
Abstract
BLZ-100 is a single intravenous use, fluorescent imaging agent that labels tumor tissue to enable more complete and precise surgical resection. It is composed of a chlorotoxin peptide covalently bound to the near-infrared fluorophore indocyanine green. BLZ-100 is in clinical development for intraoperative visualization of human tumors. The nonclinical safety and pharmacokinetic (PK) profile of BLZ-100 was evaluated in mice, rats, canines, and nonhuman primates (NHP). Single bolus intravenous administration of BLZ-100 was well tolerated, and no adverse changes were observed in cardiovascular safety pharmacology, PK, and toxicology studies in rats and NHP. The single-dose no-observed-adverse-effect-levels (NOAELs) were 7 mg (28 mg/kg) in rats and 60 mg (20 mg/kg) in NHP, corresponding to peak concentration values of 89 400 and 436 000 ng/mL and area-under-the-curve exposure values of 130 000 and 1 240 000 h
Keywords
Introduction
For many types of cancer, surgery is a primary treatment modality, and the extent of surgical resection is directly related to survival. 1 -6 Failure to surgically remove a cancer-affected lymph node or residual cancer at the surgical margin may impact a patient’s chance for a successful outcome, often necessitating more aggressive postsurgical treatments such as repeat surgeries and more aggressive chemo/radiotherapy regimens. Alternatively, taking too much tissue can lead to significant morbidity or other health complications. Recent efforts have focused on methods to highlight tumor tissue in real time in the operating room to facilitate more accurate tumor excision. One such approach is fluorescence-guided surgery, in which contrast between tumor and normal tissue is achieved using fluorescent agents. These agents are administered to patients prior to surgery and rely on properties of the tumor, such as differential uptake of the dye or enzymatic activation, to achieve differences in fluorescent signal between tumor and normal tissue. Herein, we describe nonclinical safety and imaging data with a fluorescent peptide–dye molecule known as BLZ-100.
BLZ-100 is composed of a modified form of the chlorotoxin (CTX) peptide covalently bound to the near-infrared (NIR) fluorescent dye indocyanine green (ICG). The CTX peptides were originally isolated from scorpion venom 7 and have subsequently been shown to bind specifically to many types of tumor cells, 8 -14 allowing for potential broad applicability to a wide range of cancers, including glioma and other brain tumors, prostate, colorectal, lung, breast, head and neck cancers, and sarcomas. CTX was shown to facilitate blood–brain barrier (BBB) penetration of nanoparticles, 15 suggesting that the peptide may be able to reach brain tumors that do not have compromised BBB function. A synthetic version of the native CTX peptide (TM-601) has previously been studied and shown to be well tolerated in mice and marmosets, 16 and an iodine-131-labeled form underwent phase 1 clinical testing as a therapeutic for targeted delivery of radioactivity to gliomas and other cancers. 17 -19 The peptide component of BLZ-100 is similar to native CTX with modifications made to facilitate consistent attachment of the dye component. CTX binds directly to a phosphorylated form of Annexin A2, 20 which exists on the cell surface as a heterotetramer with S100A10 21,22 known as Calpactin. In normal cells, Annexin A2 is primarily intracellular and not phosphorylated. Matrix metalloproteinase 2 has also been proposed as a cell-surface CTX target. 23 Each proposed target is >90% identical between humans and the species commonly used for toxicology studies, with highest identity (>99%) between human and cynomolgus monkey.
ICG emits NIR fluorescent light which can be monitored during surgery using an appropriate detection device. ICG itself has been used safely for decades as a retinal angiography imaging agent. It has a reputation as a nontoxic and nonionizing agent, binds efficiently to blood lipoproteins, and does not leak from circulation. 24 Singlet oxygen produced from ICG is immediately bound to its own decomposition products, decreasing the likelihood of phototoxicity or photomutagenicity. 25 ICG does not have any known metabolites and is removed quickly and without modification from circulation into bile by glutathione S-transferase in the liver. 25
Here we show the initial safety pharmacology, PK, and toxicology profile of BLZ-100 based on studies conducted in CD-1 mice, Sprague Dawley rats, beagle dogs, and cynomolgus monkeys. Safety observations from an imaging pharmacology efficacy study conducted in mixed-breed dogs 11 are also discussed. These studies achieved a safety profile supporting first-in-human clinical trials for BLZ-100 as a human product candidate.
Materials and Methods
Studies were designed based on current International Conference on Harmonisation (ICH) guidelines, notably ICH S6(R1), S9 and M3(R2), and US Food and Drug Administration Guidance for medical imaging drugs. 26 Since BLZ-100 is intended to target tumor tissue which will not be present in normal animal safety studies, dose selection and interspecies scaling initially relied on tumor imaging data in mice to estimate a minimum effective imaging dose. In this context, an effective imaging dose was estimated by observing sufficient signal strength and contrast in mouse models to distinguish tumor from surrounding normal tissue. Furthermore, since BLZ-100 is intended to be given as a fixed intravenous (IV) bolus dose, the dosages in the animal studies were given as fixed dose levels with adjustments for the body surface area of each species used to scale doses across the species. The appropriateness of this approach was confirmed in the canine imaging efficacy study. 11 BLZ-100 was chemically synthesized by Blaze Bioscience by covalently attaching the ICG moiety to the CTX peptide. It was supplied as a lyophilized powder (purity ∼95%) and was formulated in an iso-osmotic neutral pH Tris–mannitol solution. Dosing solutions were analyzed for purity using high-performance liquid chromatography and for concentration using absorbance at 786 nm and comparison with a standard curve. Validated liquid chromatography–mass spectrometry (LC/MS) methods were used to measure BLZ-100 serum levels. Phoenix WinNonlin (Certara, Princeton, New Jersey, USA) software was used to estimate pharmacokinetic (PK) parameters for BLZ-100.
Animal studies were approved and conducted in accordance with each institution’s Institutional Animal Care and Use Committee and in compliance with the guidelines and principles listed in the American College of Toxicology Policy on the Use of Animals in Toxicology. For the Good Laboratory Practice (GLP) studies, the Sprague Dawley rats were supplied by Charles River and purpose-bred monkeys of Cambodian origin were supplied by SNBL USA.
Safety Pharmacology Studies
In vitro hERG assay (non-GLP)
Current amplitude was measured by the manual patch clamp technique at 0.2, 0.6, and 2 µM BLZ-100 (0.2 µM is equivalent to peak serum concentrations from the minimum imaging dose) in stably transfected human embryonic kidney (HEK 293) cells expressing hERG messenger RNA and incubated at 37°C. E-4031 (Sigma-Aldrich, St. Louis, MO) was used as a positive control for the assay. Quadruplicate measurements were made of the current amplitude.
Cardiovascular safety study (GLP)
Four male non-naïve cynomolgus monkeys (8.00 ± 0.17 years of age; 7.50 ± 0.39 kg) were surgically implanted with telemetry transducers to assess arterial blood pressure (ABP), heart rate (HR), respiratory rate (breaths/min), and Lead II electrocardiogram (ECG) parameters (PR interval, QRS duration, RR interval, and QT interval). Each animal was injected with ascending doses of vehicle control, 0.6, 6, and 60 mg BLZ-100, with a minimum 3-day washout period between administrations. The 3-day washout period was supported by PK data showing BLZ-100 blood levels were less than 1% of peak values 72 hours post-dose. Hemodynamic and ECG data were collected from 2 hours predose to 24 hours postdose. Lead II QT interval data were corrected for variations in HR using the Fridericia QTc (QTcF) and an individual animal correction factor (QTc1). Data points for analysis were 1 hour predose and 0.5, 1, 2, 3, 4, 5, 6, 12, and 24 hours postdose.
Studies in Rodents
Pilot toxicology study in mice (non-GLP)
Vehicle control, 0.01, 0.1 or 1 mg BLZ-100 were injected in the tail vein of CD-1 mice (6 females/group), and mice were euthanized 3 or 14 days postdose (3 females/group/time point). Measured parameters included clinical observations, body weight, abbreviated serum chemistry panel (including blood urea nitrogen, creatinine, alanine aminotransferase, aspartate aminotransferase, and γ-glutamyltransferase), and histopathology of major organs (including brain, heart, kidney, liver, lungs, intestines, skin, and spleen). Doses of 0.008, 0.08, or 0.8 mg (molar equivalent of BLZ-100 conjugate) of unconjugated peptide were injected into an additional group of female CD-1 mice (3 females/group) for monitoring clinical observations up to 1 hour after injection.
Definitive toxicology study in rats (GLP)
Vehicle, 0.07, 0.7, or 7 mg BLZ-100 was injected intravenously in Sprague Dawley rats (10/sex/group) on 1 occasion (day 1). Rats were euthanized on day 3 (5/sex/group) or day 15 (5/sex/group). Study parameters included clinical observations, neurological observations (including piloerection, respiratory abnormalities, posture, involuntary motor movements [clonic or tonic], stereotypy, bizarre behavior, gait abnormalities, and vocalization), body weight, food consumption, clinical pathology (serum chemistry, hematology, coagulation, and urinalysis), ophthalmology, gross pathology, organ weights, and histopathology. Animals for toxicokinetic (TK) analyses (6/sex/group) were bled for serum using a staggering sampling scheme (predose, 15 minutes postdose, and 1, 3, 6, 12, 24, and 48 hours postdose).
Studies in Dogs
Pilot study (non-GLP)
BLZ-100 dose of 1 mg was injected intravenously in the cephalic vein of beagle dogs as a bolus (1 male) or 15-minute infusion (1 male). A molar equivalent amount of unconjugated CTX peptide was bolus injected in a third male dog. Blood was collected from the jugular, cephalic, or saphenous veins for evaluation of serum PK at predose and at 5, 15, and 30 minutes and 1, 2, 4, 6, 24, 48, 72, and 96 hours postdose. Clinical observations were recorded at the same time points.
Efficacy study (non-GLP)
Mixed breed dogs with spontaneous solid tumors were treated with IV BLZ-100 and imaged as described. 11 A follow-up study was conducted with subcutaneous (SC) administration of BLZ-100 at 1 to 3 mg/m 2 and surgery at 1 or 2 days postdose. The SC doses were administered at sites contralateral to tumor location. Monitoring of safety end points and intraoperative imaging were performed as described. 11
Hypersensitivity study (non-GLP)
BLZ-100 dose of 1 mg was injected intravenously in the cephalic vein of 3 male beagle dogs. Pre- and postdose blood samples were collected at 0, 5, 15, and 30 minutes and 1, 2, and 24 hours postdose. Plasma samples (8 aliquots/animal/time point) were evaluated for histamine concentration. Activation of complement results in cleavage of C3 into bioactive split products. Therefore, the total amount of intact C3 present in the serum samples is inversely proportional to the degree of complement activation. Postdose serum samples (4 aliquots/animal/time point) were incubated with complement matrix and converter reagent (Quidel, San Diego, CA) for 60 minutes at 37°C to convert intact C3 to sC5b-9 as a stable end product. The sC5b-9 was then quantified using a commercial enzyme-linked immunosorbent assay kit (Quidel).
Definitive Study in Nonhuman Primates (GLP)
Vehicle, 0.6, 6, or 60 mg BLZ-100 were injected intravenously in the peripheral vein of naïve cynomolgus monkeys (3/sex/group, 2-3 years of age; 2.3-3.7 kg). Due to the wide dose range, the BLZ-100 concentration in the dosing solutions was varied (0.2, 2, and 5 mg/mL) so that dose volumes were feasible to measure and deliver at a dose rate <6 mL/min. Monkeys were euthanized on day 15. Study parameters included clinical observations (neurological and musculoskeletal), body weight, clinical pathology (serum chemistry, hematology, coagulation, and urinalysis), ophthalmology, gross pathology, organ weights, and histopathology. Urine samples collected at days 3 and 15 were analyzed using the Odyssey CLx NIR scanner (LI-COR Biosciences, Lincoln, NE) and the level of BLZ-100 estimated by comparison to a standard curve. Blood was collected and processed to serum for TK evaluations at predose, 5 and 15 minutes, and 1, 2, 4, 8, 12, 24, 36, 48, 72, 96, and 120 hours post day 1 dose.
Results
Doses for toxicology and safety pharmacology studies were selected to provide at least a 100-fold safety margin for a starting human clinical dose of 3 mg BLZ-100. Dose ranges for human clinical trials were estimated based on results of imaging studies in mice 12 and dogs. 11 Fluorescence intensity and contrast sufficient for effective imaging were obtained with IV bolus doses of 0.1 to 0.3 mg (∼1-3 mg/m2) in the mouse and confirmed in the dog at a dose of approximately 1 mg (∼1 mg/m2). Adjusted for body surface area, these animal dose levels suggested an appropriate starting dose level in human patients with cancer having peripheral tumors would be approximately 3 mg. At this level, evidence of tumor uptake of BLZ-100 is expected to be seen, although higher doses may be warranted depending on the tumor type and goals of the surgery (eg, brain cancer may require higher dose levels).
Safety Pharmacology Studies
An in vitro assay was used to assess the impact of BLZ-100 on hERG current amplitude at concentrations up to the estimated human peak blood concentration following the highest planned clinical dose (30 mg). The effect of BLZ-100 on hERG current amplitude (% change ± standard error of the mean) in HEK 293 cells was minimal at the tested concentrations, with the only possibly significant change occurring at the highest concentration (+0.2% ± 0.6 at 0.2 µM, -0.9% ± 0.8 at 0.6 µM, and -12.1% ± 1.0 at 2.0 µM, relative to the predrug value). In contrast, the positive control, E-4031, a potent and selective hERG blocker, 27,28 reduced current amplitude by over 80% at a 0.1 µM concentration. The BLZ-100 concentrations tested (0.2, 0.6, and 2.0 µM) were equivalent to estimated human peak blood concentrations after bolus injection of 3, 9, and 30 mg BLZ-100.
In the in vivo cardiovascular study, there were no changes in clinical signs or in hemodynamic or ECG parameters (including ABP, HR, breaths/minute, PR interval, QRS duration, RR interval, and QT interval) after ascending doses of 0.6, 6, and 60 mg BLZ-100 were administered to conscious male nonhuman primates. Mean serum levels of BLZ-100 (C max) were 436 000 ng/mL (91.5 µM) at the 60 mg dose level in the definitive TK analysis (see subsequently).
Studies in Rodents
In mice (administered 0.01, 0.1, or 1 mg BLZ-100), transient decreases in spontaneous motor activity, somnolence, and prostration were noted approximately 1 to 3 minutes postdose at 0.1 mg (N = 4) and 1 mg BLZ-100 (N = 6). The hypoactivity lasted 30 to 60 minutes and was completely resolved by 4 hours postdose. Similar findings were observed in mice injected with molar equivalent doses of the unconjugated CTX peptide.
In the definitive toxicology study at 0, 0.07, 0.7, and 7 mg BLZ-100 in rats, there were no adverse changes up to 14 days postdose, including no laboratory abnormalities or changes noted by microscopic pathology assessment of tissues. Gross findings at necropsy, presumably from the green-colored ICG dye component of BLZ-100, included green-discolored kidneys at 7 mg BLZ-100 on day 3 (4 males and 4 females) and day 15 (1 female). However, there were no changes in functional urinary clinical pathology parameters or renal pathology. The no-observed-adverse-effect-level (NOAEL) was considered 7 mg BLZ-100. Exposures based on C max and C 0 increased in an approximately dose-proportional manner across all dose groups. Exposure based on area under the concentration–time curve from time 0 to the timepoint with the last measurable concentration (AUC0–t) increased in an approximate dose-proportional manner between 0.07 and 0.7 mg BLZ-100 and increased in a higher than dose-proportional manner between the 2 lower dose groups and 7 mg BLZ-100 (Table 1 and Figure 1). There was no obvious influence of gender on exposure.
Mean Noncompartmental BLZ-100 PK Parameters After Single Bolus IV Doses in Male and Female Rats.
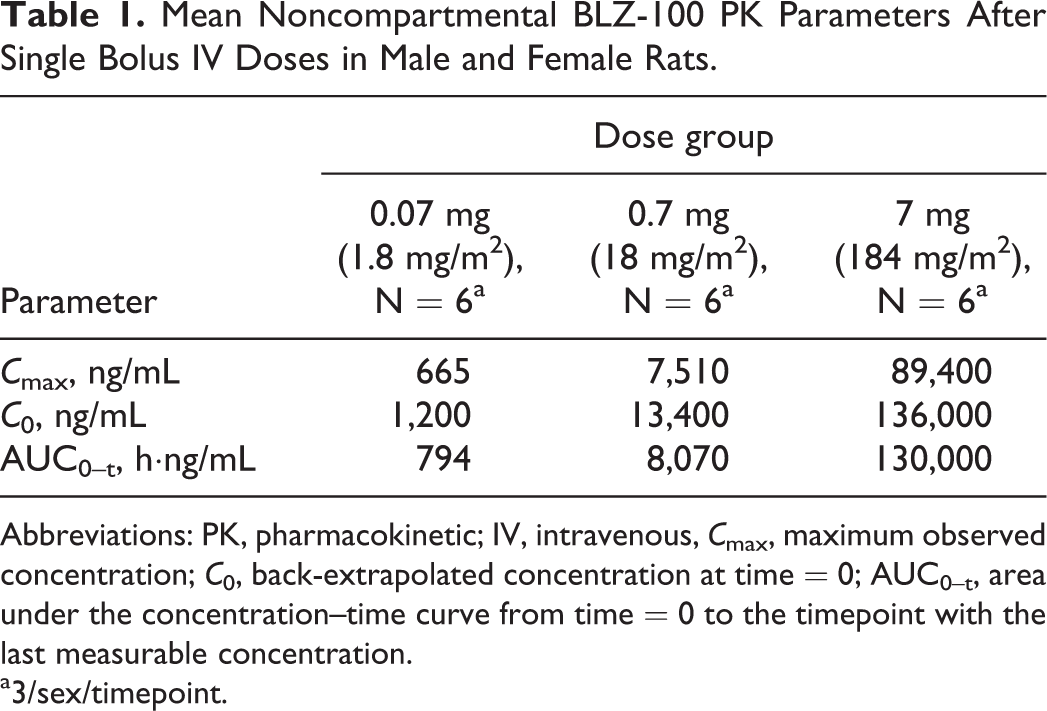
Abbreviations: PK, pharmacokinetic; IV, intravenous, C max, maximum observed concentration; C 0, back-extrapolated concentration at time = 0; AUC0–t, area under the concentration–time curve from time = 0 to the timepoint with the last measurable concentration.
a3/sex/timepoint.
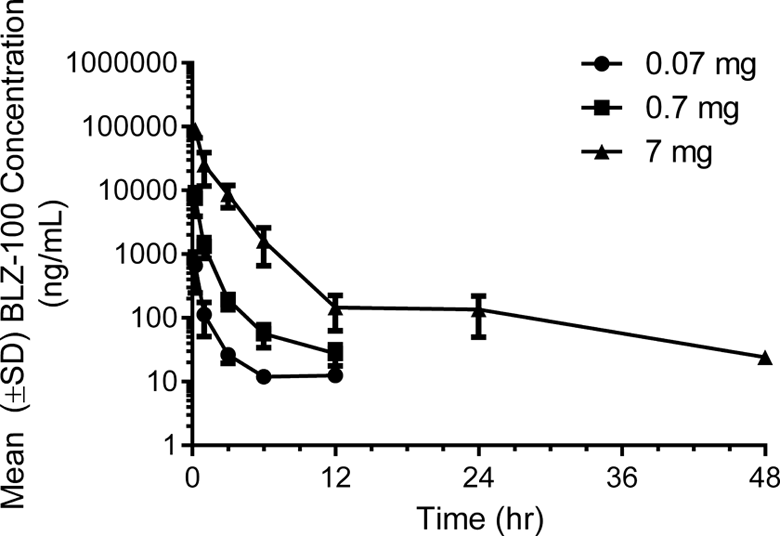
Mean BLZ-100 serum concentrations after single bolus intravenous (IV) doses in rats. The maximal concentration was observed at the first measured time point (0.25 hours postdose) in all groups (0.07, 0.7, and 7 mg BLZ-100). Mean serum concentrations were measurable out to 12 hours postdose (lower limit of quantification [LLOQ] = 10 ng/mL) in the 0.07 and 0.7 mg dose groups and out to 48 hours postdose (the last measured timepoint) in the 7 mg dose group.
Studies in Dogs
A pilot study in male dogs revealed pseudoallergic reactions shortly after administration of 1 mg BLZ-100. One dog given a bolus injection began scratching and biting its back 30 seconds postdose and was given diphenhydramine (25 mg IV) to ease the severity of the reactions. At 15 to 30 minutes postdose, the dog was still shaking vigorously, itching, and its ears were warm-to-touch. A second dog given a slower administration via a 15-minute IV infusion of BLZ-100 also demonstrated pseudoallergic reactions during the infusion (including red, warm ears and puffy, upper eyelids, and itching). Diphenhydramine was also administered to this dog. A third dog given 1 mg of the unconjugated CTX peptide by bolus injection showed no clinical signs of note.
Pseudoallergic reactions also occurred in 27 of 28 mixed breed dogs during a tumor imaging study that included safety evaluation end points. 11 All the dogs had spontaneous tumors and were undergoing solid tumor resection. The dogs were given IV injections of BLZ-100 at doses ranging from 0.1 to 1.5 mg. The hypersensitivity reactions were observed 5 to 10 minutes postdose, ranging from mild to severe pruritus, erythema, and swelling of the muzzle, and distal extremities (Table 2). The severity of the reactions was not dose related. Premedication with diphenhydramine (1 mg/kg SC) ameliorated symptoms, and additional diphenhydramine was given postdose as needed. The reactions abated 30 minutes to 4 hours after BLZ-100 injections.
Pseudoallergic Reactions in Mixed Breed Dogs With Spontaneous Tumors.
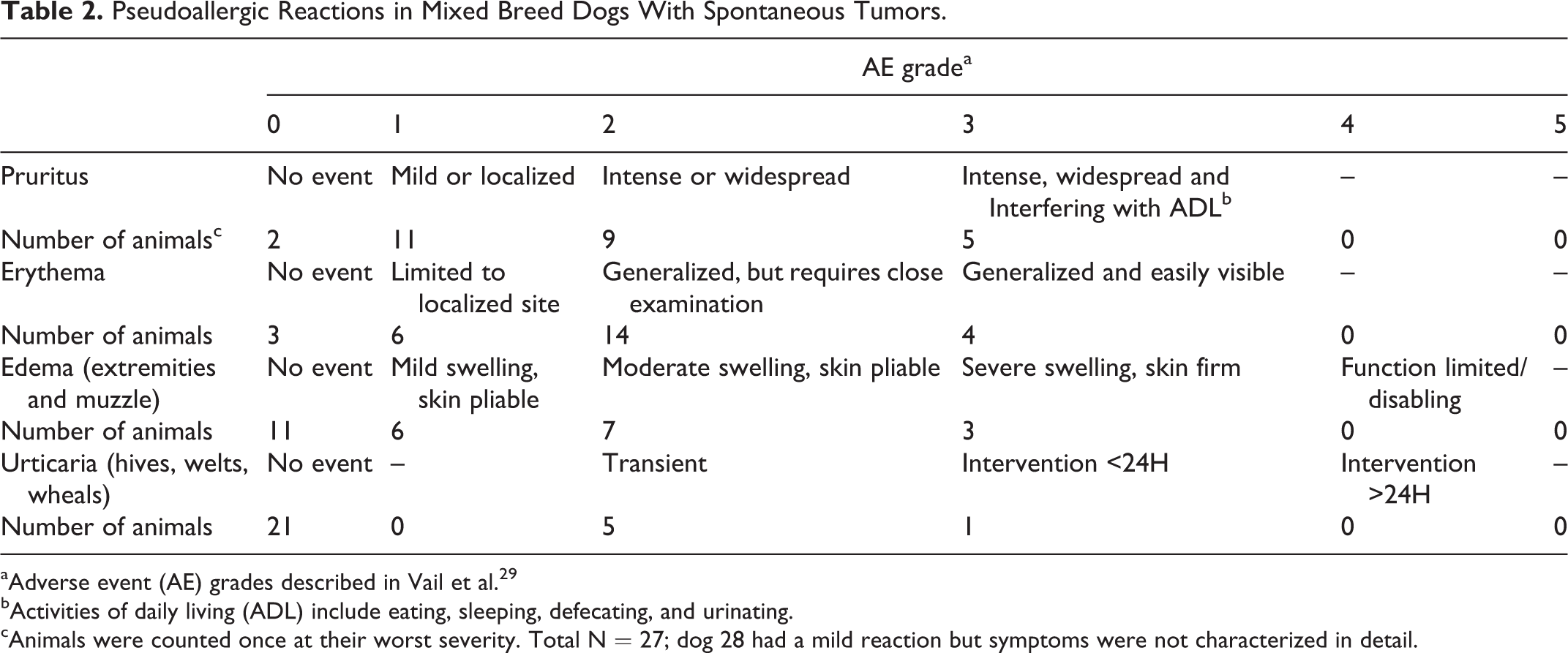
aAdverse event (AE) grades described in Vail et al. 29
bActivities of daily living (ADL) include eating, sleeping, defecating, and urinating.
cAnimals were counted once at their worst severity. Total N = 27; dog 28 had a mild reaction but symptoms were not characterized in detail.
In a follow-up mechanistic study, histamine release was observed following IV injection of 1 mg BLZ-100 to beagle dogs (N = 3). Histamine release was increased at the first time point of 5 minutes, which coincided with the first clinical signs (including scratching, erythema of muzzle and ears, increased respiration, and lethargy). Histamine release remained increased up to 1 hour postdose (Figure 2). Histamine plasma concentrations decreased by 2 hours postdose and returned to baseline concentrations by 24 hours postdose. Clear evidence of complement activation, denoted by decreased levels of sC5b-9, was not observed (Figure 3).
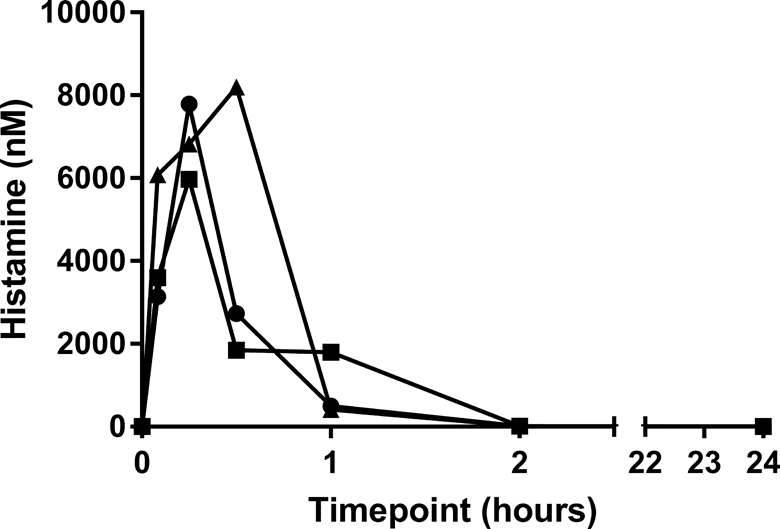
Histamine levels in plasma from canines after bolus intravenous (IV) administration of 1 mg BLZ-100. Data are plotted separately for each animal (N = 3). T = 0 values were from baseline samples collected prior to dosing. Time points listed for postdose samples are measured from the actual time of dose administration for each animal.
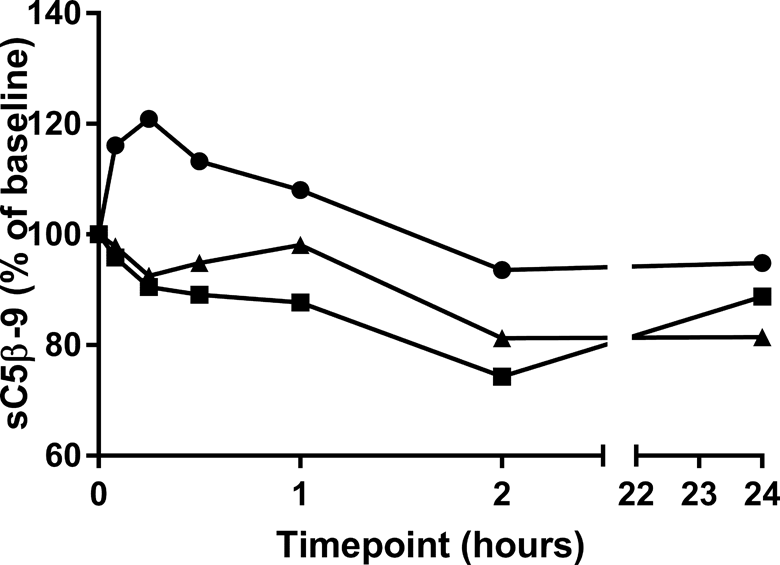
Complement in serum from canines after bolus intravenous (IV) administration of 1 mg BLZ-100. The assay measures sC5b-9 as a stable end product of C3 cleavage. Levels of sC5b-9 in the assay are inversely proportional to complement activation in the serum. Data are plotted for individual animals (N = 3).
The SC administration was evaluated for imaging efficacy and tolerability in 14 dogs. There were no obvious reactions similar to those observed after IV dosing of BLZ-100 in the dogs given BLZ-100 SC, including 2 dogs treated at 3 mg/m2 SC. Furthermore, fluorescence contrast comparable to that seen with IV administration was observed (Figure 4).
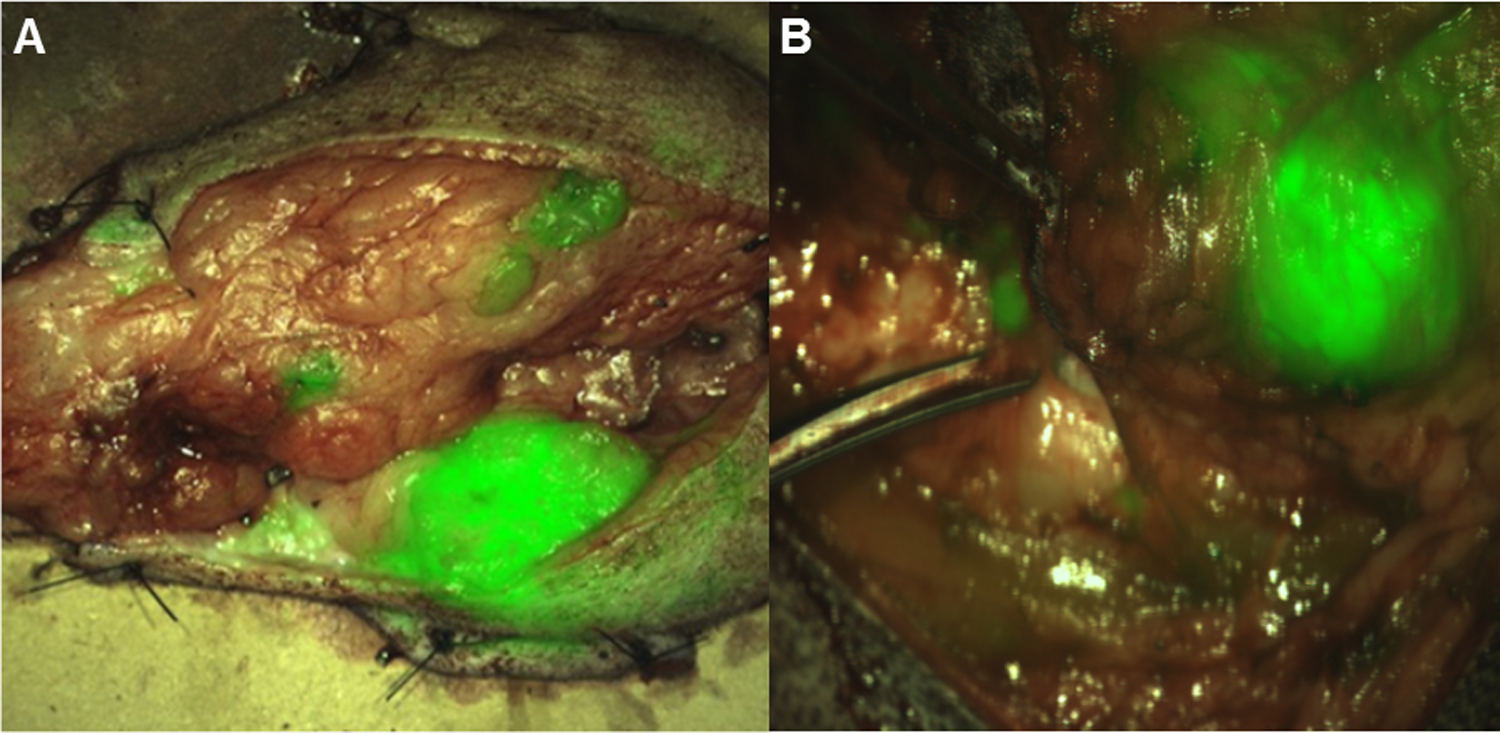
Imaging results following BLZ-100 administration in dogs. A, Imaging of a mammary carcinoma following an intravenous (IV) dose of 1.24 mg/m2 BLZ-100. B, Imaging of a soft tissue sarcoma following a subcutaneous dose of 3.0 mg/m2 BLZ-100. Primary masses and satellite lesions were distinguished from surrounding normal tissue in both cases. Imaging was performed as described. 11 Near-infrared signal is pseudocolored green and shown overlaid on the white light images.
Definitive Toxicology Study in Nonhuman Primates
In the definitive study (0, 0.6, 6, and 60 mg BLZ-100) in nonhuman primates, there were no pseudoallergic reactions or other adverse findings up to 4 and 14 days postdose, respectively. The only treatment-related finding was green-colored urine on day 3 at 60 mg BLZ-100 (1 male and 3 females). An exploratory fluorescence assay showed that the urine of most but not all treated animals had an increased fluorescent signal intensity on days 3 and 15 at both 6 and 60 mg BLZ-100. There were no clinical or anatomic pathology findings in the study. Select hematology and clinical chemistry parameters highlighting the lack of systemic toxicity of BLZ-100 are listed in Table 3. The NOAEL was considered 60 mg BLZ-100.
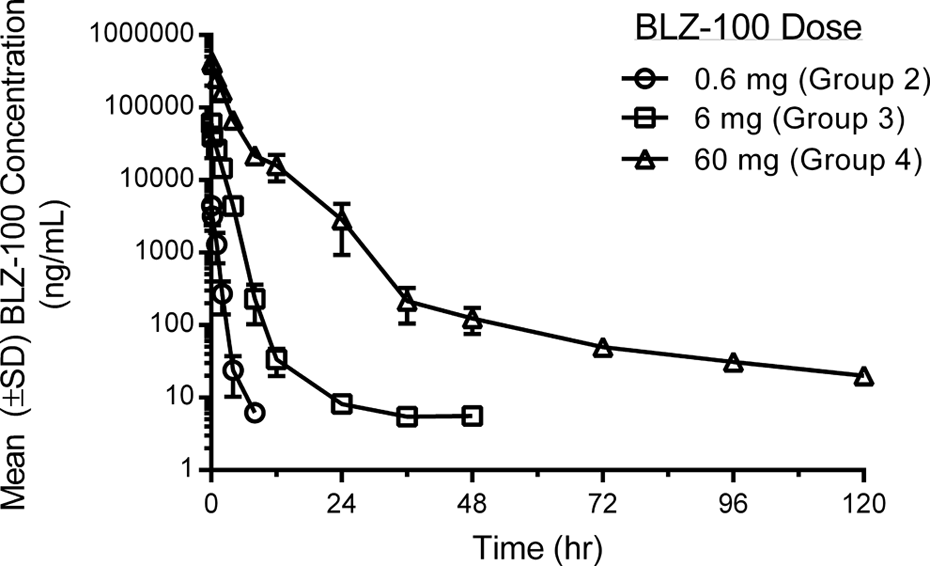
Mean BLZ-100 serum concentrations after single bolus intravenous (IV) doses in nonhuman primates. The mean maximal concentration of BLZ-100 was observed at the first measured time point (0.083 hours (5 minutes) postdose) in all BLZ-100 dose groups (0.6, 6, and 60 mg). Mean serum concentrations were measurable (>5 ng/mL) out to 8, 48, and 120 hours postdose (the last measured timepoint) in the 0.6, 6, and 60 mg dose groups, respectively.
Selected Hematology and Clinical Chemistry Parameters in Nonhuman Primates Following Single IV Bolus Doses of BLZ-100.
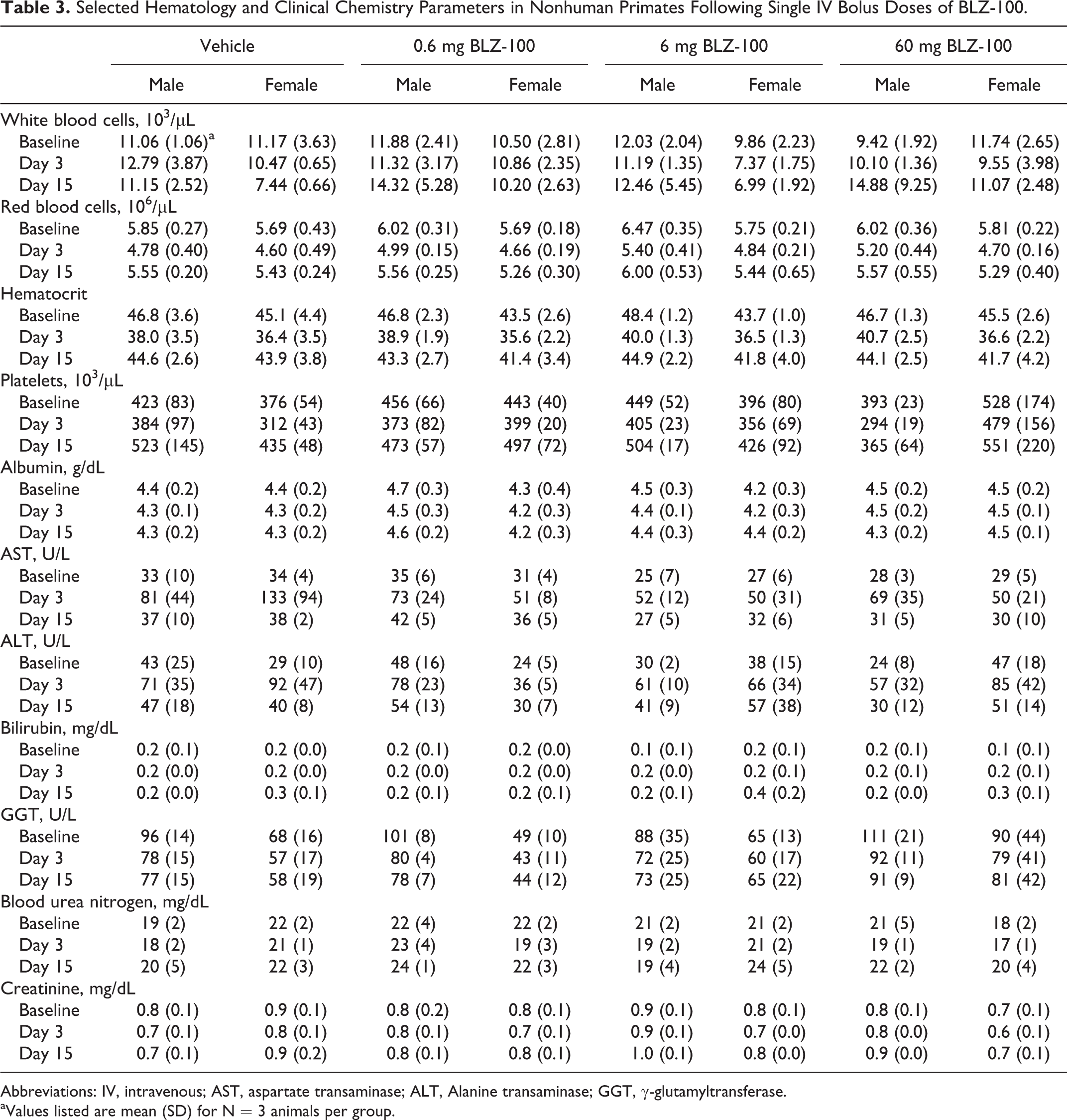
Abbreviations: IV, intravenous; AST, aspartate transaminase; ALT, Alanine transaminase; GGT, γ-glutamyltransferase.
aValues listed are mean (SD) for N = 3 animals per group.
Exposure based on C max and C 0 was approximately dose proportional across the 100-fold dose range (0.6-60 mg). Exposure based on AUC0–t, however, increased in a greater than dose-proportional manner between the 6 and 60 mg doses (Table 4). No clear gender-related differences based on C 0 and AUC0–t were observed. Additional noncompartmental TK parameters estimated at 60 mg BLZ-100 (Table 4) included an overall mean t 1/2 of 33.7 hours, clearance of 50.6 mL/h, and volume of distribution (V ss) of 211 mL (approximately equal to the plasma volume in a 5 kg monkey). In addition, examination of the LC/MS chromatograms from serum samples did not reveal the presence of major metabolites of BLZ-100.
Mean (SD) Noncompartmental BLZ-100 PK Parameters After Single IV Bolus Doses in Male and Female Nonhuman Primates.
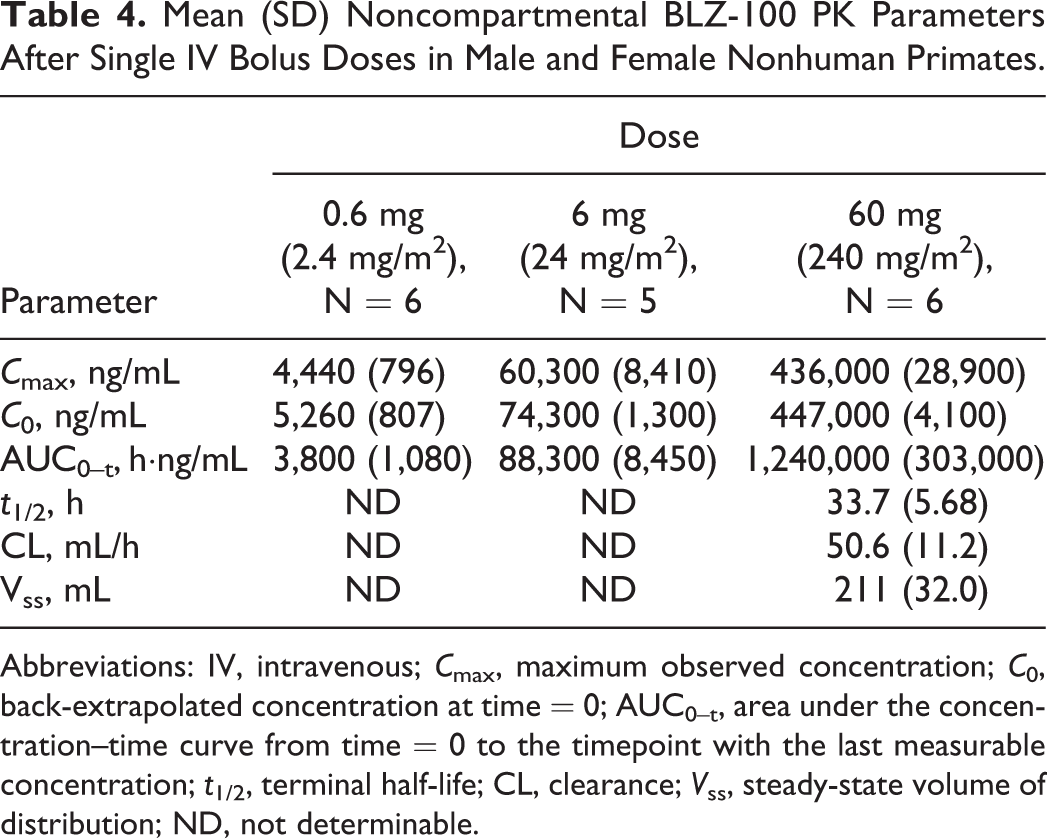
Abbreviations: IV, intravenous; C max, maximum observed concentration; C 0, back-extrapolated concentration at time = 0; AUC0–t, area under the concentration–time curve from time = 0 to the timepoint with the last measurable concentration; t 1/2, terminal half-life; CL, clearance; V ss, steady-state volume of distribution; ND, not determinable.
Discussion
Single bolus IV doses of BLZ-100 were well tolerated in mice, rats, and monkeys. Treatment-related changes observed in mice included transient decreased spontaneous motor activity, somnolence, and prostration at 0.1 and 1 mg BLZ-100. An equivalent amount of the CTX peptide produced the same effect, suggesting this response was likely peptide related. Peptides from scorpions and other insects have ion channel-blocking properties, and it is possible that high doses of the BLZ-100 and CTX in mice resulted in the transient effects seen. These changes have not been observed to date in the BLZ-100 human clinical trials or in nonclinical species other than mice. In addition to the toxicity evaluations, no effects on HR, blood pressure, respiration rate, or ECG tracings were observed in a safety pharmacology study in conscious monkeys.
In a pilot tolerability study in dogs, pseudoallergic/hypersensitivity reactions (itching/scratching, warm ears, etc) were observed during or immediately after dosing in 2 of 2 dogs at 1 mg BLZ-100 IV but were not observed in a third dog given unconjugated peptide. Similar signs of hypersensitivity were observed in most dogs given BLZ-100 in a tumor imaging pharmacology study. 11 These hypersensitivity reactions have only been observed in dogs and were consistent with a systemic release of histamine, which has been reported for a wide variety of drugs. 30,31 In an in vivo follow-up study in the dog, clear evidence of a rapid rise in plasma histamine levels was observed while complement levels appeared unaffected. These data supported the concept that the clinical signs observed in the dog were likely a result of direct mast cell/basophil activation by BLZ-100. Subcutaneous administration of BLZ-100 appears to be one method to ameliorate this potential response in the dog.
In the definitive rat and nonhuman primate studies, the only toxicology findings were green-discolored kidneys and green-colored urine, respectively, presumably from the ICG dye in BLZ-100. There were no functional or pathologic correlates. A fluorescence assay revealed that the urine of most nonhuman primates at the 2 highest doses (6 and 60 mg BLZ-100) had increased fluorescence signal intensity, suggesting BLZ-100 in urine likely accounted for the green color. There were no adverse treatment-related changes in either study (including clinical and neurological observations, body weight, food consumption, ophthalmology, clinical and anatomic pathology). The NOAELs were 7 mg (∼28 mg/kg) and 60 mg (∼20 mg/kg) in rats and nonhuman primates, respectively. Compared to the estimated minimal imaging dose in patients of 3 mg, the resulting dose safety margins (ratio of NOAEL dose in animal to human dose) are 560 for the rat and 400 for the monkey on a mg/kg basis. Converting the rat and monkey doses on a mg/m2 basis results in lower but still acceptable margins of 98 and 128, respectively. Finally, using AUC PK estimates, the safety margins are 470 for the rat and 4,500 for the monkey.
The peptide component of BLZ-100 is similar to native CTX. A synthetic version of the CTX peptide (TM-601) has been studied in mice and marmosets, and it was well tolerated. 16 The NOAEL for TM-601 after a single IV dose were the highest doses tested in the mouse (6.4 mg/kg) and marmoset (2.0 mg/kg). Repeated dosing for 7 weeks in mice at 2 and 5 mg/kg IV resulted in clinical signs of transient ptosis and hypoactivity within 1 hour postdose. No effects on hematology or tissue pathology were observed. These results appear consistent with the BLZ-100 data presented here.
ICG itself has been used safely for decades in ophthalmology as a retinal angiography imaging agent. In a review article on the use of ICG in choroidal angiography, Weichel et al 32 reported 7 reactions of 1,923 ICG angiograms performed in 1,226 patients. The reactions included nausea and vomiting in 2 cases, urticaria in 2 cases, vasovagal reactions in 2 cases, and acute hypotension in 1 case (0.3% adverse reaction rate). Olsen et al 33 highlighted there was only 1 severe reaction among the 1,226 (0.05%) patients and only 2 severe reactions among 2,820 patients receiving ICG angiograms from Japanese ophthalmologists. It is also worth noting that the typical doses of ICG vary by indication but generally range from 25 to 50 mg. By comparison, BLZ-100 contains roughly 0.15 mg dye/mg of drug product. BLZ-100 imaging doses for peripheral tumors are currently estimated to range from 3 to 12 mg or 0.45 to 1.8 mg equivalents of ICG. Doses for imaging of brain cancer appear to be higher, ranging from 18 to 30 mg or 2.7 to 4.5 mg equivalents of ICG.
Typical clinical use and exposure to BLZ-100 will be of short duration, consisting of a single injection prior to undergoing surgical excision of cancer. Second or repeat doses are possible in some subjects, possibly due to incomplete excision/tumor regrowth or a second cancer. However, it is likely the time interval between additional doses is months to years. The nonclinical safety profile presented here supported initiation of phase I human clinical trials.
Footnotes
Acknowledgments
We thank Carolyn Gombotz, Tori Pinkerton, Gordon Brandt, Claudia Jochheim, Jennifer Zimmer, Mark Stroud, Natalie Nairn, Sandra D. Love, and Devendra Dandekar for administrative and technical support.
Author Contributions
Parrish-Novak, J. contributed to conception and design, contributed to acquisition, analysis, and interpretation, drafted manuscript, and critically revised manuscript; Byrnes-Blake, K. contributed to design contributed to analysis and interpretation, and critically revised manuscript; Lalayeva, N., Burleson, S., and Hansen, S. contributed to design, contributed to acquisition, analysis, and interpretation, and critically revised manuscript; Fidel, J. and Dernell, W. contributed to conception and design, contributed to acquisition and interpretation, and critically revised manuscript; Gilmore, R., Gayheart-Walsten, P., and Bricker, G. contributed to conception and design, contributed to acquisition, analysis, and interpretation, and critically revised manuscript; Crumb, W. and Wiss, V. contributed to design, contributed to acquisition and analysis, and critically revised manuscript; Tarlo, K. contributed to conception and design, contributed to interpretation, drafted manuscript, and critically revised manuscript; Malta, E., contributed to conception and critically revised manuscript; Olson, J. contributed to conception, contributed to interpretation, and critically revised manuscript; Miller, D. contributed to conception and design, contributed to analysis and interpretation, and critically revised manuscript. All authors gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KBB and KST are consultants for Blaze Bioscience Inc and Blaze Bioscience Australia Pty Ltd. JMO is a cofounder of Blaze Bioscience Inc, holds equity in Blaze and serves on the BOD. JPN, SH, and DMM are employed by and hold equity in Blaze Bioscience Inc. DMM and EM are employed by Blaze Bioscience Australia Pty Ltd.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Portions of this study were funded with Federal funds from National Cancer Institute (NIH), Department of Health and Human Services, under contract no HHSN261201200054C.