
Abstract
Umbilical cord hemangiomas are rare lesions, for which data on pregnancy outcome is lacking. This study combines a multi-institution 4-case series with a systematic literature search (n = 52) to determine possible pathologic lesion parameters which may have an effect on pregnancy outcome. Of all 56 pregnancies, lesion size ranged from 0.2 to 23.0 cm with pregnancy outcomes ranging from healthy liveborns (58.9%), liveborns with severe complications largely due to prematurity and/or fluid overload (12.5%), intrauterine/neonatal demise (25.0%), and pregnancy termination (3.6%). Of the 52 cases included for statistical analysis, there was no significant association between fetal outcome and vascular lesion location (P = .12) or fetal outcome and single umbilical artery involvement versus involvement of other vasculature (P = .29). The mean length of vascular lesions that resulted in healthy liveborns did not significantly differ from those resulting in severe fetal complications and/or demise (P = .72). Cases resulting in severe complications and/or demise were significantly earlier at delivery than those resulting in healthy liveborns (P < .001). Combined findings suggest that functional lesion characteristics, such as the degree of turbulent flow generated, have more significance than size, especially in early gestation losses. Moving forward, standardized reporting of pathologic lesion characteristics is paramount to better predict pregnancy prognosis.
Introduction
Umbilical cord hemangiomas are rare lesions that present incidentally on ultrasound or with findings ranging from increased maternal serum alpha-fetoprotein to polyhydramnios, respiratory distress and/or intrauterine fetal demise secondary to hydrops, cord rupture, or cord stenosis. These lesions often manifest varying amounts of extravasated fluid and/or cystic Wharton jelly change due to their resultant turbulent flow, and hence have been occasionally referred to as “angiomyxomas.”
As in any other body site, pathologic diagnosis of a cord hemangioma consists of microscopic visualization of vascular channels lined by simple, cytologically bland endothelial cells that exhibit immunoreactivity for vascular markers such as CD31 and VWF. Use of Glut-1 immunostaining has been suggested to differentiate between hemangiomas of infantile origin and chorangiomas with cord involvement or a true umbilical cord hemangioma arising from remnant vitelline vessels.1-3
The literature of umbilical cord hemangiomas is limited to single reports over the past 70 years including a historical 4-case series. 4 Typically, lesion parameters reported included size, degree of cystic change, and involved umbilical vasculature; however, reporting consistency has been spotty. As a result, little is known about their prognosis or any pathologic characteristics that may help predict pregnancy outcome. This multi-institution case series combines 4 new cases with those from the literature to determine the utility of various pathologic lesion parameters toward informing pregnancy prognosis.
Case Series
Following institution ethics approval, we conducted a retrospective search of our electronic pathology databases for relevant cases accessioned 01/01/2010 to 01/01/2022 using the search terms “vascular anomaly of umbilical cord,” “arterial anomaly of umbilical cord,” “venous anomaly of umbilical cord,” “umbilical cord hemangioma,” and “umbilical cord angiomyxoma.” The search yielded 2 cases from Health Science Centre, Winnipeg, Canada, 1 case from Seattle Children’s Hospital, Seattle, USA, and 1 case from the University of Alabama Hospital, Birmingham, USA. Salient clinical and pathologic findings are summarized in Table 1.
Clinical and pathologic characteristics of umbilical cord hemangioma cases by systematic literature search.
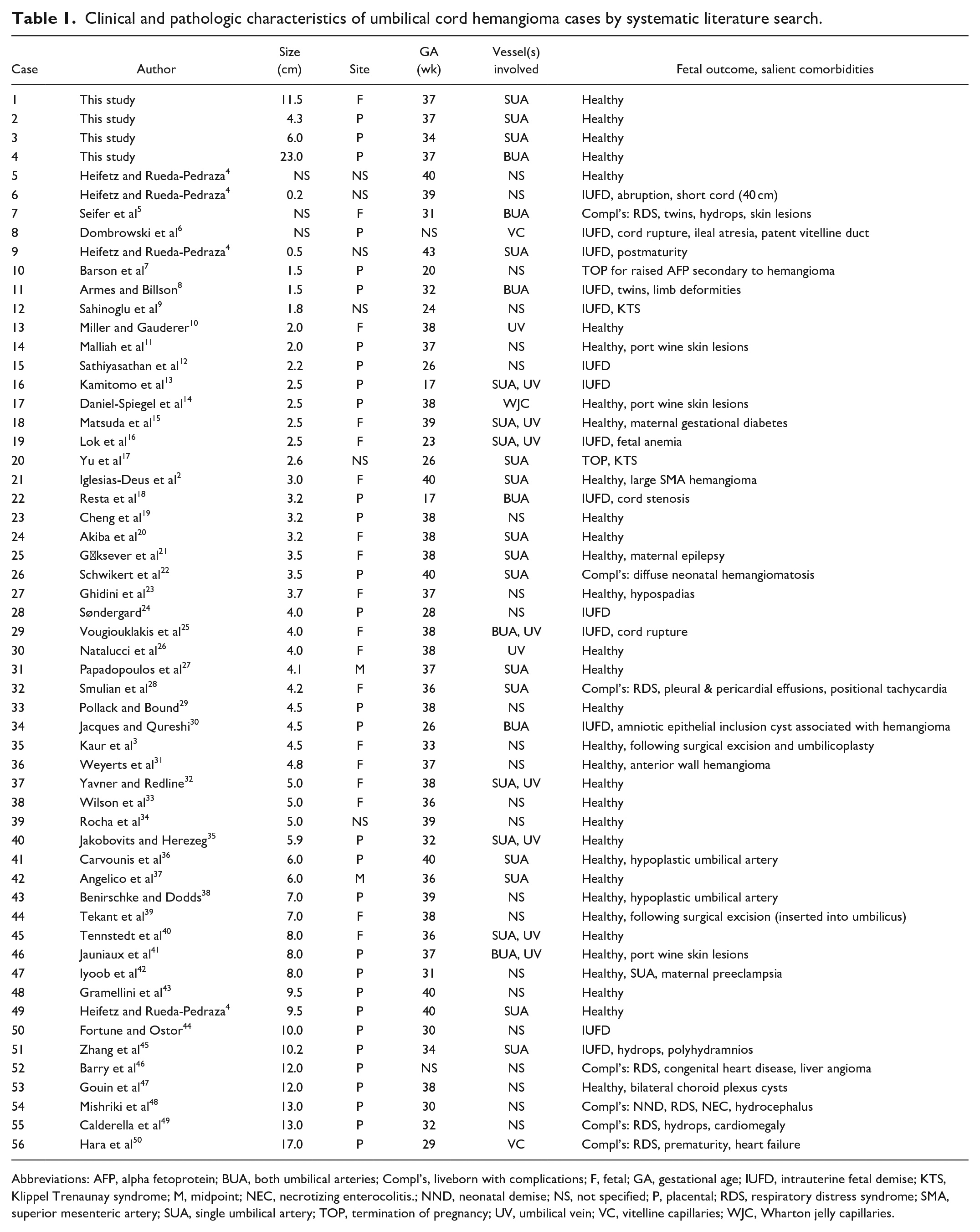
Abbreviations: AFP, alpha fetoprotein; BUA, both umbilical arteries; Compl’s, liveborn with complications; F, fetal; GA, gestational age; IUFD, intrauterine fetal demise; KTS, Klippel Trenaunay syndrome; M, midpoint; NEC, necrotizing enterocolitis.; NND, neonatal demise; NS, not specified; P, placental; RDS, respiratory distress syndrome; SMA, superior mesenteric artery; SUA, single umbilical artery; TOP, termination of pregnancy; UV, umbilical vein; VC, vitelline capillaries; WJC, Wharton jelly capillaries.
Case 1
A 36-year-old G1P0 mother was diagnosed on prenatal ultrasound with a 12 cm vascular UC mass. She was closely followed and delivered a healthy infant by Cesarian section at 37 weeks following spontaneous membrane rupture (APGAR score 9 at both 1 and 5 minutes). On gross placental examination, the UC was massively distended by a 11.5 cm tumor located 49 cm from disc insertion (Figure 1(a)). Sectioning revealed associated marked edema and cystic-type change of the Wharton jelly proximal to the lesion. Histologic examination confirmed a cytologically bland endothelial proliferation originating from an umbilical artery (Figure 2(a) and (b)). The endothelial cells were CD34-immunoreactive while negative for Glut-1 (Figure 2(d)) and D2 to 40.
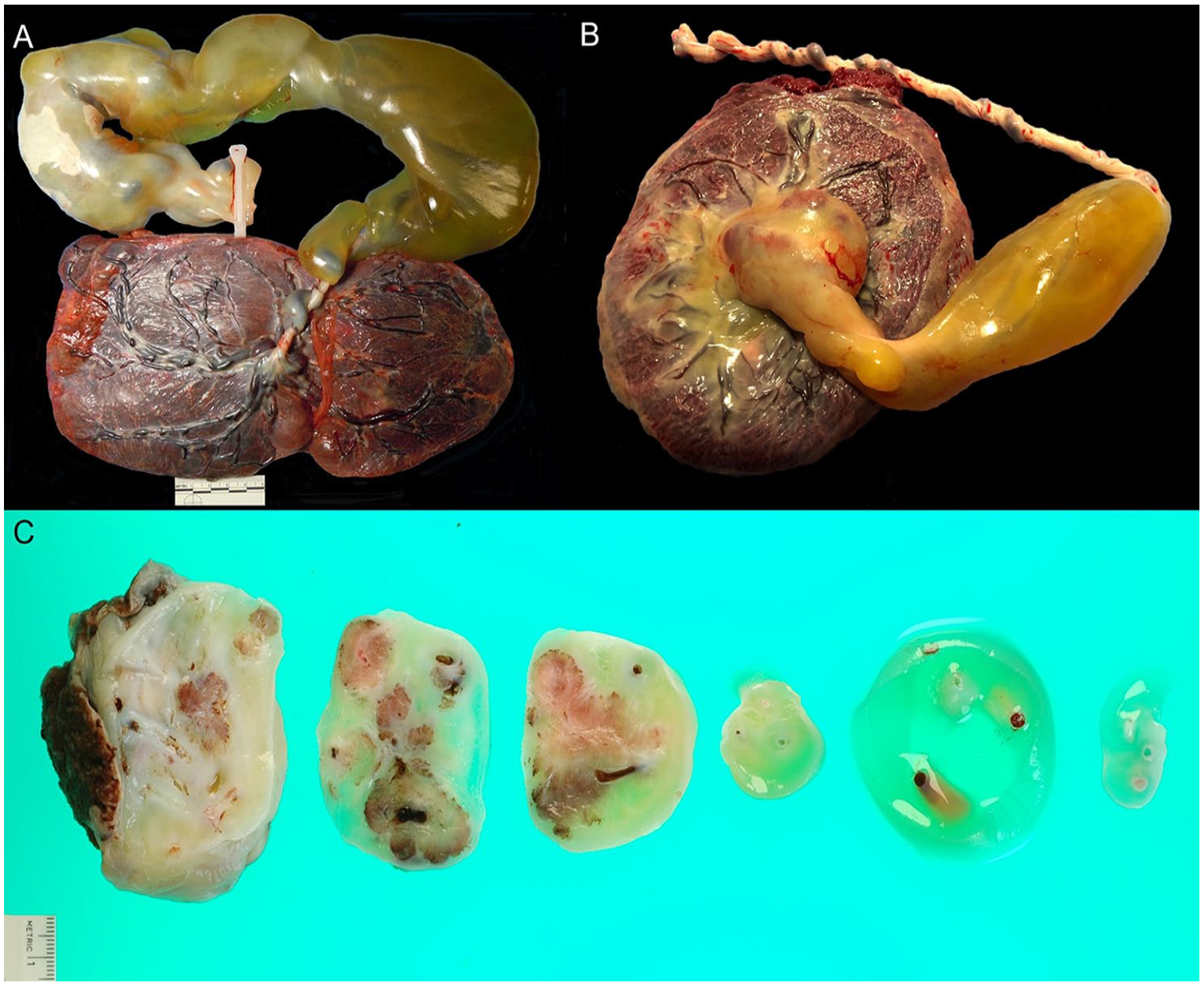
Placental gross examination in cases of umbilical cord hemangiomas (Case 1: A, Case 3: B) demonstrated massive, well demarcated, fusiform Wharton jelly edema involving a portion of the umbilical cord. Cut section of the lesion in Case 3 revealed nodules arising from an umbilical artery (C).
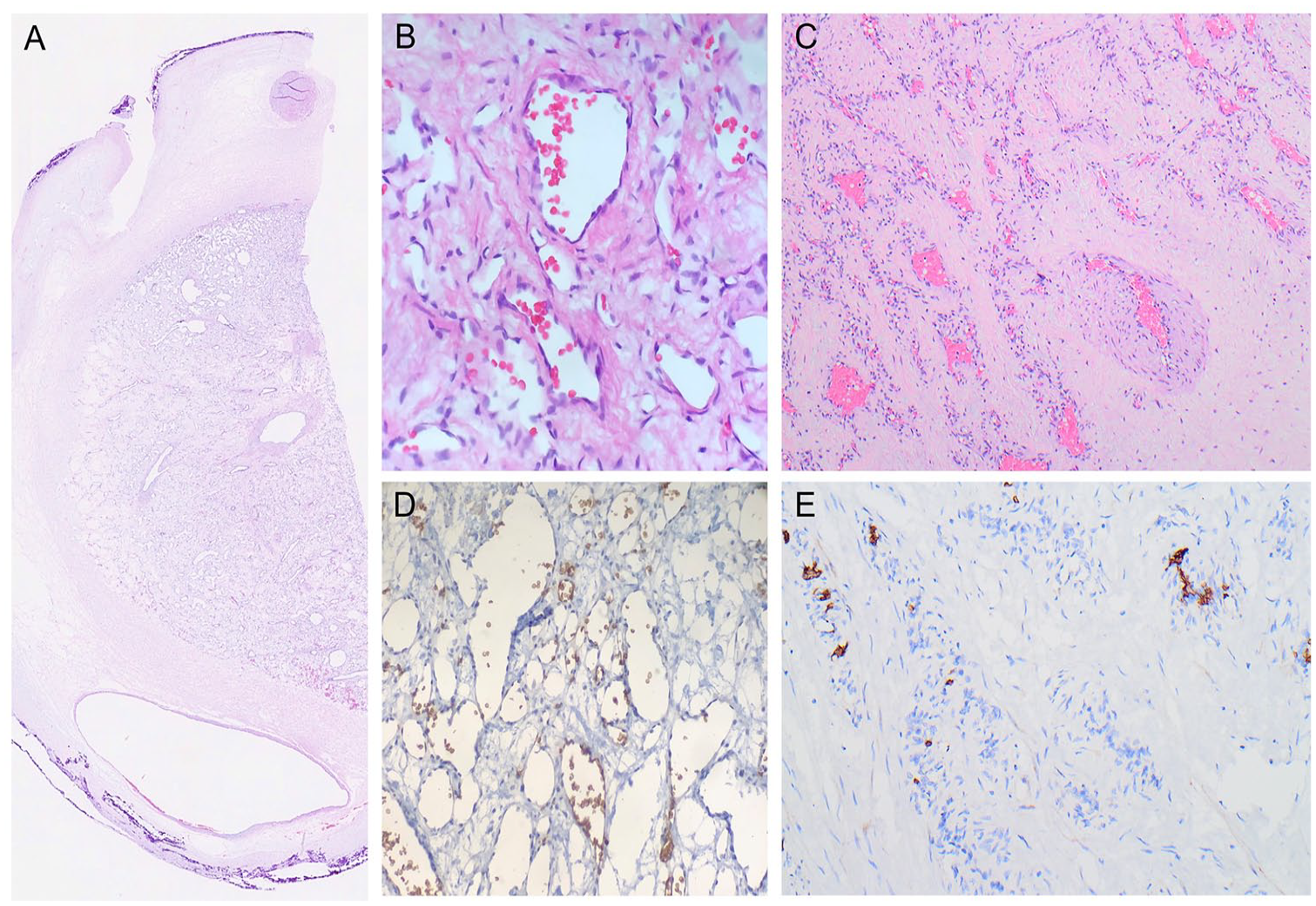
Microscopic examination in Cases 1 (H&E A: 20×, B: 400×) and 3 (H&E C: 100×) revealed cytologically bland, GLUT-1 negative (Case 1: D, 400×; Case 3: E, 200×), endothelial cell proliferations in keeping with diagnoses of umbilical cord hemangiomas.
Case 2
A 34-year-old G4P3 mother delivered a healthy infant by Cesarian section at 34 weeks following spontaneous preterm premature membrane rupture and footling breech presentation (APGAR score 9 at both 1 and 5 minutes). Maternal serum screen at 15 weeks had identified increased alpha fetoprotein (92.9 μg/L) and nuchal translucency (1.4 mm); however, prenatal ultrasounds at 12, 16, 21, and 29 weeks were normal. On gross placental examination, there was a 4.3 cm tumor located immediately adjacent to the disc insertion. Histologic examination confirmed a benign endothelial proliferation arising from an umbilical artery.
Case 3
Ultrasonography in a 31-year-old mother at 20 weeks of gestational age demonstrated a large umbilical cord mass with Doppler flow. The mother was closely followed, and labor was induced at 34 weeks. She delivered a healthy liveborn infant. Gross examination revealed a firm, pale pink mass measuring 6 cm in length × 3.5 cm in maximal diameter within the proximal umbilical cord (Figure 1(b) and (c)). Cut surface showed a tumor composed of multiple interconnected nodules within increased Wharton’s jelly, intimately surrounding the umbilical vessels. The mass approached to within 3 mm of the chorionic plate surface, but appeared distinct from it. A separate region of the distal cord, 4 cm from the proximal mass, also displayed massive dilation up to 6 cm for a length of 17 cm, with cystic dilation on cut surface, but was not directly involved by the vascular mass. Dye injection demonstrated perfusion of the mass by 1 umbilical artery, but no connection to the umbilical vein. The other umbilical artery contained thrombi that prevented perfusion. Histologically, the mass displayed a multilobulated vascular proliferation. The majority of the tumor appeared composed of arborizing small capillaries, with a few larger muscularized feeder vessels, several of which appeared to arise from 1 umbilical artery. Cells showed bland cytologic features with no mitotic figures (Figure 2(c)). Glut-1 immunohistochemical staining was negative in the vascular lesion, with good controls (Figure 2(e)). Cystic changes in the Wharton’s jelly surrounding the tumor and in the separate dilated region of umbilical cord showed myxedematous, paucicellular Wharton’s jelly with cystic regions lacking epithelial or endothelial lining.
Case 4
A 36-year-old G5P2 mother at 37 weeks gestation, complicated by polyhydramnios underwent spontaneous vaginal delivery. The newborn weighed 3080 g. Gross examination revealed a fusiform lesion of the umbilical cord measuring 23 cm × 6.5 cm near the placental insertion site. The lesion was sharply demarcated from the remainder of the umbilical cord, which was normal in caliber, but hypercoiled at 15 coils per 10 cm. Sectioning the fusiform lesion revealed a variegated red-tan cut surface with focal hemorrhage and associated diffuse edema and hemorrhage. Histologically, the lesion was composed of cytologically bland arborizing small capillaries, which appeared to intercalate within the walls of both umbilical arteries as feeder vessels. The lesion was completely distinct from the umbilical vein.
Literature Search and Statistical Analysis
A Pubmed search of the English-language literature using search terms “umbilical cord hemangioma” and “umbilical cord angiomyxoma” yielded 52 additional cases, for which salient clinical and pathologic findings are also summarized with the aforementioned case series in Table 1. For statistical comparison, fetal outcome was divided into 1 group comprised of liveborns without complications and a second group comprised of those with severe complications and/or resultant demise. One pregnancy terminated solely on the basis of elevated serum alphafetoprotein, which was retrospectively presumed due to the hemangioma, 7 was excluded from the analysis. A second pregnancy terminated for Klippel Trenaunay syndrome, 17 was also excluded from the analysis. A Fisher exact test was used to assess for differences between fetal outcome and lesion location along the umbilical cord (i.e., fetal vs placental end) as well as whether fetal outcome was different if the vascular lesion only involved a single umbilical artery as opposed to other combinations of umbilical vessel involvement. A 2-tailed t-test was used to assess for a difference in fetal outcome with vascular lesion size. Statistical significance was defined as P < .05. Cases missing the aforementioned parameters were excluded from those specific comparisons. Due to small sample size, cases which designated the hemangioma location as the cord “midpoint” (n = 2) were excluded from the lesion location comparison.
Results
Of all combined 56 pregnancies, lesion size ranged from 0.2 to 23.0 cm in maximum dimension. Thirty-three pregnancies (58.9%) resulted in healthy liveborns, 7 (12.5%) resulted in liveborns with severe complications, 14 (25.0%) resulted in intrauterine or neonatal demise, and 2 pregnancies (3.6%) were terminated for an elevated serum alphafetoprotein, 7 and Klippel Trenaunay syndrome, 17 respectively. Apart from diffuse neonatal hemangiomatosis, 22 severe complications in surviving infants were largely due to prematurity and/or fluid overload.
Eighteen (32.1%) lesions were located at the fetal end, 30 (53.6%) were at the placental end, 2 (3.6%) were at the cord midpoint, and 6 (10.7%) did not specify a cord location. Two (3.6%) cases involved all 3 umbilical vessels, 5 (8.9%) involved both umbilical arteries, 15 (26.8%) involved 1 umbilical artery, 2 (3.6%) involved only the umbilical vein, 6 (10.7%) involved an umbilical artery and the umbilical vein, 2 (3.6%) involved the vitelline capillaries, 1 (1.8%) involved the Wharton jelly capillaries, and 23 (41.1%) did not specify which umbilical vessels were involved.
Of the 52 cases included for statistical analysis, there was no significant association between fetal outcome and vascular lesion location (P = .12) or fetal outcome and single umbilical artery involvement versus involvement of other vasculature (P = .29). The mean length of vascular lesions that resulted in healthy liveborns (mean ± standard deviation: 6.1 ± 4.0 cm) did not significantly differ from those resulting in severe fetal complications and/or demise (5.6 ± 5.0 cm; t = 0.36, P = .72). Cases resulting in severe complications and/or demise were significantly earlier in gestation at delivery than those resulting in healthy liveborns (liveborn: 37.2 ± 2.3 weeks; demise: 30.1 ± 7.1 weeks; t = -5.41, P < .001).
Discussion
Although a seemingly simple pathologic diagnosis, umbilical cord hemangiomas are high risk lesions by virtue of their precarious location and potential for catastrophic effects on the developing fetus. This is the first case series of umbilical cord hemangiomas that combines those previously reported in the literature to generate rudimentary data as to which pathologic reporting parameters may be associated with pregnancy outcome. One might assume that a larger lesion would confer a poorer pregnancy prognosis but our analysis showed that the mean size of hemangiomas in pregnancies resulting in severe fetal complications and/or demise did not significantly differ than those resulting in good pregnancy outcome. This finding, combined with the observation that the pregnancies resulting in fetal demise occurred at a significantly lower gestational age, suggests that functional lesion characteristics, such as the degree of turbulent flow generated, have more significance than its size, especially in early gestation losses. That being said, the data may also be confounded by the lack of a standardized method to obtain the lesion size. Some publications specify the size of the hemangioma itself separately from the degree of cystic change, while other publications seem to combine the 2 parameters.
The lack of association between single umbilical artery involvement and better prognosis was unexpected and perhaps reflective of sample size limitations. Twenty-two of the 52 cases reported in the literature did not specify which umbilical vasculature the hemangioma involved. The lack of association between pregnancy outcome and fetal versus placental location was less hampered by sample size. Only 6 previous publications did not report the cord location and 2 reported the cord location as midpoint and were therefore omitted from analysis.
There are occasional cases associated with systemic congenital vascular anomalies such as Klippel Trenaunay syndrome and diffuse neonatal hemangiomatosis. Presence of these systemic congenital vascular anomalies in the developing fetus increase risk for hematologic complications such as localized intravascular coagulopathy. 51 There are no reports of cord hemangiomas in patients with aneuploidy or heritable syndromes.
The purported origins and nomenclature of hemangiomas involving the umbilical cord are not well established. Kaur et al’s 3 recent case report suggests that the term “hemangioma” be reserved for lesions representing true infantile hemangiomas based on presence of Glut-1 expression whereas the term “angiomyxoma” should be used in proliferations that are negative Glut-1, therefore implying an origin from remnant vitelline duct vessel remnants within the umbilical cord. This proposed definition is meant to fall in line with previous assertions made for cutaneous vascular anomalies that Glut-1 negative lesions represent vascular malformations as opposed to true neoplastic processes. 52 We feel without evidence of Wharton jelly contribution to the neoplastic process, use of the term “angiomyxoma” is misleading. That being said, future studies evaluating for a difference in pregnancy prognosis between Glut-1-positive and Glut-1-negative vascular umbilical cord lesions may be of value. Until such data becomes available, the utility of Glut-1 staining in this context remains to be seen.
Moving forward, more robust sample sizes with consistent documentation of pathologic features and fetal outcomes are paramount to progress our understanding of these lesions.
Footnotes
Acknowledgements
The authors would like to thank Dr. Raj Kapur and maternal-fetal medicine specialists Dr. Rachelle Govia and Dr. Jennifer Hunt for their assistance with acquiring cases for this study.
Authors’ Note
One of the cases and preliminary literature review were presented in poster format at the November 2021 Society for Pediatric Pathology fall meeting.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.