
Abstract
Approximately 11.3% of the U.S. population has diabetes, mostly type 2 diabetes (T2DM), and maintenance of A1c levels is vital to prevent complications among patients. Perceived discrimination in medical care settings (PDMS) affects patient care, while social support may mitigate its impact. This study aims to explore the influence of PDMS on A1c levels in T2DM patients using the All of Us Research Program, which collects health data from diverse individuals across the United States. Our study included 135 T2DM-diagnosed participants. Measures included demographic info, A1c data, self-rated health, social support, and perceived discrimination. Descriptive and multivariable regression analyses were conducted. Participants were predominantly older, female, non-Hispanic White, and had relatively high levels of education and above-average income levels. Most rated their health positively. Social support, including marital status, was considered. The average A1c level was 6.72 ± 1.54. Notably, 42% experienced high PDMS, correlating with poorer self-rated health. Multivariable regression revealed significant associations between A1c and follow-up time, age, marital status, and PDMS. Specifically, PDMS significantly correlates with poorer A1c, indicating a potential impact on diabetes management. Findings emphasize the need for tailored interventions and anti-discrimination guidelines in clinical practice. Insights from this study inform interventions mitigating discrimination and enhancing diabetes care. Health care providers fostering inclusive environments can improve patient trust and adherence to treatment, leading to better outcomes. Cultivating inclusive environments through health care providers improves patient outcomes. Diverse population inclusion in future studies is crucial.
Introduction
Approximately 38 million of the U.S. population has diabetes, and approximately 90%–95% of all diagnosed cases in adults are type 2 diabetes (T2DM) (Centers for Disease Control and Prevention [CDC], 2024). In addition to daily diabetes self-management, regular follow-up, and medication adherence are also important. As a chronic disease with many contributing factors, diabetes can be hard to manage and requires lifelong ongoing self-regulation behaviors to prevent debilitating complications such as neuropathy, nephropathy, cardiovascular disease, or blindness (Adu et al., 2019; American Diabetes Association Professional Practice Committee, 2024a).
Maintaining an ideal hemoglobin A1c level is the gold standard for diabetes care (American Diabetes Association Professional Practice Committee, 2024b). A1c is a measurement that reflects average blood glucose levels over the most recent 3-month period. The A1c goal for most people with diabetes is 7% or less, and higher A1c levels are linked to diabetes complications (American Diabetes Association Professional Practice Committee, 2024b). Maintaining A1c levels within an ideal range requires daily self-management, including regular physical activity, selecting an appropriate diet and meal preparation, adherence to medication prescriptions, regular follow-up with health care providers, and self-monitoring the signs and symptoms of hyper/hypo glycemia. To attain these outcomes, health care and social support are crucial (American Diabetes Association Professional Practice Committee, 2024a). Moreover, perceived discrimination in medical care settings (PDMS) may negatively affect patients’ overall health, diabetes care, and management (Benjamins & Middleton, 2019).
PDMS is a significant issue, encompassing an individual’s subjective experiences of unfair treatment or bias based on various factors such as race, ethnicity, gender, religion, or disability within the context of receiving medical care (Hill-Briggs et al., 2020). Existing research has consistently linked experiences of PDMS to adverse health outcomes, particularly affecting psychological well-being (Byrd, 2012; Li et al., 2022). PDMS directly heightens stress responses and impacts individuals’ mental and physical health outcomes (Forde et al., 2021; Lewis et al., 2014; Li et al., 2022). Studies have shown correlations between PDMS and increased levels of anxiety, depression, and other mental health issues among affected individuals (Basiri et al., 2023).
Despite the wealth of research on the impact of PDMS on psychological health, there remains a noticeable gap in understanding its influence on individuals’ health and health care needs (Riley, 2012). Prior research has reported that perceived PDMS contributes to patients’ underutilization of health care services (Burgess et al., 2008; Washington & Randall, 2023), failure to follow medical advice (Casagrande et al., 2007), and delayed or unmet health care needs (Benjamins & Middleton, 2019). Health care non-adherence related to PDMS profoundly impacts chronic disease self-management outcomes. Patients who perceive discrimination are less likely to follow medical advice, access health care services, or seek timely care. This non-adherence can result in poorer health outcomes, increased complications, and a greater burden on the health care system (Howren & Gonzalez, 2016). However, there is limited understanding on how experiences of discrimination within health care settings affect self-management behaviors, health care utilization, and clinical outcomes, such as A1c levels, in patients with diabetes.
Patient’s relationships with health care providers influence patients’ disease management and health outcomes (Marzban et al., 2022). To enable patients to have relevant skills and feel confident in carrying out daily practice, a productive relationship between patients and health care providers is necessary for patients to feel comfortable to discuss their questions and concerns (Molina-Mula & Gallo-Estrada, 2020). This enables patients to learn and practice diabetes self-management skills, and to feel confident in carrying them out. A trusting and therapeutic relationship is key to improved communications, shared decision-making, and patients’ satisfaction and quality of care (Sharkiya, 2023). PDMS may hinder patients’ diabetes management behaviors and further impact individuals’ health outcomes. Experiencing discrimination can compound diabetes-related stress, exacerbating poor health outcomes (McLaurin et al., 2024). For instance, a population-based study in patients with diabetes reported that individuals who reported PDMS were more than twice as likely to rate their quality of care as “fair” or “poor.” These individuals also reported feeling they did not have enough time with their physicians and were less involved in decision-making regarding their care. Perceived discrimination was prevalent across various health settings and among different providers and staff, contributing to poorer overall health care experiences and outcomes (Benjamins & Middleton, 2019).
Social support is associated with diabetes-specific self-management behaviors, better physical health outcomes, and improved mental health (Werfalli et al., 2020). A systematic review of 37 studies involving individuals with T2DM found that those with greater social support demonstrated improved A1c levels, blood pressure, and lipid levels. In addition, they experienced fewer symptoms of depression and less diabetes-related distress (Strom & Egede, 2012). Social support includes instrumental support and emotional support. Instrumental support refers to practical assistance, such as financial aid, transportation, and help with tasks addressing immediate needs and challenges. Emotional support involves offering empathy, care, and reassurance, helping individuals feel valued and better manage stress. Both types of social support have been associated with patients’ mortality rates, disease complications, and overall health. In addition, they are reported to have a positive or buffering effect, reducing the impact of perceived discrimination on negative health outcomes (Acoba, 2024).
Despite increasing awareness of PDMS, its impact on A1c outcomes in patients with T2DM remains unexplored. This study aims to examine how perceived discrimination influences A1c levels, while accounting for demographic and social support factors among individuals with T2DM. Using data from the National Institutes of Health (NIH) All of Us Research Program participants can help health care professionals better understand gaps related to the burden of diabetes management and care. Understanding gaps in research is crucial, given the prevalence and significant burden of diabetes globally. By investigating the relationship between PDMS and diabetes care outcomes, researchers can better address the barriers and challenges faced by patients with diabetes in health care settings.
Methods
All of Us Program and Sample Selection
The study participants were from the All of Us Research Program, a program led by the NIH, which aims to gather health data from one million or more diverse individuals in the United States to accelerate research discoveries and improve human health. The program is unique in its emphasis on relationship building and diversity including race & ethnicity, gender identity, geography, income, disability, and a variety of other factors (Ramirez et al., 2022). As of this study, the program had recruited over 568,000 participants who completed the program’s initial steps, including consent, sharing electronic health records (EHR), surveys, physical measurements, and biospecimen donation. Approximately 45% of participants were racial and ethnic minorities: 52.3% White, 16.67% Black or African American, 16.3% Hispanic, Latino, or Spanish, 7.0% reported multiple races/ethnicities, and 3.3% Asian (All of Us Research Hub, 2024).
The inclusion criteria for this study comprised All of Us participants who: (1) were diagnosed with T2DM; (2) were aged 18 years or older; (3) had A1c data ranging from 4% to 15% in the EHR; and (4) completed the PDMS scale. Figure 1 depicts the final analysis sample after exclusions, totaling 135 individuals with T2DM. Data analysis was conducted between October 2023 and April 2024.
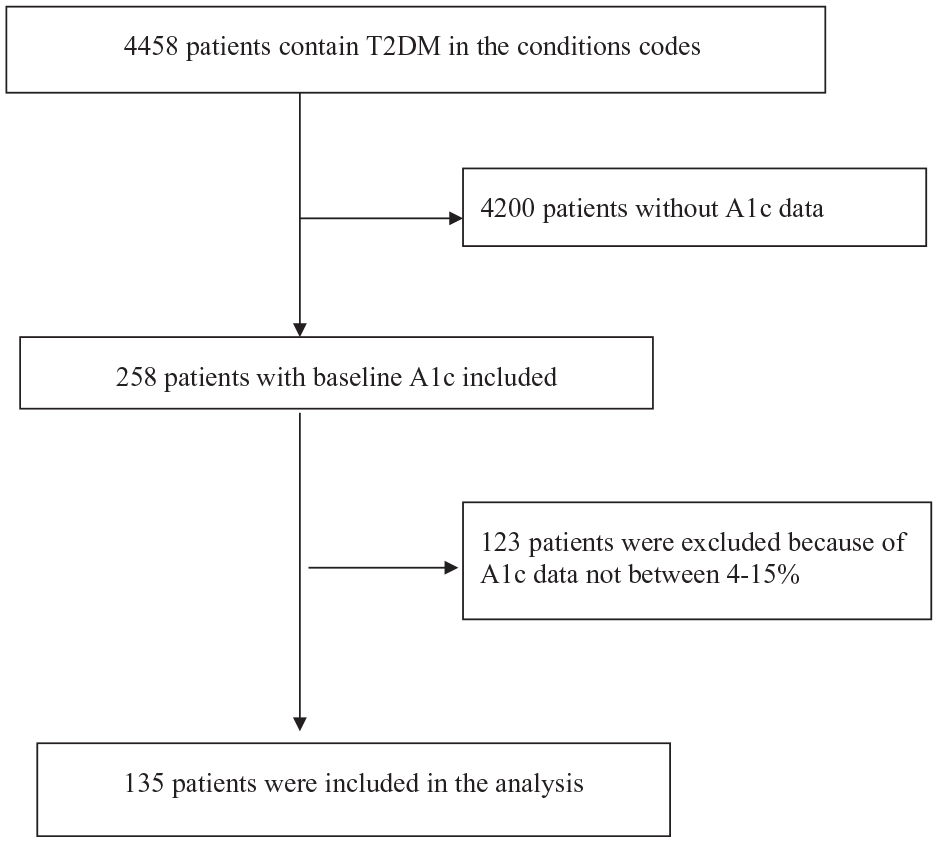
Consort Diagram of Patient Flow From the All of Us Research Program.
Measures
Demographic data encompassed race, gender identity (male, female, or other, including non-binary, transgender, and prefer not to answer), age, education (college graduate or above vs. high school or below), marital status (married or partnered vs. single or not partnered), employment status (employed vs. unemployed), and income. Age was analyzed as a continuous variable.
A1c measurements were retrieved from EHR, reported in varied units. To prevent conversion errors, the complete A1c range (4%–15%) was included. Follow-up time was reported in months and was computed based on multiple A1c checks recorded in the EHR. The months were represented by M: 88.91 ± 65.03, median: 75.73, interquartile range (IQR): 35.89, 135.28.
Self-rated health: Self-rated health (SRH) was assessed using a single question: “How would you rate your overall health at present?” Responses ranged from 0 = excellent to 4 = poor, with lower scores indicating better SRH. We dichotomized responses: scores 0–2 as “good” SRH, and 3 and 4 as “fair/poor” SRH.
Social support: Social support was assessed by using a modified measurement from the Medical Outcomes Study Social Support Survey (MOS-SS) which consisted of 19 items. The modified MOS-SS (mMOS-SS) used the first eight items from the classic MOS-SS with two subscales: Instrumental (Items 1–4) and emotional (Items 5–8). This measure has demonstrated good reliability for both subgroups and good validity (Moser et al., 2012). The score for mMOS-SS is calculated as the average score of subscale items transformed to a 0–100 scale, with higher scores indicating more support. The α in this study for Instrumental Support is .91, and .90 for Emotional Support, which indicates good reliability.
Perceived Discrimination in Medical Settings: PDMS was assessed using a seven-item instrument designed to measure experiences of disrespect, poor treatment, and feelings of being disregarded during health care encounters (Peek et al., 2011). The items included are (1) You are treated with less courtesy than other people?; (2) You are treated with less respect than other people?; (3) You receive poorer service than others?; (4) A doctor or nurse acts if he or she thinks you are not smart; (5) A doctor or nurse acts as if he or she is afraid of you; (6) A doctor or nurse acts as if he or she is better than you,; and (7) You feel like a doctor or nurse is not listening to what you were saying. Responses were rated on a 5-point Likert-type scale. The total score ranges from 7 to 35, with higher scores indicating greater perceived discrimination. This measure demonstrated good reliability (α = .82) in our study. A cutoff mean of 9 was used to categorize participants into high (score > 9) and low (score ≤ 9) discrimination groups for comparison of study variables. However, PDMS was treated as a continuous variable in univariate regression analysis to assess the magnitude of its effect on A1c levels.
Statistical Analysis
Descriptive statistics were computed for demographics, social support, A1c, and perceived discrimination. Categorical variables were expressed as count and frequency, and continuous variables as mean, standard deviation, and range. Pearson’s Chi-square and Wilcoxon rank-sum tests compared variables based on PDMS scores. Univariable regression analyzed each demographic variable, SRH, social support factors, and PDMS for A1c. Variables with p < .2 were included in multivariable regression (using gls function in R), considering p ≤ .05 significant. Two multivariable linear regression models for A1c were conducted to examine A1c levels. The first model included follow-up time, age, education, marital status, SRH, and emotional social support as predictive variables. The second model added PDMS variables to assess their influence on A1c. Interaction with follow-up time was assessed. All analyses were conducted using the Jupyter application on the All of Us Workbench within the R software environment.
Results
The study comprised 135 participants. On average, participants were older adults (mean age: 66.69 years), with 54.81% female, and predominantly non-Hispanic White (88.8%). Most held a bachelor’s degree or higher (61.5%), and approximately 63% were unemployed. Nearly 75% reported an annual income exceeding $50,000, and 66.67% rated their health as good, very good, or excellent. The average level of received Instrumental support and Emotional support were 68.87 ± 30.26 and 69.21 ± 26.99, respectively. The average A1c level was 6.72 ± 1.54. Most participants (66.67%) self-rated their health as “good,” “very good,” or “excellent,” and most (63.7%) reported being married. There were 57 (42%) participants categorized in the high-PDMS group. When comparing the participant characteristics between the two groups, individuals in the higher PDMS group reported lower annual incomes (less than $50,000), lower social support, and higher A1c levels. However, these factors did not reach statistical significance. Participants who reported higher levels of PDMS also had a higher percentage of reporting SRH as poor or fair (p = .006) (see Table 1).
Descriptive Characteristics of Sample by PDMS (N = 135).
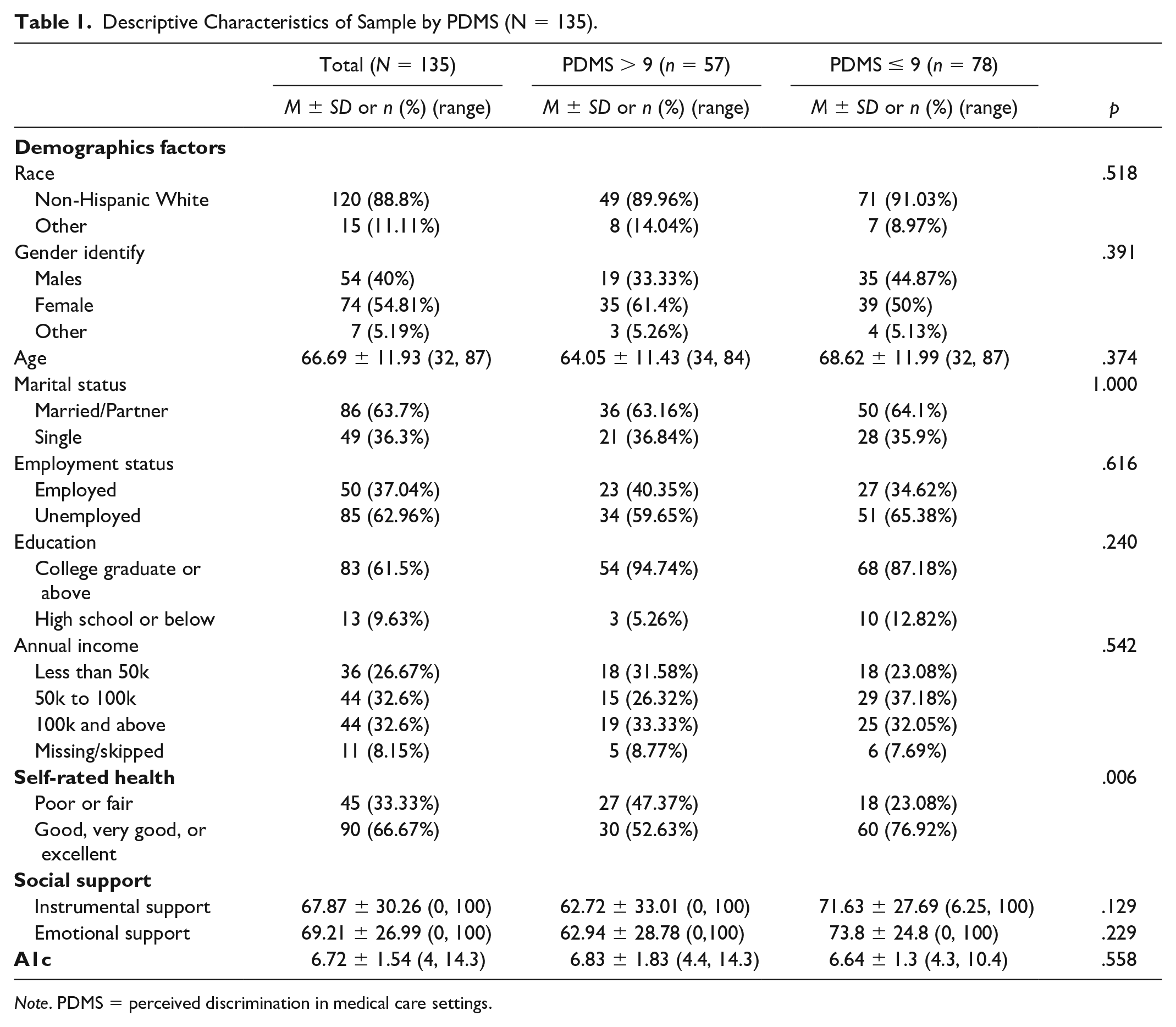
Note. PDMS = perceived discrimination in medical care settings.
Table 2 displays the outcomes of multivariable longitudinal regression analysis for A1c. In the initial model (Model 1), significant variables included follow-up time, age, and marital status. Longer follow-up durations were associated with elevated A1c levels across all age groups (β = .03, p < .001). Younger individuals (β = −.025, p = .002) and those unmarried or unpartnered (β = −.702, p = .001) showed higher A1c levels. In the subsequent model (Model 2), these variables retained significance (β = .03, p < .001; β = −.025, p = .002; and β = −.025, p = .002, respectively). In addition, PDMS significantly predicted A1c levels. Participants reporting more discrimination experiences in health care settings exhibited higher A1c levels (β = .049, p = .047); each additional point in perceived discrimination corresponded to a 0.049% increase in A1c levels on average.
Multivariable Regression of A1C Using Social Demographics and PDMS (N = 135).
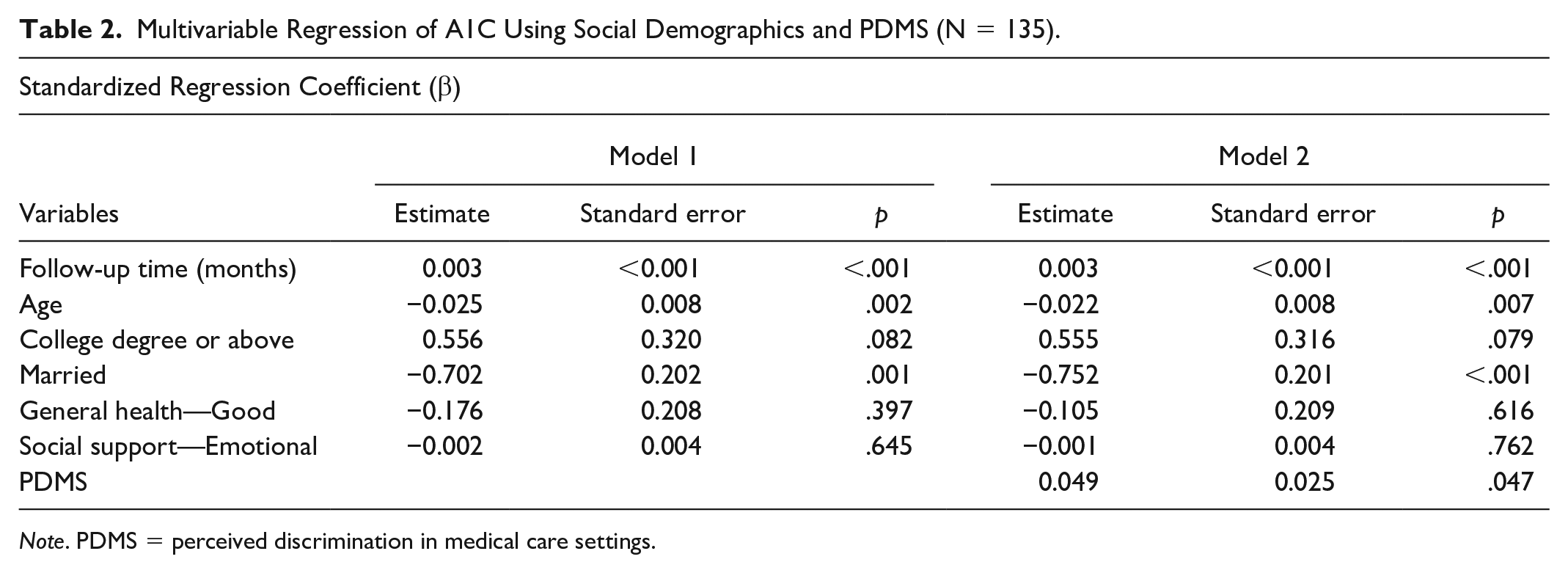
Note. PDMS = perceived discrimination in medical care settings.
Discussion
With the rising prevalence of T2DM and its consequent strain on communities and health care systems worldwide, this study investigates the influence of PDMS and social support on A1c levels. The findings illuminate the adverse impact of PDMS on diabetes management, revealing a significant correlation with poorer A1c outcomes. In addition, the study emphasizes the critical role of health care providers in fostering environments characterized by inclusivity and respect. Such environments cultivate heightened patient trust, enhance adherence to treatment regimens, and ultimately contribute to improved outcomes in diabetes management.
In our study’s descriptive analysis, 42% of participants were categorized as experiencing elevated levels of PDMS. Notably, individuals who reported heightened discrimination in medical environments also exhibited a higher prevalence of SRH categorized as “poor” or “fair.” These findings resonate with population-based research, wherein 40% of participants reported encountering diverse forms of discrimination in medical contexts (Benjamins & Middleton, 2019), with such experiences correlating with poorer SRH (Misra & Hunte, 2016).
In the regression analysis, younger age, single or unpartnered status, and heightened PDMS emerged as significant predictors of higher A1c levels among participants. This observation aligns with previous research indicating that young to middle-aged adults encounter greater difficulties in diabetes self-management (Adu et al., 2019), as these life stages often coincide with heightened stress stemming from professional, social, and familial obligations, which may divert attention from disease management (McCoy et al., 2019; Qin et al., 2020). Furthermore, extant literature suggests that individuals in marital or cohabiting relationships exhibit lower A1c levels compared to single counterparts (Ford & Robitaille, 2023). This disparity may be attributed to the emotional and practical social support offered by partners. For instance, partners may encourage healthy lifestyle choices, facilitate regular physical activity, and promote adherence to medication regimens, all of which are conducive to managing A1c levels effectively (Ford & Robitaille, 2023; Gerwitz et al., 2023).
Furthermore, our study revealed that PDMS significantly predicts A1c levels even after accounting for demographic variables and social support factors. This finding is consistent with prior research indicating that patients who perceive efficacy in patient-physician interactions and report fewer instances of discrimination tend to exhibit better A1c levels (Qu et al., 2022). These outcomes may be attributed to factors such as inadequate time spent with health care providers and limited involvement in decision-making processes, as reported in previous studies (Adu et al., 2019).
While our study did not delve into the specific types of discrimination experienced in medical settings, existing literature indicates that racial/ethnic discrimination is notably associated with unfavorable diabetes management behaviors (Hill-Briggs et al., 2020). These include poorer overall dietary habits, reduced adherence to specific dietary recommendations, diminished quality of life, lower rates of A1c checks, foot exams, and blood pressure assessments (Dawson et al., 2015). Other aspects of discrimination on health need to be explored, such as age, sex, body weight, income level, or religion, as these factors have been reported to be associated with individuals’ health outcomes (Nong et al., 2020; Scheitle et al., 2023). PDMS has also been linked to individuals’ insurance status and types. Higher levels of discrimination were reported among uninsured and publicly insured individuals compared to those with private insurance. Experiencing discrimination was linked to lacking a usual source of care, having low confidence in receiving care, delays in obtaining necessary medical care, and encountering provider-level barriers (Alcalá et al., 2020; Han et al., 2015). It would be helpful if future studies could expand the sample size and heterogeneity of participants with diabetes for sub-group analysis to expand our understanding of the impact of PDMS on patients’ health outcomes in different aspects or ethnic groups.
Moreover, our findings indicate a concerning association between perceived discrimination and poorer A1c levels. In response, health care providers should prioritize the implementation of clear anti-discrimination policies within their practices. In addition, offering training programs aimed at recognizing bias, emphasizing safety and confidential reporting mechanisms, defining expected behaviors, and taking prompt action in response to incidents are crucial steps. Fostering a culture of respect, empathy, and inclusivity is essential to ensure equitable health care delivery and ultimately improve patient outcomes (Smith, 2021).
These study findings should be interpreted within the context of several limitations. Data were sourced from the All of Us Research Program, where participants provided multiple A1c measurements across various time points in the EHR. However, demographic details, SRH assessments, social support measurements, and experiences of PDMS were obtained through a one-time survey. The cross-sectional nature of this design precludes the establishment of causal relationships. In addition, the generalizability of our findings is constrained by the demographic composition of the dataset. Notably, 88.8% of participants were non-Hispanic White, while the national average is 58.4% (United States Census Bureau, 2024), female (54.81%), with over 65% reporting an annual income exceeding $50,000, and 100% possessing health insurance coverage. Therefore, caution is warranted in interpreting the magnitude of the observed influence, particularly given the relative homogeneity of the analyzed sample.
Despite these limitations, the findings from the present study hold significant implications for clinical practice. Our study highlights that younger individuals and those who are single tend to exhibit higher A1c levels. This underscores the importance for health care providers to give heightened attention to these patient demographics, offering tailored diabetes self-management education and guidance, particularly when poor glycemic outcomes are observed.
While our results indicate a significant adverse effect of perceived PDMS on A1c levels, future studies should aim to include more diverse participant populations. Furthermore, although our analytical models encompassed various demographic factors (e.g., employment status, annual income, social support), potential confounding associations between discrimination and diabetes management may remain unaccounted for due to the absence of certain relevant variables (e.g., self-efficacy, diabetes distress) in the dataset. Moreover, identifying potential factors that may act as moderators or mediators of social support could help uncover pathways to mitigate the impact of PDMS on A1c levels. Subsequent investigations should endeavor to incorporate these factors into the analytical framework for a more comprehensive understanding of the relationship between perceived discrimination and diabetes management.
Conclusion
Insights gleaned from this study can guide the development of targeted interventions and policies aimed at mitigating discrimination and enhancing diabetes care delivery for affected individuals. Our findings highlight the substantial impact of PDMS on A1c levels, a critical metric in diabetes management and care. These results underscore the significance of health care providers creating an atmosphere of inclusivity and respect, which has the potential to bolster patient trust, enhance adherence to treatment regimens, and ultimately, result in improved outcomes for individuals managing this chronic condition.
Nevertheless, it is imperative to acknowledge that our study centered on a specific demographic subset, and additional research is imperative to encompass a more diverse array of populations. Encompassing individuals from racial and ethnic minorities, those from uninsured or underinsured backgrounds, and individuals residing in medically underserved geographic areas could offer invaluable insights into the impact of PDMS on diabetes care outcomes across various demographic groups.
Expanding the scope of our research to include a more representative sample would enable us to develop a comprehensive understanding of the multifaceted nature of PDMS and its implications for diabetes management. This broader perspective can inform the development of targeted interventions and support strategies tailored to address the diverse needs of various populations, thereby advancing the quality of care provided to individuals living with diabetes.
Footnotes
Acknowledgements
We gratefully acknowledge All of Us participants for their contributions, without whom this research would not have been possible. We also thank the National Institutes of Health’s All of Us Research Program for making available the participant data examined in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.