
Abstract
Background:
Chronic placental inflammatory lesions (CPIL) include chronic deciduitis (CD), villitis of unknown etiology (VUE), and chronic chorioamnionitis (CCA). The frequency of these lesions and their relationship with various clinicopathological parameters in preterm birth (PTB) is presented.
Material and Methods:
Preterm placentas from April 2018 to December 2020 were reviewed for presence of CPIL. PTB was classified as spontaneous, indicated, or mixed phenotype. The association of CPIL with clinical parameters like gestational age, birth weight, obstetric complications, and placental parameters like placental dimensions, weight, vascular malperfusion, acute inflammatory lesions, and basal plate myometrial fibers were analyzed.
Results:
The study included 538 preterm placentas with 54.3% from indicated PTB. CD was more common (28.4%) than VUE (17.8%) and CCA (12.6%). CD showed significant association with VUE and CCA (both P = .0001) and VUE with CCA (P = .0001). CD was more common in indicated PTB (33.8%, P = .002) and associated with lower birth weight (1591 g vs 1705 g, P = .003), lower placental weight (270.7 g vs 296.9 g, P = .004), length (14.2 cm vs 14.8 cm, P = .006), breadth (11.7 cm vs 12.2 cm, P = .007), maternal vascular malperfusion (P = .004), and basal plate myometrial fibers (P = .02). High-grade and multifocal low-grade VUE was associated with reduced placental length (13.9 cm vs 14.6 cm, P = .02)and breadth (11.5 cm vs 12.1 cm, P = .01). CCA did not show any other association.
Conclusion:
CPIL are common in PTB and their coexistence suggested a common pathogenic mechanism. Placental examination is the only definite way to identify as they lack clinical signs and symptoms. The smaller placental size associated with these lesions may suggest alter mechanisms for adverse pregnancy outcomes
Keywords
Introduction
Chronic placental inflammatory lesions (CPIL) encompass chronic deciduitis (CD), villitis of unknown etiology (VUE), and chronic chorioamnionitis (CCA). “Chronic inflammation” refers to the presence of lymphocytes, plasma cells, and histiocytes (tissue macrophages). CD is the severe lymphocytic inflammation of the decidua or basal plate along with the presence of plasma cells, 1 though recent revisions recognize a diffuse and intense non-perivascular lymphocytes, also as a type of CD. 2 VUE is chronic inflammation affecting the villous tree, at any hierarchical level with isolated involvement of basal villi in some cases.3,4 VUE is immune-mediated and is characterized by destructive infiltration of the villous tree by maternal T lymphocytes which activate the tissue histiocytes (Hofbauer cells) present in the villi leading to a lymphohistiocytic infiltrate in the placenta. 3 CCA, is a less commonly recognized lesion in the fetal membranes, than its acute inflammatory counterpart and is characterized by infiltration of maternal T lymphocytes into the fetal membranes. Recent research evidence suggests that an immune process resembling allograft rejection between the mother and placenta-fetus dyad underlies the pathogenesis of the CPIL. 5
Preterm birth (PTB), is defined as birth before 37 weeks of gestation. Globally, the prevalence of PTB ranges from 5% to 18%, with India having a PTB prevalence of 13%. PTB is a major cause of perinatal mortality and morbidity. 6 In a significant proportion of cases, a definitive cause cannot be identified. PTB can be classified either based on the underlying cause leading to PTB or according to the gestational age.7,8 Placental examination in PTB can help us understand the underlying pathology. Acute chorioamnionitis is the most common lesion found in placentas from spontaneous PTB, whereas lesions of maternal and fetal circulatory compromise are more often found in indicated PTB, which are frequently associated with pre-eclampsia or fetal growth restriction (FGR).9-11
The significance of CPIL in preterm placentas hasn’t received much through investigation. It’s crucial to thoroughly examine a substantial group of preterm placentas to determine the prevalence, distribution patterns, as well as the clinical and pathological associations of these lesions. This primary objective of this study is to analyze CPIL in preterm placentas and gain a comprehensive understanding of their significance.
Materials and Methods
Case Selection
The study included preterm placentas obtained by the Pathology department at St. John’s Medical College from April 2018 to December 2020. Preterm placentas from singleton pregnancies delivered prior to 37 weeks of gestation and fulfilling the viability criteria (deliveries that transpired after 256/7 weeks of gestation or with a birth weight exceeding 500 g), 12 were included after excluding cases of fetal demise. The study was approved by the Institutional Ethics Committee (IEC ref No. 353/2020).
Clinical Details Collected
The clinical information collected for analysis included maternal age, gestational age, parity, and any obstetric complications besides PTB. The mode of delivery (vaginal or Cesarean section), birth weight, and Apgar scores were noted. PTB were classified as spontaneous, indicated, or multiple phenotype PTB, 7 based on the reasons for preterm delivery as documented in the medical records.
The clinical presentation of spontaneous PTB was noted including preterm prelabor rupture of membrane (PPROM), preterm labor (PTL), antepartum hemorrhage, cervical incompetence, or combinations thereof. Underlying obstetric conditions leading to indicated PTB such as preeclampsia, eclampsia, chronic hypertension, FGR, Doppler changes, and gestational diabetes mellitus were recorded. If labor progressed spontaneously despite obstetric indications, it was classified as mixed phenotype PTB. Apgar score less than 7 at 5 min was recorded as low Apgar. 13
Placental Examination Details
The placental examination, which involved both macroscopic and microscopic assessment, followed the guidelines set forth by the Amsterdam Placenta Working Group consensus statement. 14 Upon receipt, the placentas were placed in 10% neutral buffered formalin and after a detailed macroscopic description, the membranes and umbilical cord were removed. The membrane was then fixed in a Swiss roll, while the placental disc was sliced at 1 cm intervals and fixed overnight in 10% neutral buffered formalin for further detailed evaluation the following day. The trimmed placental weight was recorded along with its maximum dimensions. Both the maternal and fetal surfaces were thoroughly examined and the cut surface was inspected for any infarcts, thrombohematomas, fibrin, and other lesions if present. The thickness was measured at 2 locations and the average thickness was recorded. Umbilical cord length, diameter, knots, twists, and the translucency of the free membrane were noted. Sampling of the disc included 3 full-thickness sections from central and paracentral regions, encompassing both the maternal and fetal plates, as well as any pathological lesions. Two sections from the umbilical cord, 1 from the placental end and 1 from the fetal end were taken, and 1 sections from the membrane Swiss roll was sampled for microscopic examination.
The CPIL were defined and analyzed as follows:
(A) Chronic deciduitis (CD): presence of lymphoplasmacytic inflammation in the decidua or, the presence of diffuse and intense non-perivascular lymphocytic inflammation. 2
(B) Villitis of unknown etiology (VUE): Lymphohistiocytic inflammation involving the villi. VUE was further classified as:
Low-grade
when less than 10 villi were involved and presence of more than 1 such focus. Low grade was classified as (i) focal—seen in 1 slide or (ii) multifocal—present in more than 1 slide.
High grade
When more than 10 villi are involved at least in 1 focus with multiple foci of involvement. High grade was classified as (i) patchy-multiple foci of involvement or (ii) diffuse-more than 30% of distal villous involvement.
(C) Chronic chorioamnionitis (CCA) 15 : Infiltration of lymphocytes within the chorioamnion of the chorionic plate and/or fetal membranes. Chronic chorioamnionitis was further graded and staged as
Stage 1: lymphocytic infiltration limited to chorionic trophoblast layer
Stage 2: lymphocytic infiltration into the chorioamnionic connective tissue.
Grade 1: more than 2 foci/patchy inflammation
Grade 2: diffuse inflammation
The other microscopic parameters that were analyzed include:
(a) Maternal vascular malperfusion.
(b) Fetal vascular malperfusion.
(c) Acute Inflammatory lesions: Maternal and fetal inflammatory response.
(d) Presence of nucleated RBCs (nRBCs) in fetal vasculature
(e) Basal plate myometrial fibers.
Statistical Analysis
The study presents the frequency of CPIL in preterm placentas. Mean values with standard deviation and range were used to report continuous variables, while percentages were used for categorical variables. The association between CPIL and clinical and placental parameters was analyzed using the Chi-square test for categorical variables and the independent sample t test for comparing means. A P-value of less than .05 was considered statistically significant and all the non significant parameters as denoted as P = NS.
Results
Baseline Characterization of the Study Cohort
The study included 538 placentas from PTB, after applying the exclusion criteria. The maternal age spanned from 17 to 46 years, with an average maternal age of 26.9 years (±5). The average gestational age was 33 weeks (±2.8). Primiparity constituted 46.7% of the cases. Vaginal delivery occurred in 151 cases (28%), whereas 387 mothers (72%) underwent Cesarean section. A total of 56 cases (10.4%) presented with a low Apgar score.
A total of 384 cases (71.4%) experienced obstetric complications. The most prevalent obstetric complication observed was hypertensive disorders of pregnancy, which included gestational hypertension, eclampsia, and preeclampsia, seen in 251 cases (46.7%). Other documented obstetric complications were FGR (n = 99, 18.4%), gestational diabetes mellitus (n = 55,10.2%), oligohydramnios (n = 78, 14.5%), polyhydramnios (n = 5, 0.9%), PPROM (n = 121, 22.5%), PTL (n = 82, 15.2%), antepartum hemorrhage (n = 56, 10.4%), and cervical incompetence (n = 11, 2%).
Spontaneous PTB occurred in 154 cases (28.6%), while indicated PTB was recorded in 292 cases (54.3%). The mixed phenotype PTB accounted for 92 cases (17.1%). Of the spontaneous PTB cases, the most common clinical presentation was PPROM, while pre-eclampsia emerged as the leading obstetric complication association with indicated PTB, representing 45.7% of the cases.
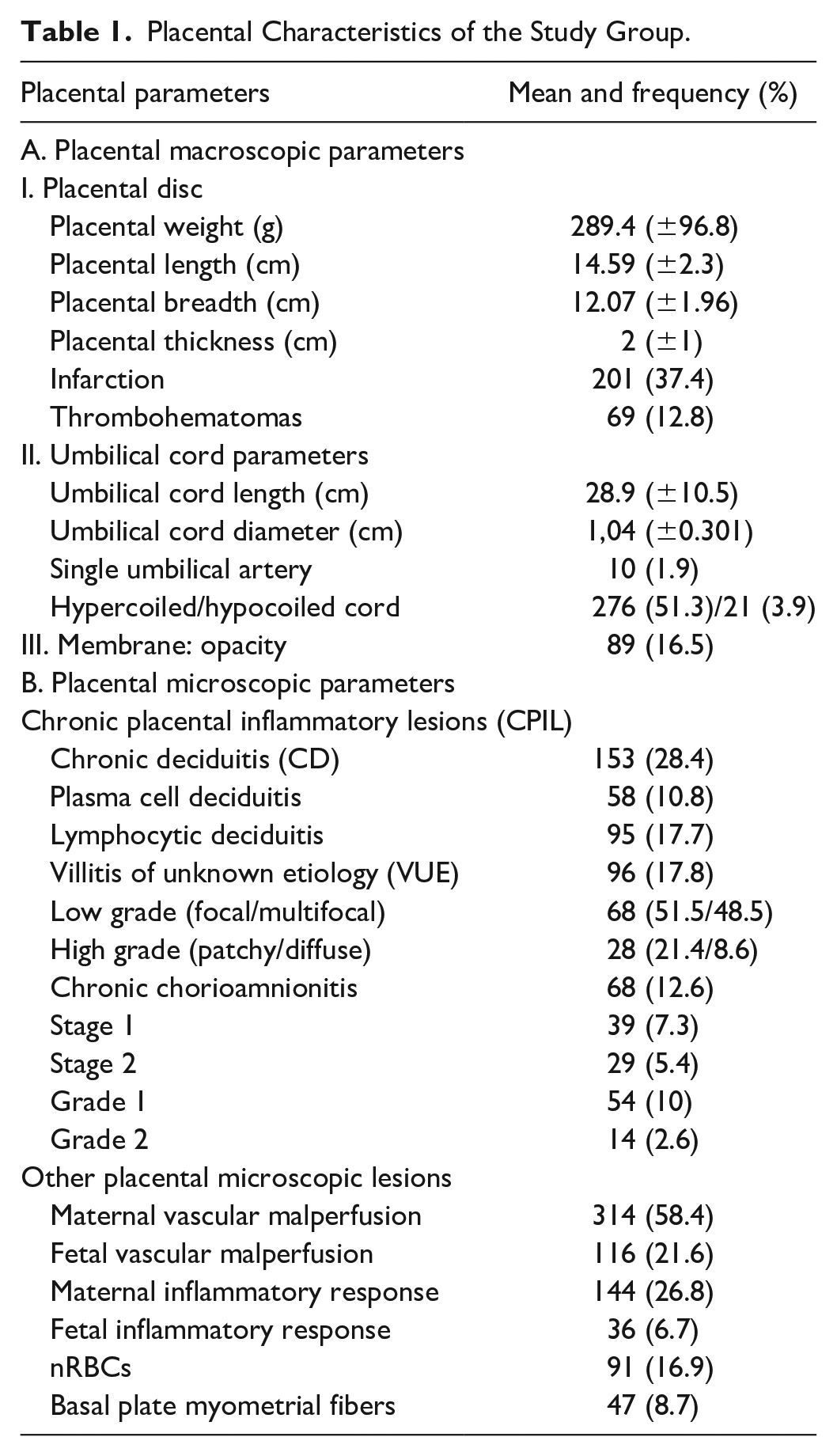
The placental macroscopic and microscopic details are described in Table 1
Placental Characteristics of the Study Group.
Chronic Inflammatory Lesions in Preterm Placentas
CD was identified in 28.4%, while VUE was observed in 17.8% and CCA in 12.6% of PTB. The association of these lesions with various clinical and placental parameters is elaborated below.
A. Chronic Deciduitis (CD)
Frequency and association with clinical parameters
Of the 153 placentas with CD, 51.3% were from multiparous women, and 74% were from Cesarean section deliveries. The mean birth weight was significantly lower in cases with CD compared to those without (1590 g vs 1710 g, P = .03). The occurrence of CD in spontaneous PTB was 20.8%, while indicated and mixed phenotype PTB featured 33.2% and 26% respectively. The difference between the groups was statistically significant (P = .02) with higher frequency of CD observed in indicated PTB.
Frequency and association with placental parameters
Placentas with CD exhibited significant differences compared to those without CD as represented in Figure 1. The mean placental weight (270.7 g vs 296.9 g, P = .004), placental length (14.2 cm vs 14.8 cm, P = .006), and placental breadth (11.7 cm vs 12.2 cm, P = .007) were lower when CD was present. However, there was no observed association between CD and placental thickness, umbilical cord length, or diameter (P = NS).
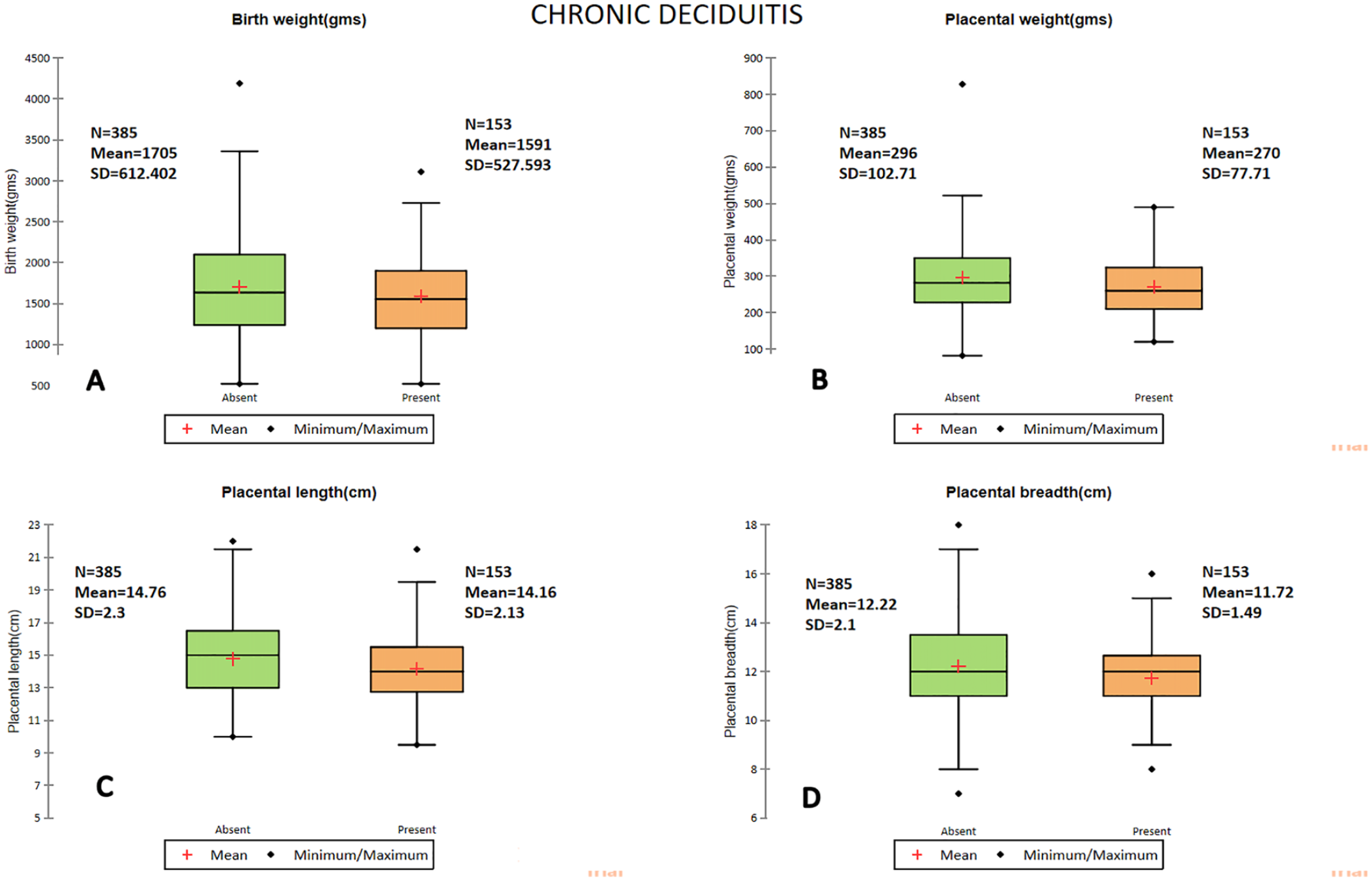
Box and Whiskers plot representing the difference in mean for birth weight (A), placental weight (B), placental length (C), and placental breadth (D), between placentas with and without chronic deciduitis.
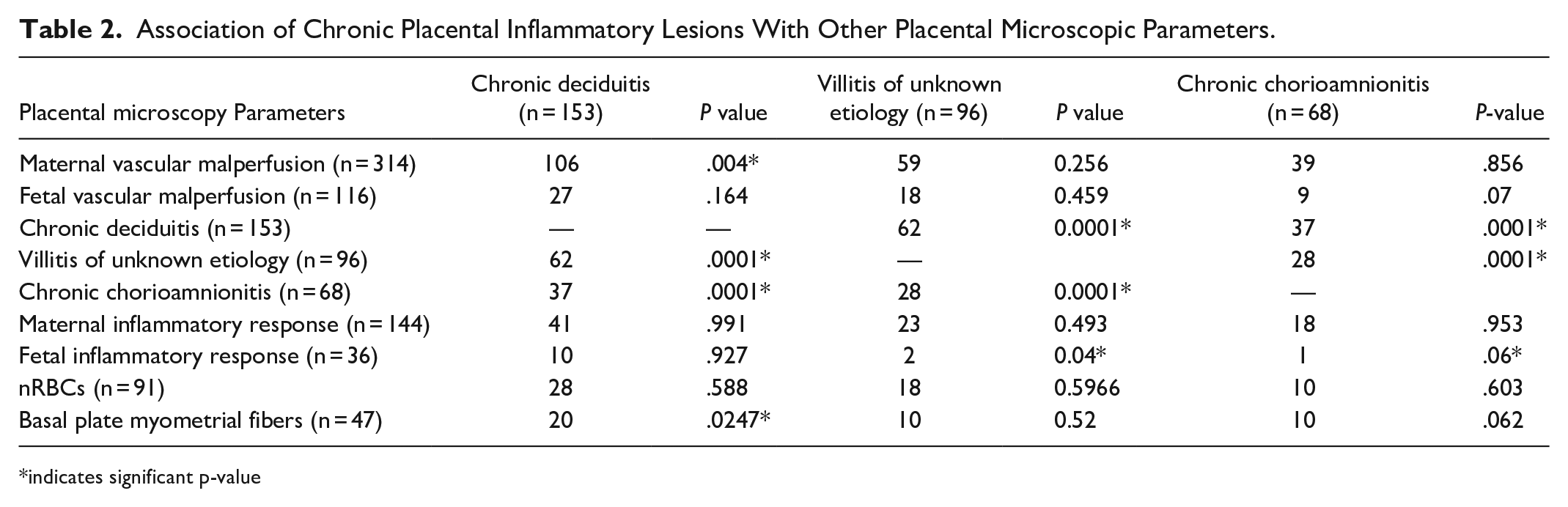
CD was found to be significantly associated with both VUE and CCA (both P = .0001). Amongst the other microscopic parameters, maternal vascular malperfusion (P = .004) and basal plate myometrial fibers (P = .02) showed significant association with CD. We did a further stratified analysis to look at the association of cell type specific deciduitis (plasma cell type CD and lymphocytic CD) with other parameters. The plasma cell type CD showed significant association with VUE (58.4%, P = .0006) and CCA (37.9%, P = .003) while no other clinical or placental parameters showed any association. The associations are shown in Table 2.
Association of Chronic Placental Inflammatory Lesions With Other Placental Microscopic Parameters.
indicates significant p-value
B. Villitis of Unknown Etiology (VUE)
Frequency and association with clinical parameters
Of the 96 placentas with VUE, 53% were from multiparous women and 69.8% cases were from Cesarean sections deliveries. The mean gestational age was higher in placentas with VUE (33.5 weeks vs 32.9 weeks, P = NS). No significant association was found between any clinical parameter and VUE (P = NS). The frequency of VUE in placentas from spontaneous PTB was 14.9% (n = 23), while placentas from indicated PTB and mixed phenotype PTB had a frequency of 19.8% (n = 58) and 16.3% (n = 15) respectively (P = NS).
Frequency and association with placental parameters
Other than its association with CD and CCA (both P = .0001), VUE did not exhibit any significant association with placental macroscopic or other microscopic parameters. Of note, the mean placental breadth was smaller in placentas with VUE (11.7 cm vs 12.14 cm, P = .07), though not statistically significant.
Upon further stratified analysis, it was found that high-grade lesions and multifocal low-grade lesions of VUE, which comprised 61 cases, exhibited a significant association with placental length and breadth. Placentas with high grade and multifocal low grade VUE had reduced length (13.9 cm vs 14.6, P = .02) and breadth (11.5 cm vs 12.1 cm, P = .01) compared to those without. The differences in means are depicted as box plots in Figure 2. Table 2 shows the association of VUE with other microscopic parameters.
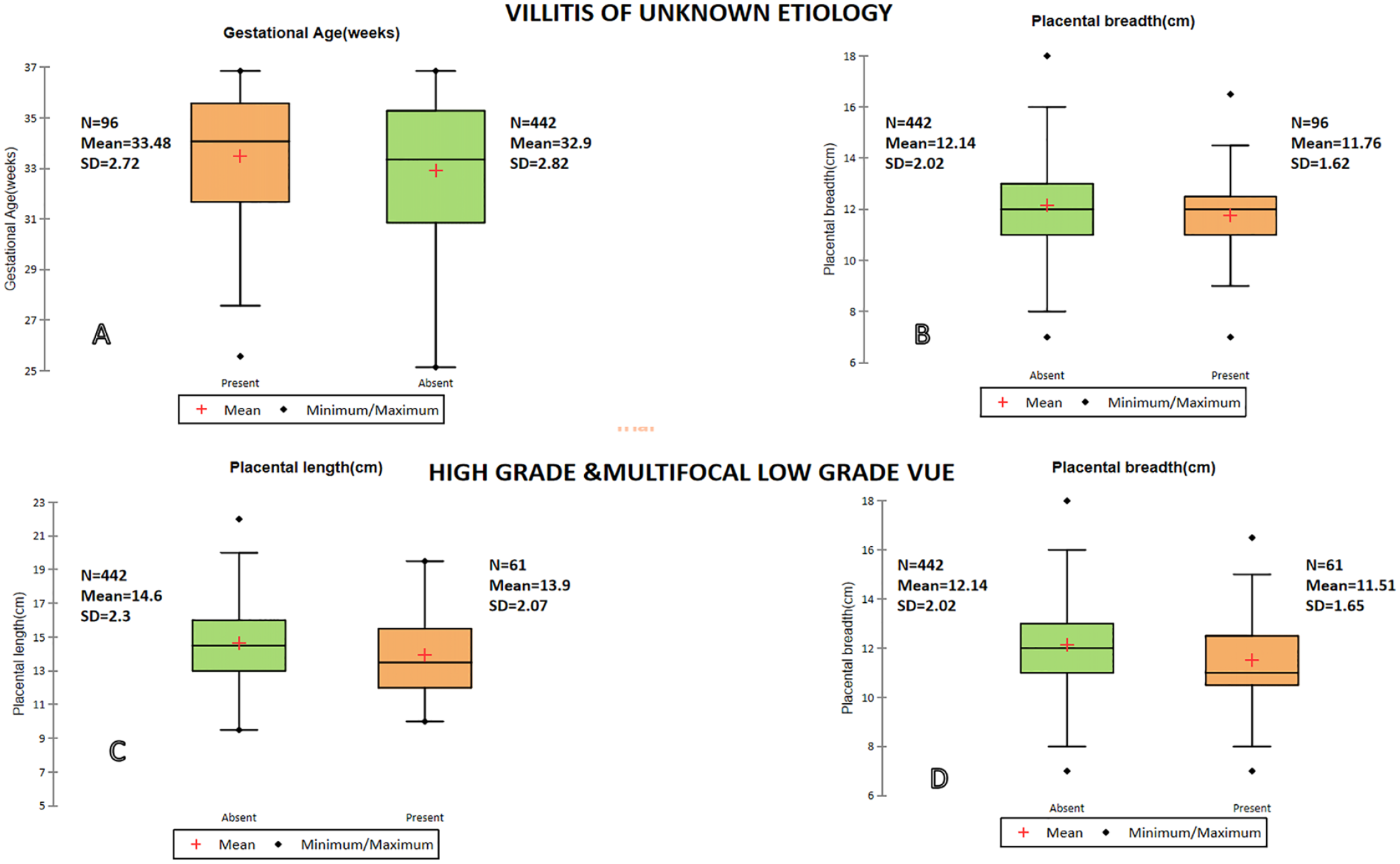
Box and Whiskers plot representing the difference in mean for gestational age (A) and placental breadth (B) for placentas with and without villitis of unknown etiology (VUE). The lower panel demonstrates the difference in mean for placental length (C)and breadth (D)for placentas with and without high-grade and multifocal low-grade VUE.
C. Chronic Chorioamnionitis (CCA)
Frequency and association with clinical parameters
Of the 68 placentas with CCA, 54.4% were from multiparous women and 85.3% cases were from Cesarean sections deliveries. The mean gestational age was higher in placentas with CCA (33.4 weeks vs 32.9 weeks, P = NS). No significant association was found with any clinical parameter (P = NS). The frequency of CCA in placentas from spontaneous PTB was 11% (n = 17), while indicated and multiple phenotype PTB featured 13.7% (n = 40) and 11.9% (n = 11) respectively (P = NS).
Frequency and association with placental parameters
There were no significant associations observed between CCA with any macroscopic or microscopic placental parameters other than CD and VUE (both P = .0001). Further stratified analysis based on stage and grade was not conducted as there was no significant association observed. Table 2 provides details of the association of CCA with other microscopic parameters.
A composite microscopic representation of the chronic placental inflammatory lesions is shown in Figure 3.
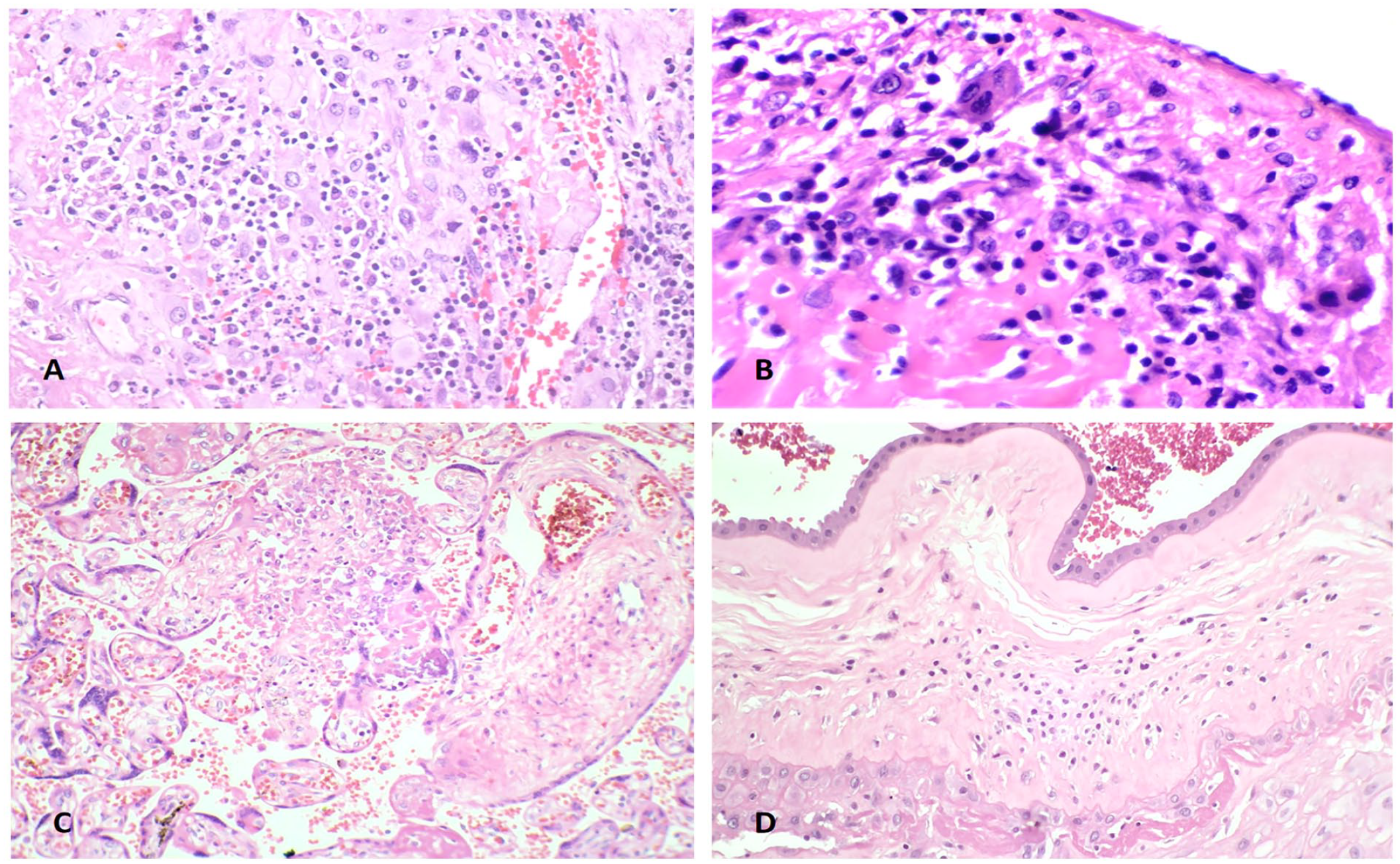
Photomicrograph showing chronic deciduitis with plasma cells (A, original magnification ×100) and lymphocytes (B, original magnification ×100). Lower panel shows villitis (C, original magnification ×100) and chronic chorioamnionitis in extraplacental membranes (D, original magnification ×100).
Discussion
PTB is a challenging obstetric condition that poses significant challenges due to its association with both immediate and long-term complication and abnormal developmental outcomes in newborns. 16 CPIL are manifestations of immune-mediated maternal anti-fetal response. 5 The objective of this study was to examine the prevalence of CPIL and explore their clinical significance in the context of PTB.
In our study CD was identified as the most frequent CPIL observed in preterm placentas. This finding aligns with previous research conducted by Edmondson et al who first reported the association between CD and preterm labor, even in the absence of clinical chorioamnionitis. 17 Edmondson et al observed no significant association of CD with acute inflammatory pathologies or villitis. However, the present study revealed a significant association with VUE, which is supported by the emerging evidence pointing toward a of common immune-mediated pathogenesis for all these conditions. 5 We have previously reported a similar association between CD and VUE in a study of 1603 placentas that included both preterm and term deliveries. 4
We observed a higher frequency of CD in cases of indicated PTB, where preeclampsia was the most common obstetric complication. This finding is consistent with previous studies that have reported and an association between decidual inflammation and preeclampsia with CD considered a factor associated with poor perinatal outcomes. 18 Another noteworthy finding was the association between the presence of CD and basal plate myometrial fibers. This association is supported by the findings of Ernst et al. 19 The frequency of basal plate myometrial fibers in this study on preterm placentas was 8.7%, which is line with the reported frequency of 9.6% in PTB according to Sherer et al. 20
VUE was observed in 18% of the cases, and high grade and multifocal low grade lesions were associated with smaller placental dimensions. These findings are supported by our previous study on VUE, where we also found a higher frequency of this lesion in PTB cases and its impact on placental dimensions. 4 Initially, VUE was considered as a lesion primarily found in term placentas with little clinical significance, 5 which was challenged in the subsequent studies, reporting higher frequency of VUE in PTB and its association with great obstetric syndromes.21,22 The association we demonstrate between VUE and CCA is supported by the work of Quershi and Jacques, 23 further suggesting a shared immunological pathogenesis for these lesions.
CCA was the least frequent CPIL in PTB accounting for 12.6% of cases. Lee et al 24 reported a frequency of 20.8% in PTB. CCA was first identified as a lymphocytic infiltrate at the choriodecidual interface of the fetal membranes by Gersell et al. 25 Subsequent studies have recognized CCA as an important etiological mechanism for preterm birth, particularly in late preterm. 24 Its association with CD and VUE underpins abnormal immune tolerance as a mechanism for its development.
The findings of the current study suggest that CPIL are relatively common in preterm placentas. However, the study is limited by the non-inclusion of term placentas for comparison of the frequency of these lesions. Nevertheless, the study utilizes a large cohort of preterm placentas from a single institution and the adherence to well-accepted placental examination and reporting guidelines, which enhances the robustness and comparability of the results to other similar studies.
To summarize, chronic placental inflammatory lesions are frequently observed in preterm placentas and may represent one of the pathogenic mechanisms leading to preterm delivery as a result of altered immune tolerance between the mother and placenta-fetal dyad. Further research into the early detection of molecules associated with cell and antibody-mediated rejection in maternal circulation may aid in understanding and supporting this hypothesis, ultimately leading to the development of interventions that prolong pregnancy and prevent preterm delivery.
Footnotes
Acknowledgements
We thank the pregnant mothers who were a part of this study
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.