
Abstract
Introduction
Prepregnancy obesity is a growing global health problem and has several risks for mother and child. The aim of this study was to systematically examine the effect of increased maternal body mass index (BMI) on placental pathology in otherwise uneventful term pregnancies.
Methods
In this analysis, we studied data of the Netherlands Amniotic Fluid study, a prospective study of women delivering in Utrecht, the Netherlands, between 2006 and 2007. We included women with uncomplicated pregnancies, vaginal delivery, and data on prepregnancy weight and height (n = 382). Placental histopathology was compared between women of normal BMI (≤24.9 kg/m2), overweight (25–29.9 kg/m2), and obese (≥30 kg/m2).
Results
Increasing prepregnancy BMI was associated with heavier placentas and higher mean infant’s birth weight. In addition, obesity was positively associated with high-grade chronic villitis (odds ratio [OR]: 18.1, 95% confidence interval [CI]: 1.6–205.2), accelerated villous maturation (OR: 1.1, 95% CI: 1.0–1.2), and lower incidence of placental weight below the 10th percentile for gestational age (OR: 0.5, 95% CI: 0.3–1.0). There was a substantial effect of parity on maternal, placental, and neonatal weights.
Conclusions
Even in uncomplicated pregnancies, maternal obesity is associated with characteristic changes in placental pathology. Further research is needed to evaluate these changes in view of later-life health of infants born to obese mothers.
Introduction
Obesity is one of the fastest growing global health problems among women of reproductive age. 1 In the United States, almost two-thirds of women of child-bearing age are overweight and one-third is obese. 2 In most European countries, including the Netherlands, obesity prevalence is lower (approximately 15%), but trends over time project similar rates within the next decade.1–4 Women with a higher prepregnancy body mass index (BMI) are at risk of a several obstetric complications (ie, gestational diabetes mellitus [GDM], preeclampsia, large-for-gestational-age [LGA] birth weight babies) associated with higher morbidity for both mother and child.2,5–9 A long-term higher risk of obesity and metabolic syndrome is seen in offspring of these obese mothers. Most of these complications are likely mediated by the effect of obesity on placental function, including placental production of growth factors, hormones, and the transport of nutrients to the fetus, causing pregnancy complications and long-term fetal programming concerns. 10 It is unknown to what extent high BMI affects characteristics of the placenta and infants in healthy uncomplicated pregnancy. Animal studies have shown that maternal obesity is independently associated with increased placental messenger RNA levels of toll-like receptor (TLR)-2 and TLR-4 and show higher levels of pro-inflammatory cytokines. 11 In humans, studies have suggested an increased maternal inflammatory response (MIR) in obese pregnancy, as shown by elevated levels of circulating IL-6 and higher levels of placental pro-inflammatory cytokines. 12 Only few studies have evaluated the relationship between obesity and placental pathology, reporting an effect of increased MIR in placentas of obese mothers (ie, chorioamnionitis), a higher prevalence of chronic villitis, and a higher prevalence of vascular lesions (ie, acute atherosis and villous infarctions) related to maternal vascular under perfusion.13–15 These reports, however, were based on both complicated and uncomplicated pregnancy.13–15 The aim of this study was to systematically examine the association between maternal BMI and placental pathology, using a well-defined cohort of women with uneventful term pregnancies with unassisted vaginal delivery stratified into different clinically relevant BMI groups.
Methods
Study Population
This study was part of the Netherlands Amniotic Fluid study, which was set up to investigate the role of intrauterine inflammation in the onset of spontaneous term labor. The full setup of this study was described previously.16,17 In short, a cross-sectional study was performed in 1 secondary and 1 tertiary hospital in Utrecht, the Netherlands. Women with uncomplicated pregnancies who had a spontaneous vaginal delivery between 2006 and 2007 were included (n = 578). Explicitly, women in this study were screened for specific pregnancy complications (ie, GDM, preeclampsia, fetal growth restriction [FGR]) when indicated according to Dutch standard prenatal care guidelines and did not get diagnosed with any of these conditions before delivery. The ethical review board approved the study, and all parents provided written informed consent for study participation. In this study, we included the women of whom information was available regarding both placental pathology and self-reported weight and height measurements before pregnancy (n = 382).
Clinical Characteristics
All necessary clinical maternal (ie, age, parity, gestational age, length, and weight) and fetal characteristics (ie, birth weight, APGAR scores) were collected as previously described.16,17 BMI was calculated according to the standard formula (kg/m2), and patients were divided in 3 groups according to World Health Organization classification: normal BMI (≤24.9 kg/m2), overweight (25.0–29.9 kg/m2), and obese (≥30.0 kg/m2). 18
Placental Pathology
All placentas were stored at 4℃ and were processed by 1 experienced pathologist (PGJN) within 72 hours. Because some of the pathological findings depend on gestational age (ie, maturation of placenta parenchyma, weight percentiles), information on gestational age at delivery was disclosed. Other clinical parameters were not disclosed to the pathologist before review.
Placental weight was defined without membranes or umbilical cord, and weight for gestational age percentiles were used from Pinar et al. 19 Placental weight below the 10th percentile and above the 90th percentile was classified as abnormal. Fetal/placental weight ratios were calculated. Macroscopic cord coiling index was determined by measuring the number of complete coils (360°) divided by the total length of the attached umbilical cord (cm). Coiling was determined fresh, before formalin fixation. A coiling index below 0.1 was considered as hypocoiling, and hypercoiling was defined as a coiling index above 0.3.
Histology
Two sections of umbilical cord, a membrane roll, and 3 slides of macroscopically normal placental tissue (including both decidua and chorionic plate) were collected and stained with hematoxylin and eosin. Additional samples were taken from areas that macroscopically appeared abnormal. A full histology examination was performed based on the criteria as previously reported.16,20,21 Placental lesions are defined in Supplementary Table 1. MIR was defined as an abnormal presence of polymorphonuclear leukocyte cells in the chorionic plate or extraplacental membranes (also described as acute chorioamnionitis). Fetal inflammatory response (FIR) was defined as aggregates of neutrophils in umbilical vascular wall with or without expansion in Wharton’s jelly (also known as acute funisitis). Chronic villitis was defined as infiltration of lymphocytes and macrophages in the placental villi.
Statistical Analysis
Statistical analyses were performed using SPSS version 21.0 (IBM Corp). χ 2 test was used to examine differences between placental pathological lesions among the groups in case of categorical variables. For continuous variables, 1-way analysis of variance testing was conducted. Linear regression was used to determine correlation coefficients between continuous variables. We considered differences to be statistically significant at P < .05.
Results
Baseline Characteristics
Maternal and Neonatal Characteristics Per BMI Category.
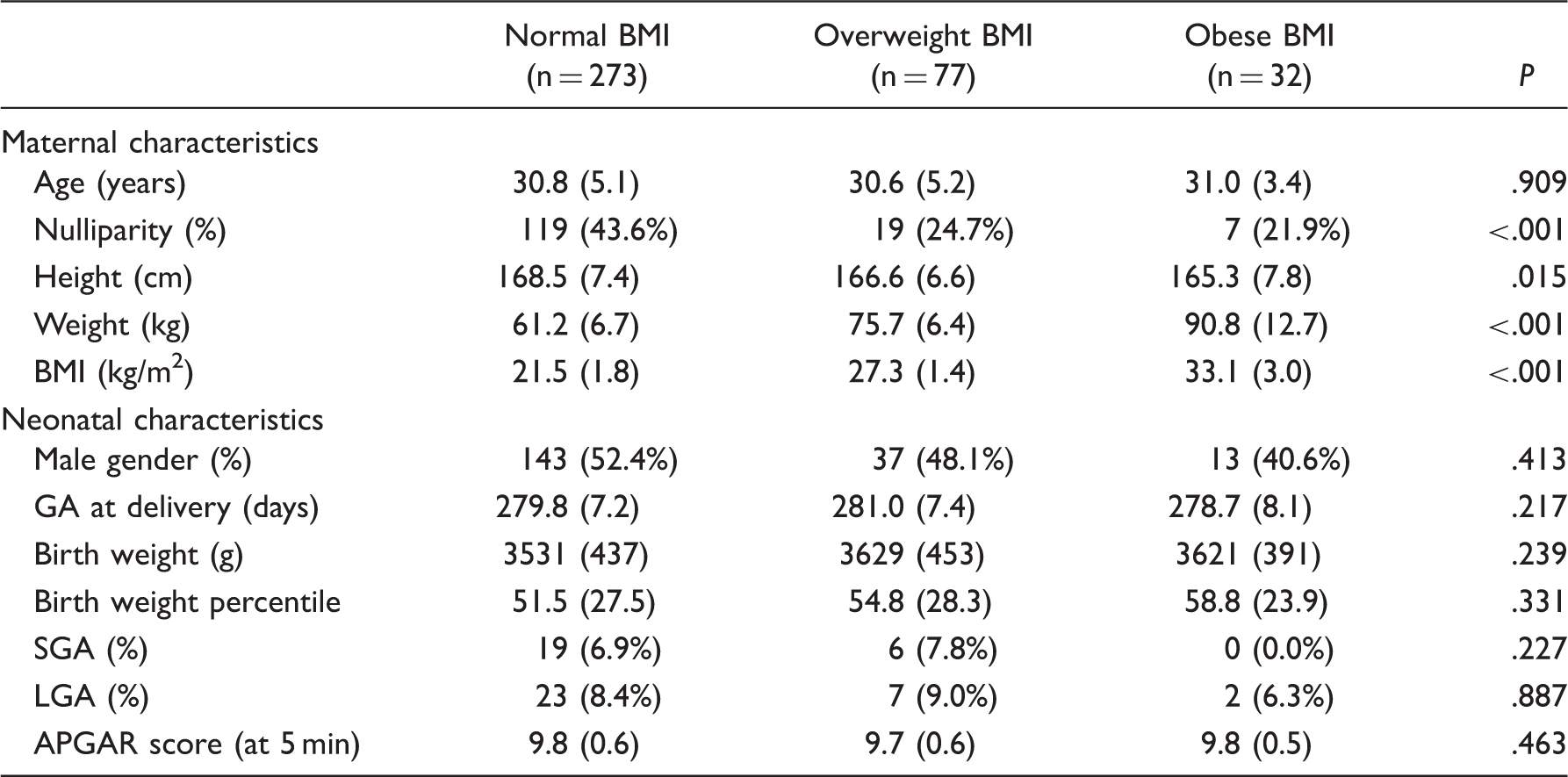
Abbreviations: ANOVA, analysis of variance; BMI, body mass index; GA, gestational age; LGA, large for gestational age; SGA, small for gestational age.
Values are presented as means (standard deviation) or as numbers (%). P values were calculated by 1-way ANOVA for continuous variables and χ2 test for categorical variables. BMI (kg/m2): normal BMI (<24.9 kg/m2), overweight (25.0–29.9 kg/m2), and obese (>30.0 kg/m2); GA (days); SGA (birthweight <10th percentile); LGA (birthweight >90th percentile). APGAR scores were determined 5 min postpartum.
Placental Pathology
Placental Pathology Characteristics Per BMI Category.
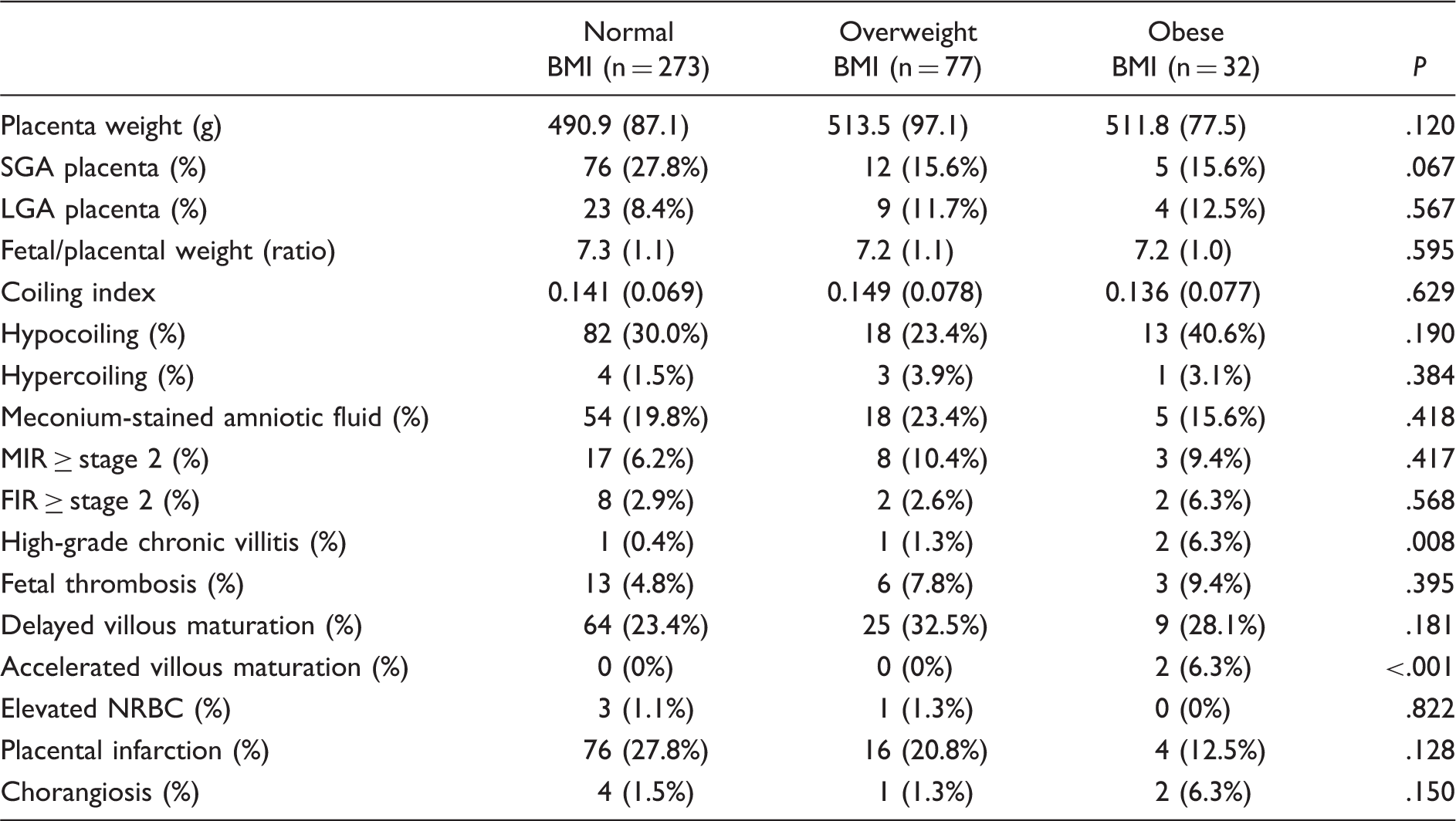
Abbreviations: ANOVA, analysis of variance; BMI, body mass index; FIR, fetal inflammatory response; LGA, large for gestational age; MIR, maternal inflammatory response; NRBC, nucleated red blood cells; SGA, small for gestational age.
Values are presented as means (standard deviation) or as numbers (%). P values were calculated by 1-way ANOVA for continuous variables and χ2 test for categorical variables. BMI: normal BMI (<24.9 kg/m2), overweight (25.0–29.9 kg/m2), and obese (>30.0 kg/m2); SGA placenta: placental weight <10th percentile. LGA placenta: placental weight >90th percentile. MIR: chorioamnionitis ≥stage 2. FIR: acute funisitis ≥stage 2. Chronic villitis: relevant when high grade/diffuse. Thrombosis: relevant when medium/high grade. Placental infarction: presence of <5% infarction in the placenta versus none.
Risk of Placental Pathology Characteristics per BMI Category.
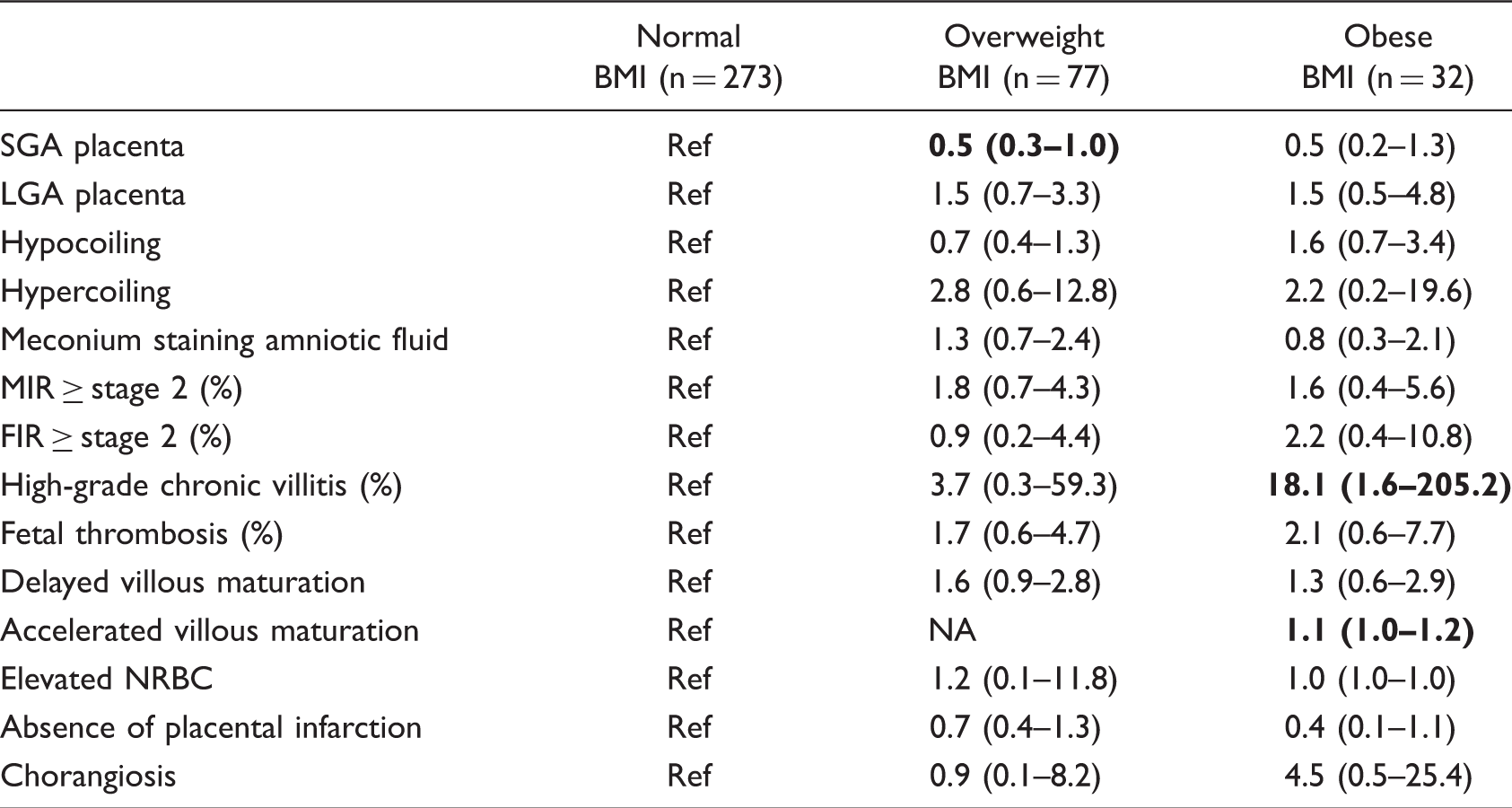
Abbreviations: BMI, body mass index; FIR, fetal inflammatory response; LGA, large for gestational age; MIR, maternal inflammatory response; NA, not applicable; NRBC, nucleated red blood cells; OR, odds ratio; SGA, small for gestational age.
Values are presented as ORs and 95% confidence intervals. Values and statistical significance were calculated by χ2 tests. OR values in bold were statistically significant with P < .05. BMI: normal BMI (<24.9 kg/m2), overweight (25.0–29.9 kg/m2), and obese (>30.0 kg/m2); SGA placenta: placental weight <10th percentile. LGA placenta: placental weight >90th percentile. MIR: chorioamnionitis ≥stage 2. FIR: acute funisitis ≥stage 2. Chronic villitis: relevant when high grade/diffuse. Thrombosis: relevant when medium/high grade.
When comparing the occurrence of high-grade chronic villitis (≥grade 2) in the overweight (n = 1 [1.3%]) and obese group (n = 2 [6.3%]) to women with a normal BMI (n = 1 [0.4%]), there was a significant difference among the groups with higher occurrence in the heavier women (OR: 3.7, 95% CI: 0.3–59.3, P = .338 and OR: 18.1, 95% CI: 1.6–205.2, P = .001, respectively). We did not find a statistical difference when looking at low-grade chronic villitis (occurrence 16.5%–18.7% among the groups, data not shown). Furthermore, we found a difference in maturation of the placental villi, with more accelerated maturation in the obese group (n = 2 [6.3%] in the obese group vs n = 0 (0%) in women with normal BMI; OR: 1.1, 95% CI: 1.0–1.2, P ≤ .001). We found more delayed maturation in the overweight group, although this did not reach statistical significance (OR: 1.6, 95% CI: 0.9–2.8, P = .07) and the data did not show the same trend in the obese group. We found that overweight women had a smaller chance of delivering a placenta <10th percentile (n = 12 [15.6%] in overweight BMI vs n = 76 [27.8%] in normal BMI, OR: 0.5, 95% CI: 0.3–1.0, P = .05). The obese group showed a similar trend, although not statistically significant (n = 5 [15.6%] in obese BMI, OR: 0.5, 95% CI: 0.2–1.3, P = .14). We found no significant differences in the presence of placental thrombosis, infarction (none vs <5%), chorangiosis, MIR, or FIR. Placental weight, coiling index, and fetoplacental weight ratio did not vary significantly among the groups.
Furthermore, we found a significant correlation between maternal BMI and birth weight (Figure 1(A), r = .113; P = .037) and weight of the placenta (Figure 1(B), r = .109; P = .027) but not with birth weight percentile or fetoplacental weight ratios (data not shown). As we found that parity was consistently and significantly different over the BMI groups (Supplementary Figure 1, r = .243; P ≤ .001), we also performed linear regression analysis comparing parity to both birth weight and placental weight and found they were both significantly correlated (r = .134; P = .0083 and r = .139; P = .0065, respectively, Supplementary Figures 2 and 3).
Neonatal birth weight (A) and placental weight (B) Pearson correlation with BMI (kg/m2) in singleton pregnancies in women with uncomplicated pregnancy (n = 382). BMI, body mass index.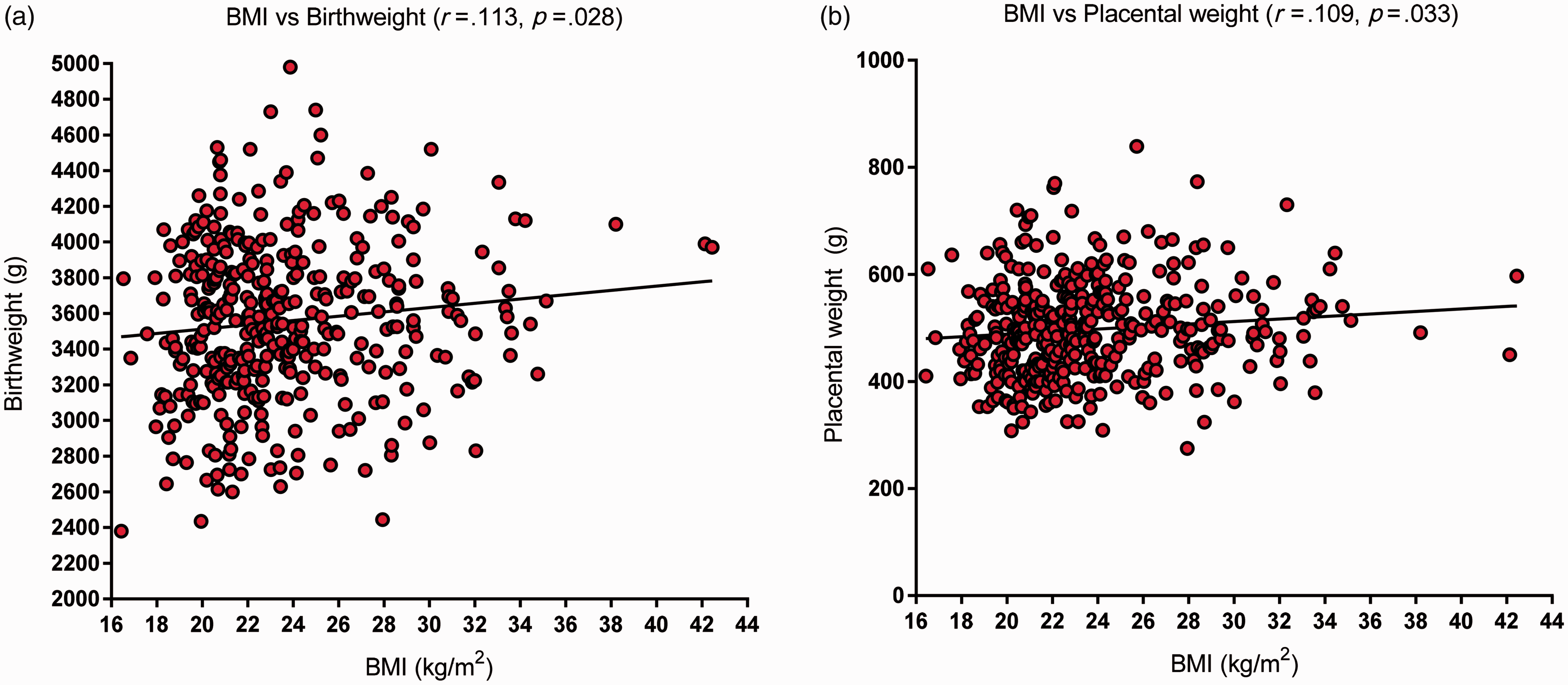
Discussion
This study shows the findings of prospective and systematic assessment of placental pathology in uncomplicated term pregnancies in a low-risk obstetric care setting, in association with prepregnancy BMI. We found that women with increasing BMI deliver placentas of a higher weight and babies with a higher birth weight. Despite the fact that these were all uncomplicated pregnancies with spontaneous vaginal delivery, we found that prepregnancy BMI was associated with characteristics of specific placental pathology, that is, more high-grade chronic villitis, more accelerated villous maturation, and less SGA placentas. We also found a substantial effect of parity on maternal, placental, and neonatal weights.
The relationship between higher BMI and adverse perinatal events is established, but the role of the placenta in mediating these complications is not entirely clear. 1 Evidence shows that women with a higher BMI deliver babies with a higher birth weight and heavier placentas.22–24 Similar to previous reports, high BMI appears to affect placental weight more than the effect on neonatal birthweight. 22 It has been well established that restrictive dietary behavior is correlated to a lower placental weight, without necessarily decreasing neonatal birth weight. 25 How the placenta responds to higher amounts of lipids, glucose, and other metabolic factors is not clear. Placental metabolism is thought to increase and lipid induced inflammatory changes take place. Consequences of these effects are unknown but are thought to affect the future health of the fetus by altering the immune response.7,26,27 Suboptimal maternal nutrition (either over or under) as well as abnormal placental weight (both high and low) have been shown to increase the risk of health problems in the adult offspring, including adult cardiovascular and metabolic morbidity.7,28,29 We found a significant correlation between BMI and parity. Parity was also correlated with higher placental and fetal birth weight. Increase in BMI is associated with parity and shows an independently higher risk of pregnancy-related complications irrespective of being overweight or obese. A higher BMI is nonetheless related to higher risk of pregnancy complications irrespective of parity. 30
Although numbers were relatively low, we found more chronic villitis present with increasing BMI. Previously published studies have shown obese women to present chronic higher levels of pro-inflammatory cytokines.12,31 This chronic pro-inflammatory state is thought to extend to in utero life and therefore shows signs in the placenta. 7 A recent study by Leon-Garcia et al. also reported more chronic villitis within placentas from obese mothers, with specific differences when women delivered a girl or a boy. When they corrected for specific maternal variables (ie, hypertensive disorders and delivery by caesarean section), the relationship with chronic villitis remained intact showing a robust association between this placenta characteristic and obesity. 15 This leads us to believe that even though our groups may have been smaller, the results remain relevant due to the uncomplicated nature of the group. Although low-grade villitis is not an uncommon finding in normal healthy placentas, high-grade villitis has a significant relation to FGR, neurodevelopmental impairment, fetal demise, and a chance of (increasingly severe) recurrence.32–35 Interestingly, about half of women who show recurrent placental chronic villitis are obese. 34 In a study in women who delivered SGA babies, increased BMI was related to increased presence of villitis and its pathological severity. 36 In our group, 3 of 4 (75%) women with high-grade villitis had placental weight below the 10th percentile (1 with normal BMI and 2 in the obese group) with 1 patient delivering a baby with low birth weight (normal BMI). Fetoplacental weight ratios in these pregnancies were high (above the 90th percentile in 3 patients with villitis) and therefore are thought to be highly effective placentas, producing babies with a normal weight despite chronic villitis. 24 Leon-Garcia et al. speculate that chronic villitis may play a role in downsizing placentas and babies that were destined to be large in women with obesity as a counter mechanism to obstetrical risks associated with LGA babies (ie, obstructed labor, dystocia). 15 The clinical relevance of chronic villitis and its relation to high BMI and/or placental metabolism, however, remains unclear and deserves further research with attention to its association with adverse pregnancy outcome.7,35 Even though we did not find a statistical difference, other studies reported conflicting results on inflammatory lesions of both maternal and fetal origin found in the placenta of obese women.13,14 The different findings among these studies or the lack of significant difference within groups is perhaps clarified by the high background inflammatory lesions in women with uncomplicated pregnancies and the inclusion of both healthy and complicated pregnancy in these cohorts.13,14
Besides chronic villitis, we found more accelerated and delayed villous maturation in the obese and overweight group. Accelerated villous maturation is a common pattern that can be seen with maternal vascular under perfusion and it may be present when the baby is growing faster than the placentas capacity. 20 This finding was not present throughout the groups, possibly due to the small number of obese patients and the uncomplicated pregnancy and history of the women in this study. Delayed villous maturation has been previously associated with both GDM and pregestational diabetes mellitus.37,38 None of the women in this cohort were diagnosed with GDM, but it is possible that these women were underdiagnosed in clinical practice and their placental pathology showed signs of glucose regulatory problems.
Strengths and Limitations
Including only healthy uncomplicated pregnancy with unassisted delivery resulted in a relatively small group of obese women. This may be seen as a limitation to ascertain statistical significance. In other studies on this subject, almost half of the obese patients investigated either had (gestational) hypertension or were delivered by caesarean section.13,15 As many obese women are at the risk of pregnancy complications, we did not include these patients to explore the role of obesity on placental pathology without interaction through pregnancy disorders that have an established association with placental pathology. As we were not able to find information on prepregnancy BMI in all patients from the original study, we were only able to study a part of this group. The pregnancy characteristics in the selected study group were similar to the ones we had to exclude due to missing data on maternal BMI and therefore show relevant and unbiased outcomes that can be extrapolated to the general uncomplicated obstetric population. The self-reported nature of prepregnancy weight and height has been shown not to be an issue when categorizing women into BMI groups. 39 A strength of this study is that all placental examinations were performed by 1 specialized pathologist and systematically analyzed by the new Amsterdam criteria. 20 Prospective collection of all patients eligible for the study in a low-risk setting is another strong point. We believe that the study therefore gives rise to the idea that obesity may affect placental function not only in high-risk, or complicated, pregnancies but also in low-risk uneventful cases. Other limitations of the study include unanswered questions regarding the role of socioeconomic factors and ethnicity (as this was a relatively homogenous cohort), which may play an additional role in driving maternal BMI, and other potential residual confounders and/or mediators.
Conclusion
Prepregnancy BMI is significantly correlated with higher placental weight and a higher birth weight of the baby. Even though we studied a group of healthy and uncomplicated pregnancies, specific placental pathology (ie, chronic villitis and difference in villous maturation) was associated with a higher BMI. With obesity being a growing health issue among women of childbearing age, the risk of adverse pregnancy-related events for both mother and child increases. Further research is needed to evaluate these changes in view of later-life health of infants born to obese mothers.
Supplemental Material
Supplemental material for Association of Maternal Prepregnancy Body Mass Index With Placental Histopathological Characteristics in Uncomplicated Term Pregnancies
Supplemental material for Association of Maternal Prepregnancy Body Mass Index With Placental Histopathological Characteristics in Uncomplicated Term Pregnancies by Laura Brouwers, Arie Franx, Tatjana E Vogelvang, Michiel L Houben, Bas B van Rijn and Peter GJ Nikkels in Pediatric and Developmental Pathology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.