
Abstract
Background:
The sudden emergence of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and scarcity of the accurate information especially in the initial phase of the struggle presented a series of challenges to health systems.
Objective:
To evaluate the changes in poisoning cases regarding distribution, types, and characteristics for better framing and planning of the role of our field in responding to pandemics.
Methods:
Study of telephone consultation calls and toxicology analysis records of poisoning cases referred to the Dammam Poison Control Center in Saudi Arabia during the first half of 2020. Their distribution according to frequencies, causes, and other characteristics was compared to the first half of 2019.
Results:
Analysis of telephone consultation calls revealed that the proportion of exposure to disinfectants and hand sanitizers during first half of 2020 increased to 20.4% (n = 496) and 3.4% (n = 83), respectively, compared to 9.8% (n = 215) and 0.4% (n = 10) for surface disinfectants and hand sanitizers, respectively, during the first half of 2019. In 2020, exposure to disinfectants and hand sanitizers dominated in preschool children (0-5 years). The total number of cases suspected for drugs/drugs of abuse overdose during the first 6 months of 2020 (n = 783) showed a significant decrease (P < 0.001) compared to the first 6 months of 2019 (n = 1086).
Conclusion:
The increased availability and use of disinfectants and sanitizers significantly increased the risk of poisoning, especially in preschool-aged children. Public health education for prevention of such home exposures is urgently needed to avoid unnecessary emergency medical system use in such critical time.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic, caused by the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has radically changed the world over the past months and as of June 16, 2020 had affected over 8,250,000 people in 215 countries and killed more than 444,000 people worldwide.1,2 The World Health Organization (WHO) declared COVID-19 a pandemic on March 11, 2020. 3 In light of spreading infection and in attempts to control the pandemic, several containment measures were adopted by many countries, as in Kingdom of Saudi Arabia.4,5 A top priority of these measures was the prevention of COVID-19 infection in households including regular use of biocidal agents, more specifically surface disinfectants and hand sanitizers. 6 Medical toxicology and infectious diseases are not specialties traditionally related to each other; however, pandemics have a way of changing convention. As medical toxicologists, we serve as a resource of knowledge for our health care colleagues and the public.
The sudden emergence of the SARS-CoV-2 and scarcity of the accurate information about its characteristics and presence of a lot of contradictory information especially in the initial phase of the struggle build up a series of challenges to health systems. In this era, the Dammam Poison Control Center (DPCC) was unexpectedly involved in the COVID-19 outbreak.
One of the biggest challenges is providing our services 24 hours/day/week as a toxicology laboratory and drug/poison information center even during the periods of quarantine and lockdown. Moreover, the processing and evaluation of biological samples of poisoned patients in addition to answering the public and medical calls in these pandemic scenarios while maintaining high quality standards of the work performed and ensuring safe work environment for laboratory staff were among the challenges we faced.
The intent of this article is to introduce our experience regarding toxicology practice in the DPCC during COVID-19 pandemic and evaluate the changes in types and characteristics of poisoning/exposure cases in the first half of 2020 compared to the first half of 2019.
Methods
The study was conducted by examination of telephone consultation calls and samples of intoxicated patients referred to DPCC (Eastern Province, Saudi Arabia) from January 1, 2020, to June 30, 2020. Their distribution regarding frequencies, pattern of poisoning, causes, and other characteristics was compared to the same period of 2019.
Statistical Analysis
Data were coded and entered using the statistical package for the Social Sciences (SPSS) version 26 (IBM Corp). Data were summarized using frequency (count) and relative frequency (percentage) for categorical data. For comparing categorical data, chi-square test was performed. Exact test was used instead when the expected frequency is less than 5. 7 P values less than 0.05 were considered statistically significant.
Results
Results of this study showed that a small percentage of telephone consultations in both years were concerned with disinfectant and hand sanitizer exposures. These exposures represented 9.8% (n = 215) and 0.4% (n = 10) out of the total consultation calls (n = 2,300) for surface disinfectants and hand sanitizers, respectively, during the first half of 2019. While the number of all consultations, 2,300 in all, did not increase substantially over the first half of 2020 (n = 2,431), there were changes in the types of exposures. Most noteworthy is that the proportion of those involving disinfectants and hand sanitizers significantly increased to 20.4% (n = 496) and 3.4% (n = 83), respectively (Table 1). Differences were highly significant <0.001 for disinfectant and hand sanitizer exposure frequencies between the 2 studied periods of 2019 and 2020.
Distribution of the Total Consultation Calls in the First Half of 2020 Compared to the First Half of 2019.

a Significant at P value < 0.05.
The active ingredients in surface disinfectant products were provided in 438 cases (88.3%). The most common was sodium hypochlorite in concentrations <5%. For hand sanitizers, trade names were provided in 65 cases (78.3%), and according to material safety data sheets, the most common active ingredients were ethanol (concentration 70%-80%), isopropyl alcohol (concentration 10%-100%), and chlorhexidine (concentration <5%), which are all skin, eye, and mucous membrane irritants with a potential for systemic alcohol intoxication.
Monthly distribution (as shown in Figure 1) of the received calls revealed that pediatric disinfectant exposure calls were significantly higher in the first half of 2020 particularly in April and May compared to April and May of 2019. The rise started in March, continued to increasing in April, reached the peak in May, and then started to decline in June.
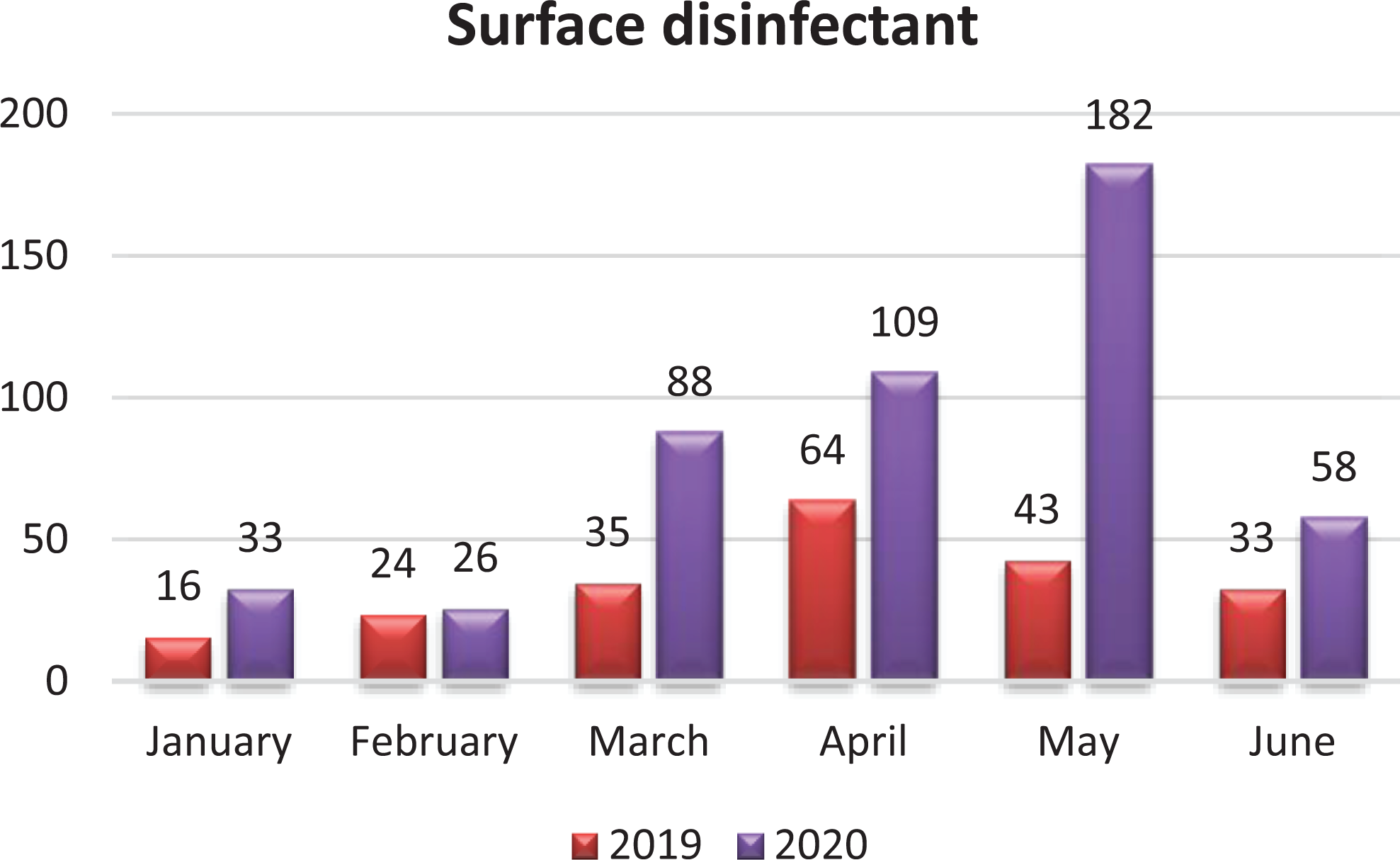
Monthly distribution of cases involving surface disinfectants reported to DPCC in the first half of 2020 and 2019.
Calls related to pediatric hand sanitizer exposures were significantly higher in the first half of 2020 particularly in March and April compared to March and April of 2019 (Figure 2).
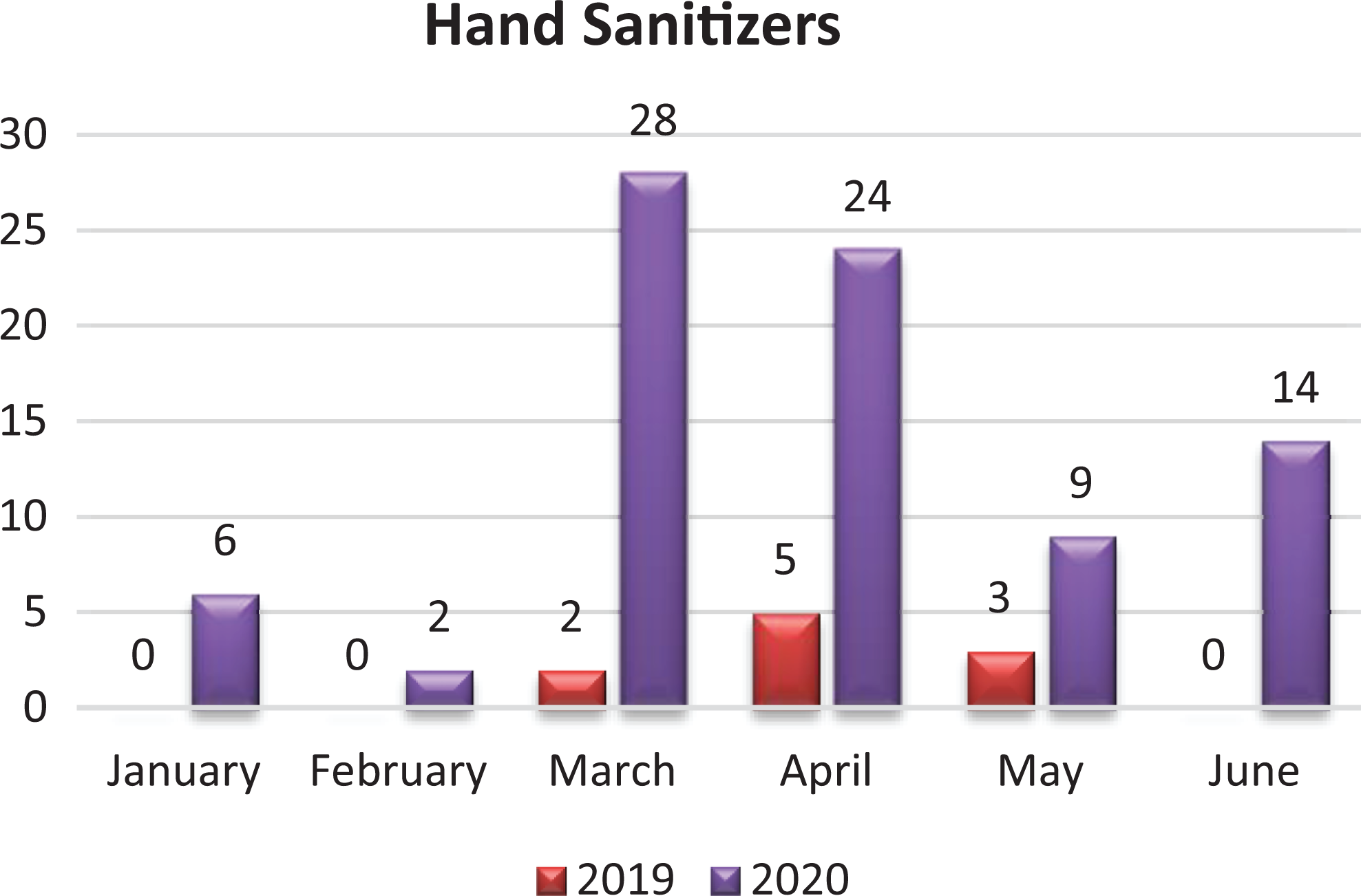
Monthly distribution of cases involving hand sanitizers reported to DPCC in the first half of 2020 and 2019.
In 2020, as shown in Table 2, exposures to disinfectants and hand sanitizers dominated in preschool-aged children (0-5 years), 85.8% and 79.5%, respectively. Exposure by ingestion was the main route in both disinfectant and hand sanitizer cases followed by inhalation in disinfectant exposure category. Accidental exposure was the prevalent in disinfectant and hand sanitizer cases (97.9% and 100%). Fortunately, most callers reported no or mild symptoms (gastrointestinal, respiratory, or eye irritation). Suspected and asymptomatic exposures were reported in 74% of those involving disinfectant exposure and 92% of those of hand sanitizer exposures.
Differences in the Pattern of Exposure to Surface Disinfectants and Hand Sanitizers From January 1 to June 30, 2020.
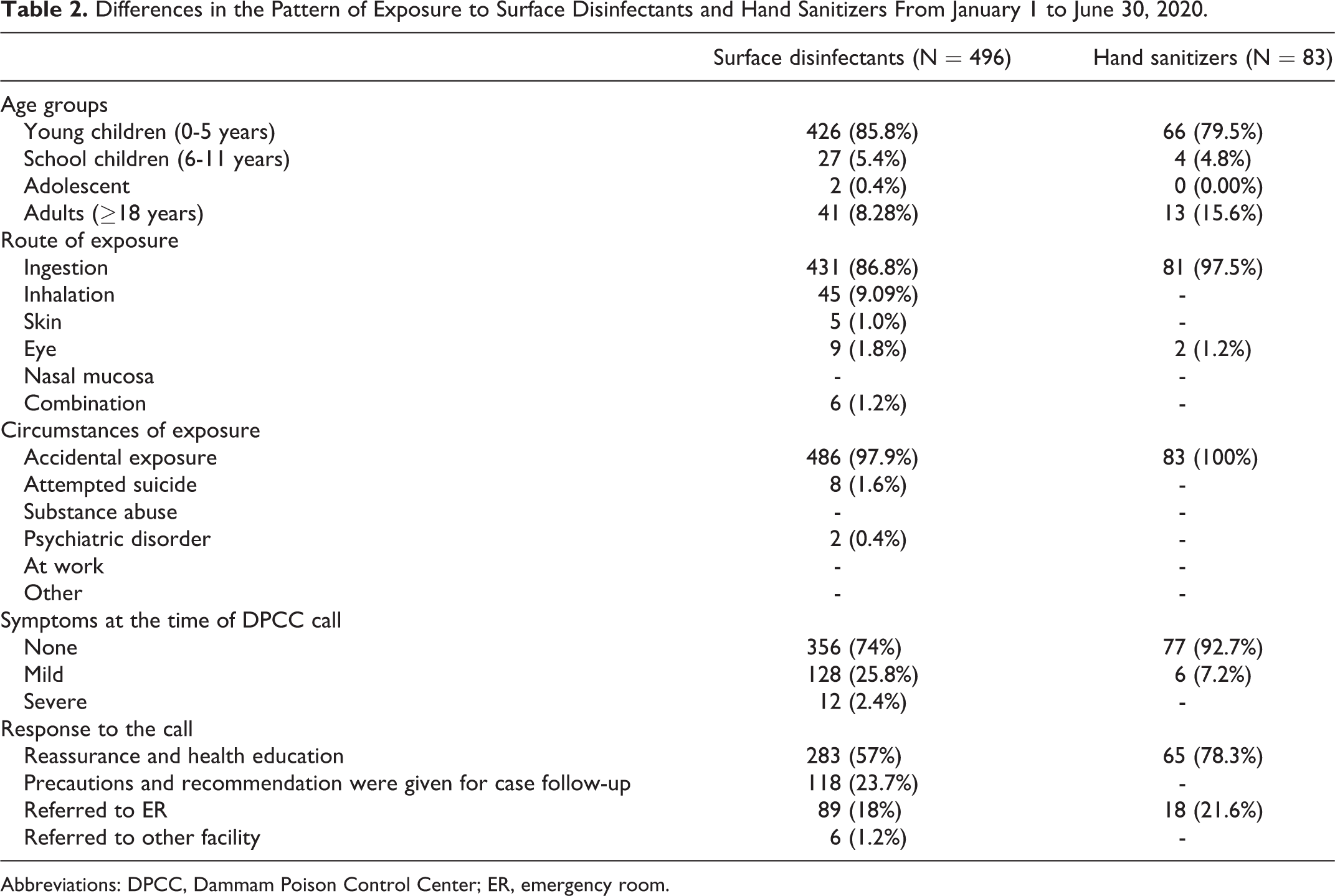
Abbreviations: DPCC, Dammam Poison Control Center; ER, emergency room.
Accordingly, most of the responses to telephone consultations were reassurance, giving special precautions and health education in 80.7% of disinfectant exposed cases and 78.3% in hand sanitizer exposed cases. Severe toxicity was recorded in (n = 12) due to inhalation of chlorine gas resulting from adding hypochlorite to hydrogen chloride and ammonium chlorides. Cases needing referral to emergency department (ED) for follow-up and management represented only 18% and 21.6% for disinfectant and hand sanitizer exposed cases, respectively.
Our results showed a notable decrease of the total number of cases suspected for drugs/drugs of abuse overdose and referred to DPCC for toxicology analysis. The total number during the first 6 months of 2020 was n = 783, of which 226 (46.1%) and 373 (66.2%) were related to drugs of abuse and other drug overdoses, respectively, compared to the first 6 months of 2019 (n =1,086), of which 308 (44.8%) and 564 (64.6%) were related to suspected drugs of abuse and other drug overdose, respectively, as shown in Table 3. There was a remarkable decrease of the total positive cases reported in 2020 (n = 563) compared to that of 2019 (n = 872). Distribution of the different detected drugs between the first half of 2020 compared to the first half of 2019 showed nonsignificant decrease as described in Table 4.
Distribution of Poisoning Cases During the 2 Studied Periods According to Their Analytical Results.

Distribution of Detected Drugs During the Studied Periods of 2019 and 2020.a
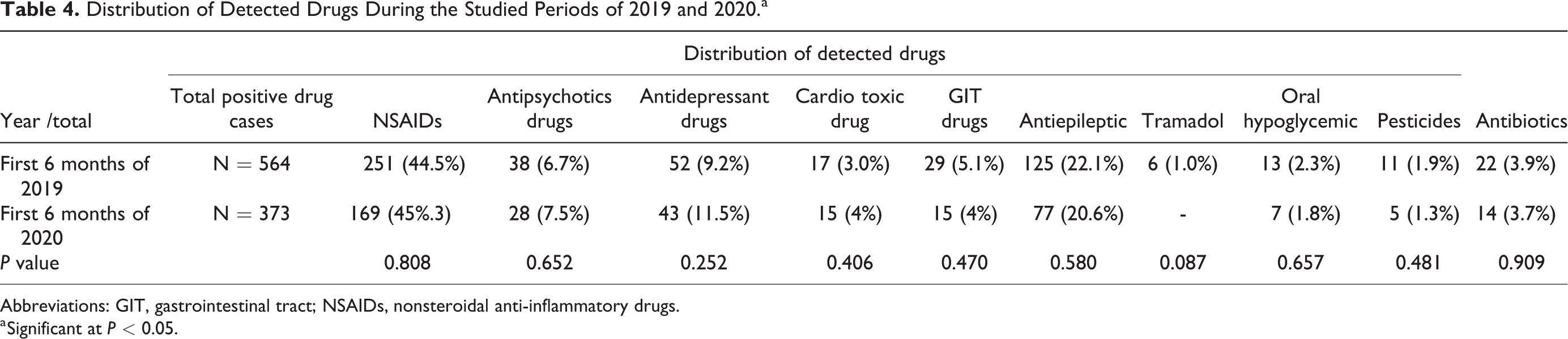
Abbreviations: GIT, gastrointestinal tract; NSAIDs, nonsteroidal anti-inflammatory drugs.
a Significant at P < 0.05.
There was a significant decrease (P < 0.008) of amphetamine positive cases over the 2 studied periods; also, there was a decrease in the positive cases of cannabis, opiates, and ethanol in the first 6 months of 2020 compared to the first 6 months of 2019 as shown in Figure 3.
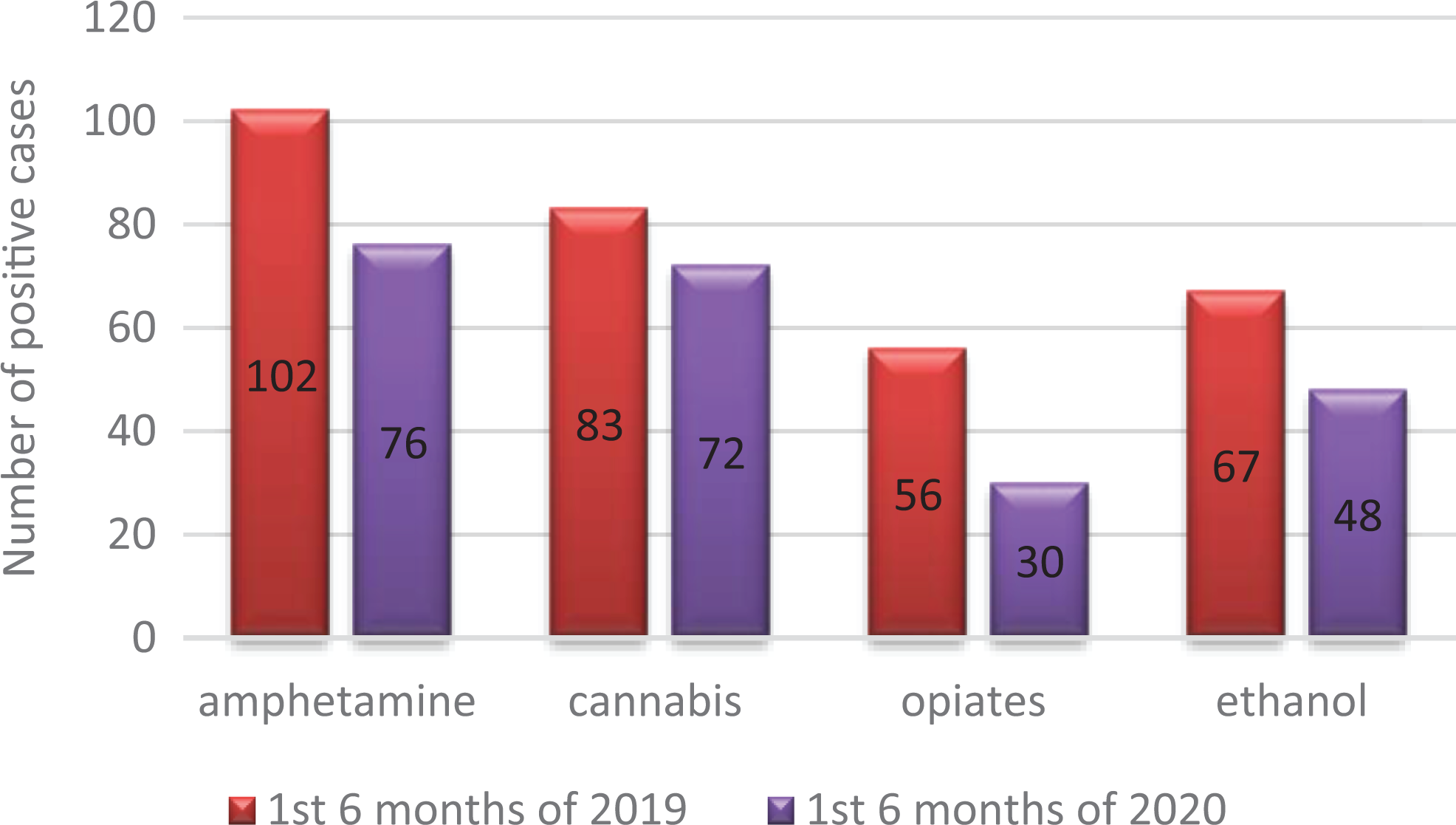
Distribution of the detected drugs of abuse in the first half of 2020 compared to the first half of 2019.
Discussion
To provide for a safe work environment and to minimize the risk of infection in the toxicology laboratory, extraordinary safety measures and guidelines were established by the DPCC through measures such as review of staffing and realigning staffing needs with the workload and working in shifts to reduce crowding and decrease the incidence of COVID-19 spread. Skin moisturizers and 70% ethanol dispensers were located at several points in the laboratory; there was a general encouragement for the usage of proper personal protective equipment and for practicing hand washing when moving from one location of the laboratory to another.
All specimens arriving to the laboratory were considered contaminated and thus having a biological threat to any laboratory personnel. The manipulation of biological samples including manual decapping, splitting, pipetting, diluting samples, and centrifuging were highly recommended to be performed with strict precautions. The higher incidence of aerosol formation and subsequent spreading of infection mandates the use of physical containment equipment such as a centrifuge with sealed rotors, eye and face protection, double gloves, and proper respirator mask. 8 All individuals who sent samples to DPCC were urged to mark the samples with a red stamp saying COVID-19 and document it on the electronic request.
Results of the recent study showed changes in the types and frequencies of the consultation calls reported by DPCC. There was a significant increase of the calls related to hand sanitizer exposure during the first half of 2020 especially in preschool children. The main route of exposure was ingestion. In accordance with these results, the American Association of Poison Control Centers reported 9,504 sanitizer exposure cases in children younger than 12 years in the first 5 months of 2020. 9 The US Centers for Diseases Control and Prevention (CDC) analyzed data reported to the National Poison Data System and stated that the major route of exposure to both alcohol and nonalcohol-based hand sanitizers was ingestion. The majority of intentional exposures to alcohol hand sanitizers occurred in children aged 6 to 12 years.10,11 Poisoning with hand sanitizers containing ethanol is a call for alert.12,13 Hand sanitizer use was suggested by WHO after the outbreak of COVID-19 in December 2019 as a preventive measure to control coronavirus spread. 14 The CDC guidelines specify that alcohol-based hand sanitizer products should contain 60% to 95% alcohol (≥ 60% ethanol or ≥ 70% isopropanol). According to the US Food and Drug Administration, which regulates alcohol-based hand sanitizers as over-the-counter drug, methanol (methyl alcohol) is not an acceptable ingredient.15,16
Alcohol-based hand sanitizers are easily accessible and effective for hand hygiene. 17 However, factors leading to increased exposure cases to hand sanitizers especially among children were revealed in our results. These included: (1) the lack of knowledge regarding use and storage of cleaners, disinfectants, and hand sanitizers; (2) attitudes about hand hygiene and disinfection; and (3) school closures with young children staying at home for long time periods of time with varying levels of supervision from adults and older children.18,19 Fortunately, methanol is banned from biocidal products in Saudi Arabia, so no cases with methanol toxicity were reported. 20
In line with other studies, pediatric disinfectant exposure cases were significantly higher in the first half of 2020, particularly in April and May 2020 compared to April and May 2019.21-23 Disproportionate anxiety about the coronavirus led to an increased incidence of exposure and toxicities, as a result of major behavior changes such as improper use of cleaning products for personal hygiene or food cleaning, repeated excessive house cleaning, and from the mixing of products. 24 Dammam Poison Control Center has a role in health education and establishment of guidelines for the public with basic advice for proper use, proper labeling, guidance on appropriate adult supervision while young children are near products, and proper storage for prevention of toxic effects caused by exposures to disinfectants and hand sanitizers, including advice to never mix products together.
The present study revealed that drug overdose cases showed a decrease in the total number and the frequency for each detected drug in the first half of 2020 compared to the first half of 2019. In line with our results, researchers in Europe noted a precipitous decline in the number of ingestions receded since the national and regional lockdowns were instituted.25,26 Other studies found that although suicide rates may have decreased temporarily, longer periods of social isolation could lead to the deterioration of the mental health of citizens, resulting in an increase in overdoses.27-29
Our results showed an overall decrease in cases of intoxication with alcohol and drugs of abuse. These could be attributed to the facts that alcohol and drugs of abuse are illegal and completely banned in Saudi Arabia, there was difficulty in getting imported supplies of abused drugs due to national and local lockdown, and fear of being infected in the emergency room. Also, there was the need to get an exit permission through electronic application from the ministry of interior during the lockdown and quarantine periods, which considered an issue for many patients who need health care after poisoning.
Other authors stated that patients with substance use disorders were already at a higher risk of suicide and overdose, and that they were disproportionately affected during the COVID-19 pandemic.27,30 This may have been due to the inability to access their abused substance or opioid agonist therapy during quarantine and lockdown periods.27,28 Also, many authors have estimated that the quarantine measures undertaken as public health protocols for disease and infection control during this current pandemic such as social distancing and stay-home instructions will inadvertently lead to worsened mental health and increased substance abuse for the general public.31,32
Conclusions
It is of fundamental importance to share the experiences and challenges experienced during the COVID-19 global crisis in different poison control centers to address our role during the pandemic in treatment of toxicities emerging from the use and misuse of approved and alternative therapies. Deciding which of these poisoned patients may stay at home will not only minimize ED visits and hospital admissions but will also restrict microbial transmission and provide a service to the overloaded medical system. Public health education about proper use, proper labeling, guidance on appropriate adult supervision, storage, and handling of products will help in decrease household poisonings, which is urgently needed to prevent unnecessary emergency medical system use in such critical time.
Footnotes
Authors’ Note
The required ethical approval was obtained from the institute ethics committee.
Author Contribution
Mahmoud, N. contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted the manuscript; and critically revised the manuscript. Al-Mazroua, M. contributed to conception and drafted the manuscript. Afify, M. contributed to design, contributed to acquisition and interpretation, and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.