
Abstract
The aim of this work is to assess DNA damage in peripheral blood lymphocytes of children prior to and following airway X-ray examinations of the chest using the alkaline comet assay and to compare data with the measured absorbed dose. Twenty children with pulmonary diseases, between the ages of 5 and 14 years, are assessed. Absorbed dose measurements are conducted for posterior–anterior projection on the forehead, thyroid gland, gonads, chest, and back. Doses are measured using thermoluminescent and radiophotoluminescent dosimetry systems. Differences between tail lengths, tail intensity, and tail moments as well as for the long-tailed nuclei before and after exposures are statistically significant and are dependent on the individual. The results demonstrate the usefulness of the comet assay as a measure of X-ray damage to lymphocytes in a clinical setting. Doses measured with both dosimeters show satisfactory agreement (0.01 mSv) and are suitable for dosimetric measurements in X-ray diagnostics.
As is commonly known, ionizing radiation induces various lesions to DNA, including double-strand breaks. Although cells can repair such lesions, they are still responsible for mutations, chromosomal aberrations, and cell death in case of misrepair or no repair at all. 1,2 To maximize the quality of radiation protection, we need to understand not only the genetic impact of ionizing radiation but also the clinical needs for such exposures. The majority of radiation is human-made, and most of the human-made radiation is from medical diagnostic and therapeutic procedures.
In pediatric hospitals and departments, radiological examinations are critical in evaluating diseases of the lung and other internal organs, yet these tests must be performed in the safest way possible. Chest radiograms are the basic radiological examination of thorax because they provide diagnostic information on the lung, heart, and skeletal system. Chest radiograms are the most frequently performed radiological diagnostic procedure in the pediatric population. 3,4 Most radiological examinations produce doses ranging from 0.06 to 0.25 mSv. 5 Understanding the risks of low doses of radiation is an important aspect in risk–benefit analysis in pediatric populations. To provide the best care for young patients, the effects of ionizing radiation should be minimized. Chest X-rays must be performed by highest standards to ensure that the young patient has the lowest risk possible. 3,6-12 The ALARA (as low as reasonably achievable) principle is the basis for radiation protection. Also, the determination of absorbed dose is a prerequisite for risk estimation of genetic damage, especially in pediatrics. 13-15
As a rapid and sensitive technique, the alkaline comet assay has gained widespread acceptance in molecular epidemiology, especially in radiation monitoring. 16-19 The comet assay permits the detection of primary DNA damage and the study of repair kinetics at the single cell level and from that point of view could be suitable for use in a clinical setting because it is a relatively simple and inexpensive technique that requires only a small amount of cells, and results can be obtained within a short time after sampling (ie, within a few hours). 20-23 In human studies, the comet assay has widely been used to quantify DNA damage in isolated lymphocytes from subjects exposed to various environmental or occupational substances. 21,24-26 In addition, many studies have successfully demonstrated that the comet assay can be applied to the analysis of cells derived from a variety of different human tissues, lending considerable weight to the suggestion that this assay could benefit many areas of clinical investigation by providing valuable information about the intrinsic DNA characteristics of individual cells and their responses to various external factors, such as radiation, chemicals, and drugs. This type of information would prove particularly relevant in the diagnosis, prognosis, and treatment of cancer. 23,27,28
Given the results of previous epidemiological research and the fact that children are one of the populations most sensitive to radiation, there is a need for follow-up of children who receive X-ray examinations. 4,6,7,29,30 Follow-up is especially advisable for children who are at higher risk of radiation-induced damage, for example, children with a predisposition to DNA damage as inherited in ataxia telangiectasia or children who undergo numerous radiological examinations in a short period of time. 2,31 Absorbed dose measurement following diagnostic X-rays is not simple. The thermoluminescent (TL) dosimetric systems have been found to be adequate for absorbed dose measurements in X-ray diagnostics. 13,32-35 The characteristics (linearity, sensitivity, reproducibility, fading, energy dependence) of radiophotoluminescent (RPL) dosimetry system as well as their comparison with TL dosimeter indicated the suitability of this system for X-ray diagnostics. 36-38
The aim of this study was to compare the absorbed dose of radiation to the possible impact on the DNA molecule during diagnostic examination of children. TL and RPL dosimetry systems were used for dosimetric purposes, and the alkaline comet assay was used to evaluate DNA damage.
Subjects and Methods
Patients and Blood Sampling
Twenty children (14 female and 6 male) between the ages of 5 and 14 years were selected randomly, all with pulmonary diseases such as pneumonia, bronchitis, asthma, and suspected tuberculosis. None of the assessed children were exposed to ionizing radiation or steroid therapy for at least the previous 6 months or antibiotics for the last 3 months. The weight and height of the patients varied between 20 and 69 kg and 110 and 177 cm, respectively. Diagnostic chest X-rays and clinical pathology exams of blood samples were warranted because of the children’s health conditions. The present study was performed in accordance with high ethical standards. Blood donors were informed about the aim and the experimental details of the study. All of the parents or legal guardians gave their informed consent and volunteered to donate blood for sampling. Every volunteer completed a standardized questionnaire, designed to obtain relevant details about his or her current health status, history, and lifestyle.
Blood samples were taken from veins in the antecubital fossae prior to and exactly 30 minutes after X-ray examination. Peripheral blood samples were collected in heparinized vacutainer tubes (Becton Dickinson, Franklin Lakes, NJ) under aseptic conditions. All blood samples were handled in the same manner. After venipuncture, samples were randomly coded, cooled to 4°C in the dark, and transferred to the laboratory on ice to minimize DNA repair after irradiation. Samples were analyzed immediately after the arrival (1 hour after collection at the latest) using the alkaline version of the comet assay.
X-ray Examination and Dosimetry
The X-ray examinations of the thorax were carried out in posterior–anterior (PA) projection on a 150-kV Shimadzu CH-200M unit (Tokyo, Japan). The conditions of exposure were normal for routine diagnostic procedures. The parameters of the irradiation were the following: the voltage of the X-ray tube varied in the range 95 to 105 kV, the quantity of charge 2 to 3.6 mAs, and the time of irradiation 5 to 11 milliseconds.
Two types of dosimetry systems were used in this research: RPL glass dosimetry system and TL dosimetry system based on LiF:Mg,Cu,P.
The RPL dosimeters consist of flat, silver-activated phosphate glass in a dosimeter capsule containing a tin energy compensation filter. After irradiation, color centers generated in the glass during UV excitation in the reader emit a radiation-induced orange fluorescent light. In our experiments, the full automatic FGD-200 Series dosimeter system with SC-1 glass dosimeters was used. The system is based on pulsed nitrogen gas UV laser excitation, which allows the electric discrimination of signals from the predose reading and the radiation-induced reading. The fully automatic system (built-in calibration factors, reference glass for correction) has the advantage of quick and easy reading.
After irradiation, the TL dosimeters detectors stayed at room temperature at least 1 day. The reading of TL signal was carried out using a modified Toledo 654 (Vinten Instruments, Beaconsfield, UK) reader. The reader is connected to a personal computer containing software (TEMES) that enables the integration of the glow curves with variable integration limits and a detailed analysis of glow curves. TEMES program was developed in the LabVIEW programming environment of National Instruments Company (Austin, Tex). The properties of used TLDs were shown in our previous article. 39 The evaluation parameters of the investigated detectors are shown in Table 1 .
Evaluation Parameters of the Investigated Detectors
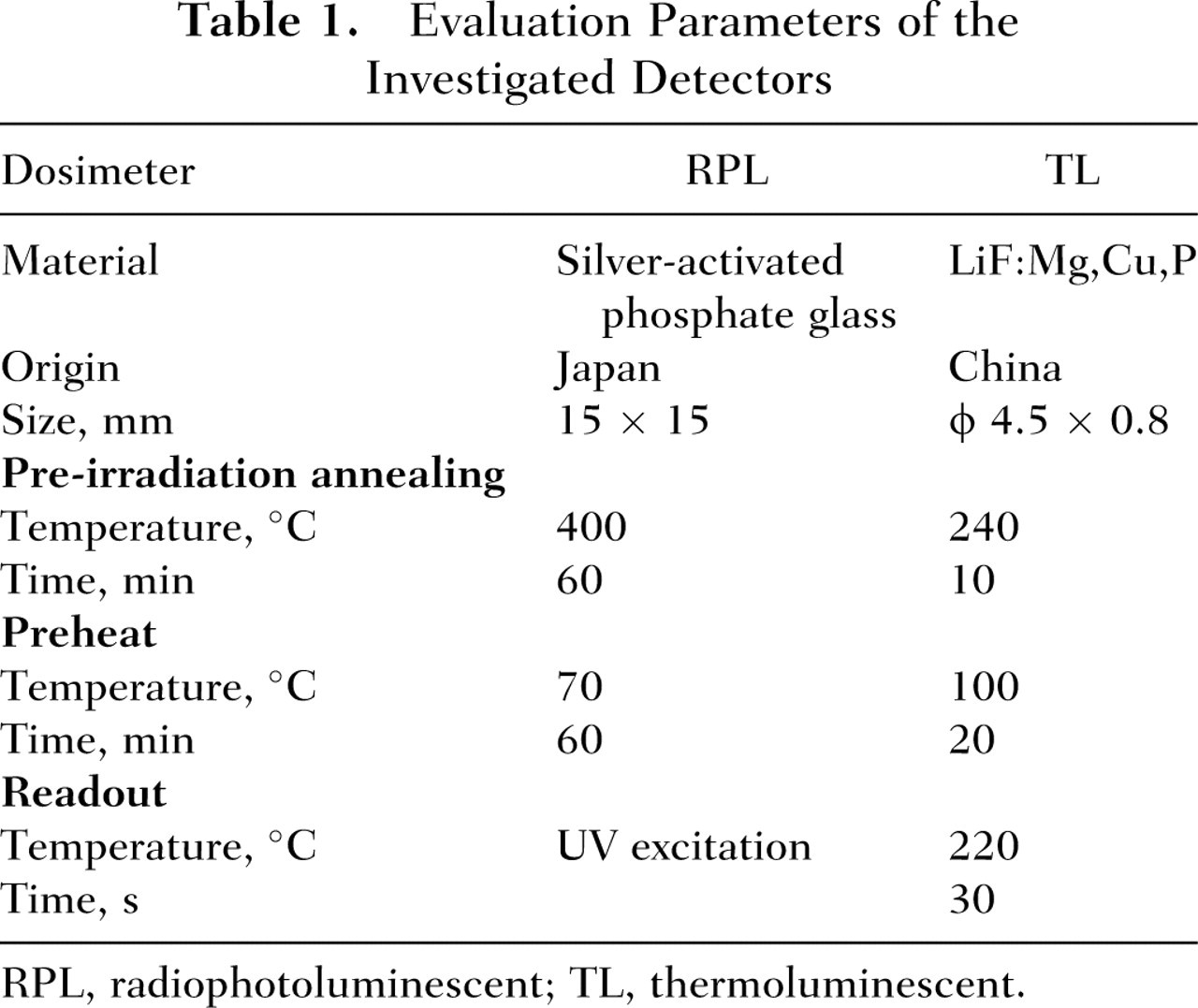
RPL, radiophotoluminescent; TL, thermoluminescent.
For irradiation, the detectors were packed in a dark polyethylene foil and placed in rubber holders. The holders with 3-mm wall thickness were used for both 137Cs and X-ray irradiations, respectively. For calibration, irradiations with 137Cs gamma ray source at the Secondary Standard Dosimetry Laboratory 40 in the Ruđer Bošković Institute were performed at a distance of 1 m from the source. The dose rate was 57.51 mGyh-1. The individual sensitivity of each TL detector was previously determined by irradiation with the same 137Cs gamma ray source, whereas the RPL detectors were calibrated individually by the manufacturer. To estimate the calibration factors, 5 TL detectors placed “free in air” were irradiated with 2 mGy. For background correction, 3 control dosimeters were used. The doses on the patients were specified in terms of Hp(10) using the factor Hp(10)/Ka = 1.21.
Absorbed dose measurements were conducted for PA projection on the forehead, thyroid gland, gonads, chest, and back. RPL dosimeters were not placed on chest and the back to ensure the radiogram quality.
Alkaline Comet Assay
To estimate the level of primary DNA damage after exposure to low X-rays, the comet assay was carried out under alkaline conditions, as previously described by Singh et al. 41 Fully frosted slides were covered with 1% normal melting point (NMP) agarose (Sigma, St Louis, Mo). After solidification, the gel was scraped off the slide. The slides were then coated with 0.6% NMP agarose. When this layer had solidified, a second layer, containing the whole blood sample mixed with 0.5% low melting point (LMP) agarose (Sigma), was placed on the slides. After 10 minutes of solidification on ice, slides were covered with 0.5% LMP agarose. Slides were then immersed for 1 hour in ice-cold freshly prepared lysis solution (2.5 M NaCl, 100 mM disodium EDTA, 10 mM Tris-HCl, 1% sodium sarcosinate [Sigma], pH 10) with 1% Triton X-100 (Sigma) and 10% dimethyl sulfoxide (Kemika, Zagreb, Croatia) to lyse the cells and allow DNA unfolding. The slides were then placed on a horizontal gel electrophoresis tank, facing the anode. The unit was filled with fresh electrophoresis buffer (300 mM NaOH, 1 mM disodium EDTA, pH 13.0), and the slides were placed in this alkaline buffer for 20 minutes to allow DNA unwinding and expression of alkali-labile sites. Denaturation and electrophoresis were performed at 4°C under dim light. Electrophoresis was carried out for 20 minutes at 25 V (300 mA) (20 minutes at 1 V/cm). After electrophoresis, the slides were rinsed gently 3 times with neutralization buffer (0.4 M Tris-HCl, pH 7.5) to remove excess alkali and detergents. Each slide was stained with ethidium bromide and covered with a coverslip. Slides were stored at 4°C in sealed boxes until analyzed. To prevent additional DNA damage, handling of blood samples and all the steps included in the preparation of the slides for the comet assay were conducted under yellow light or in the dark.
Comet Capture and Analysis
One hundred randomly captured comets from each slide were examined at 250× magnification using an epifluorescence microscope (Zeiss, Oberkochen, Germany) connected through a black-and-white camera to an image analysis system (Comet Assay II; Perceptive Instruments, Haverhill, Suffolk, UK). An automated image analysis system was used to acquire images, compute the integrated intensity profile for each cell, estimate the comet cell components, and evaluate the range of derived parameters. Comets were randomly captured at a constant depth of the gel, avoiding the edges of the gel, occasional dead cells, and superimposed comets or comets without distinct head (“clouds,” “hedgehogs,” or “ghost cells”). To avoid potential variability, 1 well-trained scorer performed all scorings of comets. To quantify DNA damage, the following comet parameters were evaluated: tail length, tail intensity (percentage of DNA), and tail moment. Tail length (ie, the length of DNA migration) was calculated from the center of the cell and is presented in micrometers. Tail intensity is defined as the percentage of fluorescence migrated in the comet tail. Tail moment was calculated as (tail length × % of DNA in tail)/100. Moreover, cells were classified as either undamaged or damaged by considering threshold levels indicating the long-tailed nuclei (LTN) comets, that is, comets with the length over the 95th percentile of the distribution of the tail lengths for each patient after exposure compared with before exposure. 42
Statistical Analysis
Each experimental set contained duplicate slides. The comet parameters of tail length, tail intensity, and tail moment measured prior to and after exposure to diagnostic X-ray exposure were evaluated using Statistica 5.0 package (StatSoft, Tulsa, Okla). Each sample was characterized for the extent of DNA damage by considering the mean ± standard error of the mean, median, and range of the comet parameters. To normalize the distribution and to equalize the variances, a logarithmic transformation of data was applied. Multiple comparisons between groups were done by means of analysis of variance on log-transformed data. Post hoc analyses of differences were done by using the Scheffé test. Statistical significance for the LTN was analyzed using the chi-square test. The level of statistical significance was set at P < .05.
Results
Radiation exposure estimates measured at the different positions on the body are presented in Table 2 . Mean values for the tail length, tail intensity, and tail moment of the alkaline comet assay as well as LTN for individual patients before and after X-ray diagnostics are summarized in Tables 3, 4, and 5. Figure 1 shows the group distribution of tail lengths, tail intensity, tail moments, and LTN measured in peripheral blood lymphocytes of the children before and after their exposure to the X-rays, and the ratio of tail length, tail intensity, and tail moment after and before exposures and LTN after exposures are presented in Figure 2.
Doses, Expressed as Hp(10), Measured at Different Positions on the Body
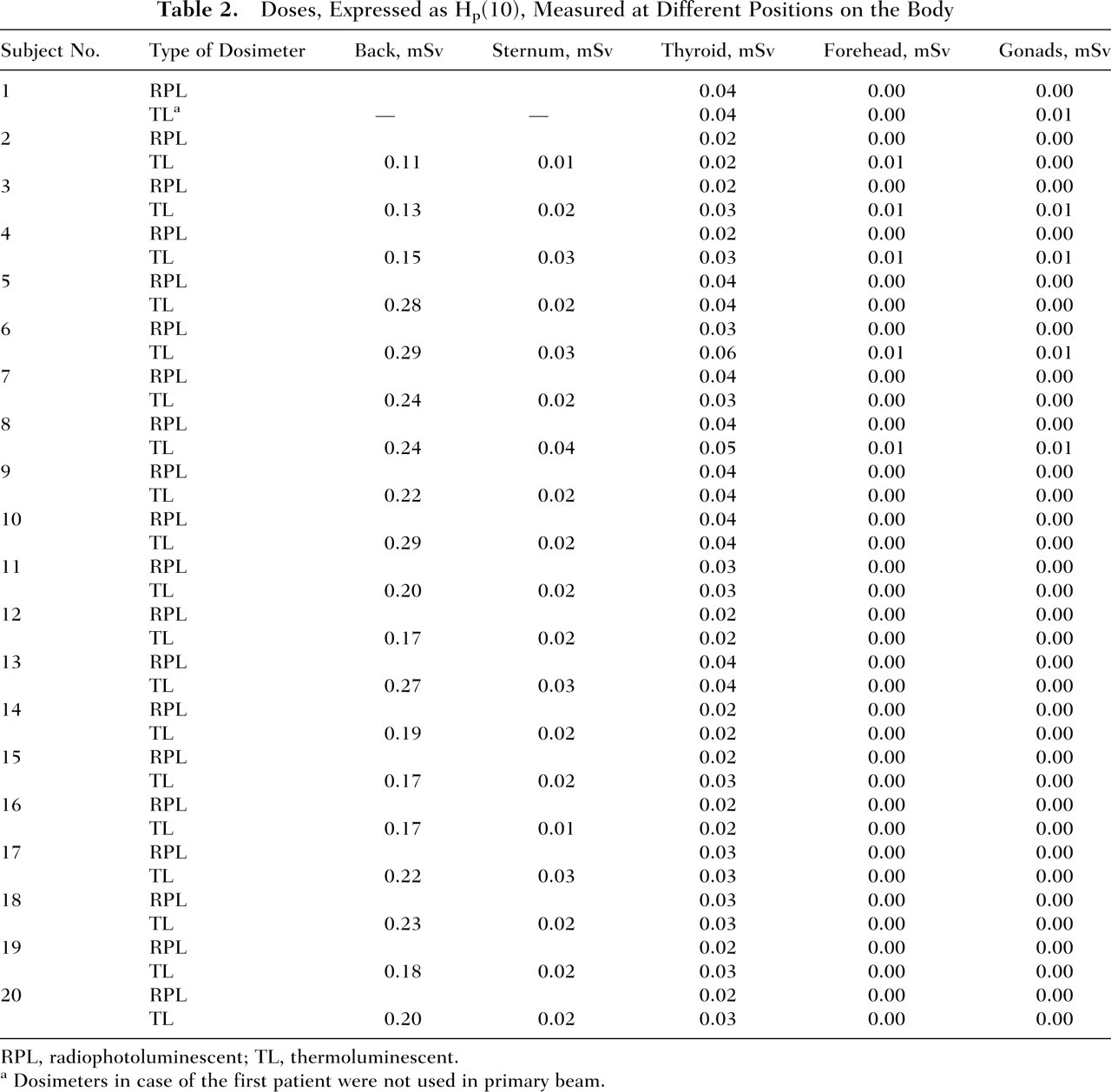
RPL, radiophotoluminescent; TL, thermoluminescent.
Dosimeters in case of the first patient were not used in primary beam.
Comet Parameters for Tail Length in Peripheral Blood Samples of Children With Pulmonary Diseases Before and After X-ray Diagnostic Examination
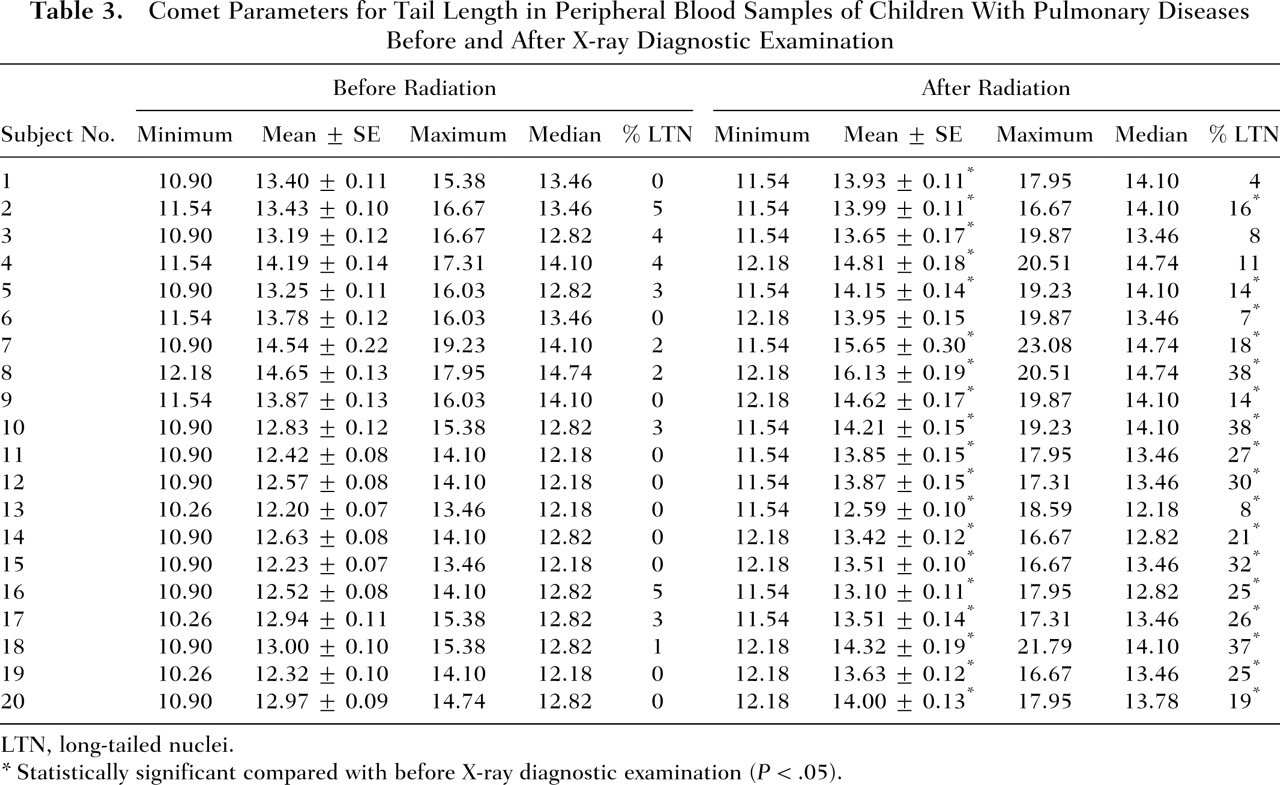
LTN, long-tailed nuclei.
Statistically significant compared with before X-ray diagnostic examination (P < .05).
Comet Parameters for Tail Intensity in Peripheral Blood Samples of Children With Pulmonary Diseases Before and After X-ray Diagnostic Examination
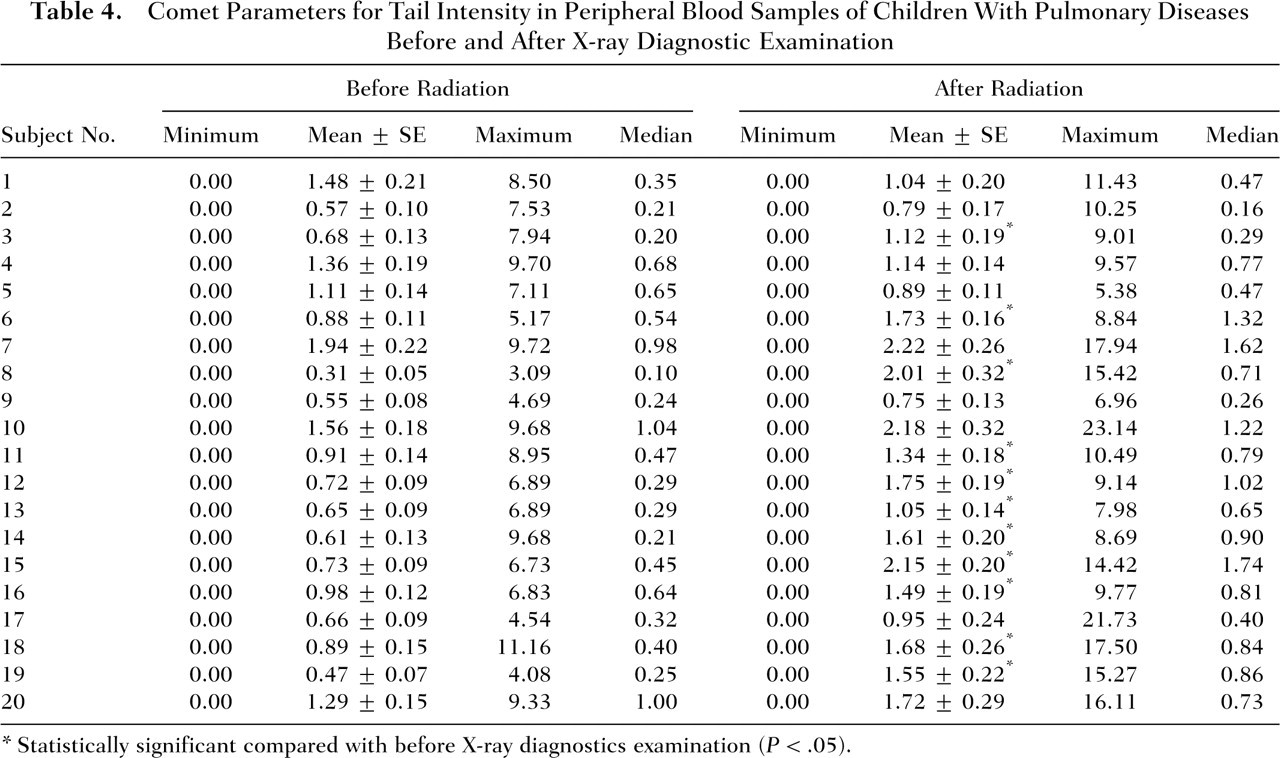
Statistically significant compared with before X-ray diagnostics examination (P < .05).
Comet Parameters for Tail Moment in Peripheral Blood Samples of Children With Pulmonary Diseases Before and After X-ray Diagnostic Examination
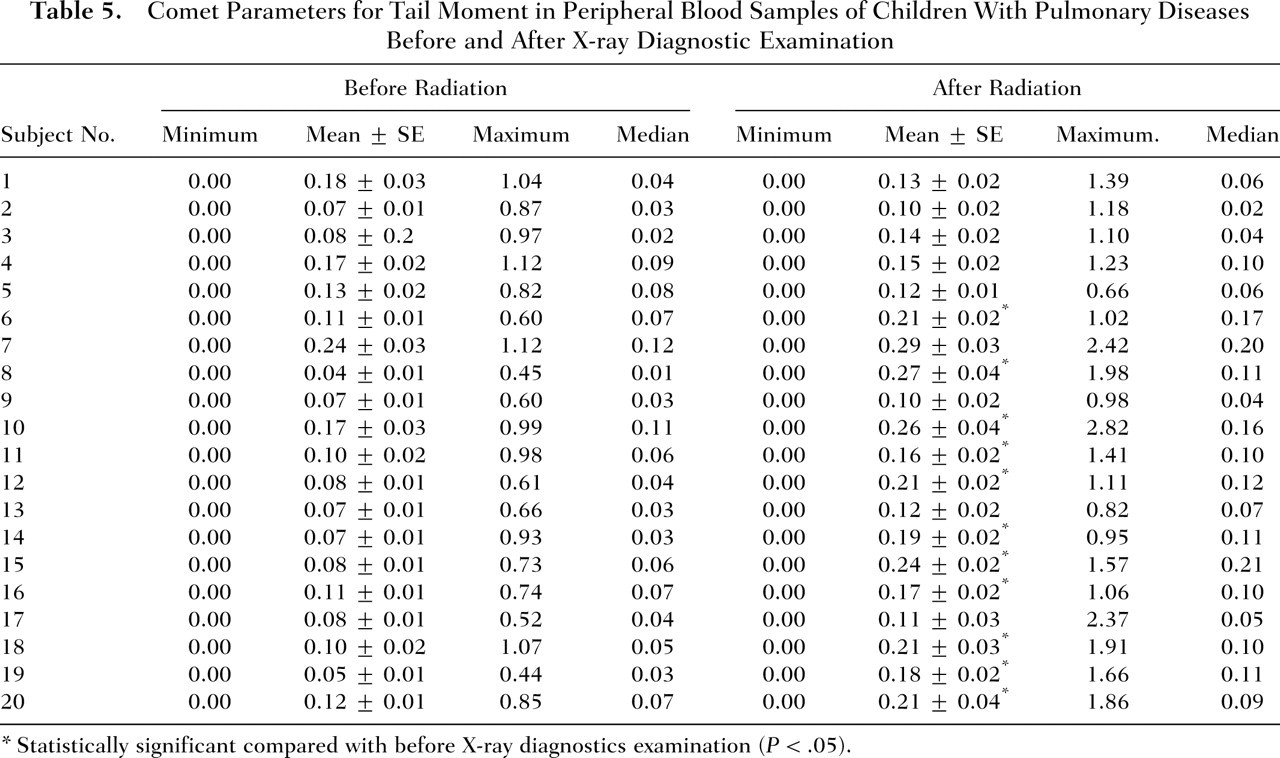
Statistically significant compared with before X-ray diagnostics examination (P < .05).
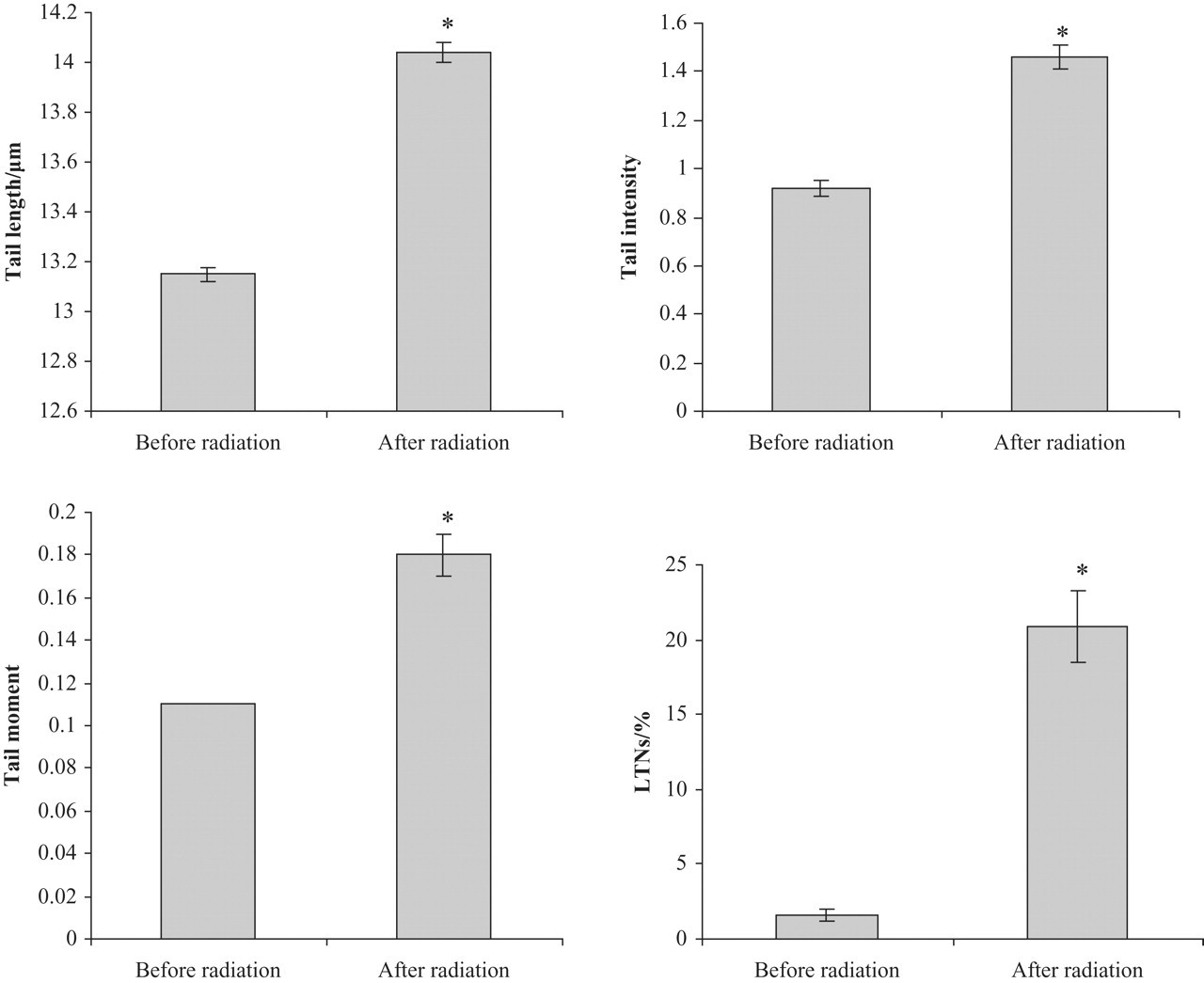
Mean group values for tail length, tail intensity, tail moment, and percentage of long-tailed nuclei in peripheral blood samples of children with pulmonary diseases before and after exposures to X-ray examination. *Statistically significant compared with before X-ray examination (P < .05).
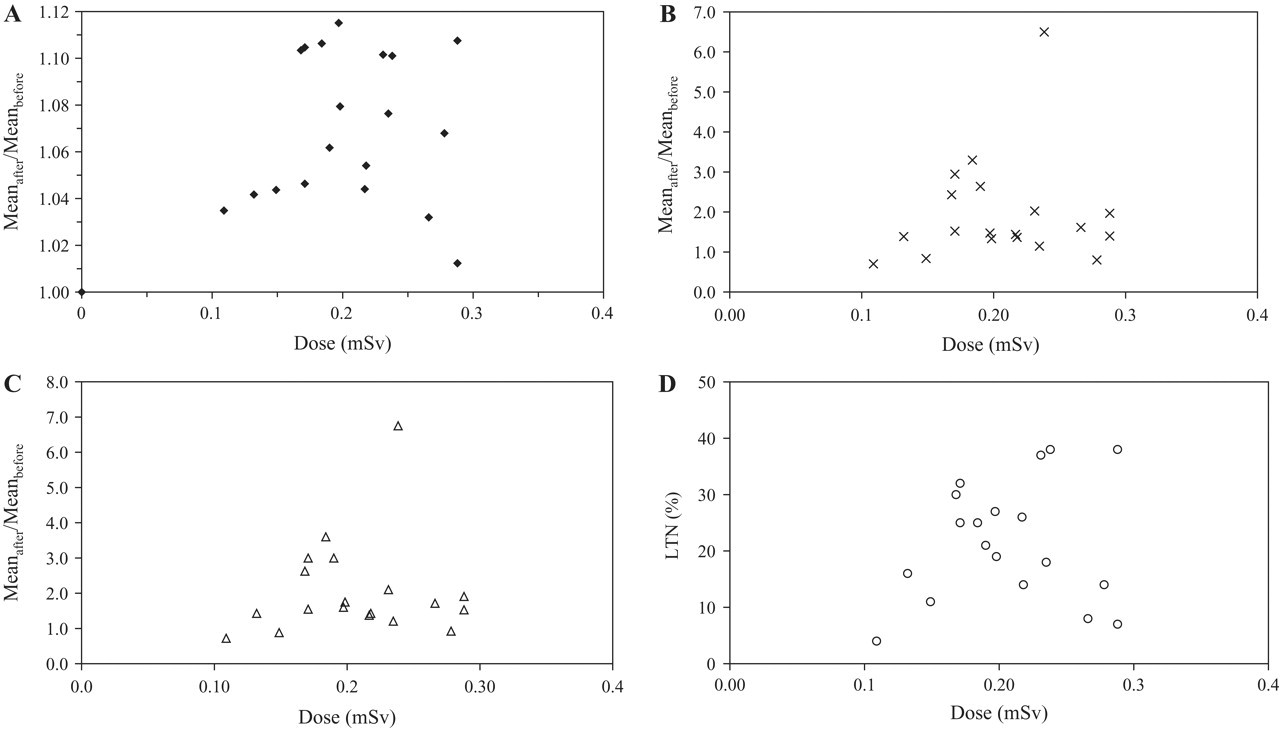
Ratio of (a) tail length, (b) tail intensity, and (c) tail moment after and before exposures and (d) long-tailed nuclei after exposures to X-ray diagnostics as a function of the entrance dose.
The X-radiation exposures measured on the back of 20 patients varied from 0.11 to 0.29 mSv, whereas X-radiation exposures measured on the sternum ranged from 0.01 to 0.04 mSv, expressed as Hp(10). Thyroid exposures ranging from 0.02 to 0.06 mSv were in good correlation with the back exposures and were on average 7 times lower. Exposures of gonads and forehead were even lower, ranging from 0.00 to 0.01 mSv. The exposures measured with TL and RPL dosimeters were in agreement within measurement uncertainty (differences within 0.01 mSv) as shown in Table 2, which corresponds to our earlier results. 37
Mean group values ± standard error of the mean of comet lengths were 13.15 ± 0.03 μm prior to the X-ray exposures and 14.04 ± 0.04 μm after X-ray exposures. The range of tail lengths before the exposures was 10.26 to 19.23 μm and 11.54 to 23.08 μm after X-ray exposures. Mean group values ± standard error of the mean for tail intensity were 0.92 ± 0.03 prior to the X-ray exposures and 1.46 ± 0.05 after the exposures. The range of tail intensity before the exposures was 0.00 to 11.16 μm and 0.00 to 23.14 after exposures. Mean group values ± standard error of the mean for tail moments were 0.11 ± 0.00 prior to the X-ray exposures and 0.18 ± 0.01 after the exposures. The range of tail moment before the exposures was 0.00 to 1.12 μm and 0.00 to 3.79 μm after exposures. All comets tail length values were classified by considering threshold levels indicating the comets with LTN. LTN represents the number of comets for each patient with tail length values higher than the 95th percentile of their distribution. Cells with tail length values below the cutoff value were classified as undamaged and those with higher values as damaged. Mean frequency of LTN comets before the exposures was 1.60 ± 0.42 and after the exposures 20.90 ± 2.40, whereas their individual values varied between 4% and 38% after the examination compared with values before X-ray exposure, which ranged from 0% to 5% and were dependent on the individual (Table 3). Differences between mean group tail lengths, tail intensity, tail moment, and LTNs were statistically significant (P < .05).
Discussion
Ionizing radiation plays a significant role in medical diagnostics and is frequently needed to diagnose diseases in pediatric patients. Good medical practice dictates that children be protected from unnecessary radiation. Recent data show that there is an increase in solid cancer risk for individuals who are exposed to radiation of 5 to 100 mSv. 43-47 Children are considerably more sensitive to the carcinogenic effects of ionizing radiation than are adults, and children have a longer life expectancy in which to express that risk. 48-51 Many cancers can be induced by radiation, and a linear dose-response has been noted for most solid cancers. 52-54 Risks of radiation-related cancer are greatest for those exposed early in life, and these risks appear to persist throughout life. 47,53,55
To evaluate possible DNA alterations after X-ray diagnostics of children with pulmonary diseases and to correlate results with dosimetry, we used the alkaline comet assay. The comet assay or single-cell gel electrophoresis assay is a rapid, sensitive, and relatively simple method for detecting DNA damage at the level of individual cells. 20,26,56 It combines the simplicity of biochemical techniques for detecting DNA single-strand breaks, alkali labile sites, and cross-linking with the single-cell approach typical of cytogenetic assays. Over the past decade, the comet assay has become a standard method for assessing genome damage with a variety of applications in genotoxicity testing, fundamental research in DNA damage, and repair as well as in population biomonitoring. 16,22,57-62 In this study, peripheral blood lymphocytes were chosen as a model system, as they were previously established as suitable biodosimeters that integrate the effects of exposure to exogenous and endogenous genotoxins. Lymphocytes are also favored because of their availability, convenient culture methods, and simplicity of sample collection. 63 The latter was particularly important in our study, as we were able to collect the blood samples from the patients using a minimally invasive procedure, without placing additional emotional or physical stress on the patients.
A number of studies support the concept that DNA is the crucial target of carcinogens and that mutations in tumor suppressor genes and oncogenes may lead to cancer. 64,65 It has often been postulated that cytogenetic end points in peripheral blood lymphocytes serve as reasonably reliable cancer predictors in epidemiology. 23,27 Cancer biomarkers should be validated for application in clinical trials of diagnostic procedures that have potential exposure to mutagens and carcinogens. 66,67 In this context, the application of this assay could be extended to the possible diagnostic use in cancer detection in pediatric, adult, and geriatric populations. 23,28,62,68,69
This study demonstrated that immediately after exposure to diagnostic X irradiation, several comet assay parameters (tail length, tail intensity, and tail moment) that are indirect measures of DNA damage were significantly changed. Long-tailed nuclei additionally indicated differences in DNA mobility between samples taken prior and after the exposures. The average number of LTN per subject as indicator of highly damaged DNA was significantly higher in the patients after diagnostic procedures, which is in accordance with our previous results on subjects exposed to diagnostic X-rays as well as with the studies done by He et al, 70,71 where the number of LTN was also higher in subjects exposed to X-rays, either as patients or occupationally. Qualitative (but not quantitative) correlation between the values of measured doses and the comet assay was observed. The ratio of DNA damage before and after irradiation suggests that X-ray diagnostic procedures could alter DNA and highlights the importance of minimizing pediatric exposure to X irradiation. The measured entrance dose range on 20 patients (0.11-0.29 mSv) is in good agreement with data reported in the literature. 5,13 The relatively large standard deviation is caused by a series of factors (irradiation conditions, patients' physical characteristics, work methods) that cannot be controlled in everyday work. To evaluate the real exposure of children to radiation, it is necessary to have a statistically relevant number of measurements, which was 20 in this work.
Today we are witnessing an increased demand in all diagnostic fields. The increased use of ionizing radiation in the diagnostic field carries risk. Our results show that genetic damage is induced by the radiation from a chest X-ray examination, which is considered to be the least harmful examination, if considering the dose as a surrogate for risk. According to Mitchel, 72 this also should be reevaluated.
These results demonstrate that there is significant potential for delayed effects to even the low level of radiation exposure resulting from diagnostic X-ray procedures and that the risk of conducting these procedures must be weighed against the benefits of the results obtained from the diagnostic X-rays. Methods such as the comet assay are useful in acute events where children are exposed to genotoxic agents. In addition, this method could be used for monitoring genetic damage in children who are often exposed to diagnostics or therapeutic procedures. It would be useful to conduct more research of pediatric diagnostics and treatment algorithms to minimize the potential damage and to maintain the optimal benefit for the young patients. This is especially important for the youngest age group. For now we have to keep the annual absorbed dose as low as possible, especially in early age, and conduct more research of the radiosensitivity time window.
Footnotes
Notes
Acknowledgments
We gratefully acknowledge the cooperation of all the volunteers who participated in this study.