
Abstract
Background:
In a non-forensic hospital setting, neonatal death within the first week of life is often related to premature birth and/or lung diseases. Without post-mortem examination, the identification of the cause of death may be challenging. Autopsy can confirm the clinical diagnosis, uncover additional information or change the diagnosis. Our study aimed to assess the correlation between the clinical diagnosis and post-mortem findings in early neonatal deaths.
Methods:
The retrospective study included autopsy cases with neonatal deaths within the first 7 days of life (arbitrary time interval 2006-2021). Discrepancies between clinical and histopathological findings were classified into 3 groups: (i) full agreement, (ii) additional findings discovered by autopsy, or (iii) autopsy changed the diagnosis.
Results:
A cohort of 27 cases could be identified and lung pathologies were the most common finding (56%). Additional findings could be discovered in 48% of cases. Major discrepancies which changed the clinical diagnosis could be found in 11% (n = 3/27) of cases.
Conclusion:
Frequently, post-mortem examinations validate the clinical diagnosis while revealing crucial information in a few cases. In these discrepant cases, autopsy findings can provide information for genetic counselling and quality control of clinical management.
Keywords
Introduction
Peri/neonatal death is the most severe complication of pregnancy and childbirth. It is less frequent than intrauterine fetal death, occurring in 2.3 per 1000 live births in Germany.1-3 Children who die in the early neonatal period are less likely to be examined by autopsy than intrauterine deaths. 2 It has to be acknowledged that “perinatal” and “neonatal” are often used as interchangeable terms, but the definition varies between different publications. Fernández-Férez et al. 4 define perinatal death as the death of the unborn or newborn child between the 22nd week of gestation and the first 7 days of life, while Cnattingius et al. 5 define neonatal death as the death within the first month after birth. Weber et al. established the term “sudden unexpected early neonatal death” (SUEND) within the first 7 days of life. 1 Our study focused on early neonatal deaths within the first week of life and intended to explore potential discrepancies between clinical and autopsy diagnosis. The aim of this study is to evaluate the frequency of concordant and discrepant diagnoses made before and around birth and after death by post-mortem examination.
Materials and Methods
We performed a retrospective evaluation of all neonatal autopsies at the Institute of Pathology (Hannover Medical School, Hannover, Germany) in an arbitrary time interval from 1.1.2006 to 31.12.2021. Retrospective evaluation was approved by the local ethics committee (#2893-2015).
Inclusion criteria were (i) early neonatal death within the first 7 days after birth, according to the SUEND definition 1 and (ii) routine pathology post-mortem examination. We excluded (i) post-mortem organ biopsy without autopsy, (ii) external examination without autopsy, and (iii) autopsy in a forensic setting.
Maternal age, gestational age, mode of birth, newborn sex, body weight, body length, foot length, and autopsy findings were summarized. The standardized neonatal post-mortem examination included neck/chest and abdomen dissection with sampling of the heart, lungs, liver, spleen, pancreas, intestine, kidneys, adrenal glands, and vertebral bone marrow for histological examination. Brain dissection including histology was performed in all but 1 case.
Newborn deaths were classified into malformation/syndrome-associated deaths, diseases of the newborn/preterm infant and others (e.g. tumor-associated such as fetal sacral teratoma or drug-induced such as angiotensin receptor antagonist-related fetopathy). Malformations were grouped according to Rossi and Prefumo 6 into limbs/skeleton, central nerve system, lungs, heart, gastrointestinal tract, kidneys, and urogenital tract. Cases presenting 2 or more anomalies were accounted as multiple malformations and considered in each organ category separately.
If available, the placenta was evaluated. Standard placental histological evaluation included umbilical cord, fetal membranes, and placental parenchyma. The placenta weight and basal surface as well as villous maturation and placenta pathologies were evaluated. Placenta pathologies were classified based on the Amsterdam criteria. 7
Discrepancies between clinical diagnosis and autopsy examination were classified according to 2 classification systems. As defined by Rossi and Prefumo, 6 cases were grouped into 3 different categories: (i) full agreement between prenatal ultrasound and autopsy, (ii) extra autopsy findings which did not change the clinical diagnosis, and (iii) extra autopsy findings which changed the clinical diagnosis.
In addition, the modified Goldman criteria, 8 according to Hickey et al., 9 were applied. Cases with newly discovered diagnosis which most likely was the primary cause of death were classified into 2 categories: discordant diagnosis 1 (DD1; a diagnosis that, if detected before death, would likely have led to cure or prolonged survival) and discordant diagnosis 2 (DD2; a diagnosis that, if detected before death, would probably not have led to cure or prolonged survival). 9 Additional findings were grouped into 3 classes: (i) identification of previously unsuspected or unconfirmed clinical conditions not directly contributing to the primary cause of death; (ii) discovery of conditions with significant implications for genetic counseling in affected families; and (iii) identification of findings due to clinical management like ventilation. 10
Tabular data collection and descriptive statistics were performed with Microsoft Excel-19 (Microsoft Corporation, USA).
Results
Characteristics of the Study Cohort
We identified a cohort of 27 cases with a lifespan between 20 minutes to 7 days. Less than half of cases were preterm births (n = 10/27; 38%) and most children were delivered by caesarean section (n = 18/27; 72%). Maternal age was median 28 years and gravida/para-status was median 2/1 (Table 1).
Characteristics of the Study Cohort.
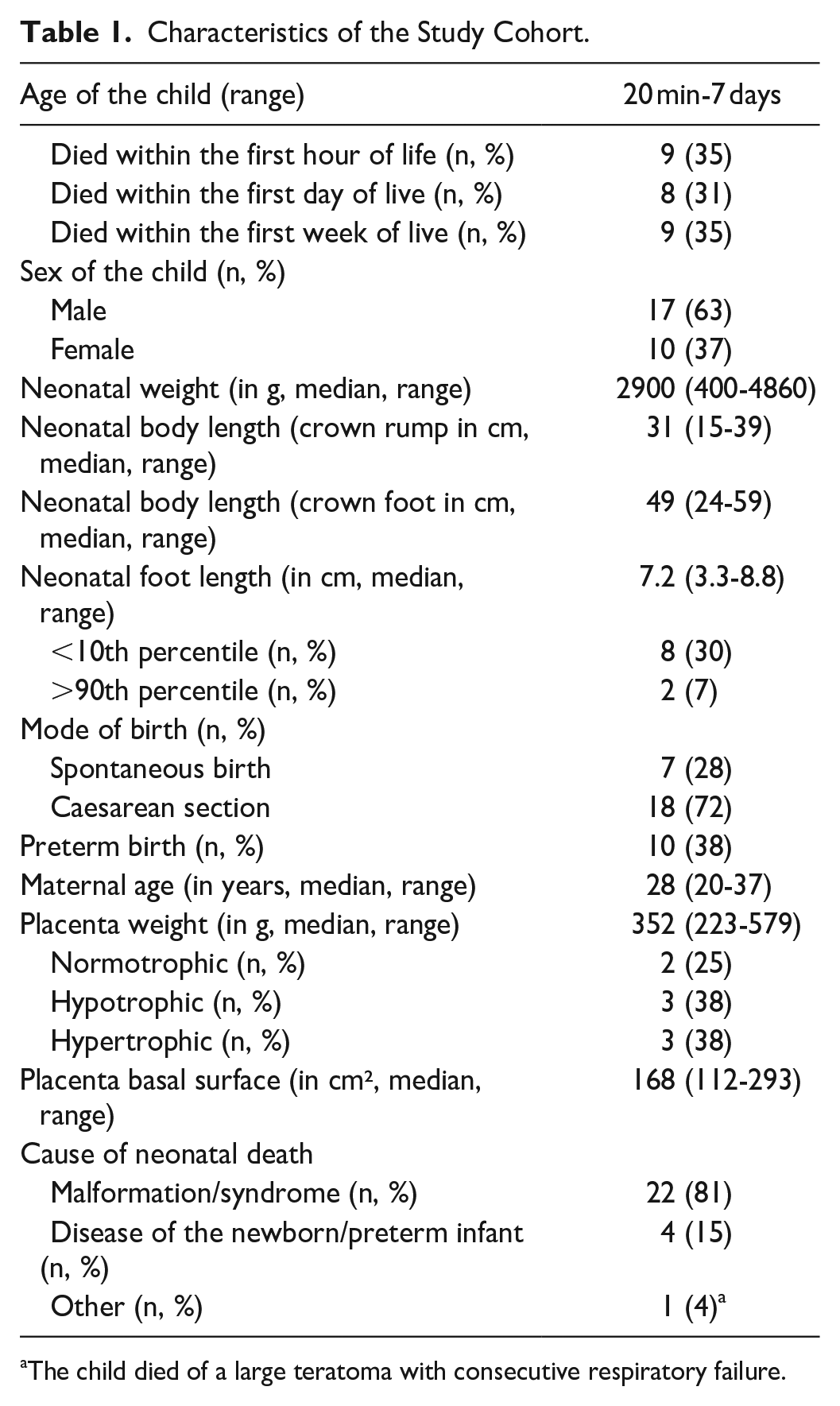
The child died of a large teratoma with consecutive respiratory failure.
Most cases had organ malformations or organ abnormalities (n = 22/27; 81%). Pathologies of the lungs were most frequent (n = 15/27; 56%), with hypoplasia/prematurity of the lung being the most common lung abnormality (n = 7/15; 47%). Several cases presented with 2 or more malformations (n = 10/27; 37%; Table 2). In 4 cases, cause of death were diseases of the newborn or preterm infant (n = 4/27, 15%). One neonate died of a massive teratoma with consecutive respiratory failure.
Fetal Malformations.
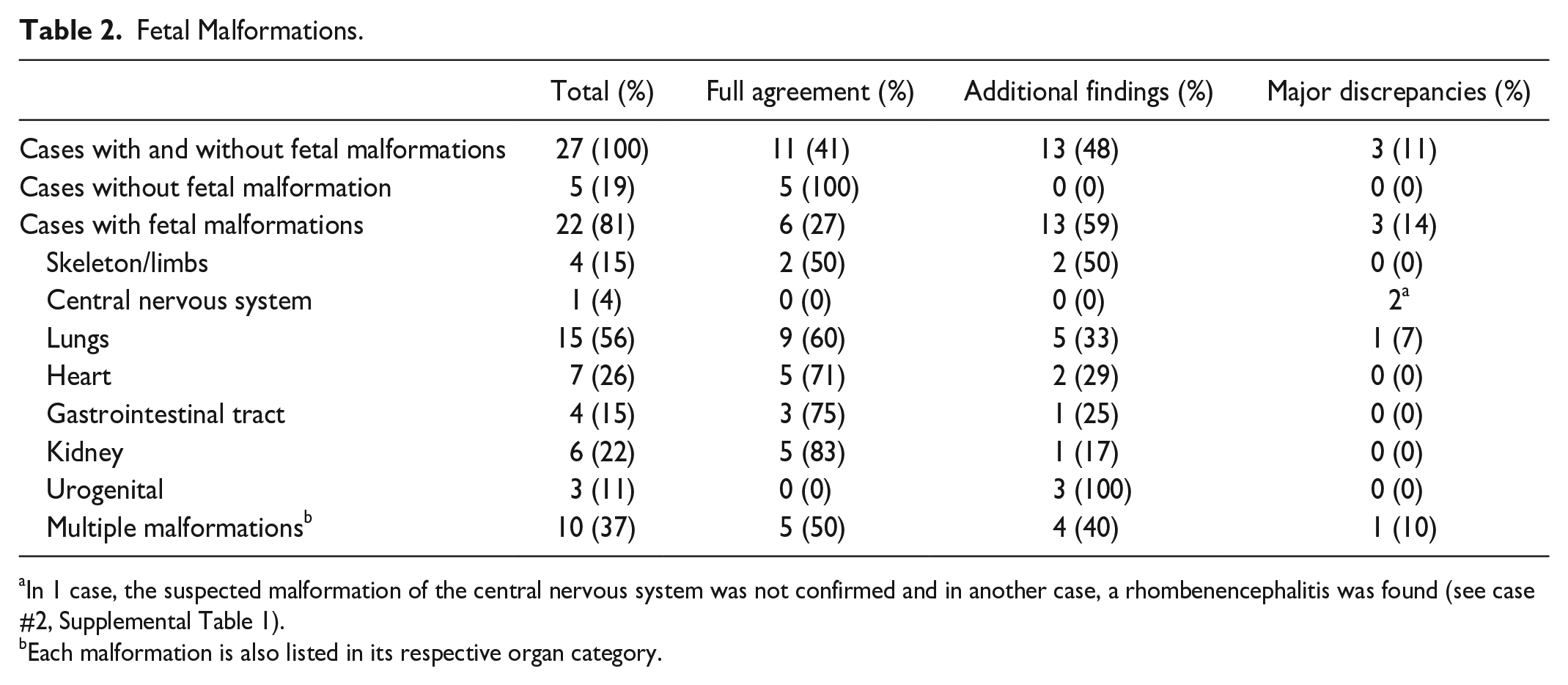
In 1 case, the suspected malformation of the central nervous system was not confirmed and in another case, a rhombenencephalitis was found (see case #2, Supplemental Table 1).
Each malformation is also listed in its respective organ category.
Concordance Between Clinical Diagnosis and Autopsy Findings
Full agreement between the clinical diagnosis and autopsy findings was obtained in less than half of the cases (n = 11/27; 41%). In most cases, the autopsy revealed complementary information regarding the cause of neonatal death.
According to the modified Goldman criteria by Hickey et al., 9 additional findings were found in 12 cases (44%; findings relevant for genetic counseling: n = 6/27). No DD1 type but DD2 type discordant diagnoses regarding the primary cause of death were found in 7 cases (n = 7/27, 26%; Supplemental Table 1).
According to Rossi and Prefumo, 6 additional findings were found in almost half of cases (n = 13/27; 48%). Most of these were found in the lungs (n = 5/13; 38%), urogenital tract (n = 3/13; 23%), and heart (n = 2/13; 15%). Major discrepancies between clinical diagnosis and autopsy findings were found in 3 cases (n = 3/27; 11%; Table 2).
Case #1 was a newborn with spontaneous birth in the 41st week of gestation. The neonate died after 2 days. Clinically, a total anomalous pulmonary venous connection was suspected. Autopsy could not confirm the suspected malformation but discovered a primary interstitial lung maturation defect with acute alveolar damage as a sign of acute respiratory failure. Specific changes like a surfactant deficiency, an alveolar capillary dysplasia or glycogenosis were not present, but histology revealed a acinar dysplasia-like delayed lung tissue maturation and secondary acute alveolar damage (diffuse developmental disorder according to Kurland et al. 11 ; Figure 1, Supplemental Table 1).
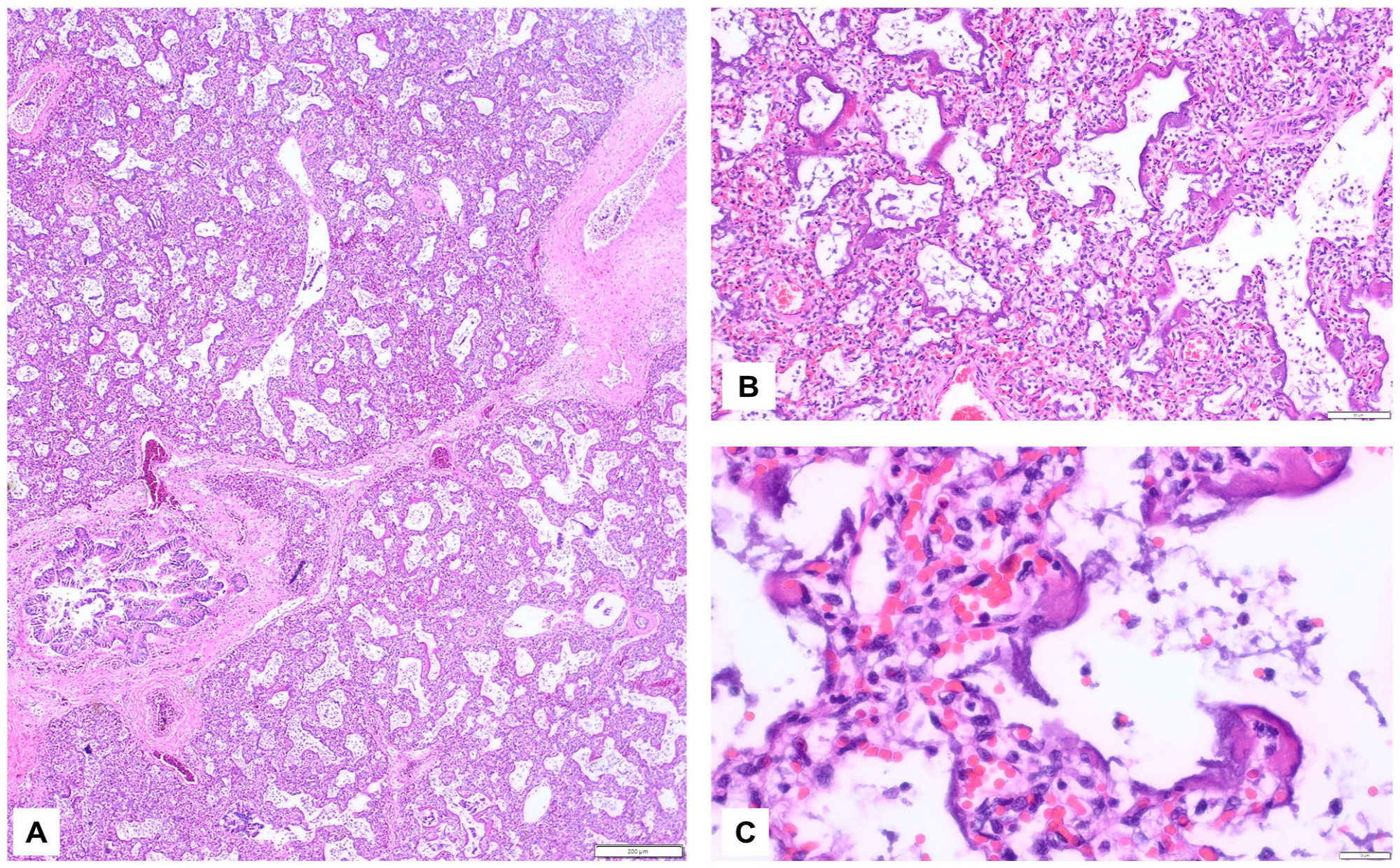
Case#1 Lung histology showing acute alveolar damage due to lung immaturity. (A) Hematoxylin and eosin staining of immature lung tissue (HE), 20x magnification, scale bar 200 µm. (B) 100x, 50 µm. (C) 400x, 10 µm.
Case #2 was a newborn with spontaneous birth in the 41st week of gestation with immediate respiratory distress. After 5 days, he died due to a respiratory failure of unknown etiology. Autopsy revealed a lymphocytic rhombencephalitis, which was most likely related to a neuro-muscular dysfunction and secondary respiratory decompensation (Figure 2, Supplemental Table 1). Histology showed no viral nuclear inclusion bodies and immunohistochemistry was negative for cytomegalovirus, herpes virus 1/2, parvovirus B19, SV40 virus and toxoplasmosis as well as negative for Epstein-Barr virus (in situ hybridization) and Coxsackie viruses (PCR). The placenta was not sent in for evaluation.
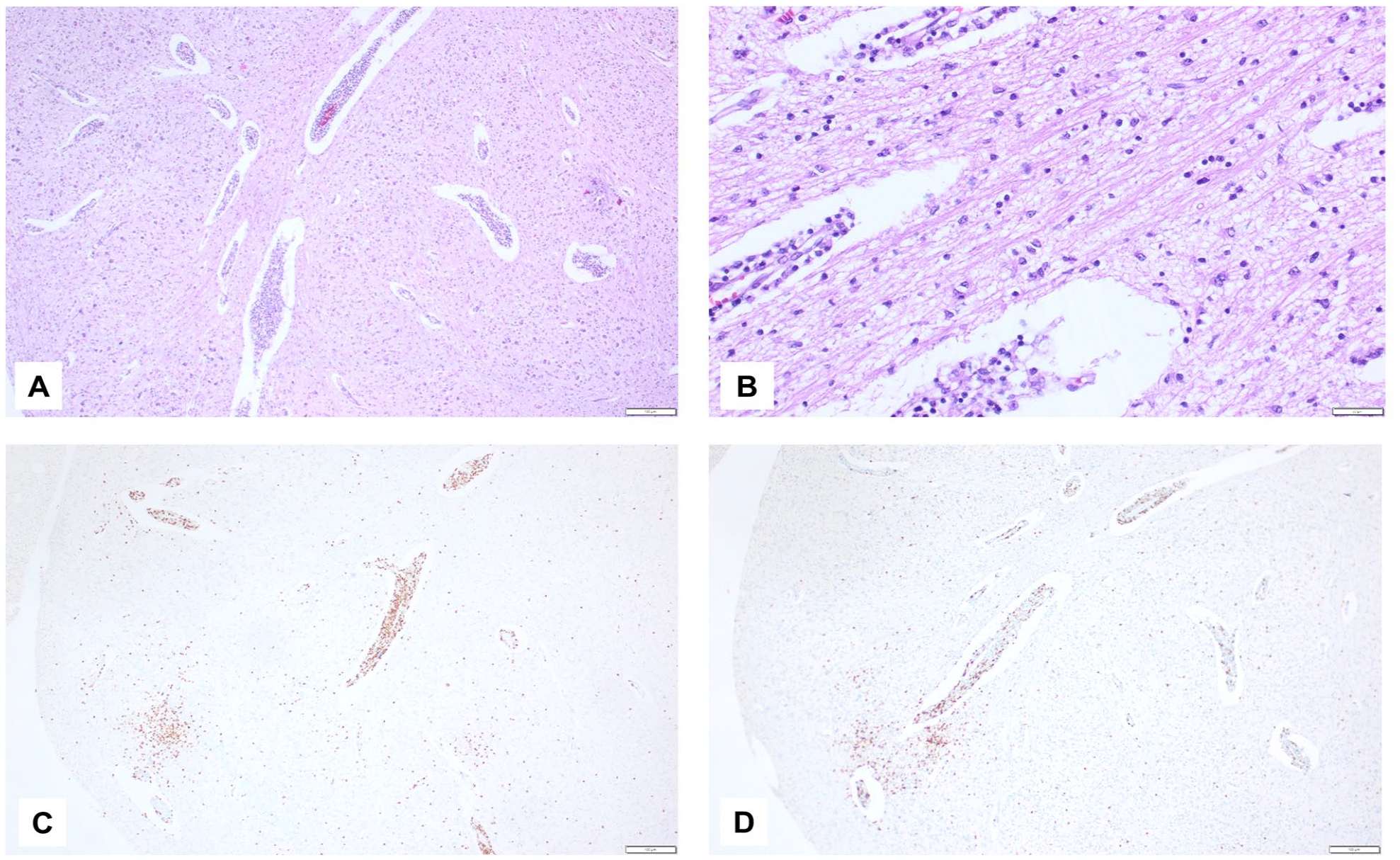
Case #2 T-lymphocytic rhombencephalitis. (A) Foci of lymphocytic inflammation; HE, 40x magnification, scale bar 100 µm. (B) Small lymphocytes and gliosis; HE, 200x, 20 µm. (C) CD4-immunohistochemistry; 40x, 100 µm. (D) CD8-immunohistochemistry; 40x, 100 µm.
In Case #3, an infant was born in the 24th week of gestation via caesarean section and died after 45 minutes. The preterm newborn was suspected to have a hydrops fetalis with anemia, pulmonary hypoplasia, pneumopericardium, and hepatosplenomegaly as well as a brain anomaly. The autopsy confirmed bilateral lung hypoplasia with hyaline membranes, marked splenomegaly, and moderate hepatomegaly with hyperplasia of erythropoiesis in liver, spleen, and bone marrow. The child had a scaphocephalic skull and brain injury was classified as secondary hypoxic due to anemia. In the bone marrow, thymus, and brain small histiocytic aggregates were thought to be unspecific secondary inflammatory reactions. The placenta was markedly hypertrophic with hydropic villi and immunohistochemistry was negative for parvovirus B19, cytomegalovirus, and herpes virus 1/2.
An autoimmune anemia was considered to be the most likely cause of the pathologies. After years, the mother was diagnosed with Gaucher disease. Retrospective re-evaluation revealed that the aggregated histiocytes were Periodic acid-Schiff-diastase-positive (Figure 3, Supplemental Table 1). Therefore, the autopsy diagnosis was consistent with a neonatal Gaucher disease.
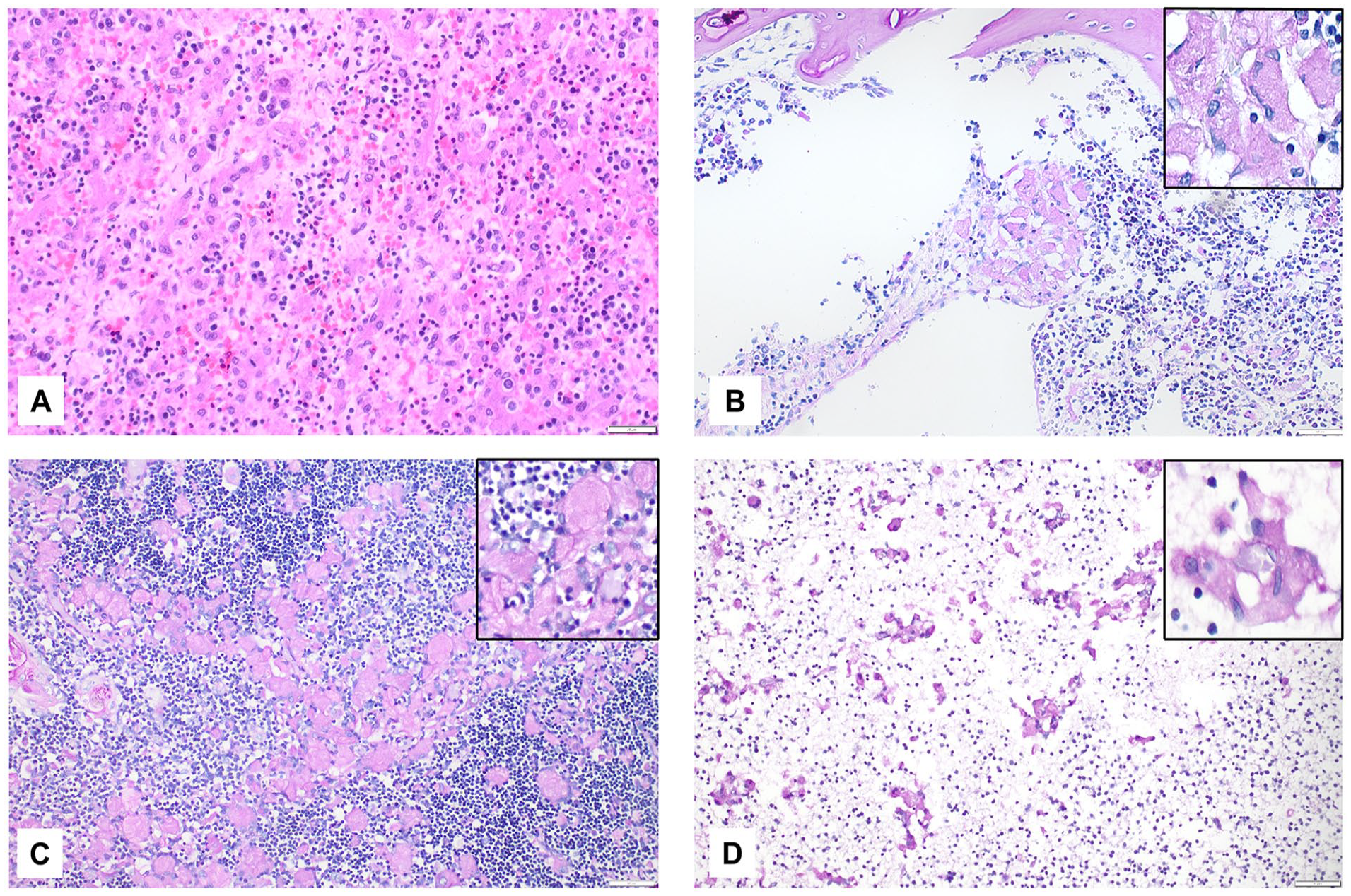
Case #3 Neonatal Gaucher disease with hyperplasia of erythropoiesis and anemia-associated chronic hypoxic brain damage. (A) Liver with hyperplastic erythropoiesis; HE, 200x magnification, scale bar 20 µm. (B) Bone marrow with atypical Periodic acid-Schiff-diastase (PAS-D)-positive histiocytes as a surrogate for Gaucher disease; 200x magnification, 20 µm, insert 400x. (C) Thymus with atypical PAS-D-positive histiocytes; 200x, 20 µm, insert 400x. (D) Neocortex with atypical PAS-D-positive histiocytes; 200x, 20 µm, insert 400x.
Placenta Evaluation
A subfraction of corresponding placentas were sent in for examination (n = 8/27; 30%). Most placentas were hypotrophic (n = 3/8; 38%) or hypertrophic (n = 3/8; 38%) and 2 cases (25%) had a normal size/weight for the gestational age (Table 1). Further pathologies were delayed maturation (n = 1/8; 13%), minor or major maternal vascular malperfusion (n = 3/8; 38%), fetal vascular malperfusion (n = 1/8; 13%), and acute chorioamnionitis (n = 2/8; 25%). Two cases (25%) showed no histological placenta pathologies, one with normal placenta size/weight and the other had a hypotrophic placenta.
Discussion
Several studies have discussed the diagnostic value of perinatal autopsy in order to evaluate the most likely cause of death.1,6,9,10,12-16 However, the inconsistent definition of “intrauterine,” “perinatal,” or “neonatal” death with overlapping time frames in different studies makes a comparison difficult (Table 3).1,6,9,10,12-16 Studies concerning “perinatal” death include intrauterine death in the 20th gestational week9,13,17-22 and extend beyond 1 year of life 23 (Table 3). While pathological changes in the placenta are relatively frequently associated with intrauterine fetal deaths, it is thought that in peri/neonatal deaths placenta pathologies are rarely sufficient to explain the cause of lethal organ failure.24,25
Review of the Literature.
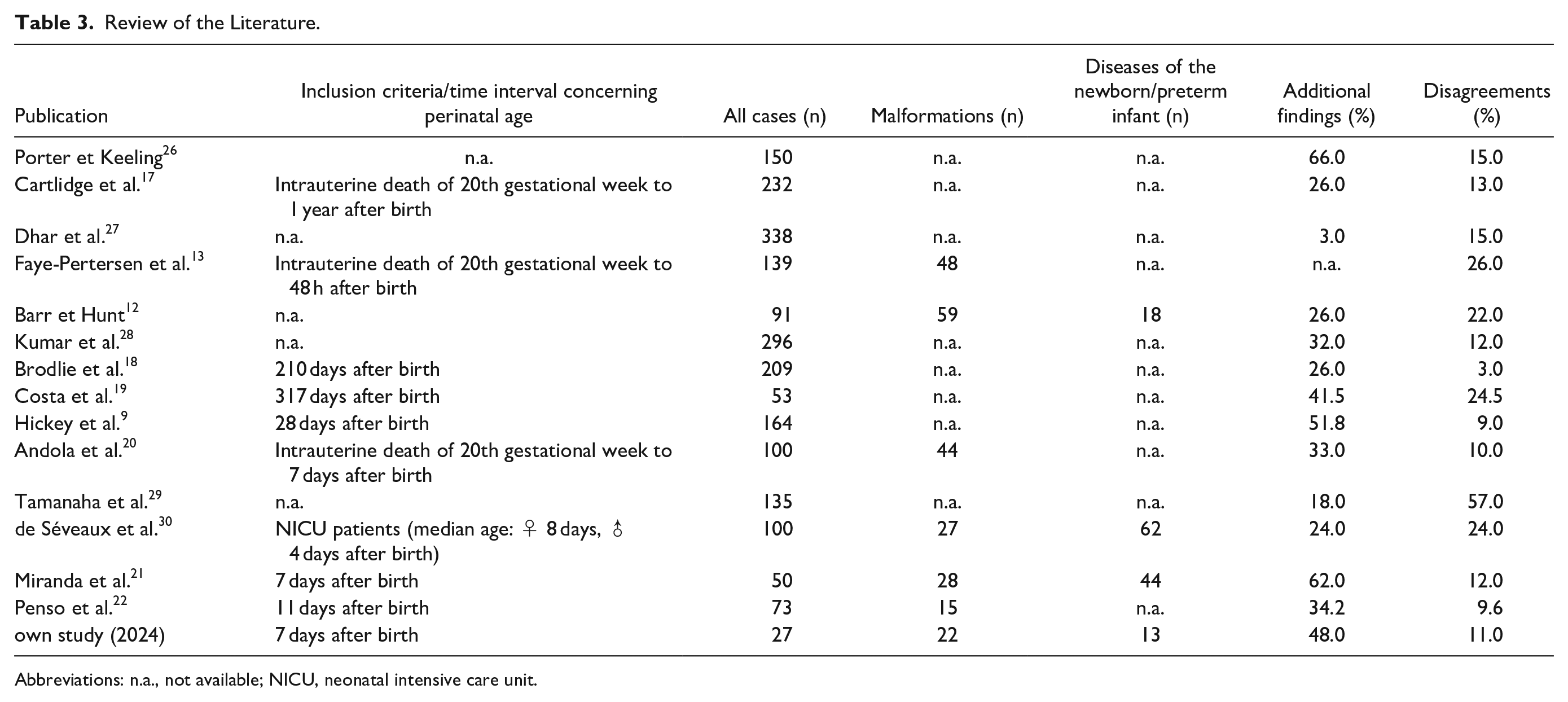
Abbreviations: n.a., not available; NICU, neonatal intensive care unit.
In a meta-analysis by Rossi and Prefumo the authors reported mean 9% major discrepancies in prenatal/fetal autopsies. 6 In perinatal autopsies, including pre- and postnatal cases, major discrepancies were found in mean 13% of cases9,12,13,17-21,26-30 (Table 3). Similar to Miranda et al., 21 we focused on autopsies after death within the first 7 days of life and major discrepancies could be identified in 12% of cases 21 and 11% (own study). In our previous study on prenatal/fetal autopsies the frequency of major discrepancies was relatively low (2%), 31 but in general a frequency of approximately 10% of major discrepancies in pre- and postnatal autopsy cases can be expected.
As could be expected, lung abnormalities were more frequent in postnatal than prenatal autopsy cases (56% vs 8%; Supplemental Table 2). 31 In early neonatal deaths, malformations and immaturity of the lung are the main factor for respiratory distress and death.32,33 Interstitial pulmonary pathologies are often undetectable by sonography. 32 In our cohort, in case #1 the interstitial lung maturation defect mimicked a total anomalous pulmonary venous connection. Therapeutic management would probably have been similar to that in most neonatal lung diseases (DD2 according to modified Goldman criteria), but the finding of a primary lung maturation defect may help to specify human genetic counseling.
Fetal rhombencephalitis is very rare and can be associated with a listeria monocytogenes infection. 34 Other infectious causes may be viruses such as herpes simplex virus 1 and 2. 23 In general, the cause of inflammation may be difficult to diagnose before death and herpes-virus-associated brainstem encephalitis has a poor outcome. 35 In case #2 the rhombencephalitis most likely manifested shortly before birth or in the early neonatal period. A specific pathogen could not be found, but an antecedent viral infection or, less likely, an autoimmune inflammation may be possible. It must be taken into account that the autopsy diagnosis of inflammatory brain diseases is depending on systematic sampling for histology and an evaluation by a neuropathology specialist could be helpful. Vice versa, sampling errors or autolysis may result in missing a relevant diagnosis. According to the modified Goldman criteria, we classified this case as “DD2”, because it is debatable whether corticoid therapy would have significantly prolonged the survival. In addition, perinatal rhombencephalitis is a very rare differential diagnosis and therefore, during lifetime of the newborn, specific brain stem imaging and serologic screening for viruses were not necessarily indicated; in persistent inflammation after virus elimination, virology would be negative.
In case #3 the aim for initiating an autopsy, was to evaluate the unusual fetal anemia and organ malformations, including a suspected primary brain malformation. In general, fetal anemia can be caused by various pathogens and autoimmune diseases, the most common being parvovirus B19 and maternal alloimmunization. 36 Other rarer causes are chromosomal/genetic defects and vascular tumors such as large chorangiomas of the placenta. 36 In case #3, non-viral autoimmunologic pathology appeared to be the most likely cause of anemia. Later on, a maternal Gaucher disease was diagnosed and, retrospectively, features of Gaucher disease were found in the autopsy tissue specimens as well. Gaucher disease is a rare autosomal-recessive lysosomal storage disease with less than 1% of cases with lethal perinatal disease. 37 On the one hand, this case shows the difficulty to discriminate histopathologic surrogates of vary rare diseases from other differential diagnoses, in this case histiocytic aggregates. On the other hand, with additional clinical information, autopsy results allow the definitive identification of the lethal neonatal pathology.
Conclusion
In most cases, post-mortem examination following neonatal death in a hospital, non-forensic setting can verify the clinical diagnosis. In few cases, autopsy can identify major macroscopic and microscopic findings, which were clinically not suspected or interpreted as other pathologies. In these cases, a major change in therapeutic management is often unlikely, but it may help the parents and the clinical team to understand the cause of the acute organ failure as well as provide additional information for human genetic consultation.
Supplemental Material
sj-xlsx-1-pdp-10.1177_10935266241288869 – Supplemental material for Comparison of Clinical Diagnosis and Autopsy Findings of Early Neonatal Deaths: Diagnostic Challenges and the Value of Autopsy in Identifying Rare Pathologies
Supplemental material, sj-xlsx-1-pdp-10.1177_10935266241288869 for Comparison of Clinical Diagnosis and Autopsy Findings of Early Neonatal Deaths: Diagnostic Challenges and the Value of Autopsy in Identifying Rare Pathologies by Jan-Theile Suhren, Kais Hussein, Hans Kreipe and Nora Schaumann in Pediatric and Developmental Pathology
Supplemental Material
sj-xlsx-2-pdp-10.1177_10935266241288869 – Supplemental material for Comparison of Clinical Diagnosis and Autopsy Findings of Early Neonatal Deaths: Diagnostic Challenges and the Value of Autopsy in Identifying Rare Pathologies
Supplemental material, sj-xlsx-2-pdp-10.1177_10935266241288869 for Comparison of Clinical Diagnosis and Autopsy Findings of Early Neonatal Deaths: Diagnostic Challenges and the Value of Autopsy in Identifying Rare Pathologies by Jan-Theile Suhren, Kais Hussein, Hans Kreipe and Nora Schaumann in Pediatric and Developmental Pathology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.