
Abstract
Background:
We describe a novel extracorporeal knotting approach (ECKA) that enables secure mesh fixation via extracorporeal suture manipulation, anchoring the mesh firmly within the abdominal cavity.
Methods:
A retrospective analysis was conducted on 17 patients (14 males, 3 females) who underwent laparoscopic herniorrhaphy with mesh fixation using the ECKA technique. Key parameters included patient demographics, method of hernia repair (totally extraperitoneal [TEP] or transabdominal preperitoneal [TAPP]), laterality, and operative duration. Hernias were classified by procedure, with each side analyzed independently.
Results:
From April 2024 to July 2025, a total of 21 hernia procedures were performed on 17 patients using the ECKA technique. The average patient age was 70.3 years (range: 47.1–88.5 years), with a mean body weight of 65.9 kg. Of the hernia types, 15 were direct, 3 were indirect, and 3 were mixed. Laterality distribution was as follows: right-sided (n = 6), left-sided (n = 7), and bilateral (n = 4). Nine procedures utilized the TAPP approach, while 12 were performed using the TEP approach. The average operative time was 88.4 minutes (range: 60.4–145.4 minutes). Postoperative analgesia consisted of diclofenac sodium administered three times daily for three days. No recurrences were observed during a mean follow-up period of 10.3 months (range: 2–17 months).
Conclusions:
The ECKA technique provides a reproducible, minimally invasive solution for fixing mesh in direct, indirect, and combined hernias via either TEP or TAPP approaches. Its extracorporeal knotting system streamlines mesh fixation, ensures consistent clinical outcomes, and enhances operative efficiency across various hernia configurations.
Background
Innovations in laparoscopic inguinal hernia repair increasingly favor techniques that minimize tissue trauma and reduce dependence on costly fixation devices. We developed a novel method—ECKA (extracorporeal knotting approach)—which enables mesh fixation through extracorporeal suture manipulation, securely anchoring the mesh within the abdominal cavity.
Methods
This study was approved by the Ethical Review Board of Chang Gung Memorial Hospital (No. 202501042B0). A retrospective analysis was conducted on 17 patients (14 males, 3 females) who underwent laparoscopic herniorrhaphy with mesh fixation using the ECKA technique (Fig. 1). All operations were performed by a single surgeon (S.H.W.). Key parameters included patient demographics, method of hernia repair (totally extraperitoneal [TEP] or transabdominal preperitoneal [TAPP]), laterality, intraoperative blood loss, and operative duration. Hernias were classified by procedure, with each side analyzed independently. Operative time was measured from skin incision to closure.
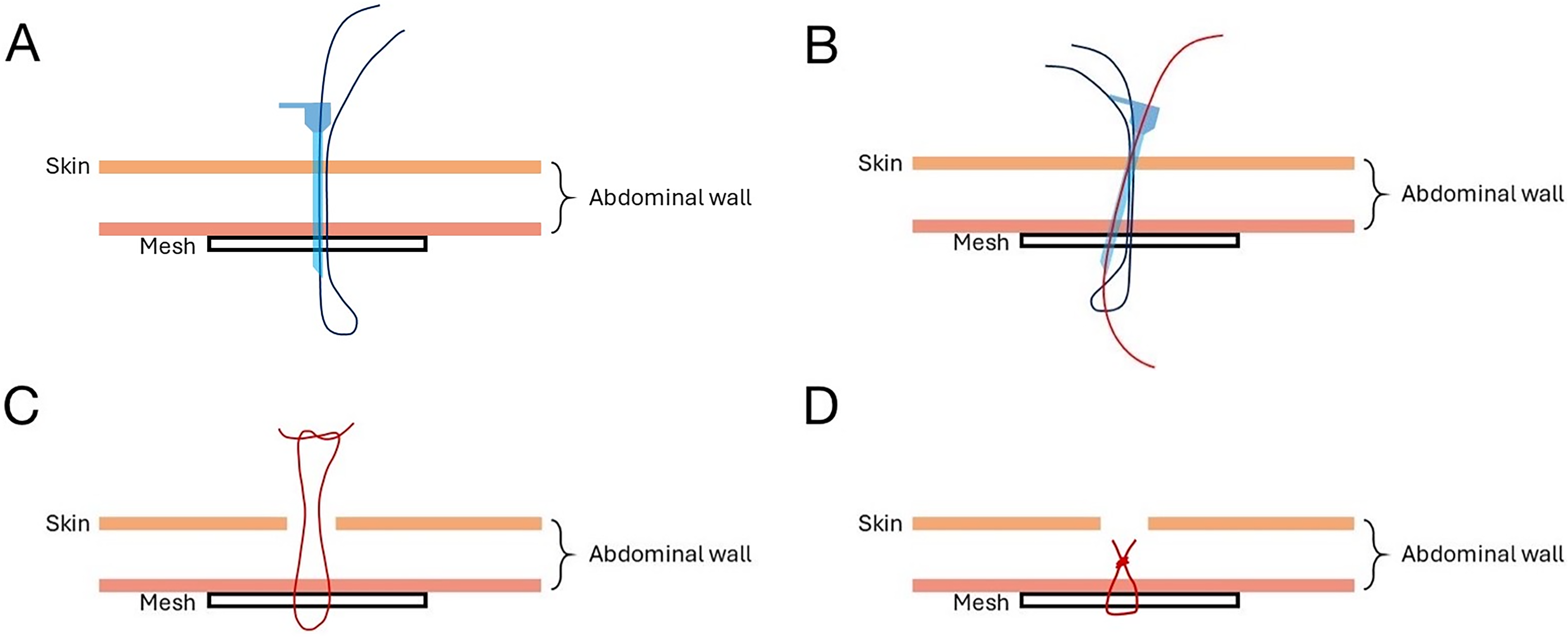
Procedures of the ECKA.
Results
From April 2024 to July 2025, a total of 21 hernia procedures were performed on 17 patients using the ECKA technique. The average patient age was 70.3 years (range: 47.1–88.5 years), with a mean body weight of 65.9 kg and a body mass index of 24.3.
Common comorbidities included hypertension (n = 4), cardiovascular disease (n = 3), and liver disease (n = 3). Recognized risk factors for hernia included physical exertion (n = 2), voiding difficulty due to benign prostatic hyperplasia (n = 1), and elevated intra-abdominal pressure caused by constipation or ascites (n = 2).
Of the hernia types, 15 were direct, 3 were indirect, and 3 were mixed. Laterality distribution was as follows: right-sided (n = 6), left-sided (n = 7), and bilateral (n = 4).
Nine procedures utilized the TAPP approach, while 12 were performed using the TEP approach. Lightweight meshes (10 × 12 cm, B. Braun) were used in all patients (Figs. 2 and 3).
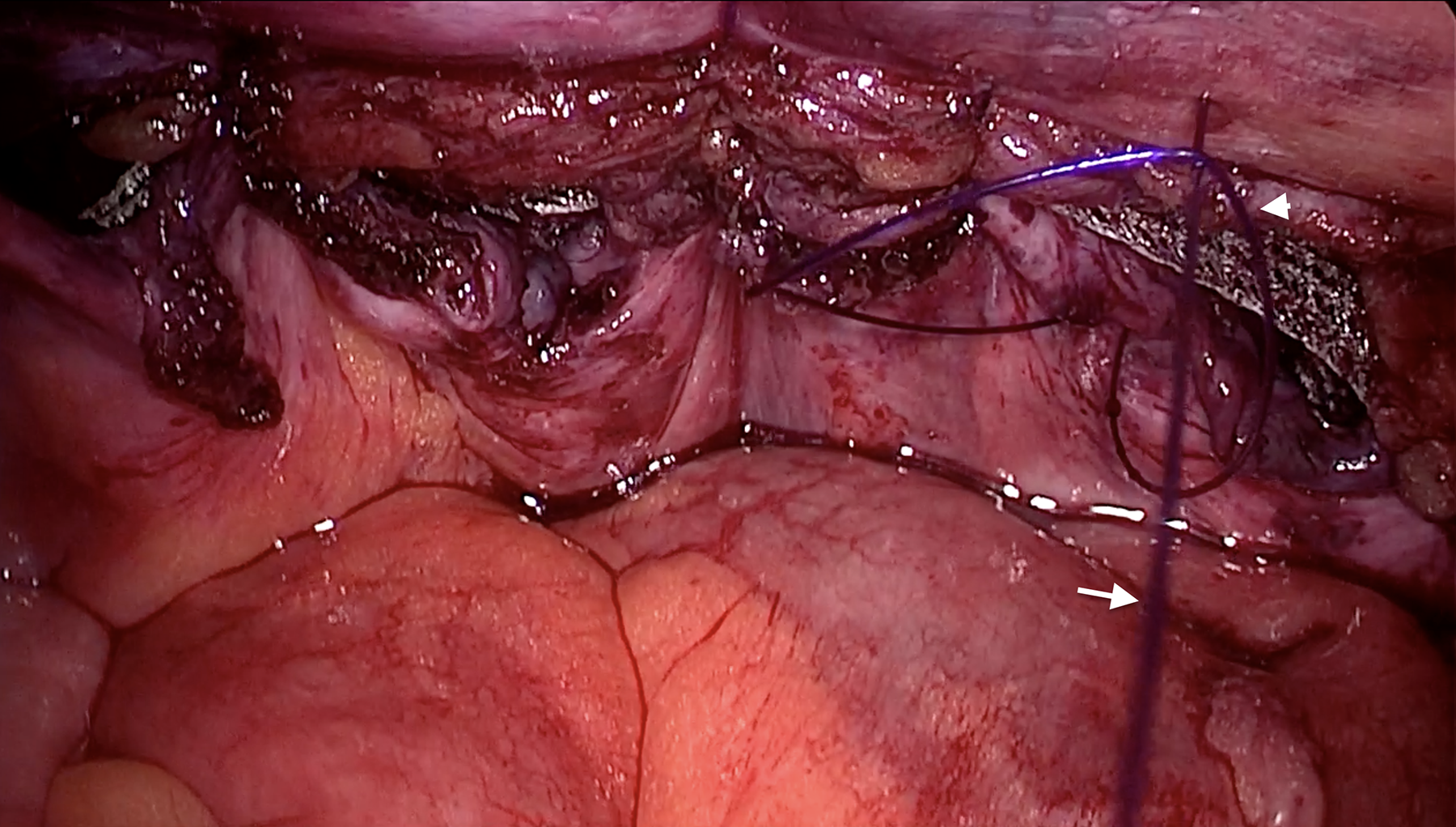
Mesh fixation including the peritoneum closure during the TAPP. The right most stitch showed a second 2-0 PDS (white arrow) passing through the first suture loop (arrow head).
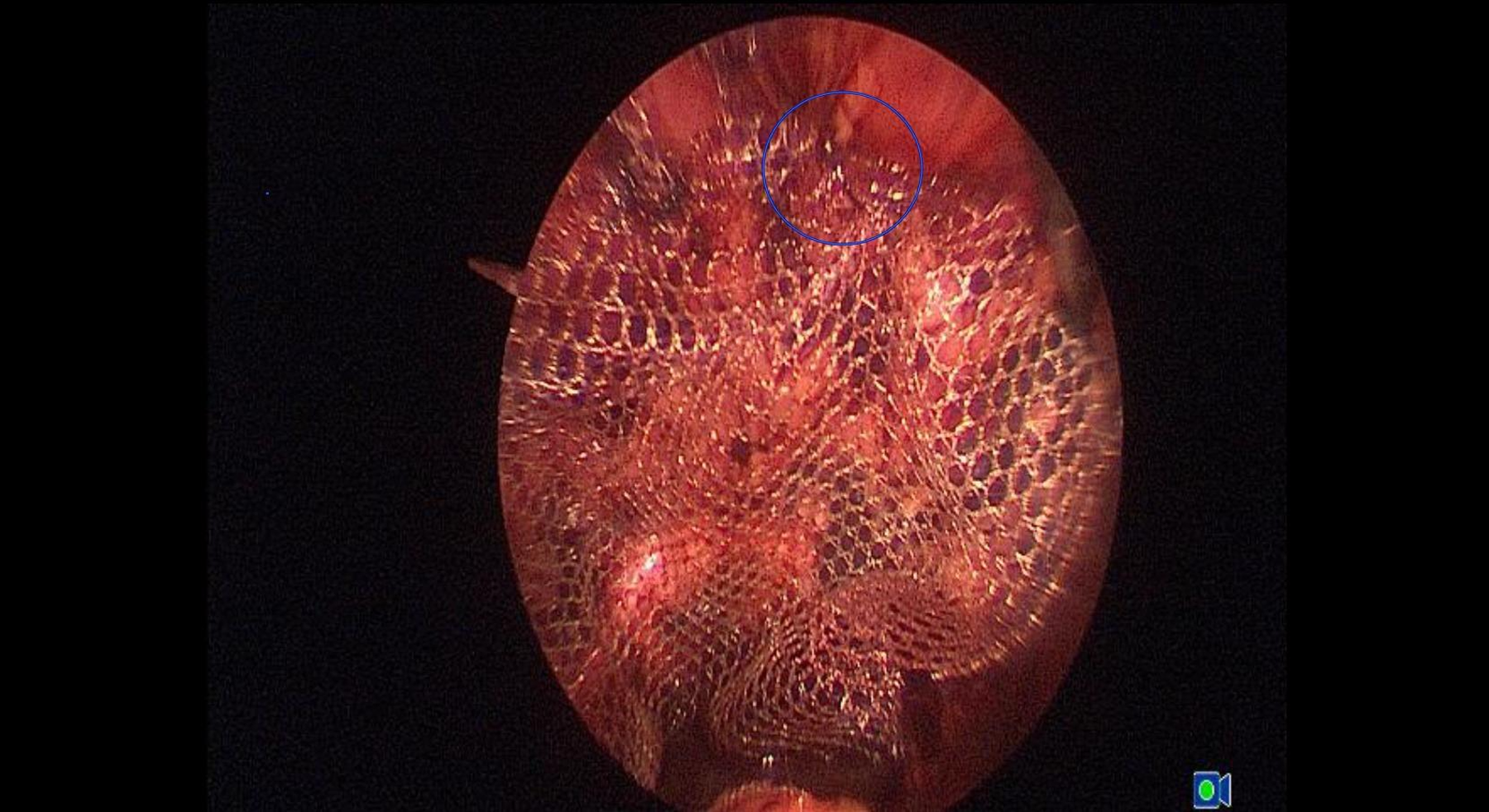
Mesh fixation using the ECKA technique during the TEP.
The average operative time was 88.4 minutes (range: 60.4–145.4 minutes), and the mean intraoperative blood loss was 17.8 ± 14.6 mL. Postoperative analgesia consisted of diclofenac sodium administered three times daily for 3 days. All puncture sites healed with minimal or no visible scarring, and none of the patients required additional pain medication 1 week after surgery.
No recurrences were observed during a mean follow-up period of 10.3 months (range: 2–17 months).
Discussion
While the necessity of mesh fixation in laparo-endoscopic hernia repair remains a topic of ongoing debate, it is generally recommended in cases of medial or combined hernias.1–3 Suturing the anterior abdominal wall during laparoscopic/endoscopic procedures is technically more challenging than in other intraabdominal surgeries. This difficulty arises from the fact that the suture sites typically align with the working-port locations, complicating instrument maneuverability.
Several traumatic and atraumatic devices and materials have been developed to assist with mesh fixation. However, postoperative acute pain and recurrence rates must still be closely monitored. 4 Moreover, the use of such advanced technologies increases the overall cost of hernia surgery. 5
Extracorporeal suturing has previously been reported in the literature. However, those techniques typically required specialized instruments such as suture passers or fascia closure devices to complete the procedure.6–8 The concept behind the ECKA technique was inspired by the percutaneous internal ring suture method used in repairing the adult indirect inguinal hernias. That method employed a simple 16G or 18G needle to close the internal ring with an extracorporeally tied suture.9,10
As Figure 1 showed, the ECKA technique presents a straightforward and versatile approach for accessing nearly any site along the anterior abdominal wall. Its simplicity lies in the use of a single instrument: the Gauge 18 needle, which can carry the suture and penetrate the abdominal wall. In both TEP and TAPP procedures, we routinely utilize 2-0 PDS sutures to secure the mesh—two positioned medial to the internal ring that via the same suprapubic puncture hole and another lateral to the internal ring. Sutures are loosely tied to minimize the risk of acute postoperative pain. Although long-term follow-up is still pending, we are optimistic that device-induced chronic pain will be minimal, as PDS sutures are bioabsorbable and expected to resolve within 6 months.
With a mean operative time of 88.4 minutes, the technique is on par with standard laparoscopic herniorrhaphy. The minimal intraoperative blood loss and lack of major complications further underscore its safety and efficacy. The consistent use of lightweight mesh likely contributed to reduced foreign body sensation and improved postoperative comfort. Standard analgesia with diclofenac for 3 days proved sufficient, with no patients requiring additional pain management beyond the first postoperative week. This supports ECKA’s minimally invasive profile and its potential to enhance recovery.
The ECKA technique has demonstrated promising results in laparoscopic inguinal hernia repairs. Outcomes include low postoperative pain, nearly invisible puncture marks, and no recurrences observed during short-term follow-up. Compared to conventional mesh fixation methods involving tacks, staples, or adhesives, ECKA offers a novel and cost-effective alternative by utilizing extracorporeal suturing for secure anchoring.
While early results are encouraging, this study is limited by its small sample size and retrospective design. To fully establish ECKA’s clinical value, long-term follow-up and randomized comparative trials with other fixation techniques will be essential.
Conclusion
The ECKA technique represents a reproducible, minimally invasive approach applicable to a broad spectrum of hernia types—including direct, indirect, and combined cases—utilizing either the TEP or TAPP method. Its extracorporeal knotting system streamlines mesh fixation, delivering consistent clinical outcomes and demonstrating operative efficiency regardless of underlying pathology or hernia configuration.
Footnotes
Acknowledgments
This study is partly supported by the Grant CMRPG6P0021 and NSTC 114-2823-8-182A-001–from Shih-Hsien Wang. CORPG6M0181, NMRPG6P0101, CMRPG6N0221 from Dong-Ru Ho. CMRPG6M0381, CMRPG6L0391 from Ju-Bei Yen.
Disclosures
S.‐H.W., J.-B.Y., C.-C.C., C.-M.Y., H.-C.Y., and D.-R.H. have no conflicts of interest or financial ties to disclose.