
Abstract
Introduction:
Gestational diabetes mellitus (GDM) is a common metabolic disorder linked to adverse pregnancy outcomes. Recent research indicates that HbA1c is reliable in detecting maternal glycemia during the first trimester but may underestimate glucose intolerance in the late second to third trimesters. Therefore, it is reasonable to hypothesize that mothers with GDM, despite apparently normal HbA1c levels in the third trimester, may give birth to infants displaying characteristic features often seen in infants of diabetic mothers with suboptimal glycemic control. This study aimed to describe a case series of autopsy cases involving stillborn or deceased neonates delivered in the third trimester to mothers diagnosed with GDM and having normal HbA1c levels at or around the time of delivery. The primary focus was on identifying and documenting the characteristic features commonly associated with “infants of diabetic mothers” with suboptimal glycemic control in this series of cases.
Materials and Methods:
We conducted a retrospective review of autopsy reports from our institution spanning 7.5 years. The study included cases that met the following criteria: (1) stillborn or infants who died in the early neonatal period, delivered in the third trimester; (2) mothers diagnosed with GDM; (3) normal maternal HbA1c levels of ≤6.1% at or around the time of delivery; (4) birthweight or femoral length exceeding the 90th percentile for gestational age; and (5) absence of genetic aberrations. We also examined these cases for other characteristic features associated with “infants of diabetic mothers.”
Results:
Ten autopsy cases met our inclusion criteria, including 9 stillbirths and 1 neonatal death. Gestational age at delivery ranged from 32 to 39 weeks (mean: 35.7 weeks). Femoral length exceeded the 90th percentile in all cases, and 6 cases had birthweights above the 90th percentile. Puffy facies were observed in 6 cases. Among the 9 cases with complete autopsies including internal examination, 6 exhibited excess adipose tissue, 4 had cardiomegaly, and 3 showed pancreatic islet hyperplasia. Hypoxic-ischemic encephalopathy was detected in 7 cases. No structural abnormalities were noted.
Discussion:
Our findings demonstrated that fetuses and neonates born to mothers with apparently normal HbA1c levels in the third trimester could still display characteristic features commonly observed in infants of diabetic mothers with poor glycemic control, also known as “infants of diabetic mothers.” This study underscores the potential of third-trimester maternal HbA1c measurements to underestimate maternal glycemia and its consequential impact on fetal development, as well as the subsequent manifestation of features of “infants of diabetic mothers.”
Keywords
Introduction
Gestational diabetes mellitus (GDM) is a metabolic disorder that commonly affects pregnant women and is characterized by any degree of glucose intolerance that is either first recognized or begins during pregnancy. 1 It is estimated to impact approximately 7% to 10% of all pregnancies worldwide.2 -5
Poor control of GDM during pregnancy can result in high maternal blood glucose levels, which can lead to fetal hyperglycemia and hyperinsulinemia. 6 Infants born to diabetic mothers with suboptimal glucose control are often larger than expected for their gestational age and may have puffy facies, excess adipose tissue, cardiomegaly, and pancreatic islet hyperplasia.7-13 These infants are commonly referred to as “infants of diabetic mothers.”
GDM is associated with adverse pregnancy outcomes. 14 As a result, the Society of Obstetricians and Gynaecologists of Canada (SOGC) and the American College of Obstetricians and Gynecologists (ACOG) recommend the evaluation of maternal blood glucose levels as part of the investigation protocols for stillbirth cases. The recommended test for this purpose is maternal hemoglobin A1c (HbA1c).15,16
However, a recent prospective cohort study reveals that while HbA1c is a reliable marker for maternal glycemia in the first trimester, it may underestimate maternal glucose intolerance during the late second-to-third trimesters. 17 Therefore, we postulate that in cases of third-trimester stillbirths and early neonatal deaths associated with GDM, a normal HbA1c measurement during the third trimester might underestimate the mother’s glycemic levels. Consequently, it may not accurately reflect the true impact of maternal glycemia on fetal development. This, in turn, could potentially result in infants demonstrating characteristics commonly observed in “infants of diabetic mothers,” despite their mothers having seemingly normal “non-diabetic” HbA1c measurements.
This study aimed to describe a case series of autopsy cases involving stillborn or deceased neonates delivered in the third trimester to mothers diagnosed with GDM and having normal HbA1c levels at or around the time of delivery. The primary focus was on identifying and documenting the characteristic features commonly associated with “infants of diabetic mothers” with suboptimal glycemic control in this series of cases.
Materials and Methods
This retrospective case series was approved by the University of Calgary Conjoint Health Research Ethics Board (REB14-2391).
Fetal and Neonatal Autopsies
This case series was based on autopsies conducted at Alberta Children’s Hospital/Alberta Precision Laboratories from January 1, 2015, to April 30, 2022. In Alberta, Canada, the indications for fetal and neonatal autopsies are broad and are determined by the requesting physician. Autopsies were conducted only with the written, informed consent of the parents. A complete autopsy examination involves photography, whole-body X-ray, external and internal examination, cytogenetics analysis, microscopic examination of body tissue, placental examination, and potential ancillary studies (e.g., bacterial cultures and viral molecular studies). Placental examination protocol was described in our previously published paper. 18
All autopsies were performed by pathologists specializing in perinatal and pediatric pathology, while pathologists specializing in neuropathology examined the brain and spinal cord. Perinatal/pediatric radiologists interpreted the X-rays. The results of each autopsy were combined into a single, final autopsy report.
Fetal and Neonatal Autopsy Reports Extraction
Reports of autopsies conducted at Alberta Children’s Hospital/Alberta Precision Laboratories from January 1, 2015, to April 30, 2022, were extracted from the Cerner (North Kansas City, MO, USA) Millennium Laboratory Information System.
Inclusion Criteria
To identify cases for this case series, we manually reviewed the autopsy reports and applied the following inclusion criteria:
The case involved either a stillborn delivered in the third trimester (i.e., late-to-term stillbirth) or an infant who was born in the third trimester and died within 7 days of life (i.e., early neonatal death).
The mother was diagnosed with GDM in accordance with Canadian Diabetes Association’s (CDA) 2018 practice guidelines. 19 The diagnostic process involved an initial 50 g glucose challenge test (GCT), followed by a 75 g oral glucose tolerance test (OGTT) if the GCT results were abnormal. Alternatively, the diagnostic process could involve only a 75 g OGTT.
The mother had a normal or recommended target HbA1c level, defined as ≤6.1% according to the CDA and SOCG guidelines,19,20 at or around the time of delivery.
The fetus’s or infant’s birthweight or femoral length exceeded the 90th percentile according to previously published parameter standards.21,22
Cytogenetic testing (rapid aneuploidy detection or chromosomal microarray) yielded normal results.
Review of Autopsy Cases
We first identified autopsy cases that met the inclusion criteria, and for those cases, we reviewed the autopsy reports, X-rays, hematoxylin-and-eosin-stained slides, and immunohistochemistry slides.
We then extracted the following information from the autopsy and X-ray reports: type of autopsy (complete or partial), whether the demise was stillborn or early neonatal death, gestational age at delivery, gender of the fetus or neonate, maternal age, gravida, parity, maternal body mass index (BMI) at 12 weeks of gestational age (GA), GA when GDM was diagnosed, HbA1c level at or around delivery, GDM treatment, degree of fetal maceration, birthweight, femur length, and presence or absence of the following features including puffy facies, excess adipose tissue, cardiomegaly, congenital malformations, and hypoxic-ischemic encephalopathy. We also reviewed histologic and immunohistochemical slides of pancreatic tissue to determine the presence or absence of pancreatic islet hyperplasia. Furthermore, we noted the placental weight and any placental anomalies. Finally, we recorded the cause of death for each case.
Percentiles of birthweights, femoral lengths, placental weights, and fetal to placental weight ratios were assigned using previously published ranges.21-24
Additionally, we conducted insulin immunohistochemistry on formalin-fixed, paraffin-embedded tissue sections of the pancreas. Briefly, 4-μm sections of formalin-fixed, paraffin-embedded sections were deparaffinized, rehydrated, and pre-treated with a target retrieval solution, followed by incubation with insulin polyclonal FLEX RTU antibody (Agilent, Santa Clara, CA, USA). The signal was developed using a high pH, DAB+ Substrate Chromogen visualization system (Agilent, Santa Clara, CA, USA) on a Dako Omnis automated stainer (Agilent, Santa Clara, CA, USA).
Results
A total of 10 autopsy cases met the inclusion criteria, consisting of 9 stillbirths and 1 early neonatal death, all from different mothers. Among these cases, 9 had a complete autopsy performed, while 1 had a limited autopsy restricted to external examination, X-ray, and cytogenetics analysis. The characteristics of all 10 cases are detailed in Tables 1 to 3.
Clinical Characteristics of Autopsy Cases.
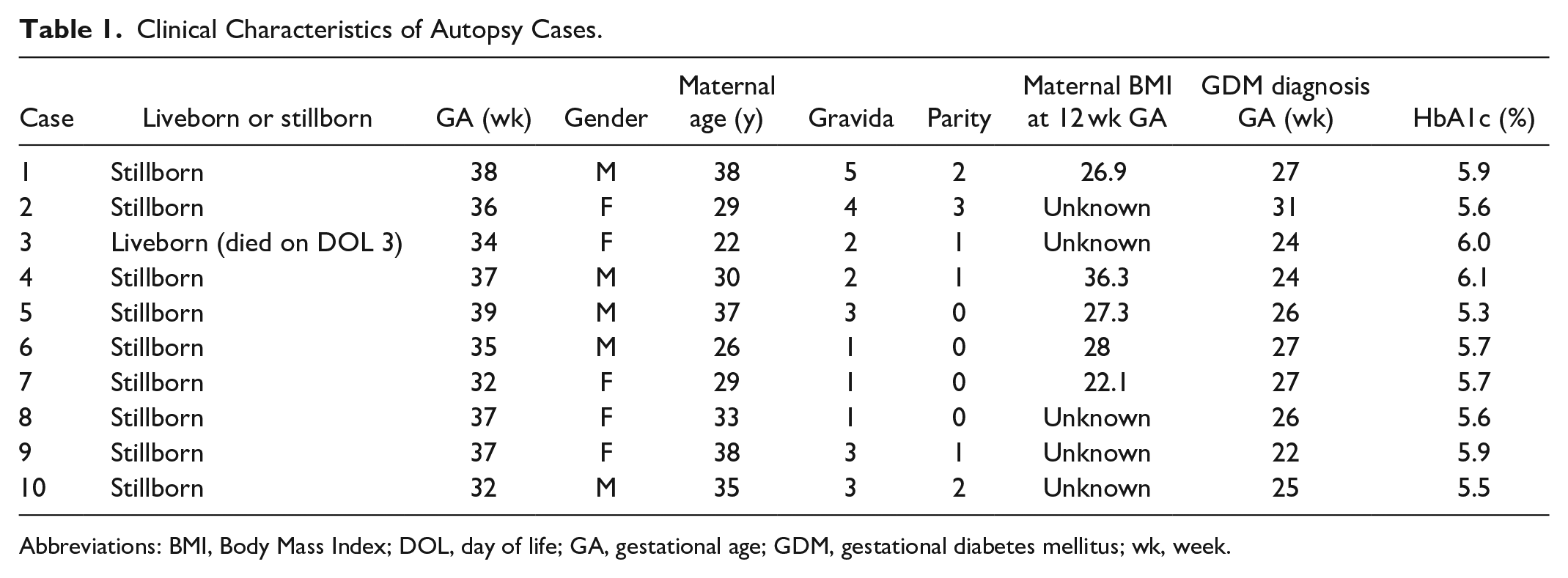
Abbreviations: BMI, Body Mass Index; DOL, day of life; GA, gestational age; GDM, gestational diabetes mellitus; wk, week.
Postmortem Findings of the Case Series.
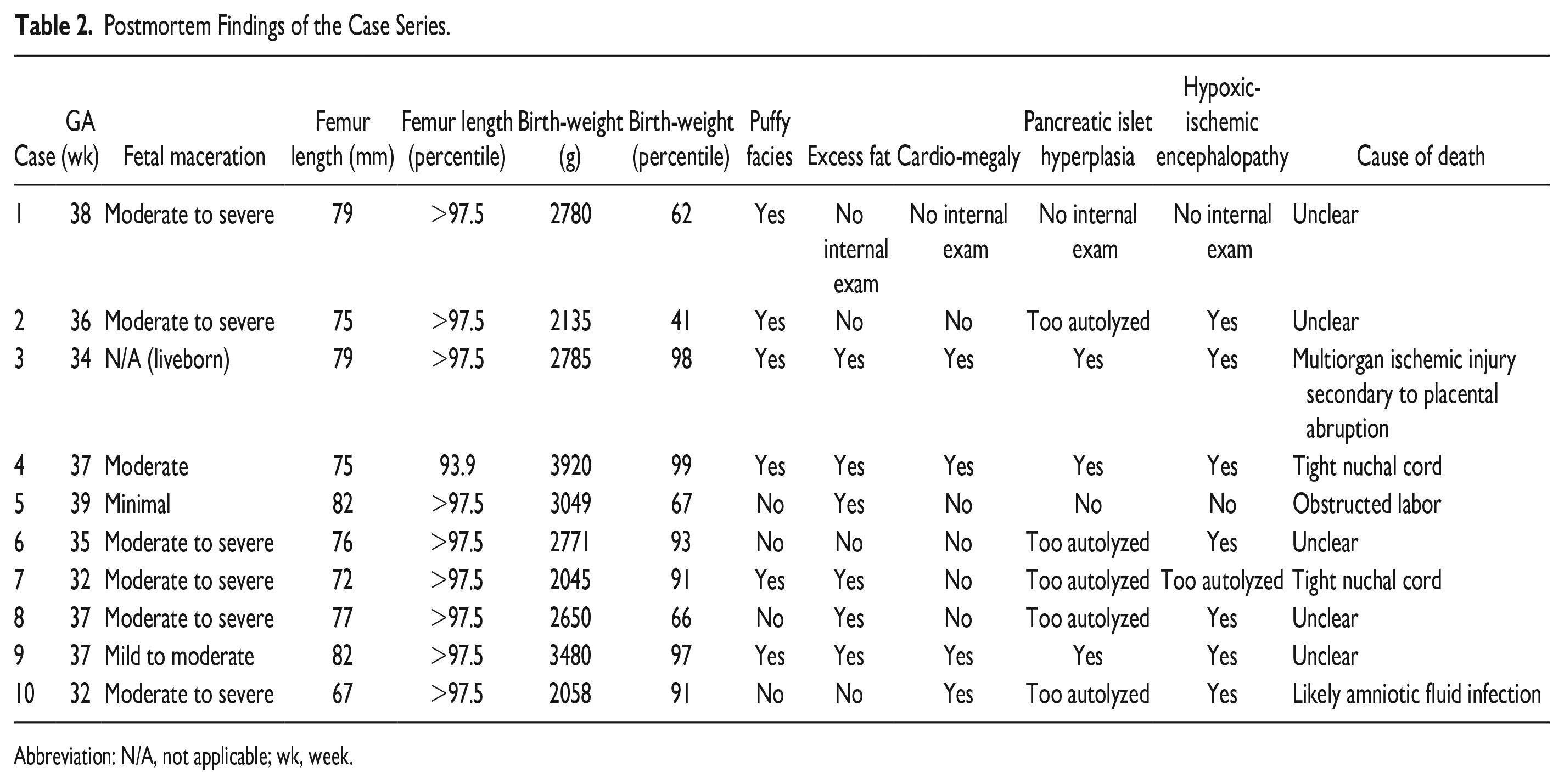
Abbreviation: N/A, not applicable; wk, week.
Placental Characteristics of the Case Series.
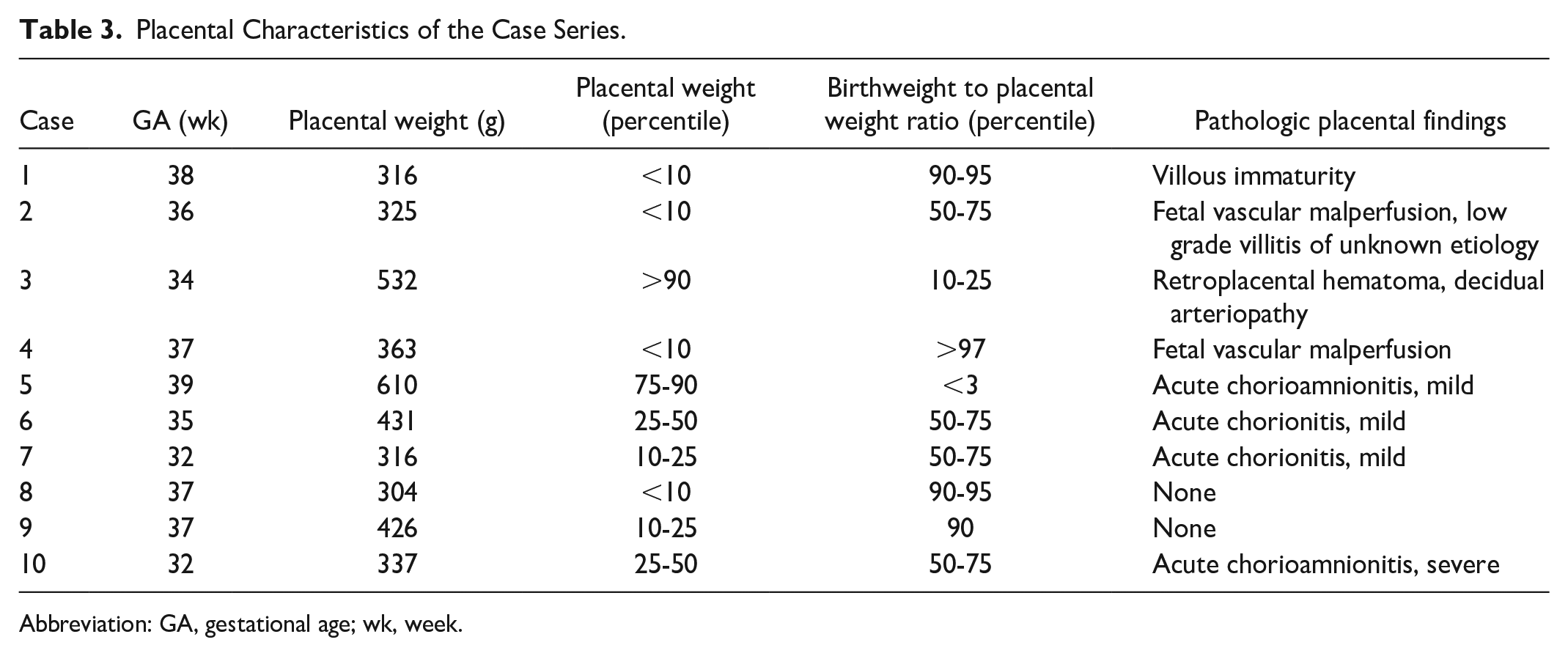
Abbreviation: GA, gestational age; wk, week.
The gestational age at delivery of the 10 cases ranged from 32 to 39 weeks (mean = 35.7 weeks). Maternal age ranged from 22 to 38 years (mean = 31.7 years). All 10 mothers were diagnosed with GDM by 50 g GCT and/or 75 g OGTT between 22 and 31 weeks GA (mean = 25.9 weeks GA). Maternal HbA1c levels at or around delivery ranged from 5.3% to 6.1% (mean = 5.73%). None of the mothers in our study exhibited anemia, as there have been reports suggesting a potential impact of anemia on HbA1c levels.17,25,26
In each of the 10 cases, the fetal or neonatal femoral length measurement exceeded the 90th percentile for gestational age, with 9 cases surpassing the 97.5th percentile.
Six cases had a birthweight greater than the 90th percentile for gestational age.
Puffy facies were noted in 6 cases (Figure 1(a) and (b)).
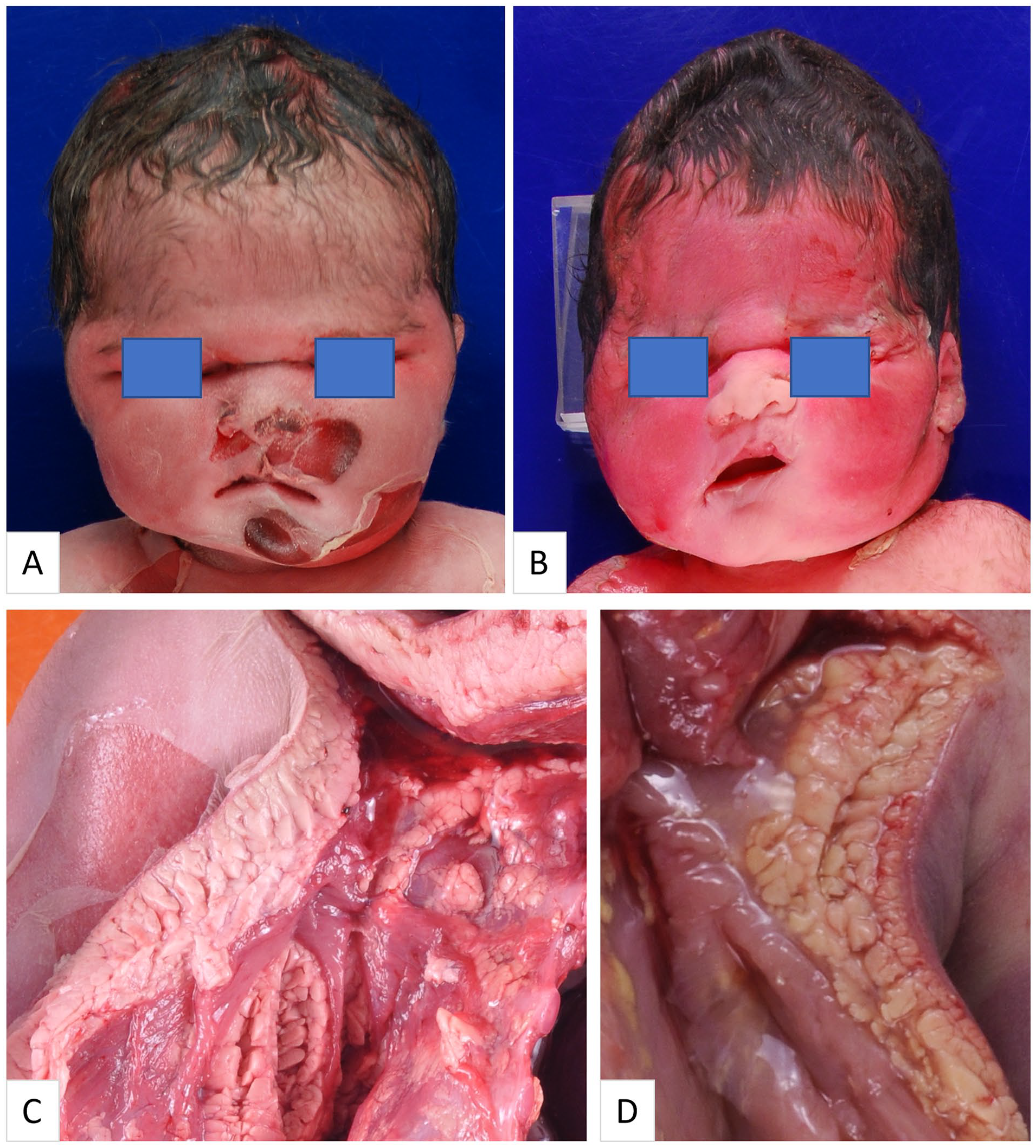
(A) (Case 4) Puffy facies with sunken eyes observed in a 37-gestational-week stillborn. The pregnancy was complicated by gestational diabetes mellitus (GDM), but the mother had a normal HbA1c of 6.1% at the time of delivery. (B) (Case 7) Puffy facies with sunken eyes observed in a 32-gestational-week stillborn. The pregnancy was complicated by GDM, but maternal HbA1c was normal (5.7%) at the time of delivery. (C) (Case 4) Excess subcutaneous adipose tissue observed in 37-gestational-week stillborn. (D) (Case 3) Excess subcutaneous adipose tissue observed in a 3-day old neonate delivered at 34 weeks of gestation. The mother had GDM but maternal HbA1c was normal (6.0%) at the time of delivery.
Among the 9 cases that underwent a complete autopsy, including internal examination, 6 cases exhibited excess adipose tissue (Figure 1(c) and (d)). Cardiomegaly was observed in 4 cases. Histologic evaluation of the pancreatic tissue was limited by severe autolysis in 5 cases, while relatively well-preserved pancreatic tissue was present in the remaining 4 cases, of which, 3 cases revealed pancreatic islet hyperplasia compared to gestational-age-matched controls (Figures 2 and 3).
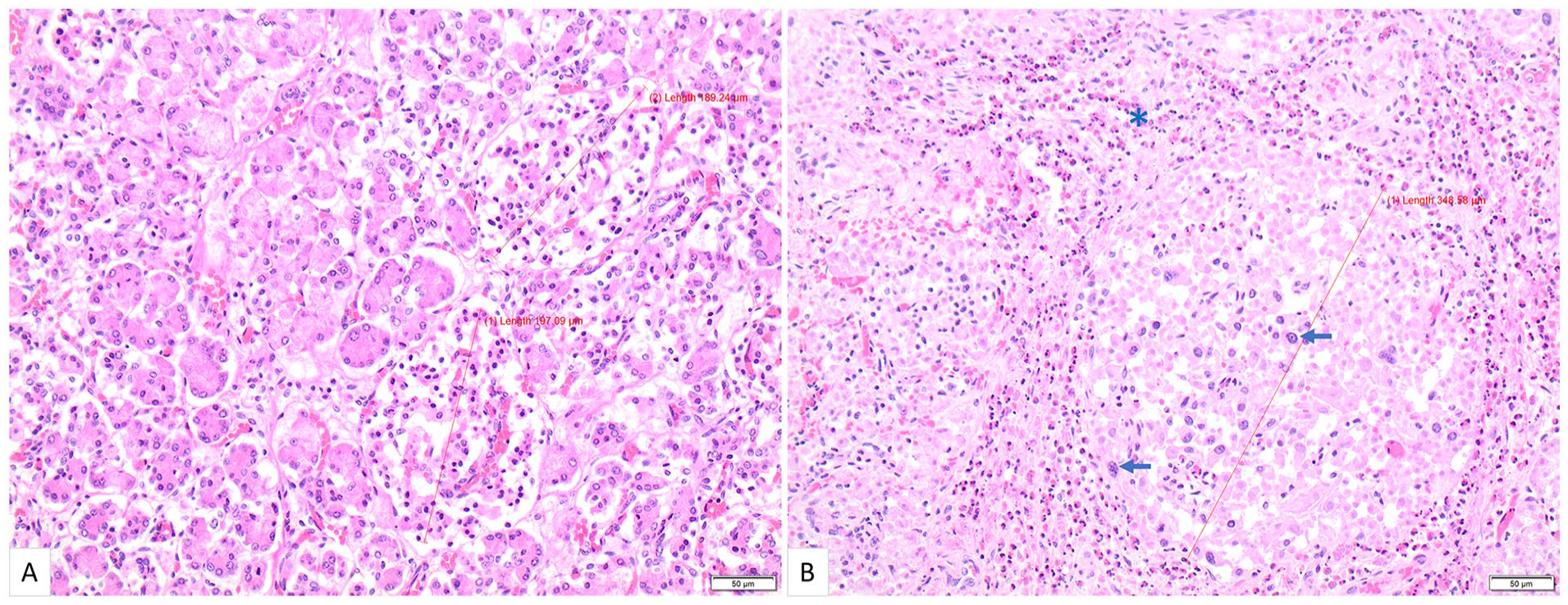
(A) Normal pancreas from a neonate who was born at 34 gestational weeks and died on day 1 of life, with no history of maternal diabetes. Note that the islets are generally under 200 μm in diameter (hematoxylin-and-eosin, 200×). (B) (Case 3) Pancreatic tissue from a neonate who was born at 34 gestational weeks and died on day 3 of life. The pregnancy was complicated by gestational diabetes mellitus, but the mother had a normal HbA1c of 6.0% at the time of delivery. Many of the islets are enlarged, measuring greater than 300 μm in diameter. Islet cell nucleomegaly (arrow) and eosinophil infiltration (*) are also present (hematoxylin-and-eosin, 200×).
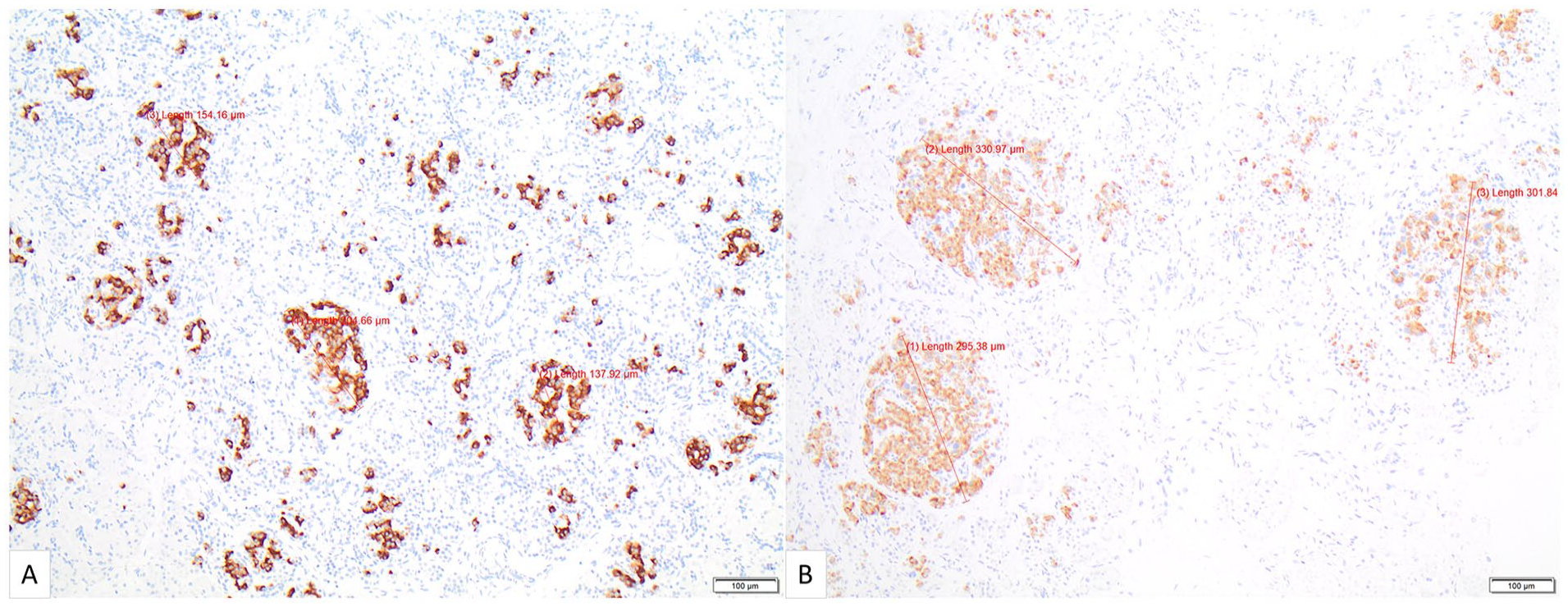
(A) Pancreas from a 37-gestational-week stillborn. There was no history of maternal diabetes. Note that the islets generally measure less than 200 μm in diameter (insulin immunohistochemistry, 100×). (B) (Case 9) Pancreas from a 37-gestational-week stillborn. The pregnancy was complicated by gestational diabetes mellitus, but the mother had a normal HbA1c level of 5.9% at the time of delivery. Note that many of the islets are enlarged, measuring approximately 300 μm in diameter (insulin immunohistochemistry, 100×).
Additionally, brain examination was conducted in 9 cases, and 7 cases showed evidence of hypoxic-ischemic encephalopathy. One case did not demonstrate hypoxic-ischemic encephalopathy, and in the remaining case, the brain was too autolyzed for pathological examination.
No structural abnormalities were noted in any of these cases.
Out of the 10 autopsy cases, the cause of death was determined in 5 cases: multiorgan ischemic injury secondary to placental abruption in 1 case, tight nuchal cords in 2 cases, obstructed labor in 1 case, and severe amniotic fluid infection in 1 case. The remaining 5 cases did not have a definitive cause of death identified.
In 4 of the 10 cases, the placentas were small, weighing less than the 10th percentile. Additionally, in 4 of 10 cases, the birthweight to placental weight ratios were equal to or more than 90th percentile for gestational age.
Discussion
Pregnancies complicated by GDM carry an increased risk of adverse outcomes, 14 underscoring the importance of assessing maternal glycemic levels in cases of perinatal demise. As a result, the evaluation of maternal HbA1c has become a standard component of stillbirth investigation protocols, as recommended by SOGC and ACOG guidelines.15,16 However, recent research indicates that HbA1c may underestimate maternal hyperglycemia in the late second-to-third trimesters. 17 Therefore, we theorized that “normal” maternal HbA1c levels in the third trimester might underestimate maternal hyperglycemia and its impact on intrauterine fetal development. We postulated that fetuses and neonates born to women with GDM in the later stages of pregnancy could potentially manifest characteristic traits of “infants of diabetic mothers,” despite the maternal HbA1c levels around the time of delivery falling within the normal range.
We performed a retrospective case series study utilizing data from our autopsy database, encompassing a period of approximately 7.5 years. The objective of this study was to describe a series of autopsy cases involving stillborn or deceased neonates delivered in the third trimester to mothers diagnosed with GDM but with normal HbA1c levels at or around delivery. The primary aim was to identify and document the characteristic features commonly associated with “infants of diabetic mothers” within this case series.
Out of the 10 cases identified, 9 were fetal deaths, and 1 was an early neonatal death. All 10 cases displayed intrauterine overgrowth (an inclusion criterion), evident through measurements of femoral length or birthweight. Moreover, 6 cases exhibited puffy facies, a common feature seen in “infants of diabetic mothers.”
Among the 10 autopsy cases, 9 underwent a complete autopsy including internal examination. Excess adipose tissue was observed in 6 cases, while cardiomegaly was detected in 4. Microscopic evaluation of relatively well-preserved (i.e., not severely autolyzed) pancreatic tissue was possible in 4 cases, with 3 showing pancreatic islet hyperplasia. Out of the 9 cases that underwent brain examination, 7 displayed evidence of hypoxic-ischemic encephalopathy, 1 did not, and 1 case could not be assessed due to autolysis. While hypoxic-ischemic encephalopathy is not typically associated with “infants of diabetic mothers,” there is an increased risk of this condition with maternal diabetes. 27 Nonetheless, in our experience, hypoxic-ischemic encephalopathy is not uncommon in stillbirths unrelated to maternal glucose intolerance.
Previous research has suggested that maternal HbA1c levels may not accurately reflect maternal blood glucose levels in late gestation.17,28,29 This study builds on these findings by demonstrating that maternal HbA1c levels could potentially underestimate the impact of maternal hyperglycemia on fetal development in utero. Specifically, our study demonstrated that third-trimester fetuses and neonates could exhibit characteristic traits commonly observed in “infants of diabetic mothers” with inadequate glycemic control, even when maternal HbA1c levels appeared to be normal around the time of delivery. This suggests that third-trimester HbA1c levels may not always accurately reflect maternal hyperglycemia and its impact on fetal development.
It is important to note that our case series represents a specific subset of autopsy cases, and our study solely aims to provide a descriptive account. Consequently, the findings cannot be extrapolated to all pregnancies characterized by GDM and normal maternal HbA1c levels in the third trimester. In other words, our observational study does not imply that the majority of women with GDM and normal HbA1c levels experience elevated blood glucose levels, or that their offspring are consistently or frequently adversely affected. Furthermore, our study does not suggest a direct GDM-related cause for the fetal or neonatal deaths observed in this case series.
Rather, this case series highlights that in certain instances of third-trimester stillbirths and early neonatal deaths associated with GDM, there may be suggestions of maternal hyperg-lycemia evident in the fetus or neonate during autopsy, despite a normal maternal HbA1c level at or around the time of delivery.
The observations of this study, namely, the presence of features of “infants of diabetic mothers” in the offspring of women with GDM despite having a normal third trimester HbA1c, may not come as a surprise. HbA1c were commonly used to reflect average blood glucose levels over the past 3 months in non-pregnant individuals, but it is not simply a mean of the blood glucose levels during that period. Instead, it is a weighted mean, where recent blood glucose levels have a greater impact on the HbA1c level than blood glucose levels from 2 to 3 months prior.30,31 This is because recent blood glucose levels influence the amount of hemoglobin glycation in the younger red blood cells, which comprise the majority of circulating red blood cells, while older blood glucose levels influence the amount of hemoglobin glycation in the older red blood cells, which comprise a smaller portion of circulating red blood cells. 32 During pregnancy, the increased production of red blood cells means that a larger fraction of younger cells are in circulation, leading to further overweighting of recent blood glucose levels on the HbA1c measurement. 32 Therefore, a single HbA1c measurement in the third trimester may not fully reflect maternal glycemic levels in the preceding months, which could have already impacted fetal development.
The observations presented in this case series have the potential to impact clinical practice. Obstetricians and pathologists may overlook the possibility that a stillbirth or neonatal death is linked to maternal GDM or glucose intolerance if the maternal HbA1c level were reportedly normal. In other words, obstetricians and pathologists may overlook or disregard the possibility of stillborn infants having features of infants of diabetic mothers when the maternal HbA1c level is within the normal range. Therefore, pathologists need to carefully consider the potential presence of features of “infants of diabetic mothers” when performing autopsy cases associated with GDM, even if the mother has a normal HbA1c level at the time of delivery.
Among these 10 cases, the cause of death remained unclear in 5 cases. Notably, 4 of these cases exhibited either a small-sized placenta (≤10th percentile for gestational age), or an elevated birthweight to placental weight ratio (≥90th percentile for gestational age). It is plausible that placental insufficiency might have played a contributory role in the fetal or neonatal demise.
There are a number of strengths associated with this case series. Pathologists specializing in pediatric and perinatal pathology conducted all autopsies and placental examinations, while pediatric and perinatal radiologists interpreted all X-rays in this study. All laboratory tests, including the GCT, OGTT, and HbA1c, were conducted in our centralized laboratory in Calgary, Alberta, Canada. This eliminated any lab-to-lab variability in the laboratory results. Moreover, in Alberta, Canada, standardized prenatal care is provided to all pregnant women, and extensive maternal laboratory investigations are performed in cases of pregnancy loss, which helps to rule out many confounding factors, particularly infections. Together, the comprehensive prenatal care and postmortem investigations contribute to reducing potential confounding variables in this case series.
This study also has several limitations and caveats that should be acknowledged. Some of the mothers in this case series were overweight or obese. Maternal BMI at 12 weeks of gestation was available in 5 cases, with 1 normal (18.5 to <25), 3 overweight (25.0 to <30), and 1 obese (≥30.0). Several studies have demonstrated that fetuses and neonates of obese women tend to have larger measurements than those of non-obese women.33,34 Therefore, in some cases, the large size of the fetus and neonate in our series may be solely or partly due to the elevated maternal BMI. Nonetheless, it is well-established that a higher proportion of obese women develop metabolic disorders, including glucose intolerance, during pregnancy than normal-weight women.35,36
There is no consensus regarding the defining features of “infants of diabetic mothers” with inadequate glycemic control. In this curated case series, we specifically included only fetuses and neonates who were large-for-gestational age, as this criterion can be objectively determined and extracted from autopsy reports. However, we acknowledge that there may be other fetuses or neonates who do not meet the large-for-gestational age criteria but exhibit other commonly observed features in “infants of diabetic mothers,” such as pancreatic islet hyperplasia, who are not encompassed in this series.
Additionally, we adopted a broader definition for large-for-gestational-age by utilizing femoral length above the 90th percentile as an alternative marker, irrespective of whether the conventional criteria based on birthweight (i.e., exceeding the 90th percentile for gestational age) were met. This is because fetuses can lose weight in utero with increasing intrauterine retention duration following demise, 37 which could result in an underestimation of large-for-gestational-age based solely on birthweight. On the other hand, longitudinal bone measurements, such as femoral lengths, have been shown to be strongly correlated with gestational age,38-40 making them a reliable marker for gauging intrauterine fetal overgrowth. Consequently, we used femoral length above the 90th percentile as an indicator for large-for-gestational-age, considering the well-established correlation between long bone lengths and gestational age.
Furthermore, we deliberately did not include macrosomia as a specific criterion for inclusion, despite its common association with infants born to diabetic mothers. The reason behind this decision is that macrosomia is typically defined as a birthweight exceeding 4000 or 4500 g, depending on the sources cited. 41 However, this definition fails to consider non-full-term fetuses and neonates, including preterm and near-term infants, who may exhibit signs of intrauterine overgrowth and possess a birthweight surpassing the 90th percentile for their gestational age, while not meeting the absolute weight criteria for macrosomia.
Maternal diabetes is known to cause pancreatic islet hyperplasia in the offspring, but assessing postmortem pancreatic tissue is challenging due to significant autolysis in most cases. In our series, among the 9 cases that underwent internal examination, only 4 had adequately preserved pancreatic tissue suitable for histological and immunohistochemical assessments. Among these 4 cases, 3 exhibited evidence of pancreatic islet hyperplasia. It is worth noting that there is a lack of published data regarding the normal size of pancreatic islets at different gestational ages. Therefore, for the purpose of diagnosing pancreatic islet hyperplasia in this study, we utilized gestational-age-matched controls as a basis for comparison. Furthermore, this series of cases underscores the possibility of underdiagnosing pancreatic islet hyperplasia in GDM-related cases due to the susceptibility of pancreatic tissue to rapid autolysis.
Conclusion
Our study reveals that even if maternal HbA1c levels during the third trimester appear normal around the time of delivery, the offspring can still exhibit traits commonly associated with “infants of diabetic mothers” with suboptimal maternal glucose control. This suggests that third trimester HbA1c levels may underestimate the influence of maternal glycemia and its subsequent effects on fetal development.
This case series highlights a potential limitation in relying solely on maternal HbA1c testing to evaluate maternal glycemic control in the investigation of stillbirths related to GDM. Although the SOGC and ACOG recommend using HbA1c to assess maternal glycemic levels in such cases, solely relying on this test may not fully capture the extent of maternal hyperglycemia during pregnancy and its potential impact on the offspring in GDM pregnancies. Therefore, it is important to recognize the limitations of HbA1c measurements when investigating stillbirths and neonatal deaths associated with GDM.
Footnotes
Acknowledgements
The authors would like to thank Kathryn Buchanan and Charlotte Monroe for their invaluable administrative support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.