
Abstract
Extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma) is an indolent non-Hodgkin lymphoma rarely seen in pediatric patients. MALT lymphoma most commonly involves the gastrointestinal tract or peri-orbital tissues, potentially as sequela of chronic antigenic stimulation or immune dysregulation. Rare cases of MALT lymphoma arising from the gynecologic tract have been reported in older adult patients. We present the unique case of a 16-year-old postpubescent female with MALT lymphoma localized to the gynecologic tract, who initially presented with abdominal fullness, abnormal uterine bleeding, and obstructive acute kidney injury secondary to urinary outflow obstruction. Intraoperatively, dense fibrosis of the uterus and left fallopian tube was noted which mimicked abdominal cocoon syndrome. She was treated with 6 cycles of bendamustine and rituximab with complete anatomic and metabolic remission. In this report we highlight a very unusual presentation of a rare malignancy in the pediatric population as well as unique treatment considerations given this patient’s young age and tumor location.
Keywords
Introduction
Extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma) is a rare, indolent mature B-cell neoplasm that accounts for less than 2 percent of all pediatric non-Hodgkin lymphomas. 1 Often associated with chronic infections, such as Helicobacter pylori, or immune dysregulation in adults, MALT lymphoma presents at a median age of ~66 years, with incidence increasing exponentially with age.2-4 MALT lymphoma arises most frequently from in stomach, and less commonly in the ocular adnexa; however, other primary sites have been reported, including the salivary gland, lung, spleen, breast, and skin. 4 The gynecologic tract is an extremely rare primary site of disease, with only sporadic cases reported in the fourth to eighth decades of life.5-10 Here we present an unusual case of a MALT lymphoma arising from the gynecologic tract of a postpubescent pediatric patient.
Case Report
An otherwise healthy 16-year-old female with no significant past medical history presented with 3 weeks of abnormal uterine bleeding, left lower extremity pain with progressive swelling, and 2 months of increased lower abdominal fullness. Initial laboratory evaluation demonstrated renal injury with a creatinine of 5.9 mg/dL, blood urea nitrogen (BUN) of 38 mg/dL, potassium of 6.4 mEq/L, and phosphorus of 6.7 mg/dL. Her hemoglobin was 8.1 g/dL, and her platelet count was 366,000/mm3. D-dimer was 3.0 µg/mL. Lactate dehydrogenase (LDH) was normal. The patient reported sexual activity with a single partner; pregnancy testing was negative as was testing for gonorrhea, chlamydia, human immunodeficiency virus (HIV), syphilis, and hepatitis B and C. A lower extremity ultrasound was negative for deep venous thrombosis; however, abdominal ultrasound showed severe bilateral hydroureteronephrosis, a heterogeneously enlarged uterus and cervix, an indistinct bladder-uterine interface, and enlarged bilateral ovaries. Magnetic resonance imaging of the pelvis (Figure 1) demonstrated diffuse cervical and uterine enlargement with lobulation concerning for a malignant process. Physical examination was notable for a firm lower abdominal mass extending 4 cm above the pubic symphysis. On bimanual examination, the distal 3 cm of vagina was palpably normal; the proximal vagina and pelvic structures were fixed and firm. An immobile, nodular mass measuring 8 cm occupied the posterior cul-de-sac on rectovaginal examination.
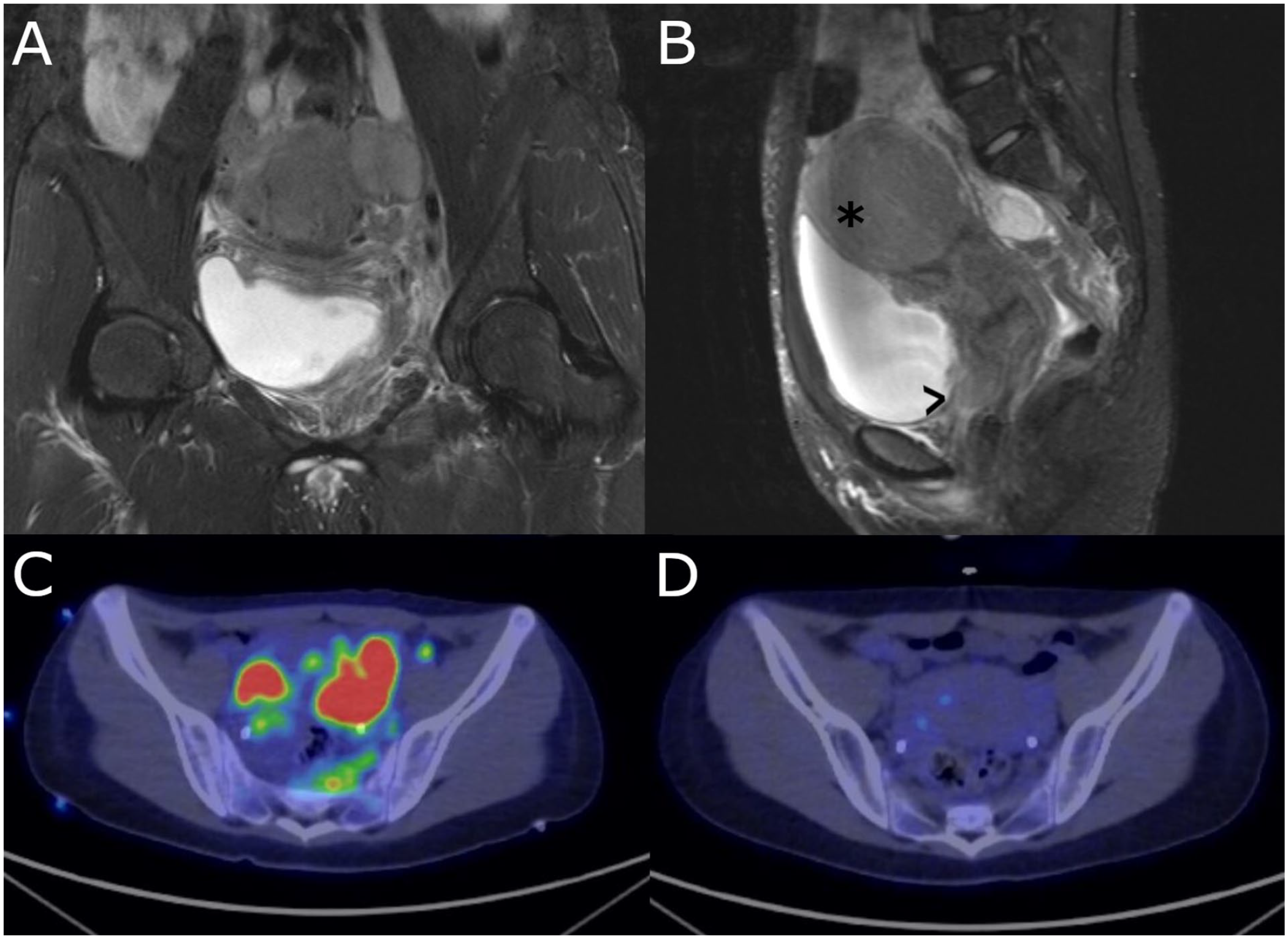
Cross-sectional imaging of the patient’s abdomen. (A) Coronal and (B) sagittal STIR images of the pelvis at presentation demonstrate a lobulated and heterogenous mass of the uterus (asterisk), cervix and vagina (arrow), and surrounding tissues. (C) Axial FDG-PEG image prior to treatment demonstrates extensive hypermetabolic soft tissue signal in the uterine and peri-uterine regions as well as retroperitoneal lymph nodes. (D) Axial FDG-PET image following 2 cycles of treatment with rituximab and bendamustine shows resolution of abnormal hypermetabolic signal.
Following emergent stabilization of her electrolytes, the patient underwent urgent placement of bilateral percutaneous nephrostomy tubes. Cystoscopy during the procedure showed external compression of the bladder neck, trigone, and dome without mucosal penetration. On laparoscopic visualization, the uterus, left fallopian tube, and left ovary were enlarged; the right ovary was not visualized. The uterus and left fallopian tube were largely covered with dense fibrous material, described intraoperatively as being “hard as a rock” and adherent to the left pelvic sidewall, with an appearance reminiscent of abdominal “cocoon syndrome.” Left salpingectomy was performed to obtain diagnostic tissue while preserving fertility.
On gross examination, the fallopian tube was firm, tan-pink, 5.5 cm long, and 0.8–2.0 cm in diameter with intact fimbriae and focal fibrous adhesions on the serosal surface. Upon sectioning, the fallopian tube wall was markedly thickened. On histologic examination, hematoxylin and eosin (H&E) stained sections showed a diffuse atypical lymphoid infiltrate composed of small-to-intermediate sized cells with round to ovoid nuclei, somewhat irregular nuclear borders, slightly coarse chromatin, inconspicuous/absent nucleoli, and small amounts of cytoplasm. Scattered plasma cells were present in the background. These atypical lymphocytes expanded and distorted the fallopian tube fimbriae, densely infiltrated the muscular wall, and involved the broad ligament (Figure 2). The neoplastic lymphocytes further extended into the adjoining serosal soft tissue. No well-formed lymphoepithelial lesions were identified and no areas of nodular growth were appreciated. Accompanying stromal desmoplasia was present.
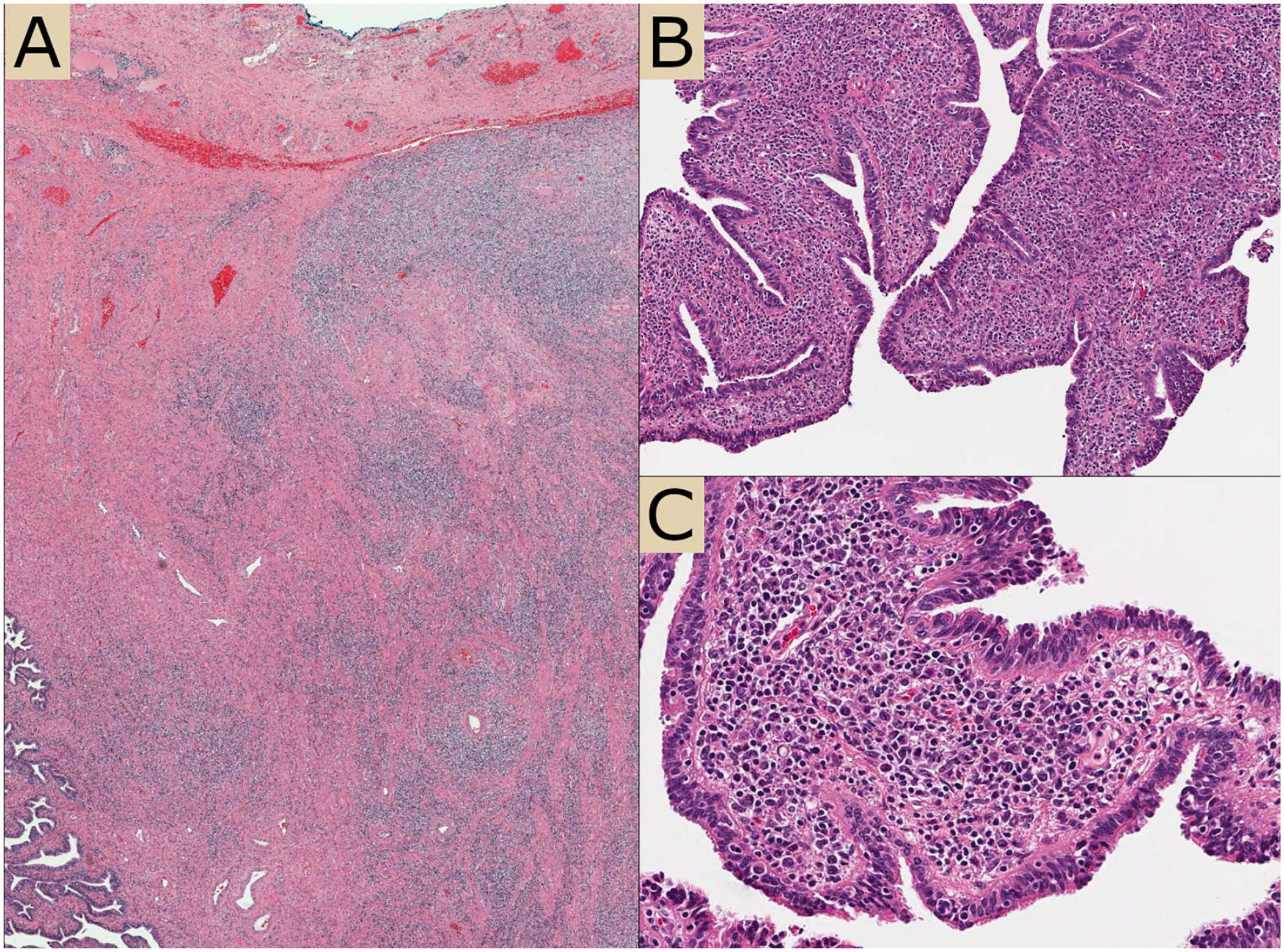
Histologic images of the neoplastic infiltrate. (A) Representative section showing extensive involvement of fallopian tube and adjacent tissues. (B) Distortion of fallopian tube fimbriae by neoplastic cells. (C) High power image.
Immunohistochemical stains performed on the formalin-fixed, paraffin-embedded tissue demonstrated the infiltrating lymphocytes were B-cells co-expressing CD20, CD43, CD45, and CD79a (Figure 3) without CD10 or ALK1. No follicular dendritic cell meshworks were identified by staining for CD21. Kappa and lambda immunohistochemical stains were performed but were difficult to interpret and did not show clear light chain restriction. In-situ hybridization for EBER was negative. The Ki67 proliferation index was low (<5%). Flow cytometry was attempted on a portion of the fresh tissue, but evaluation was limited by poor specimen viability. B-cell clonality testing demonstrated a clonal rearrangement of the IGH gene (270bp; BIOMED-2 FR2 primer set), supporting a diagnosis of an extranodal marginal zone lymphoma of the gynecologic tract. Subsequent molecular interrogation by a next-generation sequencing panel identified the presence of a mutation in CHEK2 c.470T>C with a variant allele frequency of 49%.
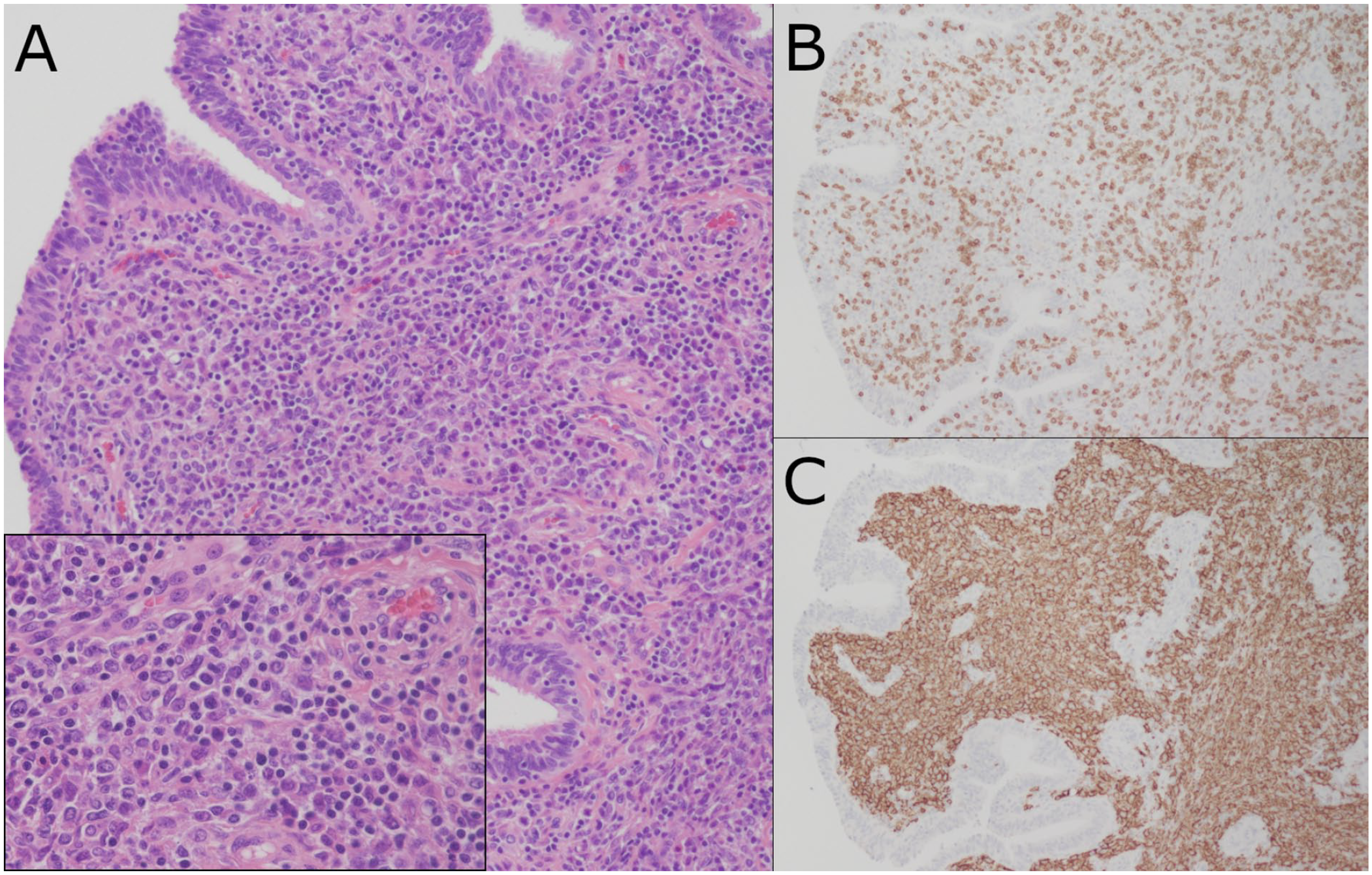
(A) H&E-stained section demonstrating neoplastic lymphocytes with round to ovoid nuclei, irregular nuclear borders, slightly coarse chromatin without prominent nucleoli and small amounts of cytoplasm (with inset showing higher magnification). Immunohistochemical stains highlighting the (B) background CD3+ T-cells and the (C) diffusely infiltrating CD20+ neoplastic cells.
Examinations of the cerebrospinal fluid and bone marrow were negative for disease involvement. Staging positron emission tomography demonstrated extensively hypermetabolic soft tissue throughout the pelvis without metastatic disease (Figure 1(c) and (d)). The patient was treated with 6 cycles of rituximab and bendamustine according to MALT2008-01, a multicenter phase 2 trial of adult patients. 11 She achieved complete anatomic and metabolic remission following 2 cycles of treatment, which was maintained at the completion of all 6 cycles. Her nephrostomy tubes and ureteral stents were removed following completion of chemotherapy. She experienced minimal treatment-related toxicity during therapy. However, she continues to have Grade 3a chronic kidney disease off therapy as sequela of her presenting renal injury.
Discussion
MALT lymphomas are biologically heterogenous tumors that display varying histologic and molecular features based upon the site of the primary tumor.2,12 In many cases, these low-grade lymphomas develop secondary to chronic antigen stimulation, such as infection with Helicobacter pylori in gastric cases or Chlamydia psittaci infection in ocular cases. MALT lymphomas arising from the gynecologic tract are rare, with a limited number of reports in the medical literature.5-10 Therefore, the natural history, etiology, and clinical associations of these tumors have not been well described.
The intra-operative appearance of this patient’s lymphoma was very unusual, with dense fibrous adhesions resembling those described in abdominal cocoon syndrome. Abdominal cocoon syndrome is rare and characterized by total or partial encapsulation of abdominal organs by dense fibrous adhesions.13,14 This syndrome most often involves the intestinal tract, presenting with signs and symptoms of obstruction. The etiology is poorly understood, but secondary forms have been described in the setting of intrabdominal inflammation, autoimmune disease, and following abdominal surgery. The patient’s initial imaging and atypical intraoperative appearance elicited a broad clinical differential which included rhabdomyosarcoma, other soft tissue sarcoma(s), various lymphomas, germ cell tumors, and unusual infectious processes, such as peritoneal tuberculosis. In this case, the MALT lymphoma diffusely infiltrated the pelvic structures causing marked thickening which lead to an abdominal cocoon-like appearance, though notably the bowel was not involved.
Given its biological heterogeneity, treatment for MALT lymphoma can vary significantly. Treatment ranges from active surveillance and/or antibiotics (particularly for Helicobacter pylori-positive gastric lymphomas) to surgery and/or multiagent chemotherapy. Given the patient’s young age, normal LDH and low stage disease, this patient was classified as low risk,15,16 with acknowledgment that risk classification systems were validated in adult populations. With only sporadic descriptions of MALT lymphoma in children and young adults, management has been predictably heterogeneous without consensus in approach.1,17,18 Given this patient’s age and childbearing potential, extensive pelvic involvement, obstructive uropathy, and abnormal uterine bleeding, immediate medical management was initiated without an aggressive surgical approach. Gynecologic MALT lymphoma has not, to our knowledge, been definitively associated with chronic infections, and this patient’s broad testing for sexually transmitted infections was negative; however, the possibility of preceding inflammation leading to the development of a clonal B cell proliferation cannot be excluded. Interestingly, molecular interrogation of the tumor showed a likely pathogenic CHEK2 c.470T>C [p.I157T] mutation with a variant allele frequency of 49%, suggestive of a germline mutation. CHEK2 encodes the CHK2 protein which is involved in mediation of the DNA damage response pathway. Mutations in CHEK2 have been associated with increased risk of cancer in multiple organs and may confer a moderately increased risk of non-Hodgkin lymphoma (NHL). However, Havranek, et al 19 showed the missense variant identified in our patient (c.470T>C) did not differ significantly between the NHL patients and controls in their study of 340 lymphoma patients, making the significance of this finding uncertain.
Adult MALT lymphoma patients treated with the MALT2008-01 regimen chosen for this patient have had very good outcomes with 4-year progression free survival of 88%–97% among patients with Stage I/II disease and few severe toxicities. 11 Although patients on this trial who demonstrated a complete response after 2 cycles were treated with 4 total cycles, we decided to give six total cycles due to her excellent tolerance of this regimen and younger age (to maximize the chance of a long-term remission). Extended surveillance for recurrence will be particularly important for this patient, given the indolent nature of her initial disease presentation in combination with the anticipated duration of her long-term follow-up.
This patient’s age and primary tumor site highlight a very unusual presentation of extranodal marginal zone lymphoma. The extensive stromal responses elicited by this lymphoma resulted in a cocoon-syndrome like intraoperative appearance that to our knowledge has not been described in association with low grade lymphomas. This case further raises unique considerations for her treatment and long-term follow up.
Footnotes
Acknowledgements
We would like to thank the patient and her family for allowing us to share this report in the literature. We would like to thank Drs. Adam Lamble and Kim Riehle for contributions helpful to writing this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.