
Abstract
Introduction:
Skeletal growth arrest lines (GAL) are transverse lines of metaphyseal radiodensity accompanying episodic severe physiological stress. They are poorly described in fetal remains.
Materials and Methods:
We searched our autopsy practice for instances of fetal GAL in post mortem radiology, and correlated them with long bone histology and placental pathology. We describe the appearance, distribution, and pathology of GAL in a cohort of fetal autopsies, and compare the placental pathology accompanying GAL to the placental pathology of asymmetrical growth restriction (AGR) in the same time period.
Results:
In 2108 consecutive fetal post mortems, we found 20 cases with GAL. About 16 were in singletons with AGR. In these 16, the distribution of placental pathologies was similar to a contemporaneous cohort of 113 cases with AGR. Of the remaining 4, two twins out of 9 sets of monochorionic twins with AGR demonstrated GAL. One case of GAL had symmetrical growth restriction with cytomegalovirus infection, and one case had no AGR and an old, unexplained retroplacental hemorrhage. On histology, GAL are characterized by a region of mineralized chondroid, which is variably incorporated into irregular trabecular bone.
Discussion:
GALs accompany a variety of placental pathologies and twin-twin transfusion, suggesting episodic disease progression.
Introduction
Park-Harris lines (Growth Arrest Lines (GAL) or Growth Resumption Lines) are a radiological finding of radio dense transverse metaphyseal lines that accompany episodic severe illness or nutritional deprivation, typically in children or neonates.1,2 The histology and physiology of bony growth arrest lines has been investigated by means of pediatric autopsy, animal modeling, and radiological-clinical correlations. In the setting of severe illness, the chondrocyte columns of the epiphyseal plate cease or slow elongating, and bone is deposited in a transverse pattern near the deep surface of the epiphysis. When growth resumes these transverse seams of bone are left behind as a radiodense transverse line of trabecular bone in the metaphysis. 3 In neonates, growth arrest lines have been related to a physiological stressful peripartum, 4 but there is little exploration of the occurrence of Park-Harris lines in fetal remains, and they are often not even referred to in large series of post mortem fetal radiographs.5,6
Fetal growth arrest often reflects uteroplacental insufficiency and is often informed at post mortem by placental examination. A wide variety of placental and umbilical cord pathologies are associated with growth restriction, including maternal and fetal vascular malperfusion, placental inflammatory conditions, and multiple gestations and their sequela. 7 The effects of asymmetrical growth restriction on human bone histology have been explored at the costochondral junction8,9 but there is little systematic exploration of the effects of placental disease on long bone histology.
In the course of our practice we and others 8 have encountered transverse metaphyseal lines suggestive of growth arrest at fetal or neonatal autopsy, usually in the context of severe fetal disease, and often accompanying growth restriction. However, it is not clear whether fetal growth arrest lines are characteristic of any particular pathology or groups of pathologies, nor is there literature on what these radiological lines correspond to at the tissue level. Accordingly we set out to characterize the histology of fetal growth arrest lines, to review the pathological context of fetal growth arrest lines in our population and to determine, if possible, whether the presence or absence of growth arrest lines could be used to identify specific underlying placental conditions.
Materials and Methods
We searched our autopsy database for 10 years for recorded instances of growth arrest lines in fetal or neonatal autopsies, using text word searches for “growth arrest line”, “transverse metaphyseal line”, “growth restriction”, and “growth retardation” or “growth arrest” in the diagnostic field section. In our practice, significant asymmetric growth restriction (AGR) was identified as long bone growth delay (as measured by metaphyseal length of the femur) of two weeks or more from the clinically estimated gestational age, or body a weight less than the expected body weight minus two standard deviations for gestational age, with a brain to liver weight ratio of greater than 4 in a non-macerated fetus in the context of other features of chronic fetal compromise (e.g., severe placental disease, lipidization of the fetal adrenal cortex, and severe osteopenia) or a brain to liver weight ratio of greater than 6 in either a macerated or non-macerated fetus.
In the study period, whole body fetal radiographs (AP and lateral) were acquired using a Hewlett Packard Model 83855 cabinet faxitron as a routine part of all post mortem fetal examination. These radiographs were also retrieved and reviewed. For each case, the gestational age, autopsy diagnoses, placental and umbilical cord pathology, timing of death (neonatal, in utero fetal death, termination of pregnancy) fetal sex, and the presence or absence of growth arrest lines were recorded. Instances were included if the fetal examination involved a complete post mortem examination, including microarray cytogenetic studies, examination of the viscera, and of the placenta. For each case of asymmetrical growth restriction, severity of growth restriction was calculated by determining the difference between the clinically estimated gestational age and the 50th centile gestational age for femur length as determined from the radiographic normal ranges. Histological sampling of costochondral junctions was available as a part of routine autopsy protocol in all cases. Where consent permitted and radiological review was completed prior to histological sampling, affected long bones demonstrating growth arrest lines were harvested and histological sections made following fixation in formalin and decalcification in 8% formic acid, and this histology compared to the radiological images of growth arrest on the same case. Over the same time period we also sampled femurs from 10 fetal autopsies (age range 20-37 weeks gestation) without growth restriction or skeletal anomalies, and from 20 fetuses with AGR but without GAL.
Placental pathology reports for each case were reviewed and placental and umbilical cord diagnoses were recorded. Placental pathologies of interest were defined prior to review, and collected directly from reports. Tabulated categories were maternal vascular malperfusion, fetal vascular mal-perfusion, chronic lymphohistiocytic villitis (Villitis of Unknown Etiology) chronic histiocytic intervillusitis, massive perivillous fibrinoid deposition, intervillous thromb-ohematomas, retroplacental hematoma, isolated villous infarction, delayed villous maturation, villous dysmaturity, placenta accrete spectrum disorder, meconium exposure effects, acute chorioamnionitis, villous edema, and circulating nucleated fetal red blood cells. Umbilical cord morphology was recorded as over coiling, single umbilical artery, marginal insertion, membranous insertion, normal, or other. Fetal vascular malperfusion was included if it was high grade, 10 and the diagnosis of maternal vascular malperfusion was made there was chronic maternal vascular malperfusion as manifested by at least two of decidual arteriopathy, villous infarction, accelerated villous maturation or excess syncytiotrophoblast knots. Isolated villous infarction was included as maternal vascular malperfusion if it was pre-term, or if term there were multiple infarcts or the infarct was large (>2 cm diameter). For purposes of preliminary examination, we used isolated villous infarction as a separate category, on the suggestion that infarction might produce a step wise progression of fetal compromise.
All research processes were reviewed and approved by institutional ethics review board.
Results
Growth Restriction
We searched the reports of 2108 unrestricted fetal post mortems in the included time period. Of these 189 were recorded as demonstrating growth restriction and/or growth arrest lines in the diagnosis. Of the cases without growth arrest lines, we excluded those with aneuploidy, significant congenital malformations or disruptions, skeletal dysplasias, chronic infections, lacking cytogenetics or placental pathology, or with symmetrical growth restriction, we were left with 122 cases of asymmetrical growth restriction, 9 of which were from 9 sets of twin pregnancies, and 113 from singleton fetuses. Of cases of singleton AGR, 64 were in utero fetal deaths, 5 were neonatal or intrapartum deaths, and 44 were terminations of pregnancy for severe growth restriction.
We found 20 cases with growth arrest lines: 16 occurred in singleton gestations with asymmetrical growth restriction: 6 of these were terminations of pregnancy for growth restriction and 10 were in utero fetal deaths. Two additional cases of growth arrest lines in asymmetric growth restriction were each a member of a separate set of monochorioninc twins. Both of these were, on the basis of post mortem examination, likely the donor twin in a twin-twin transfusion. Two further cases did not demonstrate asymmetrical growth restriction: one was in the setting of an old retroplacental hemorrhage with porencephaly, and one was in a case of congenital cytomegalovirus infection with severe symmetrical growth restriction and fetal hydrops. The mean gestational ages of cases with and without GAL were similar (P > .05)
Radiologically, the growth arrest lines in all but two cases appeared as a radio-dense, irregular subchondral zone, followed by a relatively radiolucent zone, with a subjacent transverse linear area of increased radiodensity (Figure 1). Transverse lines often involved multiple bones in the same fetus. GAL were most frequent in the femur (15/16) followed by humerus and iliac crest (12/16 each) and tibia (10/16). In 7 all the long bones of the limbs were involved, in three the scapula, and in three the ribs, When present in the radius or ulna, they were always present in the femur, humerus and tibia. In the sole case that they were absent in the femur, they were present in the iliac bones only. 15 of the 16 cases were bilaterally symmetrically distributed: in a single case there was a unilateral femoral line. Usually both proximal and distal metaphyses were involved, but in two cases, the proximal femur only, or the proximal femur and proximal humerus, were involved. In 4 cases multiple GAL were present in a single bone (Figure 1).
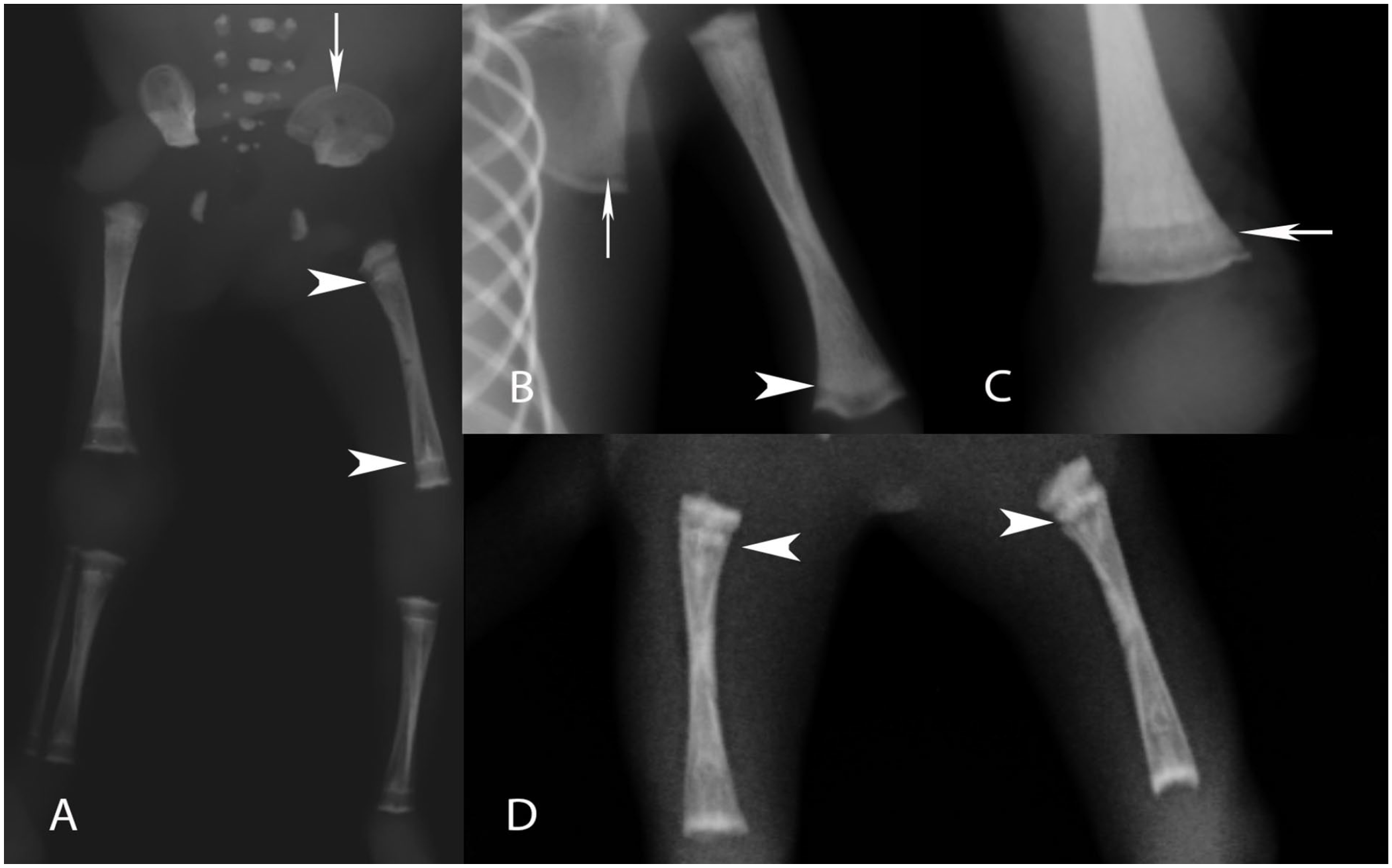
Plain film radiographs of fetal remains demonstrating growth arrest lines. (A) Arrowheads with symmetrically placed long bone transverse lines in the femurs and tibias, with fainter lines in the iliac crest (arrow), 27 weeks gestation. (B) Transverse line of relative radio density underlying area of radiolucency in the humerus (arrowhead) with similar pattern in the scapula (arrow), 26 weeks. (C) Arrow pointing to a faint transverse line in the middle of a radiolucent area of distal femoral metaphysis (28 weeks gestation). (D) Densely sclerotic transverse lines in proximal femoral metaphyses only, 21 weeks gestation.
Atypical radiological patterns
In two cases , the distal long bones were more radio-dense along a thick zone extending from an irregular epiphysis into the metaphysis with a normal appearing diaphysis. In both these cases there was fetal hydrops: one of these had congenital Cytomegalovirus infection, with symmetrical growth restriction. The other case demonstrated asymmetrical growth restriction with marked muscle wasting and thick subchondral zones of radiodensity, although more typical linear densities were present in the iliac bones (Figure 2).
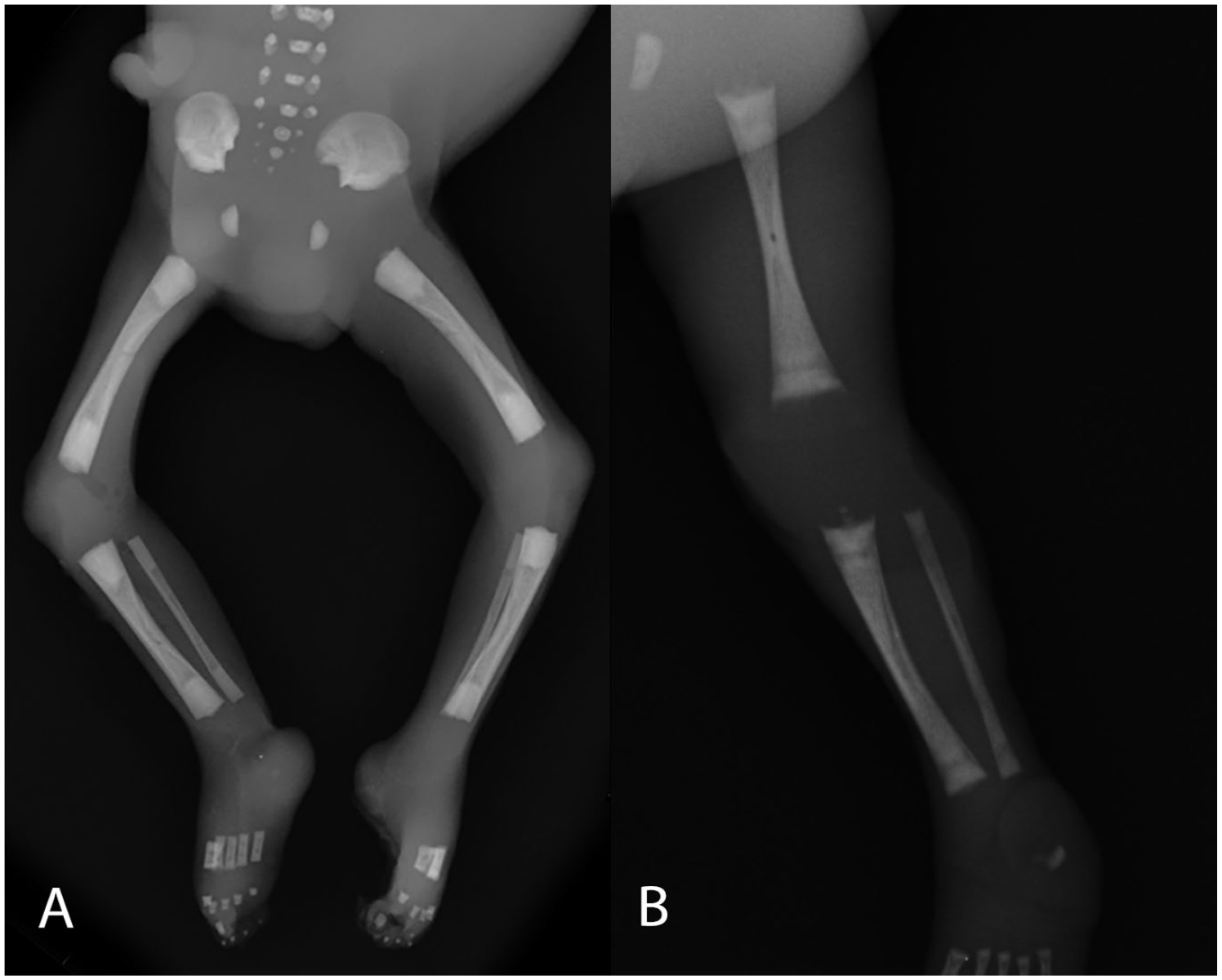
Atypical features (A) Lower extremities, of an approximately 24 week gestation IUFD with hydrops, showing thick radio dense long bone metaphyses. (B) Left lower limb of a case with similar radiology in congenital cytomegalovirus, also demonstrating irregular epiphyseal radio-density (24 weeks gestation).
Histology of Costochondral Junction and Growth Arrest Lines
The histology of costochondral junctions from cases of growth restriction with growth arrest lines were examined. All the costochondral junctions showed marked changes of growth arrest (Figure 3). In midgestation specimens, the rib shafts demonstrated scant ossification and abundant, unremodeled, and partially mineralized chondroid with few organized bony trabeculae similar to the bizarre pattern of growth arrest noted by da Cunha Castro and Popek. 9 In later gestation fetuses, the bony trabeculae were generally thin and irregular and contained an excess of chondroid. Patterns of growth arrest ranged from banding and bridging of chondroid below the growth columns to large regions of unossified and partially mineralized chondroid in the center of the rib shaft. In general, the pattern of abnormal ossification in the ribs matched those seen in the long bones of the each case (see below).
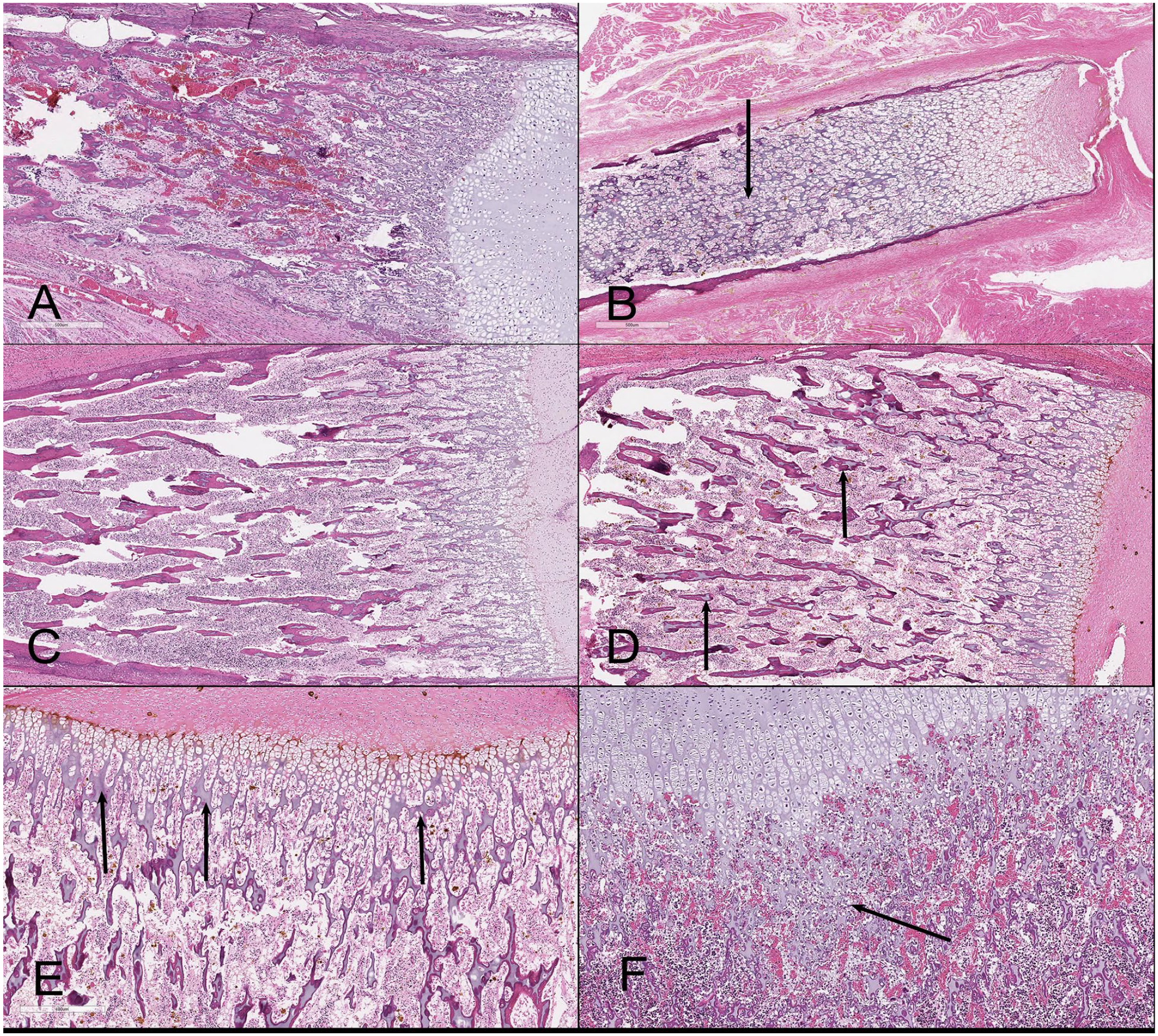
Histology of costochondral junctions. (A) 22 weeks normal fetal costrochondral junction demonstrating from right to left the cartilage, growth plate, zone of ossification, and then bony trabeculae. (B) 22 week fetus with asymmetrical growth restriction and GAL in long bones: the rib shaft displays little orderly ossification and abundant chondroid, with very small areas of mineralized bony trabeculae (arrow). (C) Normal rib at 32 weeks, demonstrating roughly parallel arrays of thick bony trabeculae, each containing only small amounts of chondroid. (D) Rib at 32 weeks gestation from case with GAL, demonstrating thin irregular trabeculae each of which contains unremodeled chondroid. (E) Same case, higher power, demonstrating (arrow) prominent banding of cartilage below the chondrocyte columns (i.e., banding). (F) Different case with GAL, demonstrating masses of unremodeled and poorly vascularized cartilage matrix below the deep margin of the epiphyseal plate (arrow).
Histology of growth arrest lines was available in 5 cases of asymmetrical growth restriction and 10 cases of growth restriction without GAL (Figure 4). In all cases of growth restriction the epiphyseal plates were irregular, with highly variable cell column length in the hypertrophic zone of the epiphyseal plate. All demonstrated excess chondroid matrix between the deeper aspects of the hypertrophic cell columns, and between chondrocytes in the columns of the hypertrophic zone. There was also deposition of matrix between the deep aspects of the cell columns and the bony trabeculae, and an impingement of the marrow space on the deep aspect of the zone of provisional calcification. In cases with growth arrest lines, the radio-dense subchondral area corresponded to the zone of provisional calcification and early osteoid deposition (Figure 4). Deep to this area was a metaphyseal area of thin, poorly branching, or irregular trabeculae (Figure 5) sometimes largely composed of chondroid with little osteoid deposition or containing islands of partially mineralized cartilage. Deeper to this is a zone of thickened, irregular, transversely branching bony trabeculae containing abundant mineralized chondroid, or anastomosing trabeculae of mineralized chondroid, which appears to correspond to the growth arrest line (Figure 6). The accompanying costochondral junction pathology was reviewed for these cases as well. All cases with growth arrest lines displayed excess unremodeled chondroid within the rib shaft.
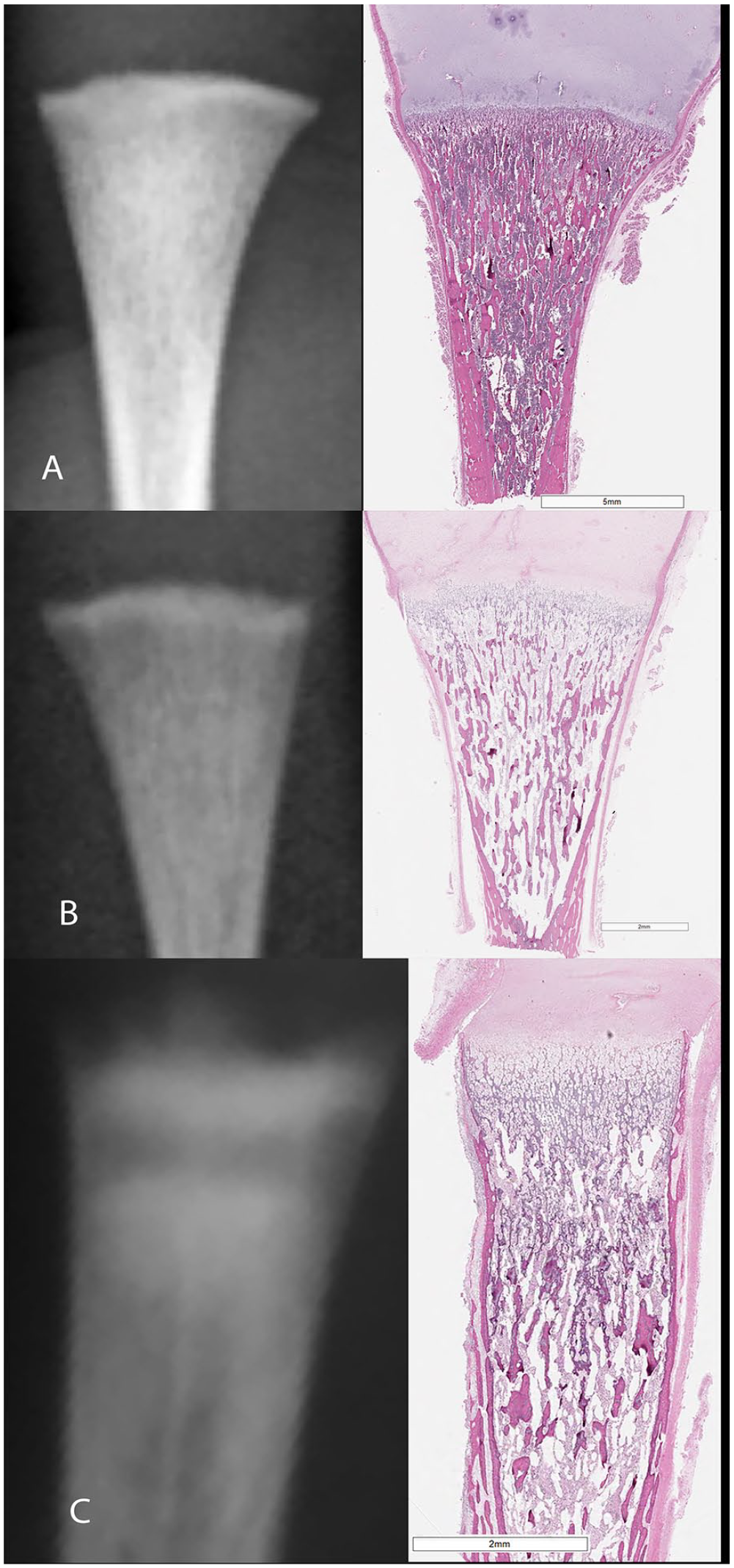
Fetal radiograph with matching whole mounted distal femur, all 24 weeks gestation. (A) Normal Distal femoral metaphysis (top) at 24 weeks gestation demonstrating even radio density and smooth epiphyseal-metaphyseal junction. (B) Asymmetric growth restriction without growth arrest lines demonstrating an even pattern of osteopenia relative to A. (C) Growth arrest line demonstrating thick subepiphyseal area of provisional calcification flowed by radiolucent zone, with more distal thick transverse line of irregular trabecular thickness.
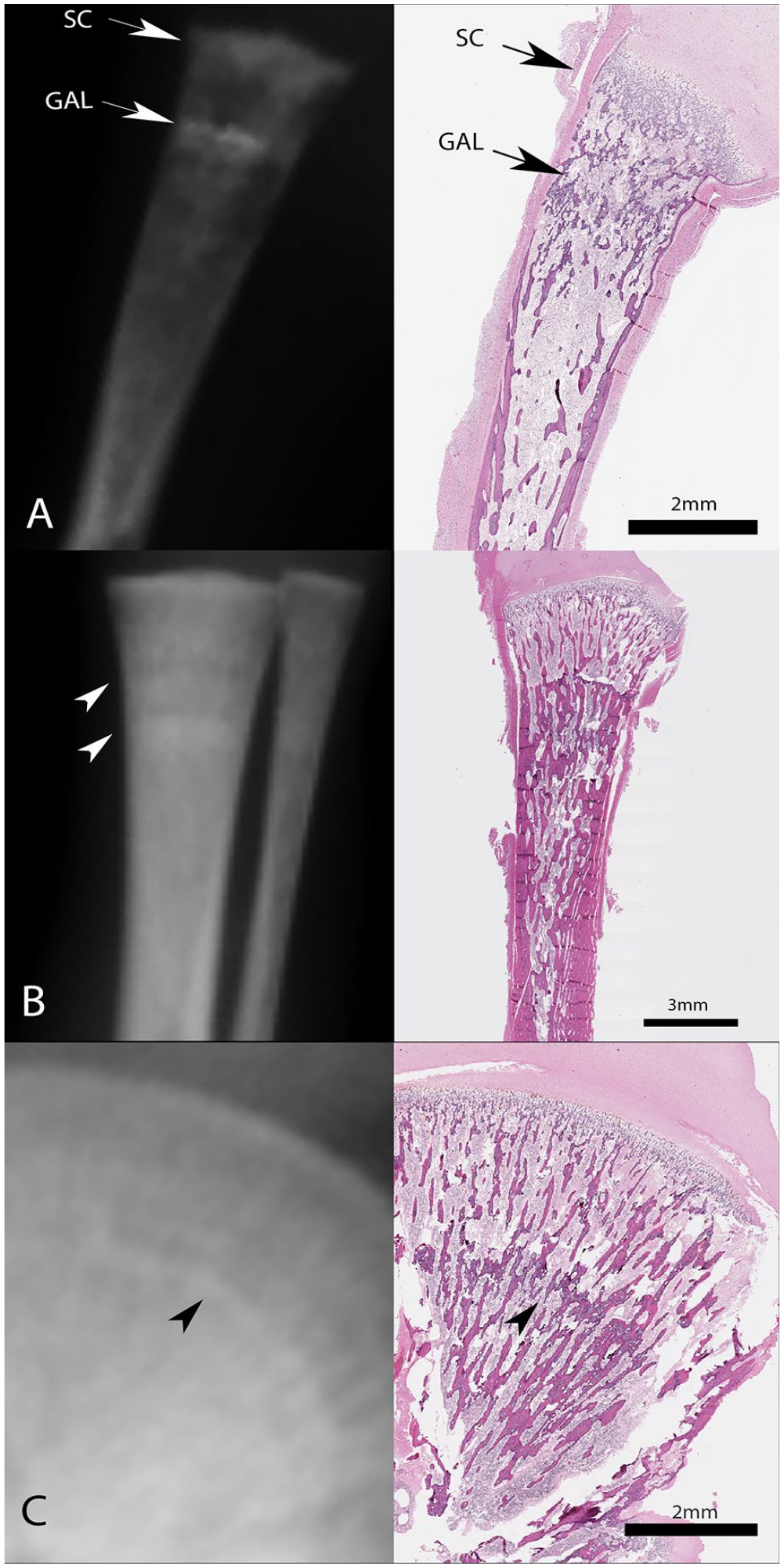
Radiographs of growth arrest lines with matching whole mounts. (A) Right proximal humerus, 24 weeks gestation. The thick subchondral radio density (SC) correlates with an irregular thick zone of provisional calcification, while the traverse metaphyseal line (GAL) represents an irregular band of trabeculae. (B) Arrowheads pointing to multiple apparent lines in distal tibia (27 weeks gestation) with 1 definitely corresponding to a distinct band of thickened transverse trabeculae. (C) Iliac crest of same case as in B, demonstrating similar histology with a line of thick irregular trabeculae.
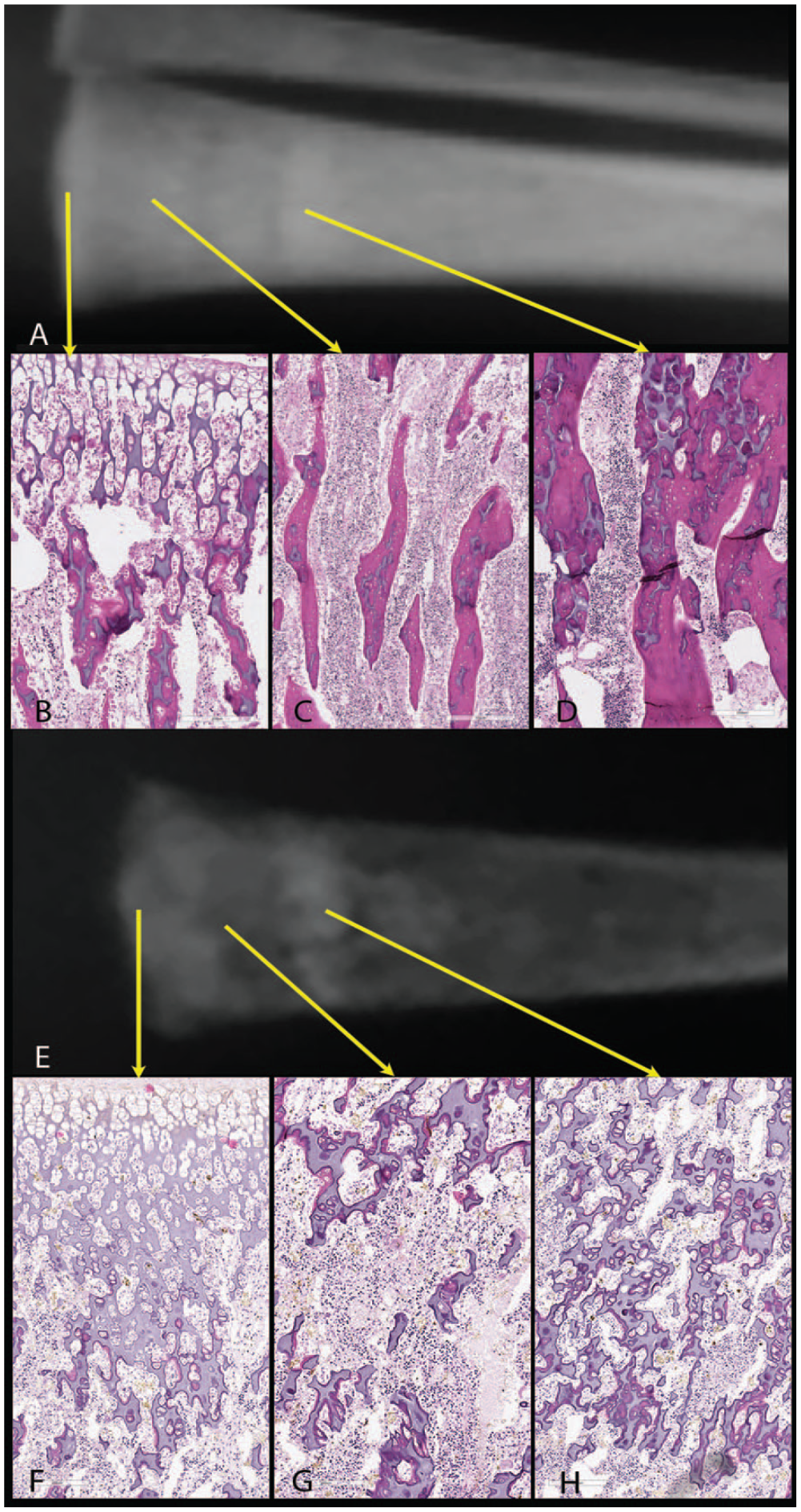
Higher power of histology, same case as in 4B. (A) Radiograph of distal tibia. (B) The epiphysis demonstrates short, irregular columns of hypertrophic cells with chondroid deposition interrupting the regular parallel cell columns. (C) The subjacent metaphysis contains gracile trabeculae oriented in parallel with the axis of the bone. (D) The growth arrest line contains thickened trabeculae joining each other laterally and containing large amounts of unmineralized chondroid. (E) Radiograph of whole mounted distal tibia, 22 weeks gestation. (F) The epiphyseal columns are again irregular and short with chondroid deposits often forming large pools. (G) The immediately subjacent metaphysis shows widely spaced, irregular deposits of chondroid some with small amounts of osteoid deposition. (H) The growth arrest line demonstrates irregular, cross linked trabeculae containing marked excess chondroid with scant remodeling and some deposition of osteoid.
Placental and Umbilical Cord Pathologies in Asymmetrical Growth Restriction
Of the 113 cases of singleton asymmetrical growth restriction, 64 demonstrated maternal vascular malperfusion and 53 demonstrated fetal vascular malperfusion. Fifty seven cases demonstrated significant umbilical cord pathology, which was usually over-coiling (n = 46) and/or membranous insertion or insertion less than one cm from the margin of the placental disc (n = 17; Figure 7). Six cases of growth restriction did not show placental histopathologies but had structural abnormalities confined to the umbilical cord. Of these, three demonstrated marked placental hypoplasia, one placenta was received incomplete and fragmented, and two others demonstrated features of prolonged intrauterine retention after death, with a high risk umbilical cord coiling pattern. It is entirely possible, therefore, that in these three significant placental pathology was present but could not be confirmed due to the limitations of the placental examination. One case that did not demonstrate abnormal placental or umbilical cord pathology but was received fragmented and likely incomplete demonstrated growth arrest lines.
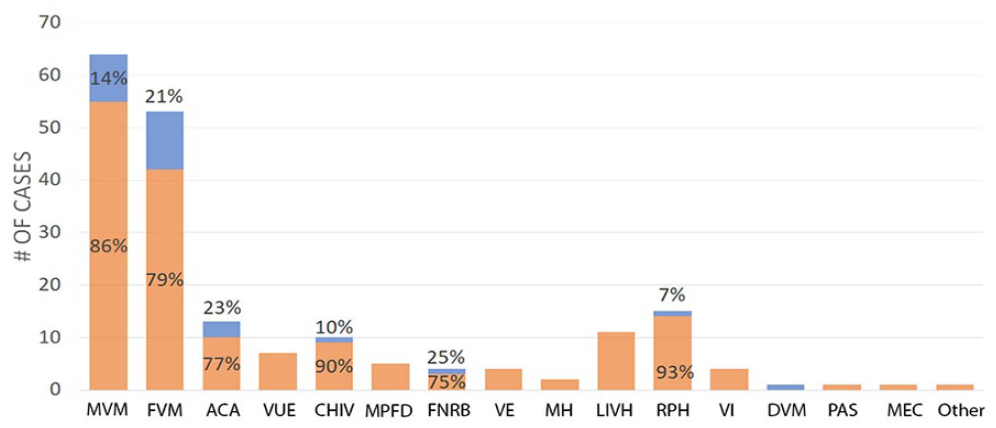
Frequency of placental diagnoses with proportion affected by growth arrest lines (in blue). Diagnostic categories are not mutually exclusive and individual cases may be counted in multiple disease states. There is no obvious pattern of disease association.
Because the large majority of cases with growth arrest lines occurred in the context of asymmetrical growth restriction attributable to placental pathology in singleton pregnancies, we compared the distribution of placental and umbilical cord pathologies in cases with growth arrest lines to the distribution of such pathologies in our autopsy cohort of isolated asymmetrical growth restriction in singletons. The mean gestational age (t = 0.2, P = 0.994) and placental (Figure 7) and umbilical cord pathologies was similar in fetuses with and without growth arrest lines (Figure 8). Given that most placental pathology was either maternal or fetal vascular malperfusion, or a combination of both, cases with other pathologies were excluded from the analysis and the result was same: maternal vascular malperfusion, fetal vascular malperfusion, or a combination of both is not over represented in our autopsy series of cases with growth arrest lines, compared to cases of asymmetrical growth restriction in general (Figure 9). Finally, the degree of growth restriction as measured by the difference between expected gestational age estimated by post mortem femur length as measured on conventional radiography and the gestational age estimated clinically did not differ between cases with and without growth arrest lines (t = 0.5, P > 0.1). In general it can be said that growth arrest lines are not specific to a particular underlying placental pathology.
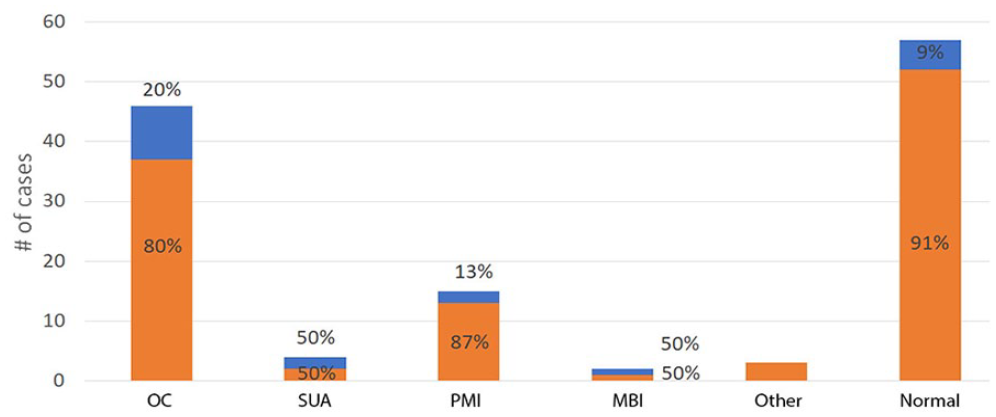
Distribution of growth arrest lines according to umbilical cord pathology. Blue represents cases with GAL. Diagnostic categories are not mutually exclusive and individual cases may be counted multiple times. Although some pathologies (Single umbilical artery, Membranous insertion) have a high rate of growth arrest lines, the number of cases in each is low.
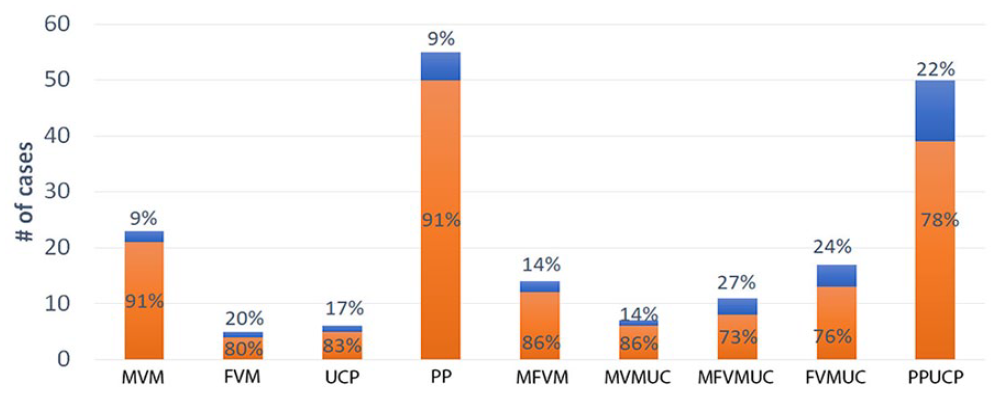
Distribution of growth arrest lines in common placental pathologies and umbilical cord pathologies. Blue represents cases with GAL.
Discussion
Enchondral ossification is characterized by the proliferation of resting cartilage into columns of chondrocytes, which become hypertrophic, produce matrix, and undergo apoptosis. The chondroid matrix is mineralized, vascularized, and osteoid is deposited by osteoblasts to and the columnar chondroid scaffold is resorbed. Transverse metaphyseal radio-dense lines (Growth Arrest Lines) can be formed during periods of severe physiological stress: in the long bones of children and in animal models these lines correspond to a layer of osteoid deposition across the metaphyseal aspect of the epiphyseal plate. These lines reflect poor or arrested elongation of the chondrocyte columns, with abnormal patterns of matrix deposition, poor vascularization, and subsequent mineralization and osteoid deposition in the absence of linear growth. Subsequent resumption of growth leads to the GAL being left behind in the metaphysis as bone elongation resumes at the epiphyseal plate.2,3 Our results show a mixed histological picture: in 3 of 5 cases, the histology suggests that a growth arrest line consists of abnormally oriented thickened seams of bony trabeculae surrounding abnormal amounts of residual chondroid. This is congruent with the idea that poor matrix remodeling leads to abnormal transverse patterns of osteoid deposition. By contrast, in 2 of the fetal cases (at 19 and 23 weeks GA), the growth arrest lines consist of abundant unremodeled and partially mineralized chondroid with only scant osteoid deposition. Chondroid remodeling is thought to be dependent on neovascularization and osteoblast invasion, and the variable but excess chondroid suggest that these energy dependent processes are more impaired than chondroid deposition in the setting of fetal growth restriction. Although the two cases with histology with this pattern were at younger gestational ages than the other three, the number of cases in which histology is available overall are too low as to comment confidently on the effect of gestational age on GAL histology.
The effects of fetal growth restriction on the histology of fetal bone growth is best described at the fetal costochondral junction. In fetal growth restriction, accumulations of mineralized chondroid matrix accumulate adjacent to the bone marrow cavity during periods of growth restriction, although well-defined growth arrest lines are not usually observed in the rib. The histology of fetal growth arrest lines in long bones suggests that growth arrest in the long bones is similar to that in the ribs and that fetal growth arrest lines are also the result of an abnormal deposition pattern of matrix accompanied by impaired remodeling, with osteoid deposited to a variable degree on the unremodeled mineralized chondroid. The histology likely reflects the fact that vascularization and resorption of chondroid is an energy dependent process, and will be impaired in uteroplacental insufficiency. Possibly the salience of chondroid matrix in fetal growth arrest lines, as opposed to pediatric GALs, reflects the limited time for remodeling available between formation of the GAL and fetal death in these cases. Alternatively, it may be that the degree of nutritional deprivation necessary to form a growth arrest line in postnatal life or in animal models might be more quickly fatal to a growing fetus, and so survival and subsequent growth resumption is rare.
If the usual understanding of growth arrest lines is correct, it might be possible to provide an estimate of the minimal gestational age at which growth was arrested, provided one has growth arrest lines present at both ends of a long bone: the distance between the growth arrest lines should correspond to a minimal estimate of the length expected at the gestational age where growth was first arrested. A similar approach was used to demonstrate that incidental growth arrest lines in the proximal femur of neonates likely corresponded to subclinical perinatal stress. 4 The estimate of the timing of intrauterine compromise may be imprecise, given that growth restriction may already have commenced before the GAL is formed. In one case such a calculation has been evaluated by serial ultrasound imaging. In that case, there was no growth restriction, but there were growth arrest lines and the brain demonstrated porencephaly: the ultrasound onset of brain injury seemed to precede by roughly a week the formation of the GAL as calculated by measurement of femur length between the growth arrest lines. 11 The timing of a GAL in such a case may reflect a short lag between injury and growth arrest, or alternatively might simply reflect the biological variability from case to case in growth trajectory with gestational age. In either event, the notion that GAL can approximately mark a significant intrauterine injury remains plausible.
In this series, fetal growth arrest lines were present in a minority of the fetal remains studied, and predominantly in remains demonstrating asymmetrical growth restriction. Given that they may take at least a week to form after severe injury, 11 the presence of GAL at post mortem imply a chronic fetal disease. This is congruent with the range of severe placental pathologies documented. Although the large majority of GAL accompany severe placental disease, here and elsewhere they may occasionally accompany other diseases. It should be noted that growth arrest lines are much more difficult to appreciate on histology than radiology, and all of our diagnoses of GAL were first identified on radiological examination prior to histology. Radiological examination of the fetus is therefore useful and complementary to fetal autopsy and examination of the placenta at post mortem.
In this study we did not demonstrate a consistent correlation between the various placental causes of growth restriction and growth arrest lines. This is perhaps surprising, as some placental diseases are diffuse and seem progressive (e.g., chronic histiocytic intervillusitis and twin-twin transfusion) while others seem intuitively more episodic in their progression (e.g., fetal vascular malperfusion) and fetal cases with either disease can demonstrate growth arrest lines. The presence of growth arrest lines would appear to suggest severe physiological stress followed by partial recovery, suggesting an intermittent tempo to the progression of disease. Indeed, the presence of transverse metaphyseal lines was not always accompanied by clinical growth restriction: in one case there was no growth retardation, but there was old retroplacental hemorrhage and brain injury with pelvic growth arrest lines. In this cohort, GALs were present across the spectrum of placental disease, suggesting that any process can vary temporally in its effects on fetal growth, and that the fetus and placenta can have significant physiological reserve in the presence of disease.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.