
Abstract
Human papillomavirus (HPV) is a leading cause of preventable cancers, yet vaccination rates among children remain low in the United States, especially in rural and Hispanic/Latino communities. This study addresses the significant gap in HPV vaccination coverage in rural Washington State, where rates fall below national targets due to barriers like limited health care access, low awareness, and socioeconomic challenges. Hispanic/Latino communities in these areas face additional risks, including higher cervical cancer incidence and unique barriers to vaccination. To address these disparities, we applied an adapted Boot Camp Translation (BCT) approach within the PREVENT study, co-creating culturally tailored HPV vaccination messages and materials with English- and Spanish-speaking parents and caregivers. Through a collaborative process involving community members, health care providers, and researchers, we co-developed messaging and materials about HPV vaccination that emphasize its safety, effectiveness, and role in cancer prevention. The engagement approach led to positive shifts in vaccination intentions, particularly among Spanish-speaking participants, and identified key message themes and preferred dissemination channels such as patient mailers, text messaging outreach, live call outreach, educational website resources, and clinic materials. These findings underscore the value of community-engaged, culturally responsive interventions to address vaccine barriers and improve uptake in underserved populations. The adapted BCT model provides a scalable framework for developing effective and relevant health communication strategies, contributing to improved health equity and reduced cancer disparities.
Keywords
Human papillomavirus (HPV) is a common viral infection and a leading cause of several cancers, including cervical, oropharyngeal, anal, penile, vaginal, and vulvar cancers (Lewis et al., 2021). Each year, over 37,000 people in the United States are diagnosed with HPV-related cancers (CDC, 2024a). Vaccination against HPV is safe and effective, preventing up to 90% of these cancers when administered before exposure. Early vaccination, recommended for children ages 9–17, is therefore critical for long-term cancer prevention (CDC, 2024b; Kjaer et al., 2021).
Despite the vaccine’s proven safety and efficacy, HPV vaccination coverage in the United States remains suboptimal. As of 2022, fewer than 40% of children ages 9–17 had received at least one dose (Villarroel et al., 2024). In Washington State, vaccination rates fall well below the Healthy People 2030 goal of 80%, leaving many children at risk for preventable cancers (Washington Chapter of the American Academy of Pediatrics [WCAAP], 2023). Disparities are especially pronounced in rural communities, where vaccine coverage is 10–13 percentage points lower than in urban areas and HPV-related cancer rates are higher (Villarroel et al., 2024; WCAAP, 2023). Contributing factors include limited access to care, low awareness and knowledge of HPV, and socioeconomic barriers (Khalil et al., 2023).
Within rural and Hispanic/Latino communities, social trust and community cohesion play an important role in HPV vaccination uptake, while affordability, transportation, scheduling challenges, and access to reliable information remain significant barriers (Frietze et al., 2023; Roncancio et al., 2017). To address these challenges, several studies have explored innovative strategies such as text message-based interventions, which have proven effective in improving HPV vaccination completion among both Hispanic/Latino and low-income communities (Aragones et al., 2015; Kepka et al., 2011; McGlone et al., 2024; Wynn et al., 2021). These findings highlight the potential of novel health strategies to reduce disparities and expand access, particularly in underserved communities. The urgency of these efforts is underscored by persistent health inequities: Hispanic/Latino women experience a 36%–40% higher incidence of cervical cancer compared to non-Hispanic/Latino White women (American Cancer Society, 2024). Tailored communication strategies that leverage trust, cultural values, and community networks have been shown to strengthen vaccination uptake in these groups (Harrington et al., 2021).
Community-engaged approaches, such as Boot Camp Translation (BCT), have shown success in developing locally relevant and culturally appropriate health messages that improve vaccine awareness and uptake (Brewer et al., 2020). The effectiveness of the BCT approach in fostering community engagement and improving HPV vaccination attitudes has been previously documented (Brewer et al., 2020). BCT is a dynamic, collaborative process in which community members and health partners work together through ongoing dialogue to design health communication that reflects local cultural values and community preferences. Few interventions have specifically addressed the intersection of rurality and Hispanic/Latino heritage in HPV vaccine promotion, with recent studies highlighting the need for tailored approaches in these communities (Fernandez-Pineda et al., 2021).
To address this gap, our study used an adapted BCT approach within the PREVENT study to co-create HPV vaccination messages and materials with English- and Spanish-speaking parents and caregivers in rural Washington State. As the primary decision-makers for adolescent health, parents and caregivers play a critical role in shaping vaccination attitudes and uptake, particularly within Hispanic/Latino and rural communities (Colón-López et al., 2021). Their perspectives on cultural values, trusted information sources, and logistical challenges guided the development of messages tailored to family needs. This collaborative process aimed to generate community-informed strategies that enhance HPV vaccination awareness and improve higher vaccination rates in underserved populations.
Methods
Study Details
This community-engagement effort was part of the PREVENT study, a collaborative project between the University of Utah Huntsman Cancer Institute, the Kaiser Permanente Center for Health Research, and Sea Mar Community Health Centers—a large, multi-site federally qualified health center (FQHC) in Washington State. PREVENT (Practice-based Approaches to Promote HPV Vaccination in the Safety Net) is a National Cancer Institute–funded randomized trial. It tests low-cost automated and culturally tailored live reminders to increase HPV vaccination among adolescents in rural communities, aiming to reduce rural–urban disparities in HPV-related cancers. The study protocol was approved by the University of Utah Institutional Review Board (IRB #00161649). Verbal informed consent was obtained from all participants prior to the BCT activities. Spanish-speaking participants were assisted by a certified interpreter to ensure full comprehension of the project.
Study Population
Sea Mar operates 37 primary care clinics, serving over 320,000 patients across Washington. According to electronic health records, 40% of the patient population identified as Hispanic/Latino in 2023. Eligible participants were parents or caregivers of at least one child aged 9–18 who received care at Sea Mar and had medical record evidence of at least one previous vaccination (e.g., flu, MMR, DTAP). Inclusion criteria required English or Spanish language preference to ensure accessibility.
Participants were recruited through purposive sampling in collaboration with clinic staff, with the goal of enrolling 10–15 individuals per BCT session. Recruitment focused on parents and caregivers with moderate views on vaccination to encourage open and constructive dialogue. Participants received a $100 gift card for their involvement in the in-person meeting.
Study Procedures
A modified BCT approach was used to develop community-informed HPV vaccination messages and materials. BCT is a collaborative, iterative process in which community members and health partners co-create health communication tailored to local culture and preferences. The process typically involves in-person and virtual meetings, totaling 20–25 hours of engagement over 4–12 months. For this study, the BCT model was adapted to include one 5-hour in-person session and two 1-hour virtual follow-up calls, reflecting prior successful implementations by the research team. An overview of the BCT process is provided in Figure 1.
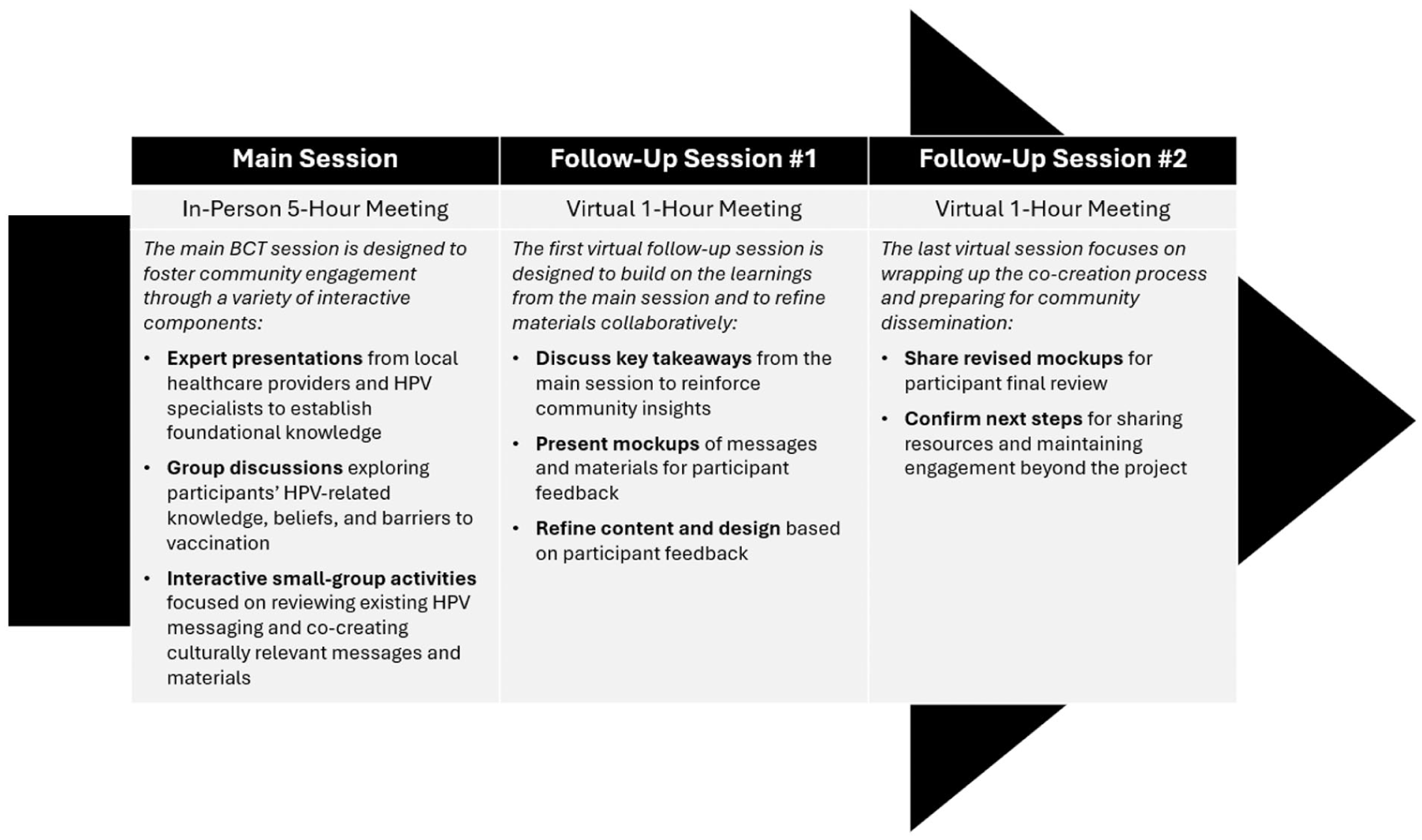
BCT Overview.
The initial in-person BCT meetings were held at two rural clinics: one in Aberdeen, Washington (English, February 17, 2024) and one in Bellingham, Washington (Spanish, March 2, 2024). Sessions included presentations from local health care providers and HPV experts, group discussions on HPV knowledge, beliefs, and barriers, and interactive small-group activities focused on message development and dissemination strategies. Review and discussion of existing HPV messaging served as a foundation for these activities.
Two follow-up virtual sessions (April 13 and July 20, 2024) allowed participants to review and provide feedback on draft materials, including suggestions on content, design, imagery, and delivery methods. Participants received a $25 gift card for each follow-up session.
Data Collection and Analysis
Field notes were collected during the in-person and virtual discussions to capture the diverse attitudes, beliefs, and preferences of English- and Spanish-speaking caregivers in rural Washington communities. The research team debriefed and outlined a summary of key learnings, with message themes formulated based on participant input. Participants shared their preferences on multiple aspects of existing materials, including content, layout, imagery, tone, message length, comprehension, and emotional impact. These insights directly informed the development of new messages and guided recommendations for effective delivery within the community. The BCT process was designed to ensure that the resulting HPV vaccination messages and materials were responsive to the unique needs of rural and Hispanic/Latino populations.
Pre- and Post-BCT Survey Responses
The study team developed brief pre- and post-BCT surveys specifically tailored to the project’s objectives (see Supplemental Appendix 1 and 2). To ensure language preference and cultural appropriateness, all surveys were administered in the language of the corresponding session, with English surveys used for English language sessions and Spanish surveys used for Spanish language sessions. The surveys were developed specifically to address the project’s goals. Survey items were informed by the team’s prior community-engagement work and reviewed for linguistic and cultural appropriateness by the research team and community advisors.
The eight-item pre-survey, designed to take 1–2 minutes, was completed in the morning following registration, while the post-survey, requiring 2–3 minutes, was administered at the end of the in-person session. The post-survey included 14 multiple choice and Likert-type-scale items, along with an open-ended prompt with general feedback. Both surveys were self-administered and distributed in hard copy format to participants during check-in. The surveys assessed participants’ HPV knowledge and attitudes, such as perceived importance of the vaccine, intent to vaccinate, and perceived barriers to HPV vaccination. For example, items included awareness of HPV and cervical cancer, knowledge of vaccine eligibility, and vaccination intent (e.g., “A vaccine to prevent HPV infection is available. Have you ever heard that cancer can be prevented by the HPV vaccine?” and “How likely are you to get the HPV vaccine for your child[ren] this year?”). Demographic information—including age, sex, race/ethnicity, education, income, insurance status, and employment—was collected exclusively on the post-survey. In addition, the post-survey included a session feedback section in which participants rated their experiences using a 5-point Likert-type scale (1 = Strongly Disagree to 5 = Strongly Agree). Items included statements such as: “Today’s session helped me understand the importance of the HPV vaccine.” These items captured participants’ perceptions of knowledge gained, clarity of communication, session pacing, respect, and overall satisfaction.
Results
Participants
A total of 24 adults participated in the in-person sessions, conducted in English and Spanish. Eighteen were parents and caregivers of children between the ages of 9–15, and their children had at least one vaccination. The remaining participants included four staff members and two health educators. The participants were divided into two language groups: the English language (EL) group, which included eight parents and two clinic staff, and the Spanish language (SL) group, consisting of 10 parents, 2 clinic staff, and 2 health promoters.
Educational attainment and socioeconomic characteristics varied across the groups. Overall, 66% of participants were high school graduates or higher, with significant variation between language groups (87% in the EL group versus 50% in the SL group). Only 17% of participants reported household incomes of $50,000 or greater, with the EL group showing a higher proportion (25%) compared to the SL group (10%). A higher percentage of the English group reported being employed (57.1%) compared to the Spanish group (40%). A significantly larger percentage of the Spanish language participants (70%) reported not having health-care insurance compared to the English language group (12.5%), which were primarily insured through public programs such as Medicare, Medicaid, or Washington Apple Health (62.5%). The English language session participants demonstrated diverse demographic characteristics. Approximately 37% of these individuals self-identified as Hispanic/Latino. The racial composition was diverse, comprising 25% American Indian/Alaska Native, 12.5% Asian, 25% Black/African American, and 62.5% White; total percentage exceeds 100% because individuals could identify with more than one race. The Spanish session was comprised of 90% Hispanic/Latino participants. Notably, all participants in both sessions identified as female.
Pre- and Post-Survey Responses
Most of the findings reported below are based on pre-survey responses collected during the in-person BCT sessions. Only one item—“How likely are you to get the HPV vaccine for your child(ren) this year?”—was included on both the pre- and post-surveys and is used to assess change in vaccination intent following the session.
The English session pre-survey indicated a high level of awareness among participants, with 87.5% familiar with HPV and 100% aware of cervical cancer. In addition, 87.5% recognized that the HPV vaccine can help prevent cancer. Regarding their children’s vaccination status, 50% reported their children had received the HPV vaccine, 25% said their children had not been vaccinated, and the remainder were unsure. The proportion of participants who were extremely likely or likely to vaccinate their children increased from 50% before the BCT session to 87.5% after the session, indicating a substantial shift toward stronger vaccination intent following the community-engagement session.
The Spanish session pre-survey results showed moderate awareness of HPV (60%) and cervical cancer (80%), with 70% aware that the vaccine can prevent cancer. Only 20% of participants reported that their children were vaccinated, while 50% said their children were not; the remainder either did not know or chose not to answer. Initial intentions to vaccinate were mixed: 30% were likely, 10% were neutral, 10% were unlikely, and 40% preferred not to answer. After the BCT session, the proportion extremely likely or likely to vaccinate increased from 30% to 60%, reflecting a more positive attitude and greater confidence toward HPV vaccination.
Both sessions demonstrated positive shifts in vaccination intentions, with the English session showing a more pronounced increase in those extremely likely to vaccinate. The results from the Spanish session suggest that the BCT session effectively addresses cultural barriers in health communication by increasing awareness through culturally appropriate and accessible health education.
Preferred Key Messages
The key messages from the BCT sessions emphasized the importance of reassuring parents about the safety and effectiveness of the HPV vaccine. Messages should emphasize the vaccine’s long-standing safety record, having been administered to millions of children worldwide since 2006. The emotional appeal to parents’ desire to protect their children’s future should be central, with phrases like “Protect your child’s future” resonating deeply. In addition, the connection between the HPV vaccine and cancer prevention must be highlighted, with messages such as “HPV vaccination is cancer prevention” underscoring the importance of the vaccine in protecting against six types of HPV cancers, and its effectiveness in preventing 90% of these HPV cancers. Participants also highlighted the significance of discussing the benefits of beginning vaccination at age 9, stressing that vaccinating before exposure to the virus, maximizes the vaccine’s effectiveness. Messages should address caregivers’ concerns about vaccine side effects and highlight the latest research, while also reassuring parents that it is “not too late” to vaccinate, and vaccination is beneficial up to age 26 and, depending on risk, up to age 45. The role of trusted health care providers is critical, with messaging being most effective when it comes directly from doctors and is tailored to individual concerns. Local statistics and community support can further strengthen the message, as can the option for parents to share information with family and friends. Finally, gender-neutral language should be consistently used to ensure both boys and girls are equally encouraged to receive the vaccine. Peer-to-peer messaging can encourage teens to discuss the vaccine, framing it as a means of mutual protection against HPV.
Preferred Dissemination Channels
Participants identified several channels for disseminating and receiving HPV vaccine messages and materials, including patient-friendly print materials, text message outreach, live call outreach, educational website resource, and in-clinic materials. First, a patient mailer—including a clear, introductory letter and an accompanying fact sheet about HPV vaccination—was recommended to deliver essential information directly to families in an accessible and understandable format. Second, text messages with links to short, animated videos and the ability to schedule vaccine appointments were viewed as efficient and engaging ways to reach parents. Third, both English and Spanish language groups highlighted the value of live phone calls from health care providers—particularly from a care coordinator—to answer questions and assist with appointment scheduling. These calls should emphasize the importance, safety, and benefits of the HPV vaccine, supporting parents and caregivers in making informed health decisions. Fourth, BCT participants expressed a preference for educational HPV vaccination websites that are easy to understand and accessible from mobile devices. Simple, dynamic websites were identified as effective tools for reaching both teens and busy parents, as well as for disseminating HPV vaccination information and resources. Finally, print materials (e.g., posters), especially those available in clinic settings such as lobbies, waiting areas, and patient rooms, were also seen as a strong option for delivering information.
While there were many similarities in the groups’ feedback, a few differences emerged. Spanish language participants placed more emphasis on including specific statistical details, such as the types of cancers prevented by the vaccine and wanted to provide more in-depth information on HPV strains and their prevalence. They also suggested providing posters for teenagers with the message “It’s not too late” to get vaccinated. The Spanish language group also highlighted the use of motivational interviewing techniques as an effective way to engage patients in decision-making in a respectful and supportive manner, addressing concerns while reinforcing the benefits of vaccination. Overall, both sessions agreed on the importance of safety, cancer prevention, early vaccination, clear communication, and respectful provider-patient interactions.
Final Co-designed Materials
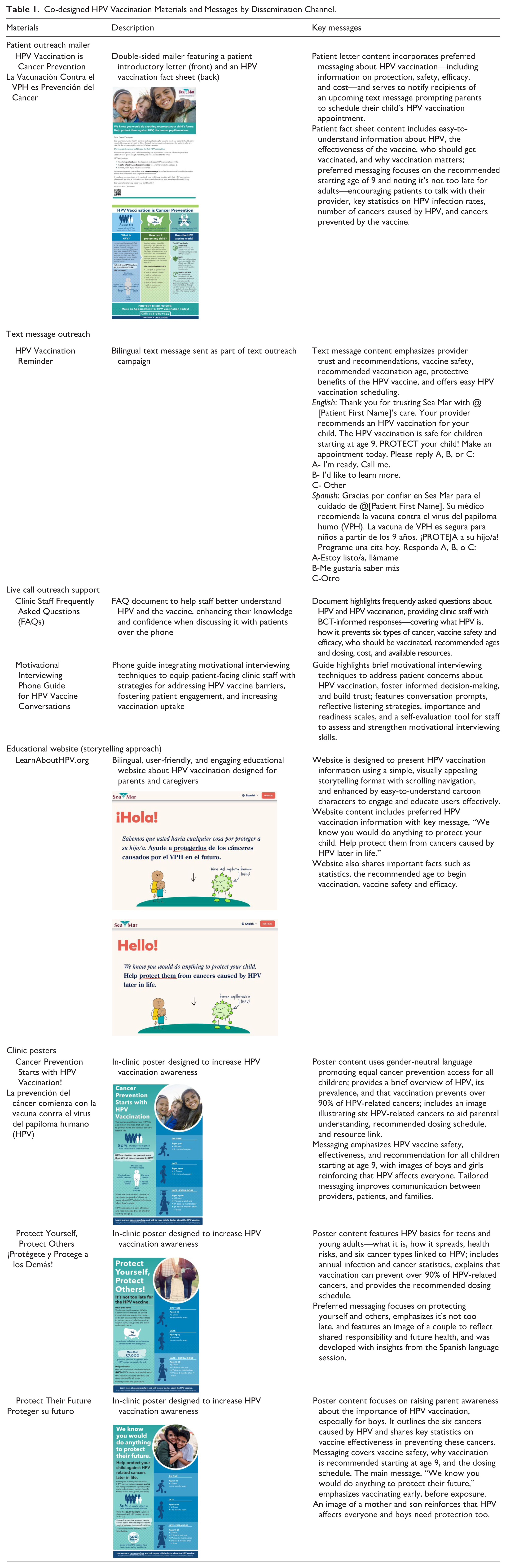
Guided by the preferred HPV vaccination messaging themes identified by BCT participants, our team collaboratively co-designed a set of materials to promote and increase HPV vaccination uptake in rural communities throughout Washington State (Table 1). We solicited feedback on draft materials and concepts, then refined these materials during two follow-up virtual sessions, each involving a subset of participants from the initial in-person BCT meetings. The finalized materials will be utilized in the main PREVENT trial intervention. All materials are publicly available at: www.PreventHPVCancers.com.
Co-designed HPV Vaccination Materials and Messages by Dissemination Channel.
Evaluation of Modified BCT Sessions
The evaluation of both the English and Spanish sessions revealed high levels of participant satisfaction and effectiveness in conveying information about HPV and its vaccine.
In the English session, all participants rated their satisfaction as either "extremely satisfied" (9 or 10 on the scale) or "very positive." Participants unanimously agreed that the facilitators communicated clearly and maintained an appropriate pace, making the information easily understandable. The session was particularly effective in enhancing participants’ understanding of the HPV vaccine’s importance. All participants reported a sense of accomplishment and felt they had gained valuable knowledge about HPV and the vaccine.
Similarly, the evaluation of the Spanish session revealed highly positive outcomes. Sixty percent of participants reported being "extremely satisfied" with the session, while the remaining attendees also provided favorable ratings. An impressive 90% agreed that the facilitators communicated clearly, making the information easy to understand. All participants agreed that the session’s pace was appropriate. Furthermore, 80% indicated that their understanding of the importance of the HPV vaccine had improved, and 70% strongly agreed that they gained valuable information and felt a sense of accomplishment as a result of their participation.
Both sessions fostered an environment of mutual respect, with most participants in both groups agreeing that differing viewpoints were respected. Overall, these results indicate that both the English and Spanish sessions were highly successful in engaging participants, respecting diverse opinions, and effectively conveying crucial information about HPV and its vaccine. The positive outcomes were consistent across both groups, suggesting the effectiveness of this community educational approach in different cultural contexts.
Discussion
This study offers valuable new insights into the effective delivery of HPV vaccination messages in rural communities, with a particular emphasis on Hispanic/Latino families. By engaging parents and caregivers through a modified BCT process, we co-created messaging and educational materials that directly address the unique barriers and motivators within these populations.
Providers reported a slight uptick in vaccination numbers after the BCT sessions which, while not conclusive, suggests a positive impact of the engagement approach. This observation aligns with prior research, including a systematic review by Escoffery and colleagues, which found that community-engaged and culturally tailored interventions can increase HPV vaccination uptake (Escoffery et al., 2023). Consistent with earlier studies of community-based participatory approaches, our findings underscore the potential of partnership-driven materials to address health disparities and improve vaccination outcomes in underserved populations through non-traditional delivery formats (Christy et al., 2023; Niccolai & Hansen, 2015). By identifying evidence-based methods to develop HPV vaccination materials that promote community-centered solutions, this research takes an important step toward reducing disparities in HPV vaccination rates and cervical cancer incidence.
Our results highlight several key findings. First, both English- and Spanish-speaking participants demonstrated increased willingness to vaccinate their children against HPV following the BCT sessions, with the most pronounced shift among English language participants and a notable increase in engagement among the Spanish group. This suggests that culturally and linguistically tailored, community-engaged messaging can meaningfully shift attitudes and intentions, even among groups with initially moderate or uncertain views about vaccination.
Second, the study revealed important differences between English- and Spanish-speaking caregivers in baseline knowledge, concerns, and communication preferences. Spanish-speaking participants started with lower awareness of HPV and the vaccine’s cancer-prevention benefits but expressed a strong desire for detailed, specific information about the cancers prevented and the scientific evidence supporting vaccine safety. They also valued motivational interviewing and respectful, supportive communication from providers. English-speaking participants, meanwhile, focused more on general vaccine safety, efficacy, and the emotional appeal of protecting their children’s future. Both groups agreed that messaging should emphasize the vaccine’s safety record, its cancer-prevention role, the importance of early vaccination, and the use of clear, gender-neutral language.
Third, a unique contribution of this study is the identification of trusted and practical dissemination channels for rural settings. Participants from both language groups endorsed a multi-modal approach, including patient mailers, text messages with website links, live phone calls from trusted clinic staff, educational websites, and clinic materials. Spanish-speaking caregivers especially valued materials that could be shared with extended family and community members, as well as direct conversations with bilingual coordinators for questions and appointment assistance. These findings highlight the importance of flexible, accessible communication strategies that extend beyond traditional clinic-based approaches.
Several limitations should be acknowledged. Participant attrition limited the final sample size, which may affect the generalizability of our findings. The study was conducted in only two rural clinics in Washington State, so results may not represent all rural or Hispanic/Latino communities nationwide. In addition, the low participation of fathers may have influenced the perspectives captured. Finally, the surveys were not adapted from existing validated instruments, as they were tailored to the project’s goals of message development. As such, psychometric properties (e.g., reliability) were not calculated.
These findings hold important implications for practitioners and health educators. First, HPV vaccination efforts in rural, Hispanic/Latino-serving clinics should prioritize bilingual, culturally responsive materials that integrate both scientific evidence and motivational narratives. Second, dissemination strategies should incorporate multiple delivery modes—particularly text message reminders, phone calls from trusted staff, and family-shareable educational materials—to reach households with varied information preferences and ensure broader message penetration within extended family networks. Finally, health systems working in rural areas should invest in training bilingual coordinators and community health workers, who may serve as vital cultural brokers and trusted intermediaries.
Future research should focus on recruiting parents of younger children, particularly those aged 8 to 10, to better understand barriers to early vaccination. It is also important to evaluate the effectiveness of BCT-developed materials on HPV vaccination rates and to expand this approach to other rural and minority communities. Furthermore, investigating the cost-effectiveness of community-engaged health communication strategies will be critical. This study highlights the ongoing tension between evidence-based practice and patient-centered care, particularly for non-native English-speaking populations in rural areas. The outcomes of this BCT process may inform the development of robust messaging frameworks for future interventions, ensuring that diverse patient populations receive the information they need to make well-informed decisions about HPV vaccination.
Supplemental Material
sj-docx-1-heb-10.1177_10901981251399649 – Supplemental material for Co-creating HPV Vaccination Messages for Rural Washington: Application of a Boot Camp Translation Approach
Supplemental material, sj-docx-1-heb-10.1177_10901981251399649 for Co-creating HPV Vaccination Messages for Rural Washington: Application of a Boot Camp Translation Approach by Jamie H. Thompson, Jennifer S. Rivelli, Priyanka Gautom, Amanda F. Petrik, Matthew Najarian, Anna C. Edelmann, Ludy Villegas, Rebecca Slagle, Kaila Christini, Gloria D. Coronado and Deanna Kepka in Health Education & Behavior
Supplemental Material
sj-docx-2-heb-10.1177_10901981251399649 – Supplemental material for Co-creating HPV Vaccination Messages for Rural Washington: Application of a Boot Camp Translation Approach
Supplemental material, sj-docx-2-heb-10.1177_10901981251399649 for Co-creating HPV Vaccination Messages for Rural Washington: Application of a Boot Camp Translation Approach by Jamie H. Thompson, Jennifer S. Rivelli, Priyanka Gautom, Amanda F. Petrik, Matthew Najarian, Anna C. Edelmann, Ludy Villegas, Rebecca Slagle, Kaila Christini, Gloria D. Coronado and Deanna Kepka in Health Education & Behavior
Supplemental Material
sj-docx-3-heb-10.1177_10901981251399649 – Supplemental material for Co-creating HPV Vaccination Messages for Rural Washington: Application of a Boot Camp Translation Approach
Supplemental material, sj-docx-3-heb-10.1177_10901981251399649 for Co-creating HPV Vaccination Messages for Rural Washington: Application of a Boot Camp Translation Approach by Jamie H. Thompson, Jennifer S. Rivelli, Priyanka Gautom, Amanda F. Petrik, Matthew Najarian, Anna C. Edelmann, Ludy Villegas, Rebecca Slagle, Kaila Christini, Gloria D. Coronado and Deanna Kepka in Health Education & Behavior
Footnotes
Acknowledgements
We gratefully acknowledge the support of Sea Mar Community Health Centers for their partnership in this project. Sea Mar served as the primary performance site for this work, and their commitment to community health and collaboration was instrumental in the successful implementation of the study. We especially thank the staff and patients who contributed their time, insights, and lived experiences to co-create culturally relevant HPV vaccination messages and materials. We also thank Stephen Gubler for project management assistance at the beginning of this study, specifically during the community-engagement work.
ORCID iDs
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The PREVENT study (Practice-Based Approaches to Promote HPV Vaccination), led by Principal Investigator Deanna Kepka at the University of Utah, is funded by the National Cancer Institute (NCI) of the National Institutes of Health (NIH) under grant number 1R01CA279973. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. No additional external funding was received for this study.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Deanna Kepka has worked as a consultant for Merck. Other authors have no financial disclosures or conflicts of interest.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.