
Abstract
Self-tracking technologies (STTs) in the form of smart devices and mobile applications enable consumers to monitor, analyze, and interpret personal performance data on health and physical or financial well-being. As a result of self-tracking, consumers are not only expected to check their personal performance more actively but also to implement service professionals’ advice to improve their well-being more accurately. Despite the growing popularity of STTs, empirical evidence on the extent to which STT use enhances advice compliance remains scant. A field experiment with 538 participants in a health-care setting suggests that STT use does not increase advice compliance per se. Rather, the effectiveness of STTs depends on consumers’ self-efficacy. For consumers low in self-efficacy, STT use can even undermine advice compliance. A lab experiment with 831 participants replicates and generalizes the findings to a nonmedical professional service (i.e., fitness training). As assessments of self-efficacy might be difficult in practice, service providers in health care can use consumers’ body mass index as an easy-to-measure proxy to predict STT effectiveness. Finally, the lab experiment also identifies perceived empowerment and personalization as psychological mechanisms mediating the influence of STT use on advice compliance.
Keywords
Consumers increasingly engage in and act on personal analytics to realize a better quality of life (Crawford, Lingel, and Karppi 2015). This movement toward the Quantified Self goes hand in hand with the rapid development and diffusion of self-tracking technologies (STTs): smart devices and applications that seek to support consumers’ self-improvement efforts by enabling them to collect, monitor, and better understand personal performance data. Smart wearables such as wristbands (e.g., Fitbit Charge 3 or Garmin Vivosmart 4), smart rings (e.g., Jakcom or Motiv), and smartphone apps (e.g., MyFitnessPal or Mint) allow consumers to monitor well-being parameters (e.g., weight or financial situation), activities (e.g., exercise or spending), and health indicators (e.g., blood pressure or blood sugar). Reflecting their growing popularity, the global market for STTs is estimated to reach US$71.9 billion by 2022 (BCC Research 2017).
Literature on self-tracking identifies enhanced self-knowledge as a major achievement of STT use. A better understanding of their actions and the consequences resulting from those actions enhances consumers’ self-improvement initiatives (Sharon 2017). Therefore, STTs are of particular interest in professional service contexts where outcomes depend not only on the advice of an expert but particularly on customers’ advice compliance in terms of knowledgeably implementing the expert recommendations (Dellande, Gilly, and Graham 2004). Eliciting compliance with the advice of professional service providers such as lawyers, physicians, or tax accountants is hence critical to safeguard customer well-being through desired service outcomes such as debt reduction, recovery from illness, or weight loss.
On the one hand, improved self-knowledge acquired through STT use may emancipate consumers from service experts’ recommendations, thereby reducing advice compliance. On the other hand, STT use may increase advice compliance as consumers develop into more competent coproducers of a professional service. Apart from resolving this seeming contradiction, two specific reasons can be given for exploring the effect of STT use on advice compliance in a professional service setting. First, compliance with expert advice is notoriously low in many professional service industries, especially in health-care and financial advisory services (Guo et al. 2013). If left unaddressed, such noncompliance may even endanger consumers’ health conditions (Seiders et al. 2015) and economic well-being (Mende and Doorn 2015). Second, the market for professional services is rapidly growing, spanning a broad spectrum from actuaries to personal trainers to relationship counselors (Businesswire 2019). As customer demand may exceed service capacity in this market, there is a dire need to know how smart technology can support the efficiency of professional service providers.
The current research aims to empirically examine the ramifications of STT use on advice compliance. Analyzing STT use in a field experiment with 538 customers in a health-care setting (i.e., diabetic care) provides an opportunity to profoundly examine STT effectiveness in a real-world setting. Additionally, a lab experiment with 831 consumers in a well-being setting (i.e., fitness training) replicates and extends the findings of the field experiment. Following recent research in the domain of self-tracking (e.g., Crawford, Lingel, and Karppi 2015; Pantzar and Ruckenstein 2015), we differentiate between standalone STTs and STTs with social network augmentation. Standalone STTs seek to empower consumers to independently measure, understand, and react to important performance or well-being indicators (e.g., the Accu-Chek Aviva Expert blood glucose meter for diabetes self-management; Roche 2019). Network augmentation, as an additional feature, offers STT users supplementary guidance through social mechanisms such as remote support from relevant others or benchmarking their own progress against peers (e.g., the Fitbit Charge 3 peer benchmarking and community; Fitbit 2019).
Overall, our investigation of the effects of STT use on advice compliance contributes to several literature streams. First, we add to research that has explored varying approaches for improving customer adherence to expert recommendations (Guo et al. 2013; Seiders et al. 2015). While prior studies highlight positive effects of specific service provider characteristics such as expertise (Dellande, Gilly, and Graham 2004), the chosen communication approach (Seiders et al. 2015), organizational socialization (Guo et al. 2013), or customer positivity (Gallan et al. 2013), insights into the role of STTs for increasing advice compliance remain scant. This lack of insights is surprising in light of the increasing diffusion of STTs in everyday life.
Second, building on previous literature on the role of individual differences in service technology use (e.g., Blut, Wang, and Schoefer 2016; Meuter et al. 2005; Simon and Usunier 2007), we theorize and provide evidence for the role of self-efficacy. This major psychological trait determines and moderates STTs’ effectiveness in enhancing compliance with expert advice. Specifically, we find that STT use does not increase advice compliance per se: for low self-efficacy consumers, who lack confidence in their abilities to undertake recommended actions, STT use can even decrease rather than increase advice compliance.
We further test whether customers’ body mass index (BMI) may serve as an easy-to-measure, physiological proxy that determines whether STT use will effectively increase advice compliance. Our results indeed show that BMI has an effect pattern similar to self-efficacy. This finding adds to the emerging stream of marketing research on physiological traits as determinants of consumer behavior (e.g., Aspara and van den Bergh 2014; Nepomuceno et al. 2016). Taken together, we uncover a potentially harmful effect of STT use for a specific segment of consumers (i.e., low in self-efficacy and high BMI). This way, our findings also contribute to transformative service research with respect to the dark sides of service technologies and the special attention that should be paid to vulnerable consumer groups (Ostrom et al. 2015).
Finally, we shed light on the underlying mechanisms through which STT use influences advice compliance. Following literature on self-tracking (Bode and Kristensen 2016; Crawford, Lingel, and Karppi 2015), we investigate perceived empowerment (i.e., customers’ competence and autonomy to make their own decisions) and perceived personalization (i.e., the fit between customers’ needs and expert recommendations) as mediators between STT use and advice compliance. We find evidence for both mediating mechanisms, where the path via perceived personalization is stronger when compared with the path via perceived empowerment. These insights complement seminal work on the determinants of advice compliance (Camacho, De Jong, and Stremersch 2014; Prigge et al. 2015).
Conceptual Background
STTs
With the emergence of the Quantified Self-movement—an international community striving for “self-knowledge through numbers” (Wolf 2009)—academic research has devoted increasing interest to the self-tracking concept (e.g., Bode and Kristensen 2016; Crawford, Lingel, and Karppi 2015; Kristensen and Ruckenstein 2018). Self-tracking broadly encompasses self-monitoring practices of any kind, collecting and analyzing biological, physical, behavioral, or environmental information with the aim to improve self-knowledge and ultimately an individual’s well-being in terms of overall quality of life (Crawford, Lingel, and Karppi 2015).
The mounting popularity of self-tracking is fueled by the rapid development and diffusion of STTs such as smart devices, wearable sensors, and mobile applications that collect and assess data concerning a large array of bodily functions and behavioral activities (Sharon 2017). Importantly, STTs not only permit accurate data collection but also calculate specific performance indicators and produce graphs and tables to visualize complex phenomena like sleep patterns or blood sugar levels (Pantzar and Ruckenstein 2015).
In line with existing literature on self-tracking, we distinguish between standalone and network-augmented STTs. Standalone STTs require consumers to engage in self-tracking practices more or less independently, as they do not promote social interactions with experts or peer consumers. Standalone STTs thus delegate full responsibility for self-tracking and self-improvement to their users (Collier et al. 2014), as they need to autonomously collect, analyze, and interpret personal performance data through STT use. From a professional service provider perspective, standalone STTs may significantly increase the collection of relevant data in-between meetings with customers.
Network-augmented STTs explicitly encourage consumers to distribute personal data via social media platforms, smart applications, and websites to service professionals such as medical experts (Tian et al. 2014), people facing similar challenges (Sharon 2017), or fitness enthusiasts (Marinova et al. 2017). Such network-augmented STTs hence facilitate interactions with a community by, for instance, enabling peer comparisons, offering a platform for exchanging feedback, or jointly deciding courses of action (Pantzar and Ruckenstein 2015). Self-tracking consumers may even agree on penalty and reward systems in case personal goals are (not) met. Overall, network augmentation “adds a social dimension” to the everyday practices of self-tracking and may even turn self-tracking into “a social game” (Bode and Kristensen 2016). Moreover, network augmentation offers professional service providers an alternative means to interact with customers.
To sum up, STTs enable users to collect, monitor, better understand, and ultimately respond to personal performance data. As a result, STTs may generally support consumers’ self-improvement measures. For instance, STT use enhances consumers’ access to self-relevant information and gives them more control over specific life situations (Crawford, Lingel, and Karppi 2015). STTs also conduct “personal analytics” to tailor self-improvement initiatives to individual needs. Nevertheless, critics are concerned that STTs oversimplify complex phenomena such as health (physical and financial), well-being, and mood (Sharon 2017). Concretely formulating self-improvement goals and deciding on activities to realize these goals typically still involve initial encounters with professional service providers such as financial consultants, medical experts, or personal trainers (Seiders et al. 2015). STTs are thus unlikely to fully replace the consultation of service professionals but rather establish a complementary channel of influence for experts. For instance, smart health-care devices may remind consumers to take their medication or adapt the timing of a medication regime to stimulate compliance with medical therapies (Stremersch and Van Dyck 2009).
Advice Compliance and Professional Services
In general terms, compliance refers to “the target acting in accordance with an influence attempt from the source” (Payan and McFarland 2005, p. 72). In more specific terms, advice compliance represents an important outcome of influence strategies in various consumption contexts such as in expert-consumer relationships, product recalls, medical (re)testing, and social goods programs (e.g., Bowman, Heilman, and Seetharaman 2004; Camacho, De Jong, and Stremersch 2014). Fostering advice compliance has been identified as a major challenge to safeguard consumers’ physical and financial well-being (Dellande, Gilly, and Graham 2004; Guo et al. 2013; Seiders et al. 2015; Sweeney, Danaher, and McColl-Kennedy 2015).
A multitude of theoretical models attempt to explain compliance (see also the overview by Moorman and Matulich 1993). One set of models regards compliance as being activated by external cues such as physician-patient communications, marketing communications, or sales efforts of health-care companies (Bowman, Heilman, and Seetharaman 2004). Another set of models focuses on understanding how consumers think and act as recipients of expert advice. The underlying assumption is that advice compliance results predominantly from consumers’ cognitive appraisals, such as their reasoning with regard to health and well-being behaviors.
Our research adopts elements of both theoretical streams. Specifically, STTs provide a rich variety of external cues in the form of specific metrics, visualizations of daily activities, and connections to a relevant community (Bode and Kristensen 2016). These cues may directly stimulate advice compliance. At the same time, STTs are tools that educate users outside the visits to professional service providers and thereby enhance self-knowledge (Crawford, Lingel, and Karppi 2015; Seiders et al. 2015). Hence, STTs may also stimulate compliance through cognitive processes that result from their use. Our conceptual model in Figure 1 thus considers a direct effect and mediated effects of STT use on advice compliance. The Hypotheses Development section details the underpinnings of the conceptual model in the following.
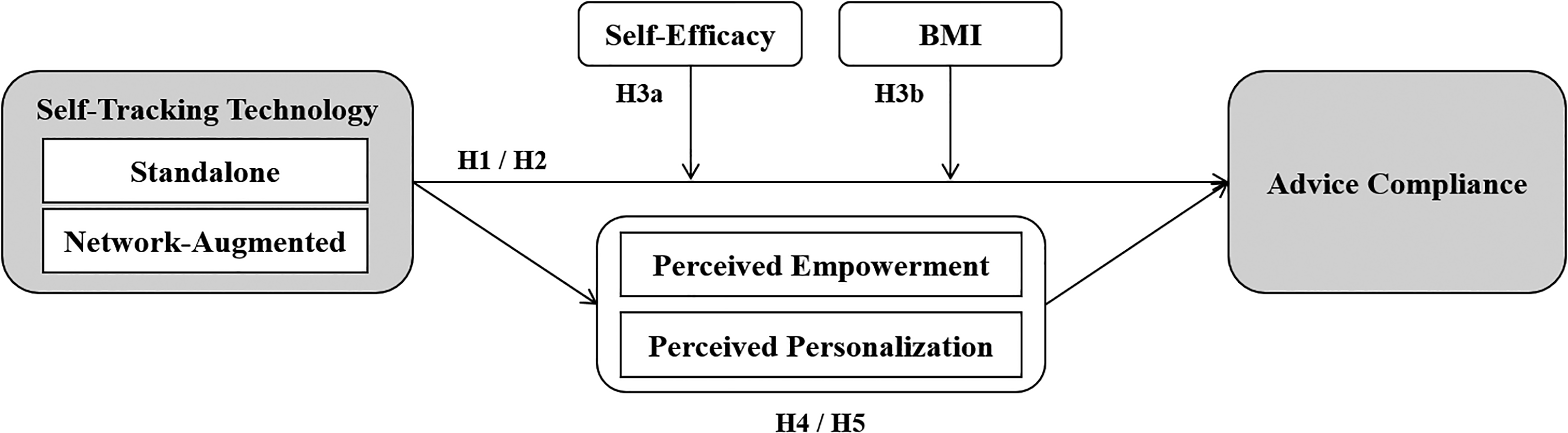
Conceptual model.
Hypotheses Development
STT Use and Advice Compliance
STTs enable consumers to accurately collect personal performance-related data and enhance users’ awareness of their individual condition, their actions, and the consequences resulting from their actions (Bode and Kristensen 2016). By quantifying and visualizing abstract phenomena like health and well-being, STTs give consumers direct access to self-relevant information (Pantzar and Ruckenstein 2015; Sharon 2017). This access to information makes it easier for consumers to manage their performance data in-between or even independent of their meetings with professional service providers. More effective self-coaching results from the greater self-knowledge that consumers acquire from the accurate and convenient measurements, analyses, and interpretations the STTs provide. Better access to self-relevant information improves an individual’s understanding of and motivation to follow expert advice (Camacho, De Jong, and Stremersch 2014).
In sum, STTs support the changing role of consumers from passive recipients of expert advice to better informed cocreators of the service outcome (Crawford, Lingel, and Karppi 2015). Moreover, STT use creates enhanced levels of awareness, which in turn stimulate consumers’ self-initiated efforts to comply with expert advice. Thus, we conjecture that:
Standalone Versus Network-Augmented STTs
An important question for both scholars and practitioners is whether the effectiveness of STTs in enhancing advice compliance depends on the type of STT, that is, whether it embodies network features or not. By sharing personal data with others via STTs with network augmentation, consumers allow increased influence of others—health promoters, friends, and followers—over personal health decisions (Sharon 2017). The additional social control and support mechanisms exerted by relevant others may stimulate advice compliance (DiMatteo 2004). However, health-care studies generally find that factors related to the self, such as personal attitudes or a sense of control over one’s actions, more strongly relate to health behaviors than social factors (Albarracín et al. 2001). For instance, consumers’ beliefs about exercise behavior (e.g., whether workouts improve well-being) and the strength of the cognitive belief structure (e.g., how much improvement can be expected) jointly form a stronger determinant of exercise behavior than the expectations of other people (Hausenblas, Carron, and Mack 1997). In addition, STTs with network augmentation are more likely to provide contradictory information (Camacho, De Jong, and Stremersch 2014). For instance, community members may not mutually agree on the best course of action or may provide advice that repudiates that of service professionals. The associated ambiguity may lower the credibility of initial recommendations and therefore decrease advice compliance. Taken together, we hypothesize:
Moderating Effects
Self-efficacy
We further posit that consumers’ psychological characteristics may affect the impact of STT use on advice compliance. In general, individual differences have been identified as important background variables explaining the adoption of self-service technologies (e.g., Blut, Wang, and Schoefer 2016; Meuter et al. 2005), the display of goal-oriented behaviors (e.g., McKee, Simmers, and Licata 2006), and the likelihood to engage in self-care behaviors (e.g., Zainuddin, Tam, and McCosker 2016). Especially the psychological trait of self-efficacy may moderate the effectiveness of STTs in enhancing consumers’ advice compliance, because a consumer’s confidence in his or her own ability to undertake actions and behaviors is essential in service coproduction (van Beuningen et al. 2009).
Individuals with higher self-efficacy, and hence greater confidence in their own ability to take necessary actions, are more motivated and capable of integrating information from various sources. For instance, high self-efficacy employees have superior abilities to effectively combine and use cues from different stakeholders for clarifying role expectations and improving job performance (Brown, Ganesan, and Challagalla 2001). In addition, previous research generally points to positive effects of technology-based performance feedback on goal-oriented behaviors for high self-efficacy individuals (Karl, O’Leary-Kelly, and Martocchio 1993).
In contrast, consumers with low self-efficacy may rather feel overwhelmed by the insights an STT offers along with expert advice, given their general self-doubt about reaching goals and resulting difficulties to persist with goal-oriented tasks (Gist and Mitchell 1992; Silver, Mitchell, and Gist 1995). According to goal systems theory (e.g., Fishbach and Dhar 2005; Kopetz et al. 2012), the tendency to be overwhelmed by information from various sources leads low self-efficacy consumers to perceive the connection between attending to STT feedback and goal pursuit as weak. Consequently, following up on STT insights is an action unlikely to be selected, and low self-efficacy individuals may cognitively “license” themselves not to comply with the expert advice. In summary, we hypothesize:
BMI
A growing stream of research in marketing uses physiological indicators as predictors for behavior (e.g., Aspara and van den Bergh 2014; Nepomuceno et al. 2016). We follow the idea of this research stream that physiological indicators may serve as proxies for psychological traits. We investigate whether consumers’ BMI can serve as an easy-to-measure, physiological proxy for self-efficacy. BMI is calculated as a person’s weight in kilograms divided by his or her height in meters squared. BMI ratios below 25 suggest normal or underweight, ratios between 25 and 30 suggest overweight, and ratios over 30 suggest obesity (Ikeda, Kang, and Ohtake 2010).
In line with prior empirical studies reporting negative correlations between BMI and self-efficacy (e.g., Ovaskainen et al. 2015; Sacco et al. 2007) and following insights from studies on goal-oriented health behaviors (Romero and Craig 2017), we expect that BMI has a negative moderating influence on the effect of STT use on advice compliance.
1
For instance, higher BMI ratios indicate a lower ability to appreciate the long-term benefits of one’s choices such as the decision to comply with expert recommendations (Ikeda, Kang, and Ohtake 2010). In addition, BMI has been linked to individuals’ general ability for self-disciplined behaviors and conduct, such that lower BMI generally relates to higher self-discipline, while higher BMI relates to lower self-discipline (Lawrence et al. 2012). We therefore expect that STTs are more effective in stimulating advice compliance for consumers with low BMI. Formally:
Mediators
Perceived empowerment
So far, we have considered STTs as external cues providing metrics, visualizations, and network connections to consumers. We now focus on consumers’ cognitive processes that could mediate the effects of STT use on advice compliance. First, STTs support consumers’ information search and knowledge development regarding their personal well-being by monitoring, analyzing, and presenting relevant performance data in a convenient manner (Crawford, Lingel, and Karppi 2015). Self-tracking provides users with a new sense of control over their activities and the resulting consequences because consumers can now quantify and analyze complex phenomena with respect to physical well-being (e.g., heart rate and sleep patterns; Pantzar and Ruckenstein 2015) or financial well-being (e.g., mobile solutions that offer holistic financial overviews; Brüggen et al. 2017). STT use also integrates consumers more tightly into the professional service system (Guo et al. 2013); they become coproducers of the service and are better able to understand the reasons behind expert recommendations, treatment rules, and procedures (Dong, Evans, and Zou 2008).
The described activities of information search, knowledge development, control, and participative decision-making represent central elements of the patient or consumer empowerment construct (Prigge et al. 2015), which reflect the competence and autonomy of consumers to make their own behavioral decisions (Camacho, De Jong, and Stremersch 2014). Empowerment goes beyond coproduction, in that it emphasizes consumers’ information search and knowledge development efforts before and after the actual service encounter (Guo et al. 2013). Moreover, empowerment stresses consumers’ ability to actively debate alternative courses of action with professional service providers given their enhanced understanding of their health or financial situation for instance (Camacho, De Jong, and Stremersch 2014). In turn, empowerment makes people feel and behave more positively and proactively, especially with regard to their well-being (Hui and Bateson 1991). Perceived empowerment has therefore been identified as a major determinant of compliant behaviors as it makes consumers feel more confident in mastering their situations together with service professionals (Prigge et al. 2015; Roth 1994). Especially a better understanding of the reasons behind recommended (health) behaviors and the opportunity to contribute to the decision-making process increase consumers’ willingness to comply with expert advice and decrease reasoned noncompliance (Camacho, De Jong, and Stremersch 2014; Dellande, Gilly, and Graham 2004). In sum, we posit:
Perceived personalization
While standardization refers to a “one-size-fits-all” approach, personalization typically implies that service providers develop and apply tailored strategies for every customer (Bock, Mangus, and Folse 2016; Huang and Rust 2017). STTs collect, analyze, and visualize individual-level data to facilitate consumers’ decisions as to which actions to engage in or which future goals to set (Crawford, Lingel, and Karppi 2015; Pantzar and Ruckenstein 2015). As such, STTs offer—by design—personal analytics that provide a basis to tailor self-improvement initiatives to individual needs. This information-rich personal data environment generated by STTs stands in stark contrast to traditional service encounters that merely consider snapshots of consumers’ personal data at specific points in time (e.g., blood pressure test during visits to the hospital; Schuell 2016). The latter situation does not provide the opportunity for customers to obtain or react to personalized information continuously.
Including personal analytics and performance data in a professional service system is likely to increase the extent to which customers feel that the respective service is tailored to their individual requirements. That is, STTs likely improve the perceived fit between customers’ needs and a professional service. For instance, STTs already play a major role in advancing personalized medicine, using individual health parameters to diagnose a disease and to provide personalized treatments (Swan 2012). In line with this development, seminal research on personalization underscores the central role of customer data for adapting service offerings to individual circumstances and preferences (Murthi and Sarkar 2003). In turn, the perceived personalization should positively influence compliance, as studies comparing personalized and nonpersonalized dietary recommendations (Brug et al. 1996), and personalized and nonpersonalized exercise recommendations (Abele and Gendolla 2007), have demonstrated. We therefore hypothesize:
Field Experiment: Testing the Effect of STT Use on Advice Compliance
Method
Design
To test our hypotheses on the effects of STT use on advice compliance in a real-world setting, we first conducted a field experiment in cooperation with a health-care company. The company introduced STTs to support customers in their daily management of diabetes in-between visits to medical experts. We employed an experimental, between-subjects design with two types of STTs and a control condition without STT. That is, participants were randomly assigned to one of the three groups: control, standalone STT, or network-augmented STT. We conducted two surveys: one immediately before the participants were exposed to the STTs and one 4 months afterward.
Both standalone and network-augmented STTs were presented as a self-tracking system that featured an electronic device and associated software that transferred diabetes data from participants’ blood glucose meter and insulin pump to their computer, smartphone, or tablet. The STTs displayed the results in easy-to-read charts and graphs. In addition, the systems provided the option to explore the results in-depth; a click on specific measurement values provided more information and/or suggestions for further reading. The STTs therefore supported respondents to view and understand their blood glucose and insulin values and to assess their self-care performance. In addition to the depicted features, the network-augmented STT linked participants to an online community to exchange their health data with other customers. They were able to benchmark their results, get recommendations and feedback on their performance, and discuss with peers as well as experts through public or private messages and chats. The discussion forum focused on diverse topics such as diabetes-related diets, nutrition, physical exercises, and therapy. In contrast, the standalone STT did not feature any possibility to connect or get feedback from peers or experts.
Sample and Procedure
The health-care company provided us with the email addresses of 27,727 of its customers. As a first phase of the study, we sent a letter to the full sampling frame. The letter contained an invitation to participate in an online survey, as well as general information on the objective of the study and confidentiality of responses. To encourage participation, we offered respondents a possibility of winning Amazon vouchers worth of 20 Euros in a lottery.
The first-wave online survey was accessible for 2 consecutive weeks. In the survey, participants were first asked about their diabetes treatment. Thereafter, we included background questions (gender, age, and level of education), psychological measures (self-efficacy, customer ability, role clarity, and motivation), BMI measurement questions (height and weight), details on the history and type of diabetes, and the therapy’s form and requirements.
In total, 3,374 individuals participated in this survey, for an initial response rate of 12.2%. These respondents were then randomly assigned to the experimental conditions. Participants in the two STT conditions were provided with access to the respective technologies as well as extensive use instructions. All participants were invited to participate in a follow-up survey 4 months later. The follow-up survey had the same content and structure as the first-wave survey but also included questions about the key dependent variable: advice compliance (see Appendix for the measurement items).
Typical of survey-based experiments in health-care settings (de Graaf et al. 2000; Young, Powers, and Bell 2006), we experienced substantial attrition of participants between the first and second stage of the survey. The final sample consisted of 538 participants (73.6% male, agemean = 53 years, agemin = 14 years, agemax = 87 years) for a participation rate of 21.8% (of participants completing the first-wave survey).
Checking for Attrition Bias
To assess whether nonresponse or attrition bias might influence our results, we first compared the participants who answered both surveys (n = 538) with those who only participated in the first stage (n = 2,836). We conducted our analyses on the study’s focal variables (i.e., self-efficacy and BMI) and on several other variables (e.g., age, education, physical activity, and weight control). We found no significant differences in the mean values of these variables. This provides an indication that attrition or nonresponse bias did not pose a serious threat to the validity of the results of the current study.
To statistically check for attrition bias, we employed Heckman’s procedure. Specifically, a probit regression estimated the participation (i.e., nonattrition) in the second-wave survey (0 = nonparticipation, 1 = participation), for the sample of all first-wave participants (N = 3,374). To account for the possibility that participation depended on the experimental treatment variables or the key moderator variables, we included these variables in the selection equation (i.e., self-efficacy, BMI, and treatment dummies). In addition, covariates of customer ability, role clarity, and motivation were included. Further, we incorporated the following control variables that might also have affected the participant’s likelihood to participate in the second wave of the survey: age, gender, education, mindfulness, self-reported adherence to nutrition plans, frequency of weight control, and frequency of physical activity. This probit regression procedure resulted in an additional control variable for the second-stage regression equation: the inverse Mills ratio, which captures the likelihood of the respondent to have participated in the second wave of the survey. The results show that the inverse Mills ratio did not significantly affect advice compliance (p = .28). We thus conclude that attrition and nonresponse bias do not pose serious threats to the validity of our empirical results.
Measures
To operationalize the constructs of interest, we relied on existing measurement scales and adapted them to our context where necessary. Eight health-care experts helped us refine the scales. Unless otherwise indicated, respondents answered the items on a 7-point Likert-type scale, anchored by totally disagree and totally agree. The items for advice compliance were adapted from the work of Dellande, Gilly, and Graham (2004) and Hausmann (2004). Self-efficacy was measured using a 3-item scale based on Glasgow, McCaul, and Schafer (1987). We calculated participants’ BMI based on the self-reported body height and weight (Caperchione et al. 2008). As covariates, measures for role clarity, customer ability, and motivation were adopted from Dellande, Gilly, and Graham (2004). We also obtained information on participants’ demographics (i.e., gender, age, and education). 2 Appendix offers an overview on the measures and reliabilities.
Results
Confirmatory Factor Analysis and Descriptive Statistics
We first conducted a confirmatory factor analysis to check for convergent and discriminant validity of the constructs. We find that the average variance extracted (AVE) is larger than .50 for all constructs (AVEcompliance = .66, AVEself-efficacy = .60, AVEroleclarity = .61, AVEcustomerability = .77, and AVEmotivation = .59) and exceeds the squared correlation between the constructs. This provides evidence for both convergent and discriminant validity of the constructs (Fornell and Larcker 1981). Table 1 presents descriptive statistics and correlations for the dependent variable, moderators, and covariates. As expected, both self-efficacy (r = .43, p < .001) and BMI (r = −.20, p < .001) significantly correlate with advice compliance as well as with each other (r = −.20, p < .001). While our focus is on the effect of self-efficacy, we also seek to investigate whether BMI can serve as a proxy for the self-efficacy effects. Thus, we include the two constructs as separate moderators in the following analysis.
Descriptive Statistics and Correlations (Field Experiment).
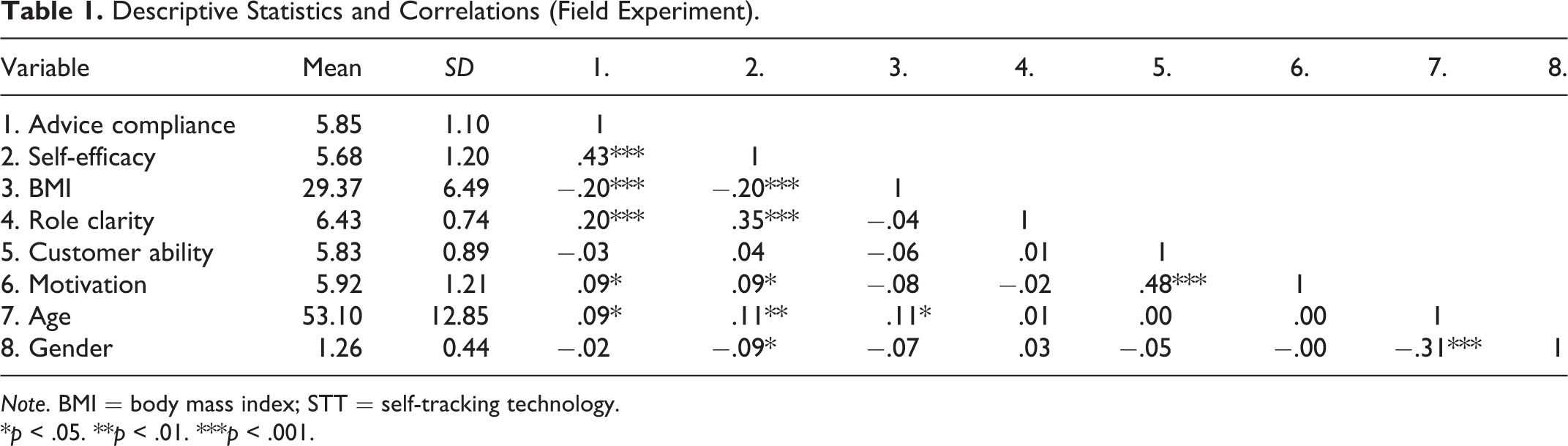
Note. BMI = body mass index; STT = self-tracking technology.
*p < .05. **p < .01. ***p < .001.
Main Effect
We first conducted an analysis of variance (ANOVA) to investigate the effect of general STT use on advice compliance. We find that STT use had no significant main effect on advice compliance, Mstandalone = 5.90, Mnetwork = 5.81, Mcontrol = 5.89; F(2, 535) = .36, p > .10; partial η2 = .001. Interestingly, neither the use of the standalone nor network-augmented STT resulted in higher advice compliance when compared with the control condition without STT (p > .10). Comparing standalone and network-augmented STT use, we also do not find a significant difference (p > .10). Hence, these results do not offer initial support for Hypotheses 1 and 2.
Moderation Effect of Self-Efficacy
We then conducted an analysis of covariance (ANCOVA) to test the moderating influence of self-efficacy. We find a significant interaction effect between STT use and self-efficacy, F(2, 532) = 5.32, p = .01. The effect is substantial, yielding a partial η2 of .02 (i.e., f = .14). Comparing the interaction effects of the two types of STTs with the control condition, we find that the interaction effect is positive and significant for standalone STT use (b = .36, p < .01), as well as positive and significant for network-augmented STT use (b = .18, p = .04). These results support Hypothesis 3a for both standalone and network-augmented STT use, suggesting that higher self-efficacy reinforces the positive effect of standalone and network-augmented STT use on advice compliance. The results also show a cross-over pattern, which explains the lack of a main effect of STT use on advice compliance (Hypothesis 1). Figure 2 categorizes participants into three groups (i.e., low self-efficacy [≤mean − 1 SD], mean self-efficacy, and high self-efficacy [≥mean + 1 SD]) and illustrates that for participants with low self-efficacy, STT use decreases participants’ advice compliance compared with the control condition without STTs. 3
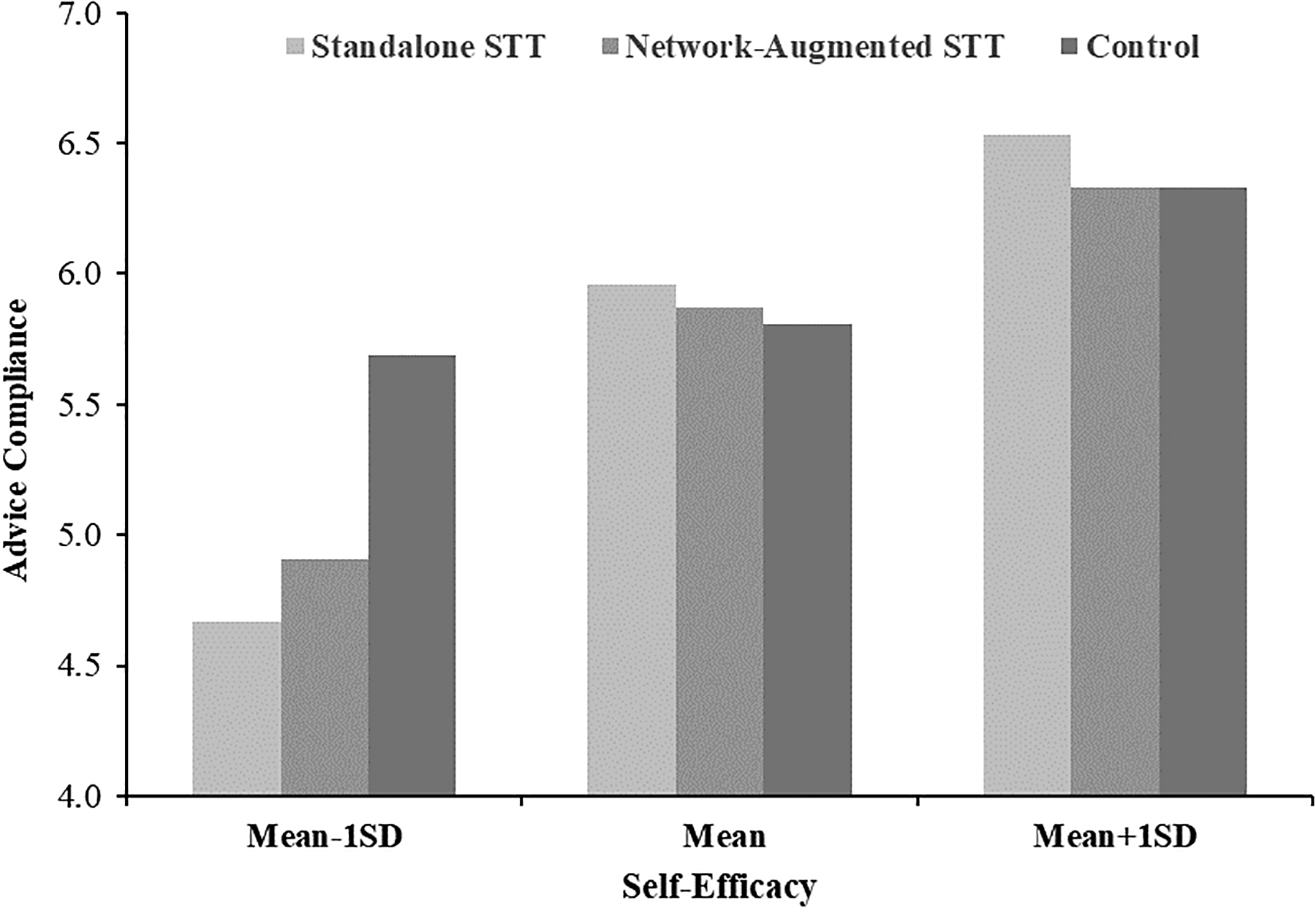
Moderation effect of self-efficacy (field experiment). Displays moderation effect of self-efficacy on advice by categorizing participants in low self-efficacy (≤ mean − 1 SD), mean self-efficacy, and high self-efficacy (≥ mean + 1 SD).
BMI as a Proxy for Self-Efficacy
We conducted an ANCOVA to test the moderating influence of BMI. The ANCOVA reveals a significant interaction effect between the use of both types of STTs and BMI on advice compliance, F(2, 532) = 5.30, p = .01; partial η2 = .02, f = .14. Comparing the two types of STTs with the control condition, we find that the interaction effect is negative and significant for both standalone (b = −.06, p < .01) and network-augmented STT use (b = −.05, p < .01). 4 As the pattern of the moderation effects is similar to the pattern for the moderation effect of self-efficacy, our findings support the notion that the physiological marker of BMI could be applied as a proxy for the psychological measure of self-efficacy. This provides support for Hypothesis 3b.
Standalone Versus Network-Augmented STT Use
Although we do not find a significant difference in the main effects of standalone and network-augmented STT use on advice compliance, we further probe the differences between the two types of STTs for high (i.e., above the mean) and low levels of self-efficacy (i.e., below the mean). We find that among high self-efficacy participants, advice compliance is higher in the case of standalone STT use compared with the use of a network-augmented STT (Mstandalone = 6.41, Mnetwork = 6.13, d = .29, p = .06), whereas among low self-efficacy participants, there is no significant difference between the two (Mstandalone = 5.39, Mnetwork = 5.42, d = .02, p > .10). These findings partially support Hypothesis 2, suggesting that the effect of standalone STT use on advice compliance is stronger than the effect of network-augmented STT use for high self-efficacy patients.
Additional Analysis and Robustness Checks
Advice compliance and well-being
We also checked the relationship between advice compliance and well-being to ensure that increases in compliance actually benefit the customer in terms of improved service outcomes. Well-being reflects consumers’ overall perceptions of their quality of life and health status (Dagger and Sweeney 2006). Using a single-item measure (“By following my therapy plan, I can enjoy my life despite my disease”) as a proxy for well-being, we find a positive and significant correlation between advice compliance and well-being (r = .35, p < .01). We thereby substantiate the role of advice compliance as a focal construct in our study.
Robustness checks
We conducted some further robustness checks. First, we conducted a randomization check to assess the equal distribution of self-efficacy and BMI between groups. We did not find a significant difference between the groups, indicating that the randomization worked (p > .10). Second, we included several covariates on participants’ psychographics (i.e., role clarity, customer ability, and motivation) and demographics (i.e., age, gender, and education) in the ANCOVA. The interaction effects of both types of STT use with self-efficacy, F(2, 521) = 5.64, p < .01; partial η2 = .02, f = .15, and with BMI, F(2, 521) = 5.22, p < .01; partial η2 = .02, f = .14, did not change compared with the model without the covariates. This provides further support for Hypotheses 3a and 3b. Comparing standalone and network-augmented STTs in a model with covariates further suggests that standalone STT use is more effective than network-augmented STT use for high levels of self-efficacy (p = .02), while there is no significant difference for low levels of self-efficacy (p > .10). This emphasizes the partial support for Hypothesis 2 for customers with high levels of self-efficacy. Third, to rule out alternative explanations, we reestimated the main ANCOVA with a Heckman procedure correction (i.e., including the inverse Mills ratio from a first-stage selection regression as a control for attrition bias); the significant moderating effects of self-efficacy and BMI remain stable and do not show any new interaction effects between treatment variables and covariates.
Laboratory Experiment: Replication of the Field Experiment and Mediation Test
The objective of the lab experiment is 3-fold: (1) to replicate the findings of the field experiment in a more controlled setting, (2) to use a more generalizable setup of the experiment that does not focus on customers in a medical treatment program but on customers that seek to increase their well-being using a nonmedical professional expert service (i.e., fitness training), and (3) to examine perceived empowerment (Hypothesis 4) and perceived personalization (Hypothesis 5) as mediators to the effects of STT use on advice compliance.
Method
Design
The lab experiment resembles the field experiment in applying a between-subject design of three conditions (standalone STT, network-augmented STT, and control). It featured a general workout program targeted at customers who seek to increase their physical fitness and well-being.
Sample and Procedure
We sampled participants via an online panel. Our sample consists of 831 participants (54.9% male, agemean = 33.95 years, agemin = 18 years, agemax = 78 years). Participants were randomly allocated to one of the three conditions and were presented with a scenario asking them to imagine that they were aiming to conduct a training program to increase their physical fitness. Participants were told that they will receive a training program from a professional service provider (i.e., fitness expert). The expert would advise the customer to adhere to this program but does not explicitly check adherence. Participants in both STT conditions were additionally told that the expert provided them with a self-tracking system in the form of a fitness tracker. This self-tracking system and its benefits were described in accordance with existing offers in a fitness context (e.g., Fitbit or Garmin). The description specifically highlighted that the information provided by the self-tracking system can help participants monitor and understand their training performance, as the technology tracks, displays, and explains key fitness and training data. In the network-augmented condition, participants were additionally told that the data collected and analyzed by their tracking device will be shared (anonymously) with an online community. More precisely, the community would offer feedback on their training progress from peers in similar training programs, benchmark their performance against others', and discuss content and progress with others.
Measures
We used the same measures as in the field experiment to capture advice compliance, self-efficacy, and BMI (based on self-reported body height and weight) and the covariates role clarity, customer ability, and motivation. Additionally, we assessed perceived empowerment using 4 items based on Camacho, De Jong, and Stremersch (2014) and Prigge et al. (2015). Perceived personalization was measured using 4 items adapted from Bock, Mangus, and Folse (2016). We also obtained information on participants’ demographics (i.e., gender, age, education). Appendix provides an overview on the measures and their reliabilities.
To conduct robustness checks with respect to the effect of compliance on well-being, we measured well-being using 3 items in line with Dagger and Sweeney (2006). To rule out alternative mediators, we also measured three aspects of locus of control (i.e., internal, powerful others, and chance) based on Büttgen, Schumann, and Ates (2012), as well as two dimensions of risk (i.e., social, psychological) based on Laroche et al. (2004).
Results
Confirmatory Factor Analysis and Descriptive Statistics
In line with Study 1, we first conducted a confirmatory factor analysis. In support for both convergent and discriminant validity of our constructs, we find that the AVE is larger than .50 for all constructs (i.e., AVEcompliance = .70, AVEself-efficacy = .64, AVEroleclarity = .61, AVEcustomerability = .73, AVEmotivation = .76, AVEempowerment = .64, and AVEpersonalization = .79) and exceeds the squared correlation between the constructs (Fornell and Larcker 1981). Table 2 shows the descriptive statistics and correlations.
Descriptive Statistics and Correlations (Lab Experiment).
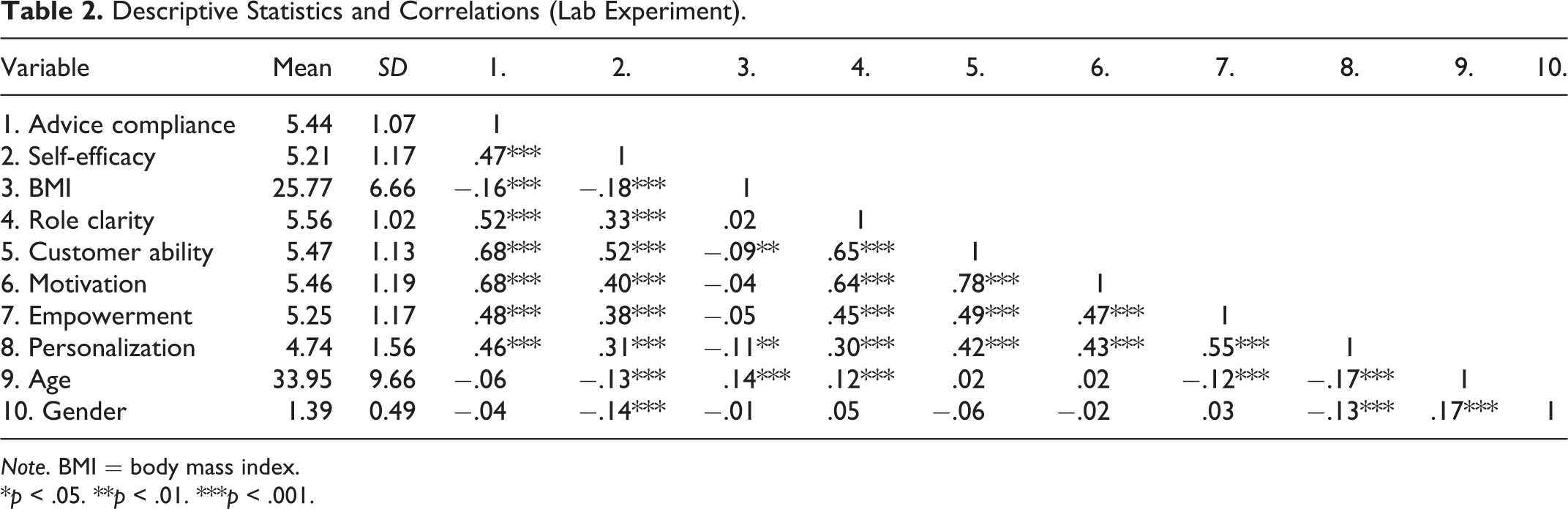
Note. BMI = body mass index.
*p < .05. **p < .01. ***p < .001.
Manipulation Check
Participants correctly identified whether they obtained a standalone STT, a network-augmented STT, or no STT, F(2, 828) = 420.18, p < .01; group differences significant at p ≤ .01.
Main Effect
To investigate the effect of STT use on advice compliance, we first conducted an ANOVA. The results reveal a significant main effect of STT use on advice compliance, Mstandalone = 5.53, Mnetwork = 5.55, Mcontrol = 5.24; F(2, 828) = 7.35, p < .01; partial η2 = .02, f = .13. Comparing the use of standalone and network-augmented STTs, we do not find a significant difference (p > .10). However, both uses of the standalone (p < .01) and the network-augmented STT (p < .01) resulted in higher advice compliance compared with the control condition without STT. Hence, we find support for Hypothesis 1, but in line with the field experiment, Hypothesis 2 is not supported.
Moderation Effect of Self-Efficacy
We then conducted an ANCOVA to test the moderating influence of self-efficacy. We find a significant interaction effect between using STTs and self-efficacy, F(2, 825) = 5.48, p ≤ .01; η2 = .01, f = .11. Contrasting the two types of STTs with the control group shows that the interaction effect is positive and significant for both standalone STT use (b = .22, p ≤ .01) and network-augmented STT use (b = .15, p = .03). The results replicate the findings of the field experiment and provide support for Hypothesis 3a. Figure 3 displays the positive moderation effect.
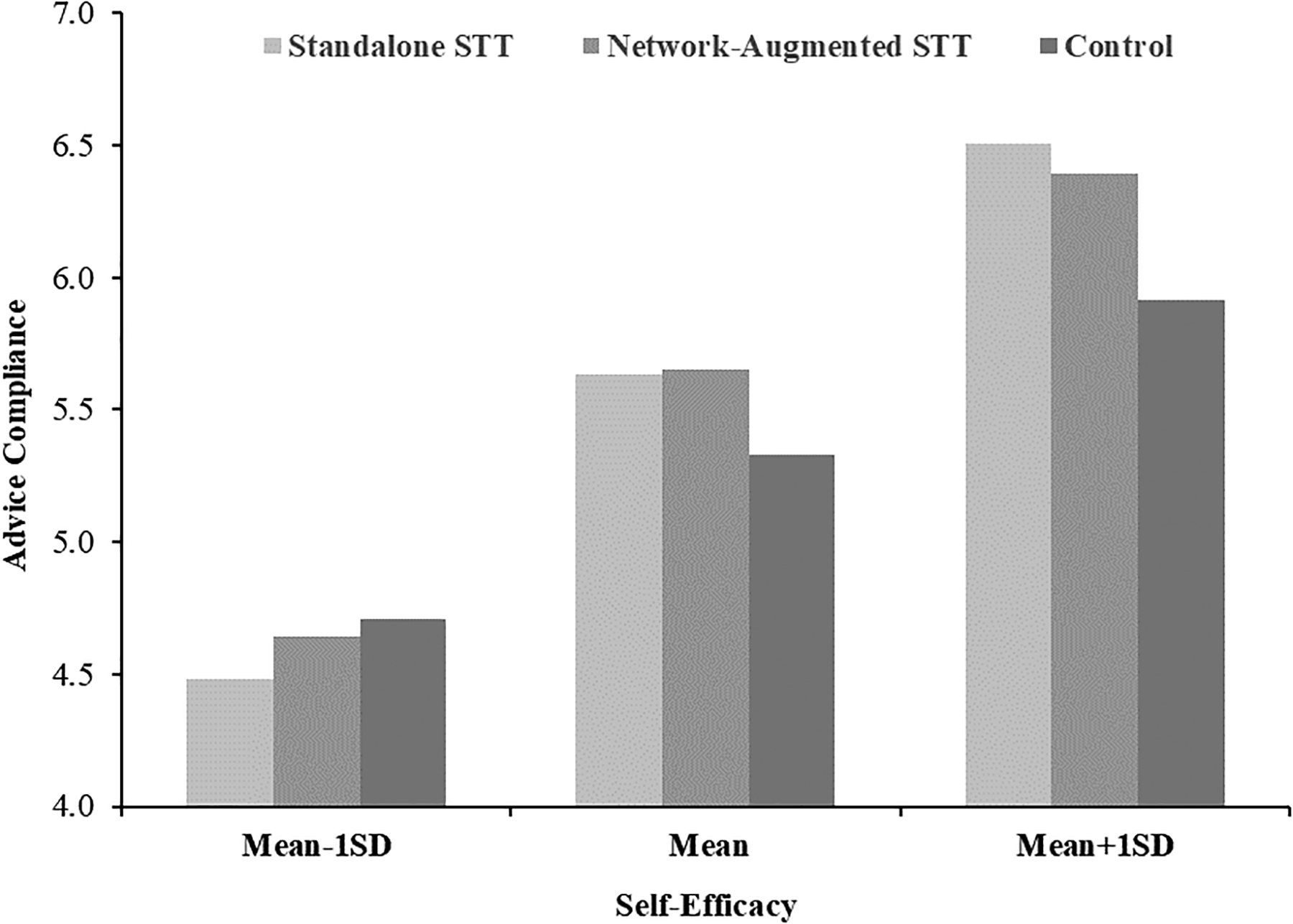
Moderation effect of self-efficacy (lab experiment). Displays moderation effect of self-efficacy on advice by categorizing participants in low self-efficacy (≤ mean − 1 SD), mean self-efficacy, and high self-efficacy (≥ mean +1 SD).
BMI as a Proxy for Self-Efficacy
Regarding BMI as a proxy for the moderation effect of self-efficacy, we find a significant interaction effect between STT use and BMI, F(2, 825) = 3.14, p = .04; partial η2 = .01, f = .09. Comparing the two types of STTs shows that the interaction effect is negative and significant for both standalone (β = −.03, p = .03) and network-augmented STTs (β = −.03, p = .03). 5 These findings replicate the negative interaction effect of BMI for both types of STTs and thus further support the role of BMI as a proxy for self-efficacy (Hypothesis 3b).
Standalone Versus Network-Augmented STT Use
As in the analysis of our field experiment, we also contrast the effects of STT use for different levels of self-efficacy. Although we find the effect of standalone STT use is stronger than that of network-augmented STT use for high self-efficacy respondents, the difference is not significant (Mstandalone = 5.92, Mnetwork = 5.89, p > .10). We also do not find a significant difference for low levels of self-efficacy (Mstandalone = 4.92, Mnetwork = 5.03, p > .10). Thus, the results do not support Hypothesis 2.
Mediation Analysis
We test perceived empowerment and perceived personalization in a parallel mediation model. Following Zhao, Lynch, and Chen (2010), we use the bias-corrected bootstrapping procedure to assess the mediation effects. Specifically, we use 10,000 bootstrap samples with a 95% confidence interval (CI) and indicator coding with the control group as a baseline.
The results indicate that standalone and network-augmented STT have a significant positive effect on both perceived empowerment and perceived personalization (both effects: p < .01). Moreover, perceived empowerment and personalization positively affect advice compliance (both effects: p < .01). Consistent with the above results, standalone STT use (i.e., b = .12, 95% CI [.07, .19]) and network-augmented STT use (i.e., b = .14 with 95% CI [.09, .21]) influence advice compliance through perceived empowerment. Similarly, standalone STT use (i.e., b = .24 with 95% CI [.16, .34]) and network-augmented STT use (i.e., b = .27, 95% CI [18, .38]) exert a significant indirect effect on advice compliance via perceived personalization. There are no significant direct effects of standalone and network-augmented STT use on advice compliance when the mediator is included. Thus, both mediators fully mediate the effect of STT use on advice compliance. In sum, the results provide empirical support for our mediation Hypotheses 4 and 5. Figure 4 visualizes the reported effects.
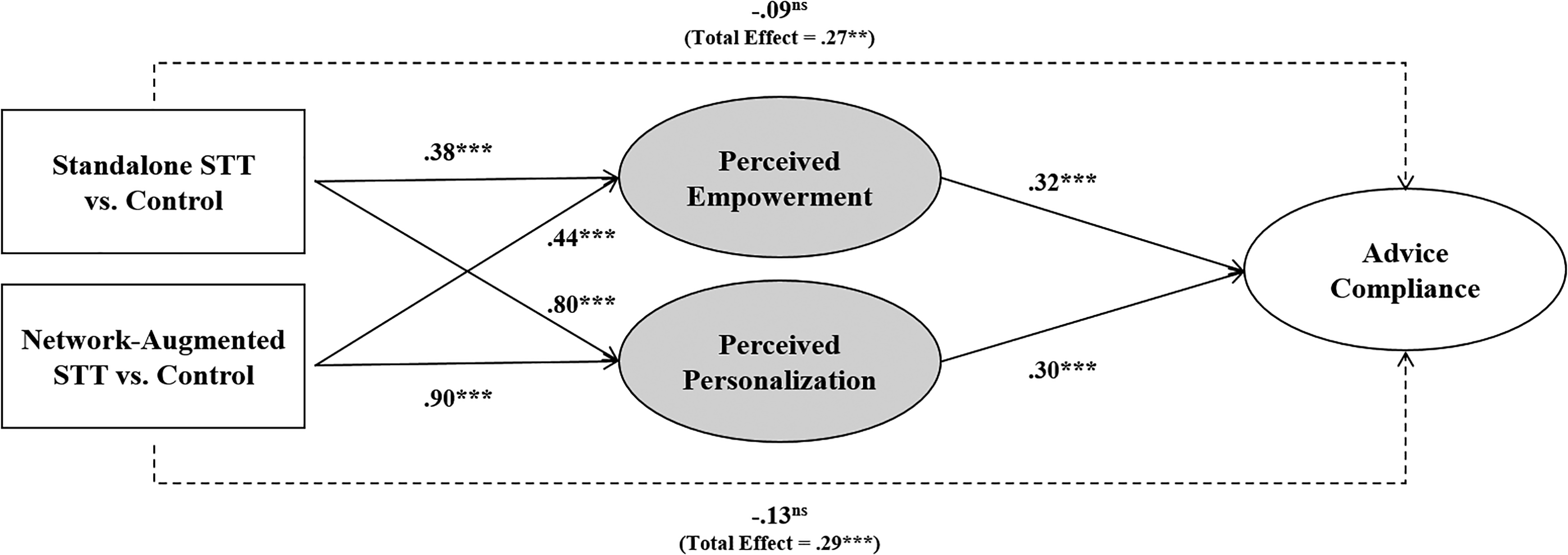
Mediation effects of perceived empowerment and perceived personalization (lab experiment). Remark: standardized values; STT = self-tracking technology. Indirect effects of standalone STTs through perceived empowerment (b = .12 with 95% confidence interval [CI] = [.07, .19]) and through perceived personalization (b = .24 with 95% CI [.16, .34]). Indirect effects of network-augmented STTs through perceived empowerment (b = .14 with 95% CI [.09, .21]) and through perceived personalization (b = .27 with 95% CI [.18, .38]).
Additional Analyses and Robustness Checks
Advice compliance and well-being
We also investigated the relationship between advice compliance and well-being to ensure the relevance of the compliance construct. Our analysis was 4-fold. First, we investigated the correlation between advice compliance and well-being. The correlation is high and significant (r = .70, p < .01). Second, we conducted a confirmatory factor analysis to establish convergent and discriminant validity (i.e., AVEcompliance = .70 and AVEwell-being = .69). Third, we conducted an ANOVA to evaluate the effect of STT use on well-being across groups. Both types of STTs display a significant effect on well-being, Mstandalone = 5.46, Mnetwork = 5.45, Mcontrol = 5.23; F(2, 828) = 4.27, p = .01; partial η2 = .01, f = .10. Participants in both STT treatment groups report higher well-being scores compared with the control condition without an STT (both p < .05). Fourth, we conducted a mediation analysis to check whether advice compliance represents the underlying mechanism that drives the effect of STT use on well-being. Applying the same bootstrapping method as before, we find a significant indirect effect of standalone STT use (i.e., b = .19, 95% CI [.07, .31]) and network-augmented STT use (i.e., b = .20, 95% CI [.08, .33]) for the path through advice compliance on well-being. There is no significant direct effect of the two types of STTs on well-being when the mediator is included (p > .10). Thus, advice compliance fully mediates the effect of STT use on well-being. This result further underlines the role of advice compliance as a central antecedent of well-being and supports our research focus on this crucial construct. 6
Ruling out alternative mediators
To further fortify perceived empowerment and perceived personalization as underlying mechanisms in the link between STT use and advice compliance, we accounted for service locus of control and perceived risk as alternative mediators. First, we find that none of the three dimensions of locus of control uncovered significant indirect effects on advice compliance. We thus ruled out service locus of control as a competing theoretical explanation. Second, perceptions of risk associated with the service (outcome) could also explain the reported effects of STT use on advice compliance (Laroche et al. 2004). However, including perceived psychological and social risk in a mediation model did not reveal significant indirect effects. These findings also rule out perceived risk as a competing mediator. 7
Robustness checks
As additional robustness checks, we first investigated the equal distribution of the measures of self-efficacy, BMI, and demographics across groups. As expected, we did not find any significant differences (p > .10). Second, we included several covariates on participants’ psychographics (i.e., role clarity, customer ability, and motivation) and demographics (i.e., age, gender, and education) in the ANCOVA. The interaction effects of both STTs with self-efficacy, F(2, 814) = 4.12, p = .02; partial η2 = .01, f = .10, and with BMI, F(2, 814) = 2.76, p = .06; partial η2 = .01, f = .08, are robust compared with the model without covariates. Comparing standalone and network-augmented STT use in a model that incorporates covariates does not reveal significant effects for high (i.e., above the mean) or low levels of self-efficacy (p > .10). Overall, these results offer additional empirical evidence for the robustness of the interaction effects.
Discussion
Summary of Results
This research sets out to investigate the influence of STT use on advice compliance in a professional service setting. We find that using STTs—both standalone STTs and network-augmented STTs—can be effective in enhancing advice compliance; yet, their ultimate impact depends on specific consumer characteristics. Empirical evidence from the field and lab experiment shows that consumers’ self-efficacy significantly affects the impact of STT use on compliant behaviors. More precisely, STT use seems especially effective for consumers with high self-efficacy. In contrast, for consumers with low self-efficacy, STTs seem to be less effective to increase advice compliance and can be even harmful compared with situations without STT exposure. Interestingly, we identify a similar interaction effect for BMI as a moderating variable in both experiments. This result underlines that service providers can use consumers’ BMI as an easy-to-measure, physiological proxy to self-efficacy when estimating the ramifications of STT use.
Our results are inconclusive on the effectiveness of network-augmented STTs. While we find that standalone STTs produce optimal results for people with higher self-efficacy in the lab experiment, there was no significant difference between the two STT types in the field experiment. We also find empirical evidence for the hypothesized mediating roles of perceived empowerment and perceived personalization. Table 3 summarizes the results of the hypotheses testing. Finally, we find evidence that supports the generalization of our results beyond advice compliance since advice compliance acts as a mediator in linking STT use to well-being. Based on the outlined empirical insights, below, we present important theoretical and practical implications.
Overview on the Hypotheses Testing.
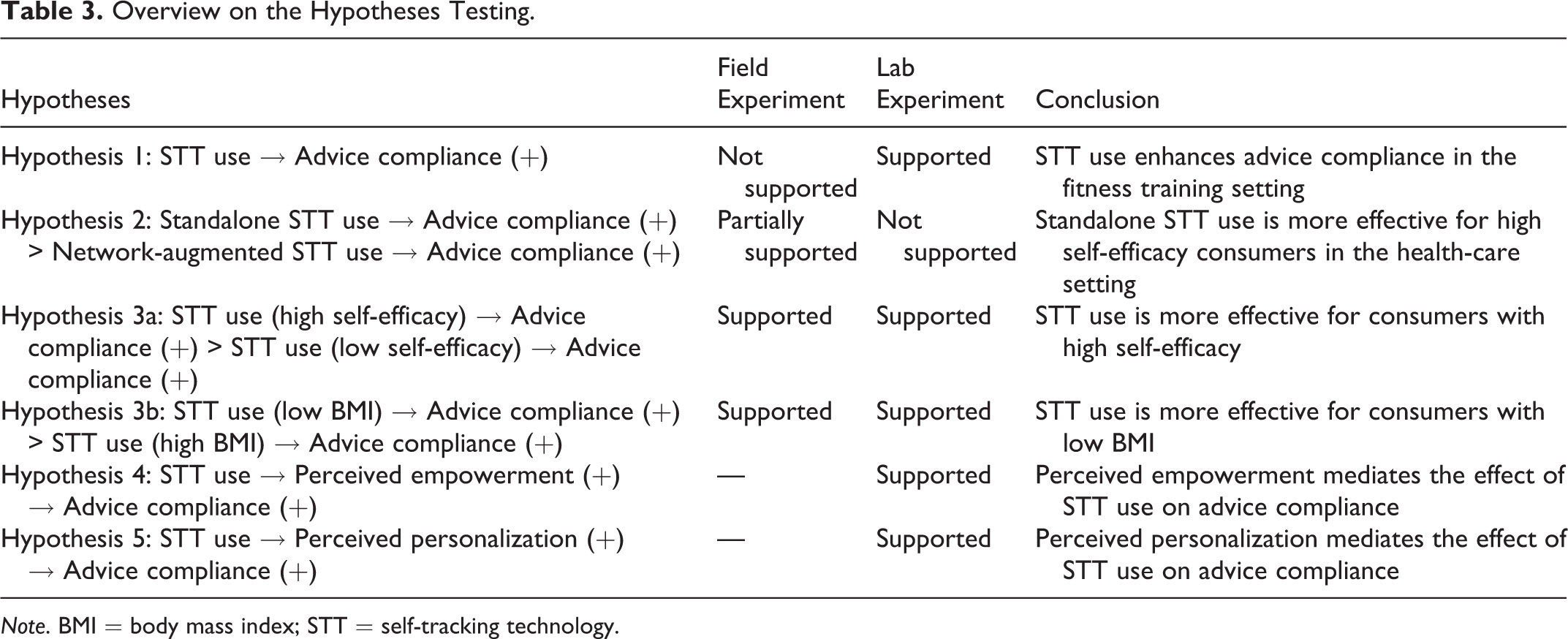
Note. BMI = body mass index; STT = self-tracking technology.
Theoretical Implications
Exploring the link between STT use and customers’ advice compliance adds to several literature streams. To start, we extend previous work on strategies and tactics to increase advice compliance. Existing studies have considered many provider-related (e.g., expertise) and customer-related (e.g., positivity) drivers of advice compliance (e.g., Dellande, Gilly, and Graham 2004; Guo et al. 2013; Seiders et al. 2015), but so far, the role of STTs to boost advice compliance had been left unexplored. We specifically add to this line of research by finding that STT use can increase advice compliance especially for consumers with high self-efficacy. Most notably, STT use empowers consumers to play a more proactive role in professional service encounters. STTs enable users to not only collect and analyze individual data but also to better organize and understand these data. The resulting improved (self-)knowledge development has been identified as a decisive element of consumer empowerment that ultimately leads to superior levels of advice compliance with expert guidance (Prigge et al. 2015). This finding also corroborates previous insights that (informational) empowerment decreases unintended nonadherence in the context of medical services (Camacho, De Jong, and Stremersch 2014).
Moreover, as put forward by qualitative studies on self-tracking (e.g., Pantzar and Ruckenstein 2015) and proponents of the Quantified Self movement (e.g., Sharon 2017), we empirically validate that STT use positively affects customer perceptions of personalization. In fact, we find the mediating effect of personalization to be more powerful than the empowerment mechanism. This insight adds to a growing stream of research that hails personalization as an essential competitive factor for customer acquisition and retention in data-intensive services (Huang and Rust 2017) and for assuring patient satisfaction in health-care settings (Gallan et al. 2013). In particular, personalization increases information relevance and enhances service convenience, utility, and technology adoption (Komiak and Benbasat 2006).
Our findings also provide an important implication for the transformative service literature that looks at the relationship between service provision and well-being (Anderson and Ostrom 2015; Sweeney, Danaher, and McColl-Kennedy 2015). Specifically, we unveil that STT use can have unintended negative consequences for consumers with low self-efficacy. We thereby respond to recent calls for better understanding of the well-being-related outcomes of technology-enabled services and provide insights about under which conditions the use of these technology-based services actually yield detrimental results (Ostrom et al. 2015). On a more general level, our results illustrate the need to go beyond considerations of individual differences as direct determinants of technology use in service contexts (e.g., Blut, Wang, and Schoefer 2016; Meuter et al. 2005; Simon and Usunier 2007) and call for considering psychological traits as important contextual factors explaining service technology effectiveness.
Our inconclusive findings on the social connectivity aspect of STTs challenge previous studies that delineate beneficial outcomes of technology-enabled communities in health care (Tian et al. 2014). This difference could result from a focus on a “need-based” service situation (i.e., the health-care context) in the field versus a more “want-based” service situation (i.e., the fitness training context) in the lab experiment. In the former situation, more hedonic elements such as connections to a network are apparently appreciated less than core functionality, while in the latter situation, the higher intrinsic motivation seems to make users appreciative of hedonic product options. Another explanation could be that people are more sensitive to sharing personal health data with a network, even if anonymous, than sharing fitness training personal data with others. This may have diminished the perceived added value of the network augmentation. However, the ramifications of network-augmented STTs are not yet fully uncovered and need further exploration.
Finally, our finding that BMI can serve as a physiological proxy for self-efficacy extends knowledge on consumer differences that affect outcomes of technology-based services. Taken together, we contribute to studies that seek to investigate the role of physiological traits in consumer behavior and decision-making in general (e.g., Aspara and van den Bergh 2014) and the one of BMI in particular (e.g., Romero and Craig 2017).
Implications for Service Providers
STTs have been described as one of the major innovations that shape professional services in financial planning, health care, and the training market of the future, from both a practical perspective (Accenture 2018) and an academic perspective (Brüggen et al. 2017; Huang and Rust 2017). Against this backdrop, our findings are of practical relevance for professional service providers that already use STTs or seek to introduce them. Professional service providers can leverage our findings to increase customer compliance with expert advice, and eventually, to improve customers’ well-being.
Service providers need to acknowledge that STTs are not effective per se, as they are less impactful and potentially harmful for customers with a low self-efficacy. To apply STTs successfully and avoid unintended consequences, service providers can consider the following recommendations. First, when incorporating STTs in their offerings, service providers should pay special attention to empowerment and personalization by assuring that the technology truly increases customers’ capabilities to participate in decision-making, while it simultaneously adapts the service offering to better meet customers’ individual needs in the service process. Second, with respect to the design of the STT, companies might need to decide between providing a standalone STT or adding a network feature. In health-care (i.e., more need-based) services, standalone STTs appear to be more effective than network-augmented STTs. That is, features promoting participation in online communities might be experienced as distressing in this context and can inhibit customers’ compliance with expert advice. Third, service providers can increase the effectiveness of STTs by segmenting their customers based on self-efficacy. Assigning STTs to customers with high self-efficacy will result in higher advice compliance, while customers with low self-efficacy could receive an alternative service without an STT or additional face-to-face interactions. Fourth, when assessments of self-efficacy are not available or difficult to obtain, service providers can use customers’ BMI as a physiological proxy. BMI as an indicator can be easily assessed by individuals’ height and weight and thus enables a convenient initial segmentation. However, we still recommend practitioners to engage in more granular analyses including customer psychographics when ultimately deciding on their segmentation.
Limitations and Avenues for Future Research
While our results provide evidence that standalone STTs are more effective than network-augmented STTs for consumers with high self-efficacy, we could not fully replicate our findings from the field experiment in a laboratory setting. This could be due to the difference between intended behavior in the laboratory and actual behavior in the field. However, the differences could also result from the differences in the context, that is, the treatment of people with diabetes versus fitness training. Thus, there is a need to further investigate the difference between the effects of standalone and network-augmented STTs in different service contexts such as for need- versus want-based services (Seiders et al. 2015).
Our results also provide empirical support for the use of BMI as a proxy for self-efficacy. However, the supporting literature for our hypothesis stems from health-care- and well-being-related studies, and perhaps the moderating effect of BMI (and its role as a proxy for self-efficacy) might only hold for professional services in health care and well-being. As the application of this measure seems less helpful for other professional services such as legal and financial services, more research is needed to investigate the role of BMI as a proxy.
In sum, although our research represents an important first step to better understand the link between STT use and advice compliance, more work is needed to generalize our findings to other professional services such as financial planning, management consulting, as well as the training and development of employees.
Supplemental Material
Supplemental Material, STT_Advice_Compliance_l_Executive_Summary_l_Dec_28 - What Gets Measured Gets Done: Can Self-Tracking Technologies Enhance Advice Compliance?
Supplemental Material, STT_Advice_Compliance_l_Executive_Summary_l_Dec_28 for What Gets Measured Gets Done: Can Self-Tracking Technologies Enhance Advice Compliance? by Kristina Wittkowski, Jan F. Klein, Tomas Falk, Jeroen J. L. Schepers, Jaakko Aspara and Kai N. Bergner in Journal of Service Research
Footnotes
Appendix
Authors’ Note
Kristina Wittkowski and Jan F. Klein contributed equally to this article.
Acknowledgments
The authors thank Niels van de Ven for his helpful comments on earlier versions of the article. We would like to thank an anonymous reviewer for pointing out the need to strengthen our mediation results by ruling out alternative mediators.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.