
Abstract
The objective of this study was to evaluate male pubertal changes associated with environmental low-level lead (Pb) exposure. The study was conducted on 180 boys aged 15 years divided into 3 equal size groups: group 1 from El-Newayrat village, group 2 from Al-Shorafaa (0.5 and 10 km, respectively, from an industrialized area), and group 3 from Talla (25 km). Blood Pb levels (BLLs) were measured and pubertal changes evaluated by measurement of testicular volume (TV), and estimation of the follicle-stimulating hormone, luteinizing hormone, testosterone, estradiol, and prolactin. Blood Pb levels of children of El-Newayrat and Al-Shorafaa were significantly higher (6.38 [1.32] and 3.84 [0.79] μg/dL, respectively) than that of Talla children (1.85 [0.72]; P < 0.001), while height, weight, and TV were lower in boys in groups 1 and 2, compared to group 3. Genitalia and pubarche staging showed greatest retardation and marked bone growth delay in boys of group 1. Hormonal assays reported significant differences in boys of the industrialized areas when compared to that of Talla. Low-level Pb exposure in boys located near an industrial area was accompanied with altered male puberty indicators.
Introduction
Lead (Pb) is an important toxicant that can endanger humans’ health. 1 Many systems are well known to be susceptible to adverse effects of high Pb exposure, including the neurological, reproductive, renal, and hematological systems. Children are more sensitive than adults to such effects of Pb, and precautions should be taken to limit childhood exposure and keep blood Pb level (BLL) below the Centers for Disease Control and Prevention’s (CDC) reference concentration level of 5 μg/dL. 2 One of the most concerning observations associated with BLL is that of a decelerating dose–response curve for childhood Pb exposure and intellectual or academic abilities. 3 -5
Puberty, the period of transition from childhood to attainment of mature reproductive function, is characterized by accelerated growth, development of secondary sexual characteristics, and psychological changes. Activation of the hypothalamic–pituitary–gonadal axis initiates puberty. Although the precise mechanisms responsible for pubertal onset are not fully understood, body mass and nutritional status, 6 psychosocial health, genetic factors, and neuroendocrine inputs to the hypothalamus are all important determinants. 7
Many studies report a relationship between Pb exposure and diminished early childhood growth, 8 -11 but no studies provide data directly relevant to the question of whether BLL <10 μg/dL adversely affects male puberty in Minia governorate.
The objective of our study was to focus on the possible pubertal changes associated with environmental low-level Pb exposure in children living in villages at the East coast of the River Nile of Minia city, which are located adjacent to a heavily industrialized area.
Participants and Methods
Participants
The current study was a case–control study, conducted at the Minia University Hospitals during the period from January 1, 2013, to December 31, 2015. It included 180 male children aged 15 years (6 months) divided into 3 equal groups (60 children each): group 1 from El-Newayrat village (500 m from the industrial area), group 2 from Al-Shorafaa (10 km from the industrial area), and group 3 from Talla, a village located to the West of El-Minia city, 25 km away from Minia industrial area, as a control group (Figure 1). The choice of the villages was based on being nearly of the same level of nutrition, socioeconomic status, water sources, and being away from the traffic exposure. The industrialized zone includes the following heavy industries: battery manufacturing, chemical and hydrocarbon production. Ethical approval to perform the study was obtained from the Ethics Committee of the Minia School of Medicine, Minia University.
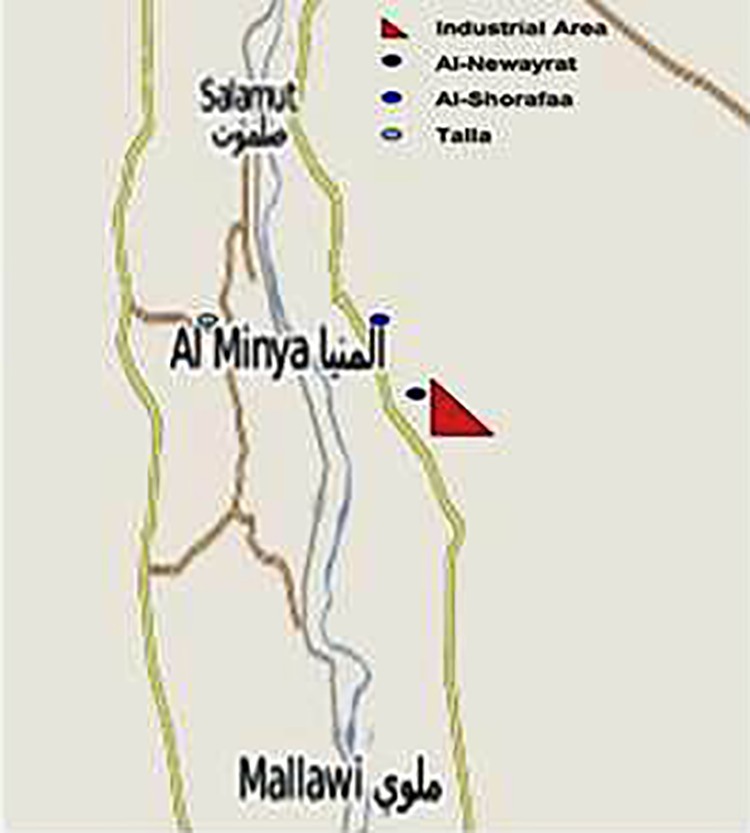
A map showing the locations of 3 villages and the industrial zone: El-Newayrat village (500 m from the industrial area), Al-Shorafaa (10 km from the industrial area), and Talla village (25 km away from Minia industrial area).
Inclusion Criteria
Male children around 15 years old seeking for medical advice in dermatology and andrology clinic for irrelevant complain (eg, itching) and living in the selected area for at least 4 years. All included children were chosen to have nearly the same nutrition, socioeconomic status, and water sources.
Exclusion Criteria
Children with BLL ≥10 μg/dL, children with mental retardation (MR) secondary to genetic and/or chromosomal disorders, children with family history of MR, children with neurological disorders, and/or systemic or debilitating diseases (eg malnutrition, diabetes mellitus).
Assessment Methods
Blood Pb level
Venous blood samples were collected using lead-free tubes containing EDTA. Samples were stored in the original tube at 4 C before being transferred to Minia Poisoning Control Center laboratory, Faculty of Medicine, Minia University. The time between receipt and analysis varied from 1 to 3 weeks. During which time, the specimens were stored refrigerated at 4°C. Lead concentration was determined by graphite furnace atomic absorption spectrometry (EXPRESS PLUS, Chiron Diagnostics, New York, USA). The detection limit was 1.0 µg/dL; measured BLL below the limit of detection were set to 0.5 for 14 (2.9%) of 481 boys.
Assessment of pubertal changes
An associate professor of andrology, with a nurse present, performed a standardized examination, including height, weight, and pubertal staging, without knowledge of the boys’ Pb levels.
Height in bare feet (to the nearest 0.1 cm) was measured using a stadiometer. Weight (to the nearest 0.1 kg) was measured with the boys in undergarments using a scale with moveable weights and level platform.
Pubertal status was staged from 1 to 5 by visual inspection and compared with published photographs according to internationally accepted criteria. 12 Pubarche (P, pubic hair stage) was determined by extent of terminal pubic hair growth. Genital staging (G) was assessed by genital size and maturity. Testicular volume (TV) was measured using a Prader orchidometer (Genentech, Inc, San Francisco, California), and stretched phallic length was measured to the nearest 1.0 mm using a firm ruler. Pubertal onset was defined in 2 ways: stage G2 or greater, or TV > 3 mL of either testis.
Bone development
An x-ray of the wrist was examined to assess actual bone age with the chronological age (15 years [6 months]). 13
Hormonal assay
Serum levels of luteinizing hormone (LH), follicle-stimulating hormone (FSH), free testosterone (Tf), estradiol (E2), and prolactin (PRL) were measured using radioimmunoassay. The reagent kits from Diagnostic Systems Laboratories Inc (Webster, Texas) were purchased from Trust Medical Co (Cairo, Egypt).
Venous samples were drawn at 8, half past 8, and 9
Statistical Analysis
Data were checked, coded, entered, and analyzed using SPSS (version 20 software). The results were expressed as mean (standard deviation [SD]) for quantitative data and number and percentage for qualitative data. Comparisons were done using the 1-way analysis of variance test and post hoc lease significant difference test for quantitative data, χ2 test for qualitative data. Statistical significance was set at P < .05.
Results
Results of the current study revealed that BLL of children of El-Newayrat and Al-Shorafaa were significantly higher (6.38 [1.32] and 3.84 [0.79] μg/dL, respectively) when compared to that of Talla children (1.85 [0.72]; P < 0.001; Figure 2A). Developmental assessment of the participants of the study revealed that height, weight, and TV were also significantly lower in the children of El-Newayrat than those of Al-Shorafaa, while the Talla children had the highest values (Figure 2B-D).
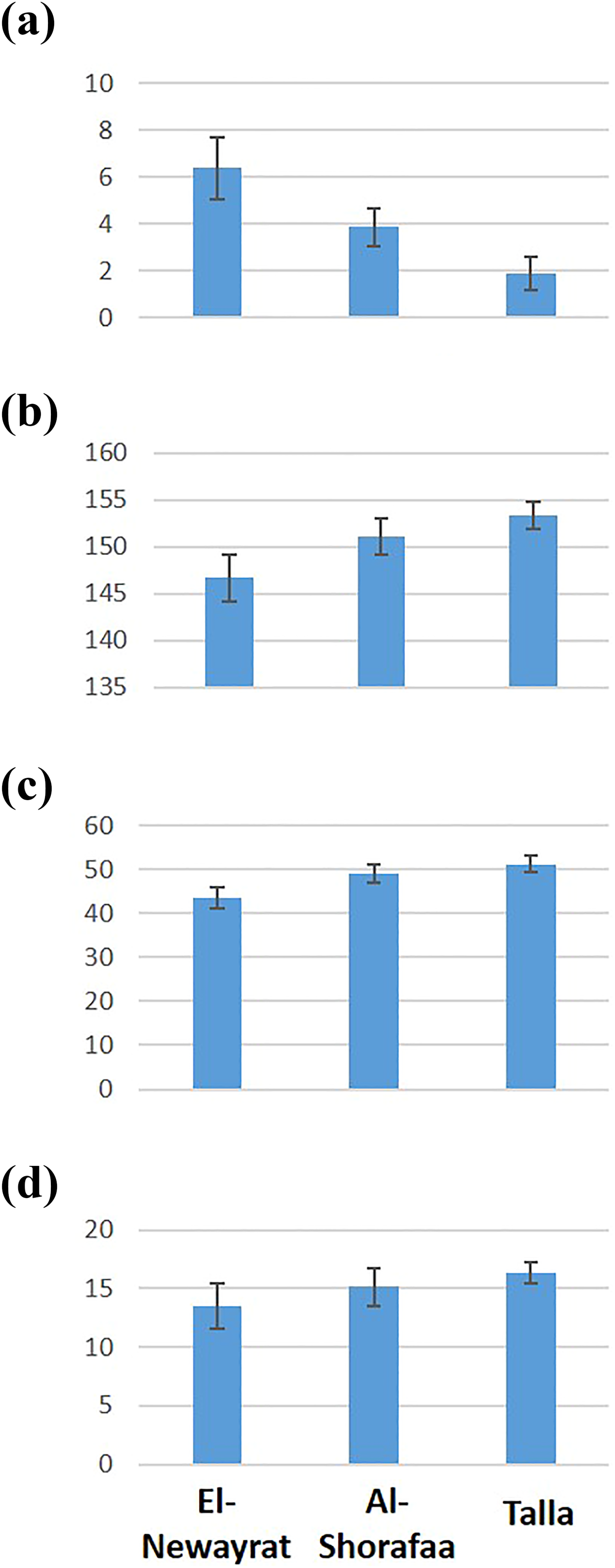
Developmental changes of the El-Newayrat, Al-Shorafaa, and Talla groups related to their (A) blood lead levels (BLLs), (B) height, (C) weight, and (D) testicular volume (mL). All values were significantly different (P < 0.001) when comparing each village.
Tanner’s staging of genitalia and pubarche showed significant retardation of external genitalia of the children of group 1 when compared to those of group 3 (Table 1).
Tanner’s Staging of the Genitalia of Different Villages.a
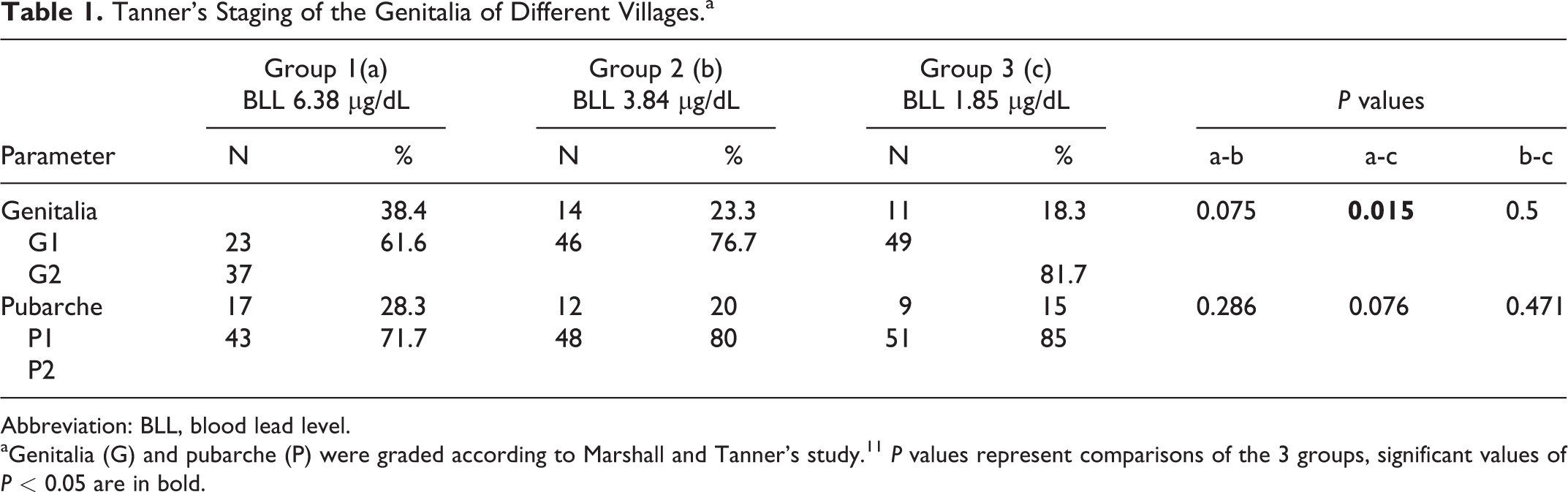
Abbreviation: BLL, blood lead level.
aGenitalia (G) and pubarche (P) were graded according to Marshall and Tanner’s study. 11 P values represent comparisons of the 3 groups, significant values of P < 0.05 are in bold.
Wrist X-rays of the participants of the present study also reported a marked bone growth delay of boys of the El-Newayrat village. It was found that the mean actual bone age was 12 to 13 years, while those of the other investigated groups were closer to the corresponding chronological age of the study cohort (Figure 3).
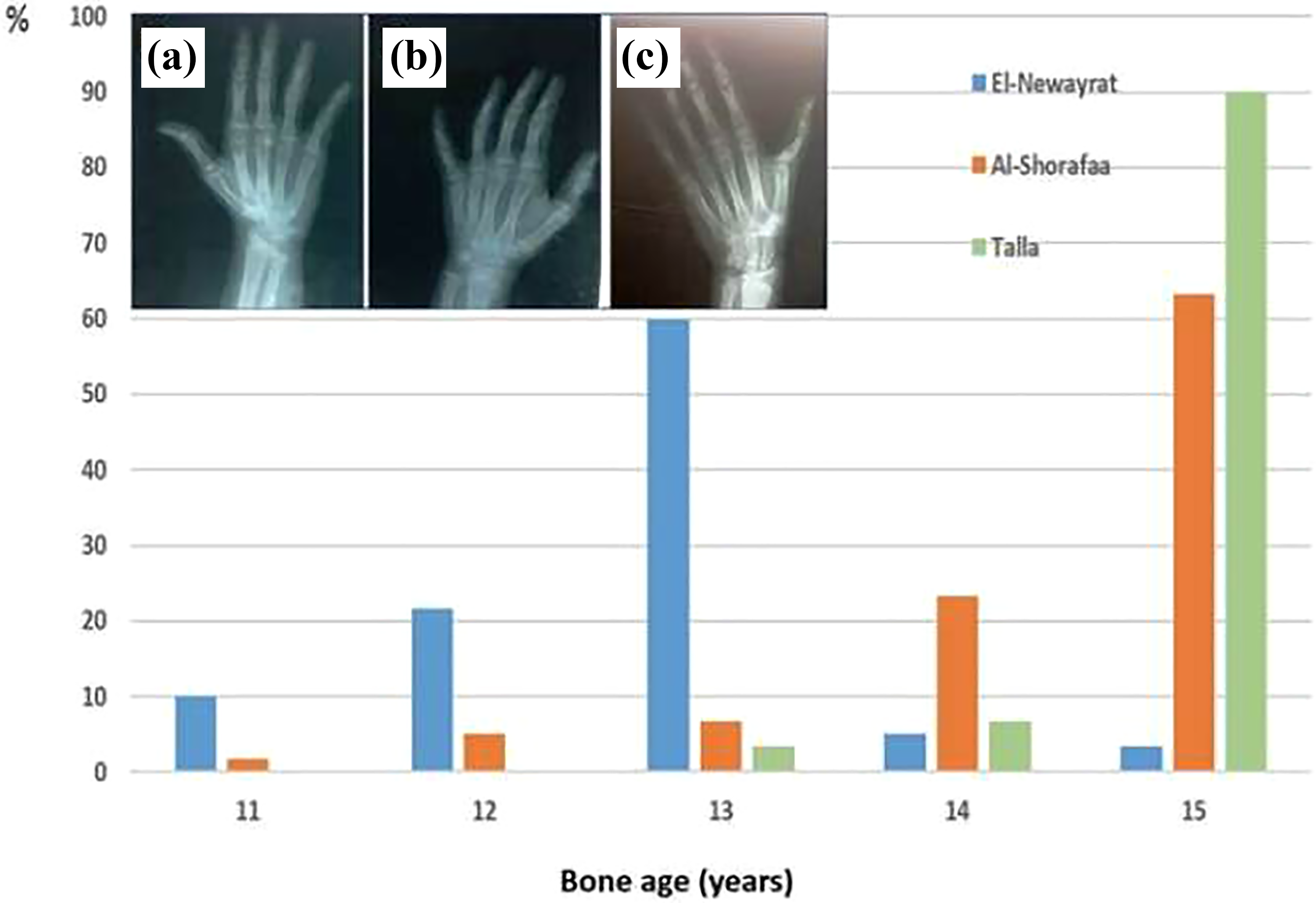
Actual bone age of the studied boys from the 3 different villages, El-Newayrat, Al-Shorafaa, and Talla, as assessed by plain X-ray of the wrist. The percentage of boys in each village is shown for each age group 11 to 15 years. Inset is an example of El-Newayrat boys wrist X-ray for (A) 11 years, (B) 12 years, and (C) 13 years. N = 60 for each village.
When assessing the results of the hormonal assays, we found a significant difference in the values of FSH, LH, and Tf in the children of group 1 followed by group 2 and the lowest levels in group 3 (Table 2). Moreover, it was found that there was a significant increase in the values of E2 and PRL in the same manner (Table 2).
Serum Hormone Values (mean [SD]) From Boys of the 3 Different Villages.a
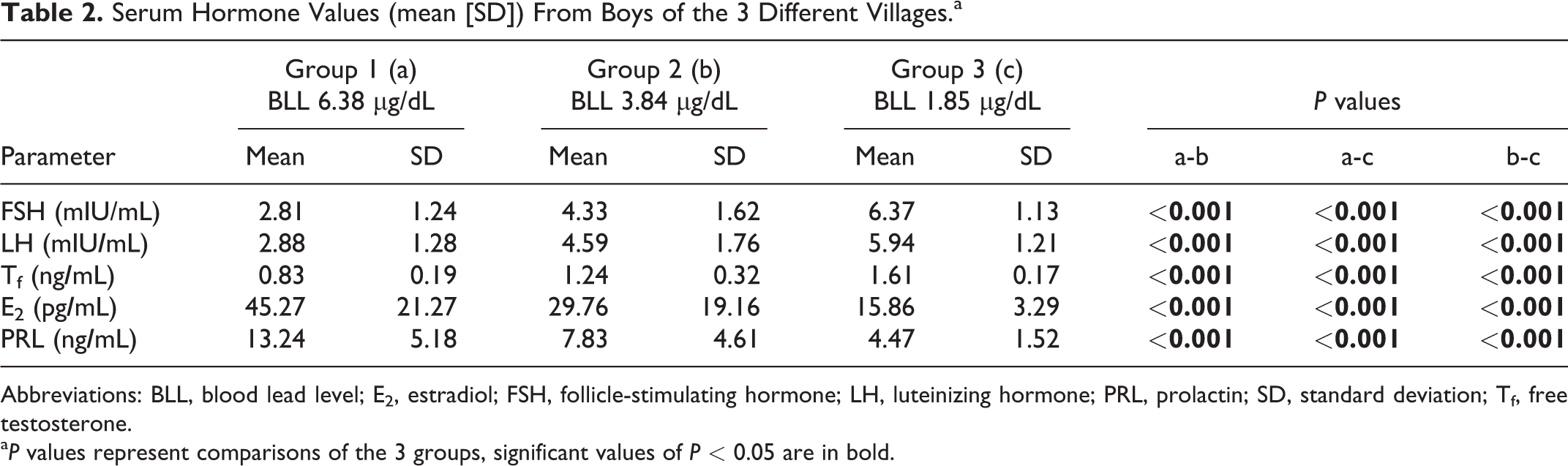
Abbreviations: BLL, blood lead level; E2, estradiol; FSH, follicle-stimulating hormone; LH, luteinizing hormone; PRL, prolactin; SD, standard deviation; Tf, free testosterone.
a P values represent comparisons of the 3 groups, significant values of P < 0.05 are in bold.
Finally, there was an inverse association between the BLL and all the measured parameters (height, weight, pubarche, etc), except with LH and E2, where the increased BLL was associated with a similar increase of both hormones.
Discussion
The transformation of a boy into an adult involves not only the increase in size, but also it involves the activation and maturation of many organs and systems. 15 However, the primary timing mechanism that initiates the activation and thus triggers puberty is unknown. 14
Delayed puberty is defined as lack of the initial signs of sexual maturation by an age that is more than 2 to 2.5 SD above the mean for the population (13 years of age in girls and 14.3 years of age in boys). 16
This study focused on the possible pubertal changes associated with environmental low-level Pb exposure in children living in villages at the East coast of the River Nile of Minia city, which is located near an industrialized area. It is of note that the distances of these 3 towns from the industrialized zones were in the order of El-Newayrat being adjacent, Al Shorafaa being near (10 km) to Talla being the furthest.
Estimating the BLL of children revealed that those of El-Newayrat and Al-Shorafaa were significantly increased when compared to that of Talla children and that their levels closely reflected the distances from the industrialized areas with El-Newayrat and Al-Shorafaa being 3.5 and 2.1 times more than the control area Talla. This clearly indicates that the industrialized zone impacts certain health parameters of the nearby population.
Regarding the developmental assessment of the participants of the study, the results revealed that height, weight, and TV were again significantly lower in the children of El-Newayrat than those of Al-Shorafaa when compared to the children of Talla. These findings are in accordance with Hauser et al, who reported that BLL was inversely associated with height, weight, and reduced odds of having entered G2. 17
The reported delayed growth development is further supported by the retarded skeletal growth that was reflected by measuring the bone age of the wrist by plain x-ray. The present study reported a marked bone growth delay of boys of El-Newayrat village. It has been found that the actual bone age was around 12 to 13 years, while those of the other investigated groups was around the corresponding chronological age. These data are in agreement with many other previous studies that reported significant negative associations between blood Pb concentration and stature and head circumference among children age 1 through 7 years 4 and suggested that even for low Pb exposure this metal may affect stature growth and gonadotropins levels. 10 In animal models, it was reported that chronic Pb exposure from gestation through puberty resulted in delayed sexual maturation of male rats measured by prostate weight and secondary sex organ development. 18
On the other hand, it has been found that the results of the present study reported a significant decrease in the values of FSH, LH, and Tf in the children of El-Newayrat followed by Al-Shorafaa when compared to that of Talla. Moreover, it has been found that there was a significant increase in the values of E2 and PRL in the same manner. These findings are in agreement with the data of a number of previous animal model studies. 19 -21 In these models, it was found that the signals within and between the hypothalamus and pituitary gland were disrupted by Pb exposure.
All of the children in this study were close to 15 years old, but the pubertal staging seems to be delayed when compared to the reference population. By this age, most boys start Tanner stage 5. Unfortunately, there are no available studies that assess pubertal staging among Egyptian children. This raises an urgent need to conduct a cross-sectional study that involves a representative sample of Egyptian children to evaluate if this phenomenon is unique to our particular investigation.
The exact mechanism(s) by which Pb can induce these effects was not the overall focus of this study. However, as puberty and activation of the hypothalamic–pituitary–gonadal system are strongly aligned the influence of the hypothalamic gonadotropin-releasing hormone, the gonadotropins LH and FSH, and the sex steroids estradiol or testosterone to coordinate the manifestations of puberty, both external (genital enlargement) and internal (testes) become critical. Any disparity of this fine balance would predictably impact the onset of puberty. It is clear from our results that this harmony has been disrupted.
Pubic hair develops independently of the activation of the hypothalamic–pituitary–gonadal pathways, largely through the effect of androgens secreted by the adrenal glands (adrenarche). 22 In boys, when puberty does not occur spontaneously or is delayed, no development of secondary sexual characteristics is observed. If pubic hair develops, this is usually due to the secretion of adrenal hormones and does not imply activation of the hypothalamic–pituitary–gonadal axis. The concentrations of the pituitary hormones LH and FSH are low when the disturbance has its origin in the hypothalamus or pituitary gland (hypogonadotropic hypogonadism); they are high when the cause is testicular failure (hypergonadotropic hypogonadism). In either case, the level of the gonadal hormone, estradiol or testosterone, is low. 23 According to these data and the results of the current study, it could be speculated that Pb may affect the male puberty at the hypothalamic level.
A limitation of this study is that we only examined Pb levels and no other toxicants. Given that the boys lived adjacent to these industrialized zones, other pollutants or combinations of other pollutants with Pb could be responsible for the delayed onset of puberty. A strength is that you could identify occupants of these areas accurately and that because they were children the study was not complicated by them having moved from different areas.
In brief, it could be concluded that low-level Pb exposure in children of the villages of the East coast of the River Nile of Minia city that is located adjacent to an industrialized area was accompanied with altered male puberty. We suggest that a larger multinational study to evaluate the extent of Pb toxicity is strongly advised so as to highlight Pb toxicity as a national health problem.
Footnotes
Author Contributions
Khalaf, M. contributed to conception and design, contributed to acquisition, analysis, and interpretation; drafted manuscript, and critically revised manuscript; Younis, R. contributed to design, contributed to acquisition, analysis, and interpretation, drafted manuscript, and critically revised manuscript; El-Fakahany, H. contributed to design, contributed to interpretation, drafted manuscript, and critically revised manuscript. All authors gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.