in differences in resource endowments. Finally, understanding service systems as cultural systems is consistent with understanding operant resources as an interactive strategic resource. Consequently, operationalizing service systems as cultural systems means developing specific relational competencies that involve cultural market sensing and the ability to synthetize this cultural market sensing into customer knowledge, which can then be used to deliver improved market offerings more effectively and efficiently (Madhavaram and Hunt 2008).
Tensions in Customers’ Experiences of Culturally Specific Resources
Consistent with the dynamic and holistic understanding of culture (Arnould and Thompson 2005; 2018), we understand that customers embody and make sense of overlapping and potentially conflicting cultural resources in their interactions with service providers. Thus, the second contribution of this article is to demonstrate how the integration of culturally specific resources from two glocalized services causes tensions in customers’ service experiences. We find that customers’ service expectations and experiences in China reflect a distinctive glocalized agglomeration of culturally shaped understandings of health, illness, and treatment. In showing thematic consistency across informants, our analysis moves between the phenomenological level of service experiences to analyze the contradictions that exist within the current culture of the healthcare service system in southwestern China. The cultural tensions between practices built into the WM and TCM schema add a dynamic systemic aspect to how sayings and doings are implemented in service practices, and how experience is interpreted and valued. Our results are consistent with previous research in medical sociology that has pointed out the limitations of episode focused, biomedical Western practices across culturally distinct systems of health and healing (Chalmers and Omer-Hashi 2002).
Based on the literature review and empirical findings, this study demonstrates that even if WM was originally a globalizing force within China, and TCM a local healthcare system, currently the consumption field of Chinese healthcare service is a state mandated intentional glocalization of both WM and TCM. Thus, healthcare has become a glocalized “contact zone” (Pratt 2007, 8), a service site of ongoing encounters between glocalized WM and TCM: interaction styles (active vs compliant patients); materials (e.g., pre-packaged “Chinese” medicines); diagnostic symbols (e.g., diagnostic tests vs palpitation); and signs (lab coat-wearing TCM doctors). The meanings of these cultural cues, and consequently the appreciation of glocalized medical service, appear to be in flux and with indeterminate consequences for customers’ service experiences. Understanding cultural tensions in a glocalized world is essential for service research as specific cultural contexts and the specific cultural resources in play affect not only customers’ expectations and experiences of service but also their sense-making of value (Cayla and Bhatnagar 2017).
Managerial Implications Culture-comparative Resource Framework
Steps of the culture-comparative resource integration framework.
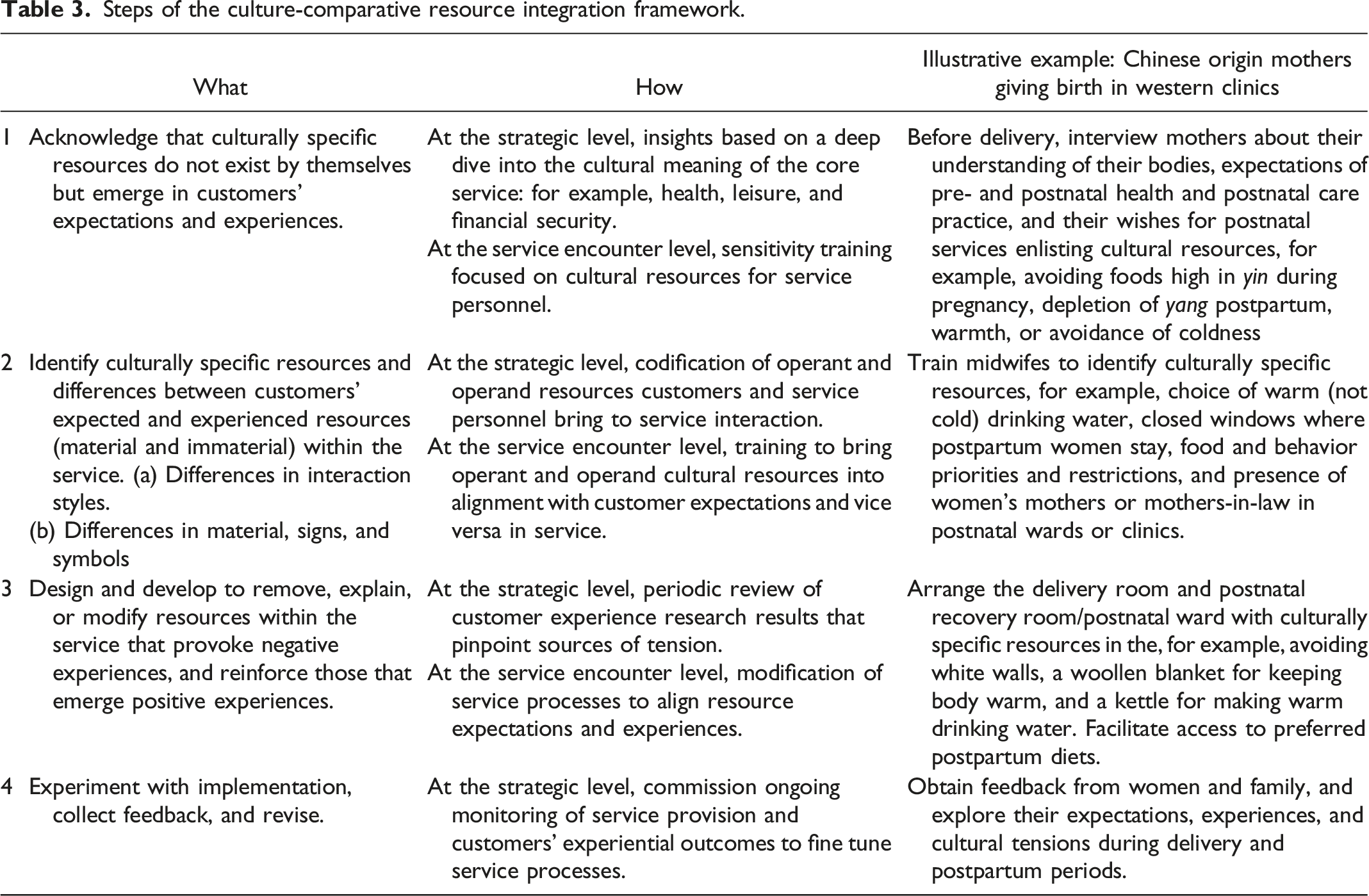
The first step is a mindset shift for service providers who operate within culturally complex environments. Service providers should recognize that even if service is increasingly glocalized, service is embedded in customers’ culturally specific service expectations and experiences. As an example, Table 3 illustrates how service providers could alleviate cultural tensions Chinese mothers might experience giving birth in western clinics (Ding et al. 2018; Lau 2012). A further example could be a Franco-Belgian, all-inclusive, holiday resort chain (Réau 2007) that has launched in China. Cultural resources core to Club Med and suitable to middle class Europeans such as inclusivity, conviviality, exercise, skill acquisition, family relations, and friendly relationships with service providers may not suit middle class Chinese. Table 3 provides guidance for the birthing example.
In the second step, service providers should identify culturally specific resources that emerge in customers’ expectations and experiences to identify differences between customers’ expected and experienced resources. Table 3 provides guidance for the birthing example. Consistent with prior S-D logic research on resource emergence (Koskela-Huotari et al. 2018), our research would suggest that Club Med identifies markers of exclusivity and luxury, as well as expressions of face, hierarchy, and deference situationally relevant to Chinese. Club Med uses terms GO, “good organizers” for service providers and GM, “good members,” for customers, respectively. These terms are embedded in the Franco-Belgian culture.
The third step in culture-comparative resource analysis encourages service providers to take a systemic approach to the service and delivery process in which resources are aligned. To alleviate negative experiences, culturally divergent resources should be aligned to facilitate customers’ positive experiences. Table 3 provides guidance for the birthing example. Additionally, for Club Med, this probably means removing rustic, self-service components of resorts along with the expectation of 5-day stays and collective conviviality. Including stereotypical representations of “French culture” and accommodating short-term stays is advisable. In case changes cannot be made, customers should be informed and motivated. For example, conventional marketing communication tools, such as looped videos playing in front line environments, could be used to allay potential tensions between customers’ culturally divergent expectations and experiences.
Fourth, as glocalization is a process, it is important to experiment with aligning resources, to collect feedback on expectations and experiences, and to revise culturally specific resources cued and mobilized in the service environment.
Future Research
S-D logic has called for more understanding of how operant and operand resources emerge within service (Jaakkola et al. 2015; Koskela-Huotari et al. 2018). We encourage future research to extend the culture-comparative resource framework to different services and cultural settings. For example, service research in international banking, transportation, insurance, and ecotourism has recognized tensions between customers’ expected local service interaction style versus globally standardized service interaction style (Lin, Nguyen and Lin 2013; Xu et al. 2014). These considerations raise the following questions: What culturally specific resources emerge in customers’ expectations and experiences in different types of service and particular glocalized settings? What specific cues in the service environment lead to the emergence of culturally specific resources? Which sources of cultural tensions reside in operant (skills, competences, and interaction styles) and which in operand (material) resources in different glocalized service contexts? What emergent culturally specific resources cause experiential tensions? When do tensions in customers’ expectations and experiences relate to cultural differences in customer characteristics such as age and gender role, or ethnicity?
Our discovery oriented, empirical study did not examine the downstream consequences of the tensions caused by the cultural misalignment between expectations versus experiences. Future research might ask, how do consumers’ process tensions in their experiences of cultural resources? Aiming to quantify causal relationships between specific glocalized operant and operand resources and customers’ service expectations and experiences would be of value, research may ask: what effects do customers’ experienced tensions of resources have upon customer experienced value? When are the effects of service provider interventions on experienced cultural resource tensions?
Conclusion
This paper adds to our theoretical understanding of customers’ active role in emergence of resources within service. This has been identified as a developing area in S-D logic. In specific, we contribute to S-D logic research by showing that resources emerge phenomenologically through resource integration in customers’ expectations and experiences. Our study also shows that these resources are culturally specific. It further shows that in glocalized service, discrepancies between customers’ expectations and experiences of cultural resources (interaction styles, materials, signs, and symbols) cause tensions that reduce customers’ positive service experiences. The cultures that underly a glocalized service system can be mobilized as relational operant and operand resources. However, disorderly operationalization of the glocalized cultural resources that underlie a service system will disengage customers from the service and lead to tensions and dissatisfactory service experiences. As operant (immaterial) and operand (material) resources intertwine with each other in practice, the resource integration construct provides theoretical language to analyze resource integration in customers’ glocalized service experiences. We encourage further research to study expected versus experienced culturally specific resources in different types of services, and how to design service to remove, explain, or modify culturally specific resources within service that facilitate positive customer experiences.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
![]()