
Abstract

Dear Editor,
Pediatric and perinatal hospital autopsy rates have been declining for decades despite their critical role in quality assurance, education, and research. A recent Canadian study revealed a 29% drop in stillbirth autopsies, 41% in early neonatal, 29% in late neonatal, and 17% in post-neonatal deaths between the periods of 1981–1992 and 2005–2015. 1 According to the National Center for Health Statistics, hospital autopsy rates in the United States in 2020 were 31.6% for children under 1 year, 55.4% for 1–4 years, and 46.8% for 5–14 years. The highest rate, 62.6%, was for those aged 15–24 years. 2
To examine differences in autopsy practices, we compared and analyzed data from 6 North American children’s hospitals (Institutions A–F) over a 6-year period (2016–2021). Our aim was to identify factors influencing autopsy rates and their impact on training.
The cumulative data showed that 3306 pediatric and perinatal autopsies were performed across the institutions during the study period. All were next-of-kin consented hospital autopsies. Notably, 1 institution also performed medicolegal autopsies in-house. Of these autopsies, 49.0% (ranging from 16.0% to 98.0%) involved patients who had previously received care at the institution performing the autopsy. Additionally, 42% (ranging from 6.0% to 76.0%) were perinatal cases (data available from 5 hospitals), and 11.0% (ranging from 1.0% to 46.0%) were restricted autopsies. A total of 61 pediatric pathology fellows completed their training across these institutions during the study period.
There was significant variation between institutions in both the total number of autopsy cases (ranging from 215 to 812) and the annual number of autopsies (ranging from 28 to 158; Figure 1(a)). Institution F, which had the highest total number of autopsies (n = 812), also conducted the highest number of inpatient autopsies, with a cumulative mean of 66.5% of their autopsies being for in-hospital deaths (Figure 1(b) and (c)). Furthermore, it performed the third-highest number of consult autopsies (n = 270, or 33.2% of total autopsies) during the 6-year period (Figure 1(d)). Institution C, with the second-highest number of autopsies (n = 782), had the highest number of perinatal autopsies (n = 535, or 68.4% of total autopsies; Figure 1(e)). Institution D, with the third-highest number of autopsies (n = 703), consistently performed a large volume of outside patient/consultation autopsies (n = 509, or 72.4% of total autopsies; Figure 1(d)). Notably, Institution A had the highest rate of restricted autopsies for each study year, with a cumulative mean of 30.2% (range: 18.0–46.0%) of their autopsies being restricted to specific organs (Figure 1(e)).
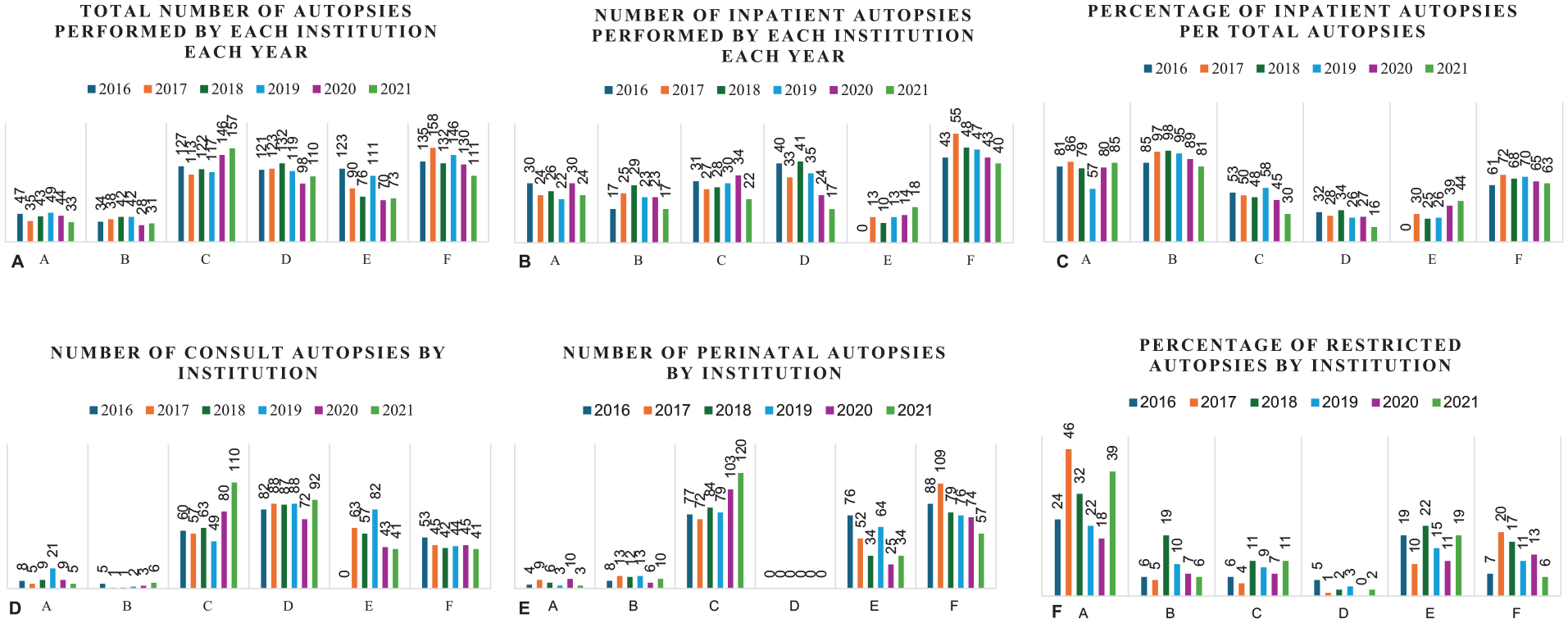
(A) Total number of autopsy cases performed by each institution per year. (B) Number of inpatient autopsies relative to in-hospital deaths per institution per year. (C) Percentage of inpatient autopsies relative to total number of autopsies per institution per year. (D) Number of consult autopsies per institution per year. (E) Number of perinatal autopsies per institution per year (data available for 5 institutions). Perinatal autopsies included stillbirth cases, fetuses delivered at 20 weeks’ gestation or later, and neonatal cases, those delivered liveborn up to 28 days of life. (F) Percentage of restricted autopsies relative to total number of autopsies per institution per year.
The number of fellows per institution ranged from 0 to 3 annually, with each institution training between 6 and 17 fellows over the study period. The annual fellow-to-autopsy ratio varied from 1:11 to 1:146, based on these statistics alone and excluding cases shared with other trainees. Notably, only 3 of the 5 U.S.-based institutions met the current procedural skill competency requirement set by the Accreditation Council for Graduate Medical Education (ACGME), when relying solely on autopsies performed within their own institution. This requirement states that pediatric pathology fellows must demonstrate competence in performing various types of pediatric autopsies—general pediatric, metabolic, forensic, perinatal, embryo-fetal, and stillborn—by performing or supervising at least 30 autopsies. 3 To address this limitation, institutions with a fellow-to-autopsy ratio below 1:30 may allow case-sharing between trainees or arrange for autopsies at other institutions. While ACGME guidelines exist regarding shared and restricted autopsies for pathology residents, no such details are specified for pediatric pathology fellows.
Autopsies are essential for building a solid foundation in anatomy, embryology, fetal physiology as well as technical and clinical communication skills. They are crucial for training residents and fellows, particularly in pediatric and forensic pathology subspecialties. The quality of autopsy education and the number of autopsies performed are key factors influencing pathology trainees’ interest in autopsy and forensic pathology. 4 Moreover, proficiency in pediatric and perinatal autopsies is a standard expectation for all practicing pediatric pathologists.
Our findings underscore the variability in pediatric autopsy service driven by institutional differences in workflow and referral patterns. Some institutions maintain high autopsy numbers through a steady volume of perinatal or consultation cases. Additionally, the number of fellows at an institution affects the distribution of autopsy cases, potentially diluting training quality if there are too many fellows and insufficient autopsies. Further research into institutional policies, staffing, and consent processes is needed to identify strategies for reducing variability, increasing autopsy rates, and addressing the negative impact of declining hospital autopsy numbers and rising restricted autopsy rates on pediatric pathology training. We advocate for continued efforts to standardize autopsy protocols, enhance training opportunities, and emphasize the critical role of autopsies in advancing pediatric healthcare.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.