
Abstract
This article expands and investigates what physicians perceive as facilitators and barriers to initiating preventive health education, also called anticipatory guidance or medical education, around secure firearm storage in the home (safe storage) and outside the home (Emergency Risk Protection Orders [ERPO]). We employ in-depth qualitative interviews with 36 New Jersey physicians randomly selected from two national physician panels. Participants were screened for inclusions based on their specialty (family medicine or internist, obstetrics/gynecology, or pediatrics), practice setting (office-based rather than hospital-based), and time spent (80% or more) on direct patient care. Based on interviews, we identify five physician-perceived barriers to providing secure firearm storage counseling: inadequate screening mechanisms to prompt conversations, physician perceptions of who is at risk for firearm injury, time pressures, concerns about patient receptivity, and a need for physician training. Our findings indicate that there are structural barriers to physician-initiated firearm safety guidance. Interventions designed to increase physicians’ willingness to have these conversations must first address why these conversations fail to occur. Physician participants expressed the need for revised patient screening tools, training on approaching conversations about secure firearm storage, and a mechanism to allocate sufficient time in a well-visit, among the many other topics they must discuss. Interview participants had minimal understanding of ERPO and how to counsel patients on petitioning for ERPO.
Firearm injury persists as a leading cause of death in the United States. In 2021, the Centers for Disease Control (CDC) reported 48,830 firearm-related deaths, a 12% increase from 2020. Moreover, from 2020 through 2022, firearm injury was a top cause of death for children ages 1 to 19 (CDC, 2022). Researchers estimate nearly half (44%) of U.S. households have at least one firearm present (Jones, 2021), a strong determinant of intentional and unintentional firearm violence (Brenan, 2022; Fleegler et al., 2013; Goldstick et al., 2022; Miller et al., 2002).
Secure firearm storage, in or out of the home, can prevent intentional and unintentional firearm injury. In-home secure firearm storage, called “safe storage” (Butkus et al., 2018), aims to limit the ability of unauthorized users to access firearms, by using safety devices, such as a trigger or cable lock; storing ammunition separate from firearms; and locking a firearm in a secure location, including a gun safe or locked cabinet. Gun-rights organizations, including the National Rifle Association and the National Shooting Sports Foundation, support such practices (Horman, 2016; Rowhani-Rahbar et al., 2016; Safe Storage, n.d.). Emergency Risk Protection Orders, sometimes referred to as ERPO or “red flag” laws, provide gun households a means to ensure weapons are stored securely outside of the home when firearms present an imminent risk (Zeoli et al., 2021). Whereas ERPOs are employed when danger is imminent, knowledge and awareness of out-of-home storage options prior to when in-home storage presents a danger, such as potential suicidality, dementia, or family violence, is important for successful uptake.
Despite significant potential for secure firearm storage to reduce injury (Miller et al., 2005), estimates among U.S. gun owners suggest that only about half employ such practices, defined as unloaded and locked away (State of Connecticut Judicial Branch, 2022). Studies have demonstrated a decreased risk for self-harm injuries among high-risk adolescents when firearms are stored securely post physician counseling (Albright & Burge, 2003; Anglemyer et al., 2014; Butkus et al., 2018; King et al., 2020; Zeoli et al., 2021), with the use of ERPO, and as required by law (Crifasi et al., 2018). As such, there is a great need to increase secure firearm storage in or outside the home when necessary.
Physician-provided medical education, key to preventive care, has successfully mitigated health risks, including home accidents, auto passenger injuries (Magar et al., 2006), and hospitalizations for chronic disease management (Nelson et al., 2003). Given this, firearm safety counseling represents an untapped opportunity to promote secure firearm storage at a population level.
Physicians are often viewed as trusted messengers of safety information, making them well-positioned to address firearm safety in routine patient education (Iott et al., 2020). However, despite strong support for this practice, Damari et al. (2018) found that 80% of physicians believe firearm safety counseling is essential—only 25% report engaging in these conversations with patients. Given the potential to reduce firearm-related injuries and deaths (Parent, 2016), physicians should prioritize firearm safety discussions as a standard component of medical education during well-visits. 1
Although researchers have looked at interventions to increase physician-initiated conversations around firearm safety, existing studies suggest that these conversations are rare and, despite efforts, have increased little over the past three decades. Dineen et al. (2024) identified five physician-perceived barriers to including firearm storage counseling in preventive health education. Internists identified inadequate screening mechanisms to trigger conversations, physician misperceptions of risk for firearm injury, time pressures, concerns about patient receptivity, and a need for training. When physicians cannot provide medical education around secure firearm storage, opportunities for preventive care are missed.
This study explores if and how facilitators and barriers to physician-initiated patient conversations regarding secure firearm storage vary by specialty among internists, obstetrician/gynecologists (Ob-Gyn), and pediatricians. A secondary purpose was to understand the extent to which physician-participants are familiar with ERPO and if they include such orders when providing counseling around secure firearm storage. Before developing an effective and scalable intervention to increase physician-provided patient education about firearm safe storage, we must understand what factors influence physician decisions about whether these conversations occur and how those factors might vary among providers who treat patients across the life course. This study explores the following questions:
Impact Statement
Physicians point to electronic medical records systems to facilitate universal firearm screening and promote firearm safety conversations. Physicians need training on assessing firearm injury risk and on how to discuss firearm safety with patients. Well-visit structure, the number of anticipatory guidance topics, the role of screening, and patient receptivity must be factored into interventions designed to promote physician-initiated firearm safety conversations.
Method
We employed in-depth qualitative interviewing to better understand what health care providers in Primary Care type specialties, view as facilitators and barriers to initiating patient education conversations around secure firearm storage. Thirty-six semi-structured interviews with New Jersey physicians were conducted between June 23 and July 17, 2023. The 45-minute interviews were conducted via Zoom, recorded, and transcribed. The University of Connecticut Institutional Review Board reviewed and approved the study protocol.
Sample and Participant Identification
Our sample was drawn from the Schlesinger and Associates panel of health care professionals and The Logit Group Panel. Both panels, covering practice areas, settings, and provider types, employ multiple recruiting strategies, including live interviewers (telephone and in-person), social networking, and online marketing. Two panels were used to obtain sufficient sample size and ensure appropriate geographic coverage. Table 1 includes the counties where participating physicians practice and the number of respondents from each county.
Participant Counties.
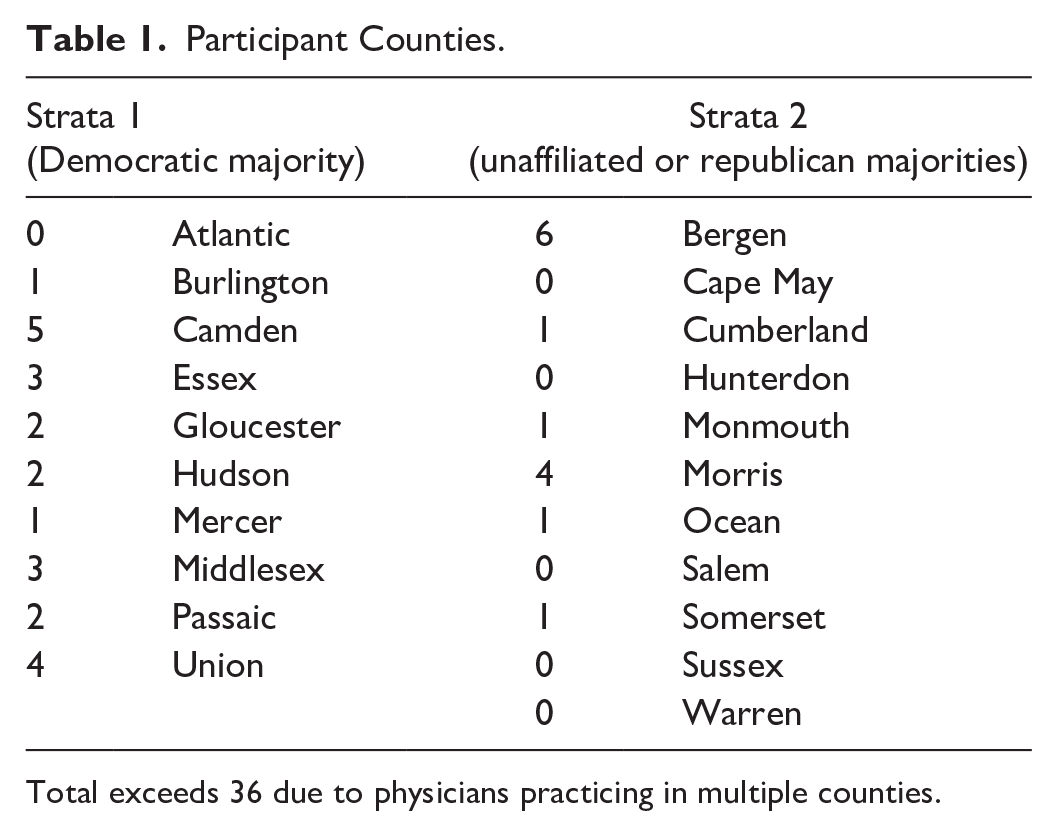
Total exceeds 36 due to physicians practicing in multiple counties.
From each panel, physicians licensed in New Jersey, who spend at least 80% of their time on direct patient care in non-hospital settings, and identified as a family medicine/internist, Ob-Gyn, or pediatrician were randomly selected. Selected participants were screened to confirm they practiced in the State of New Jersey, ensure geographic diversity within the state, and balance the sample by specialty. Specifically, we screened to ensure heterogeneous participants regarding gender, race, and specialty (Internist, Ob-Gyn, and Pediatrics). Screening also included practice-area urbanicity to capture the diverse populations and firearm cultures in New Jersey. Using State of New Jersey Elections Division data, we created two strata: one with counties where the majority of voters registered as Democrats and one with counties where the majority of voters registered as Republican or unaffiliated.
Instrument Development
The Theory of Planned Behavior (TPB) guided the creation of the interview guide (Ajzen, 1991). If, as the TPB states, beliefs about behaviors largely shape behavior intent, social influences are essential constructs of behavioral intent, and objective realities may facilitate and inhibit behavior change. Interview questions were developed to understand the behavioral, normative, and control belief constructs related to physician counseling around firearm safety (President’s Plan, 2013). If a behavior, in this case, anticipatory counseling on secure firearm storage and ERPOs, is perceived as important, and norms support the behavior, providers are more likely to engage to the extent they perceive change is within their control. We addressed these constructs through questions regarding physician attitudes toward, normative beliefs around, and perceived controls in firearm safety counseling.
After introductory statements, interview participants were asked about their practice (size, location, and patient demographics), along with the topics covered and inclusion criteria for anticipatory guidance conversations during well-visits. Specifically, we asked about counseling around the safe storage of firearms within their anticipatory guidance conversations, their level of comfort discussing firearm storage with patients, and their awareness and knowledge of ERPOs. The interview guide also asked about potential barriers to such conversations and what might necessitate the discussion of firearm storage during standard patient education during well-visits. The protocol included interview questions that were both broadly structured and open-ended, with probes to address relevant topics.
Analysis
Interview recordings were transcribed and abridged. After reviewing all transcripts, a coding frame was developed by a member of the coding team reviewing three transcripts from each specialty group (a total of nine). Three coders used that initial frame to code half the sample, iteratively refining codes during analysis. That revised frame was used with the remaining sample, iteratively refining as needed. In addition to codes, we identified contextual excerpts from the transcripts. Three members of the research team independently reviewed and coded all 36 transcripts. After independent coding, team members met to discuss all codes’ thematic and contextual meanings. The codes were revised, and all transcripts were reviewed again. In cases of coding disagreement, a member of the research team, not involved in coding, acted as a mediator. A database was created with the revised codes notating participants’ responses to questions and contextual examples. After coding and analysis by the research team, ChatGPT AI was employed to review transcripts for codes or themes the research team might have missed or improperly weighted in the analysis (OpenAI, 2025a, 2025b, 2025c, 2025d). Neither the coding frame nor theme were altered after the ChatGPT AI analysis.
Results
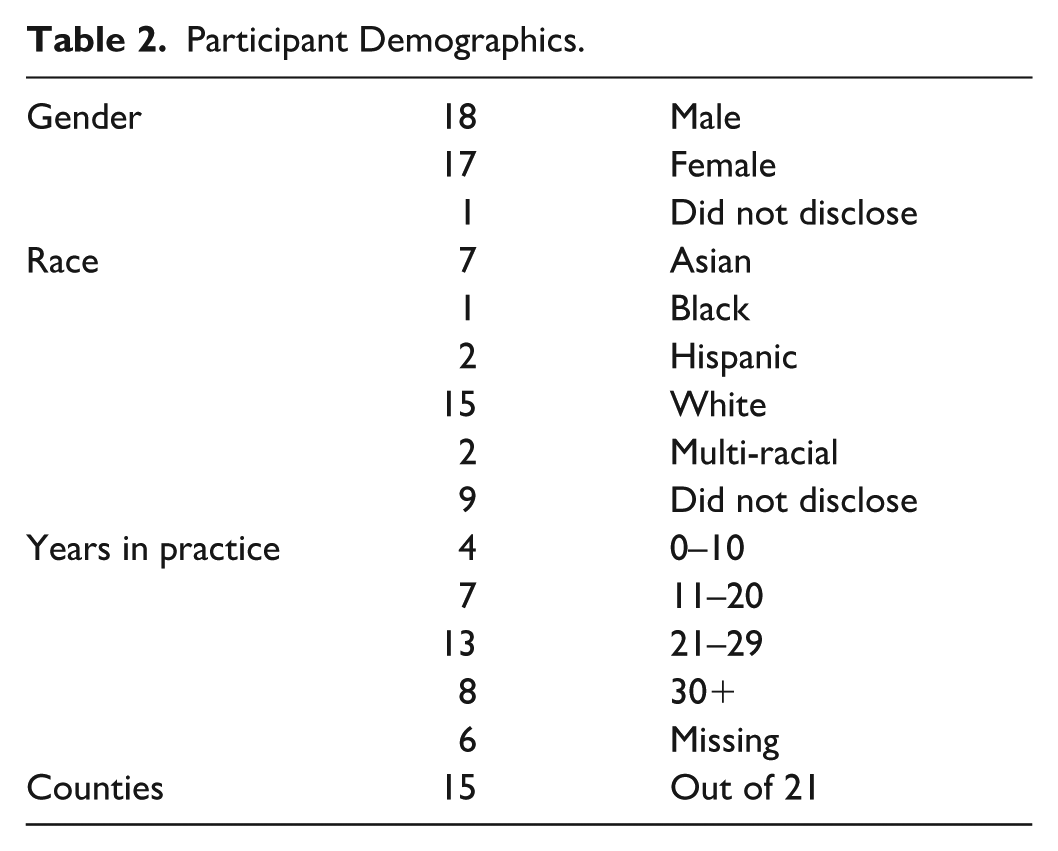
The study included 36 participants who identified as internists (n = 12), Ob-Gyn(n = 11), or pediatrician (n = 13). Participant screening produced a diverse participant pool in terms of gender (18 male, 17 female, one non-disclosed), race (15 non-Hispanic White, 12 identifying with other racial or multi-race categories, nine non-disclosed), and time in practice (three: 0–10 years, six: 11–20 years, 16: 21–29 years, eight: 30+ years, three non-disclosed). Participants’ practice areas included 15 of New Jersey’s 21 counties. Table 2 provides sample demographics.
Participant Demographics.
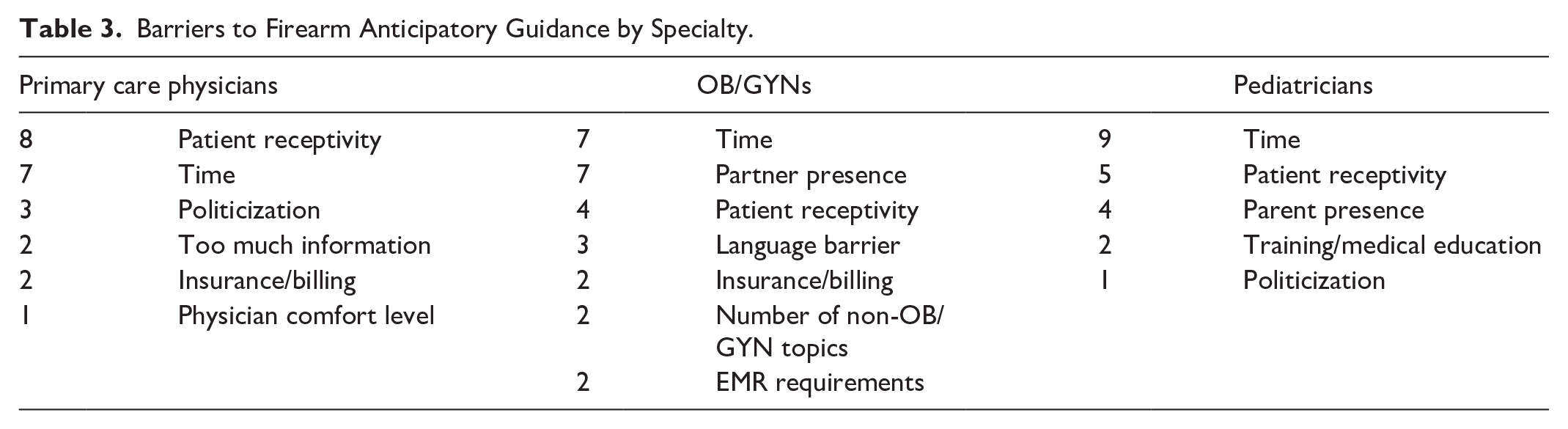
Consistent with prior work (Betz et al., 2021; Dineen et al., 2024; Webster et al., 1992), this analysis (Table 3) points to (1) inadequate screening mechanisms to prompt firearm safety conversations, (2) physician misperceptions of firearm prevalence, (3) well-visit time pressures, (4) receptivity concerns, and (5) a lack of training as contributing to the lack of patient education around secure firearm storage. When asked about ERPOs, physicians’ self-reported lack of knowledge and awareness were significant barriers to initiating guidance.
Barriers to Firearm Anticipatory Guidance by Specialty.
Patient Education During Well-Visits
Participants report regularly providing anticipatory guidance on topics including diet and nutrition, cancer screenings, alcohol and drug use, vaccines, and mental health. As shown in Table 4, anticipatory guidance topics, and their frequency, vary by specialty.
Anticipatory Guidance Topics by Specialty.
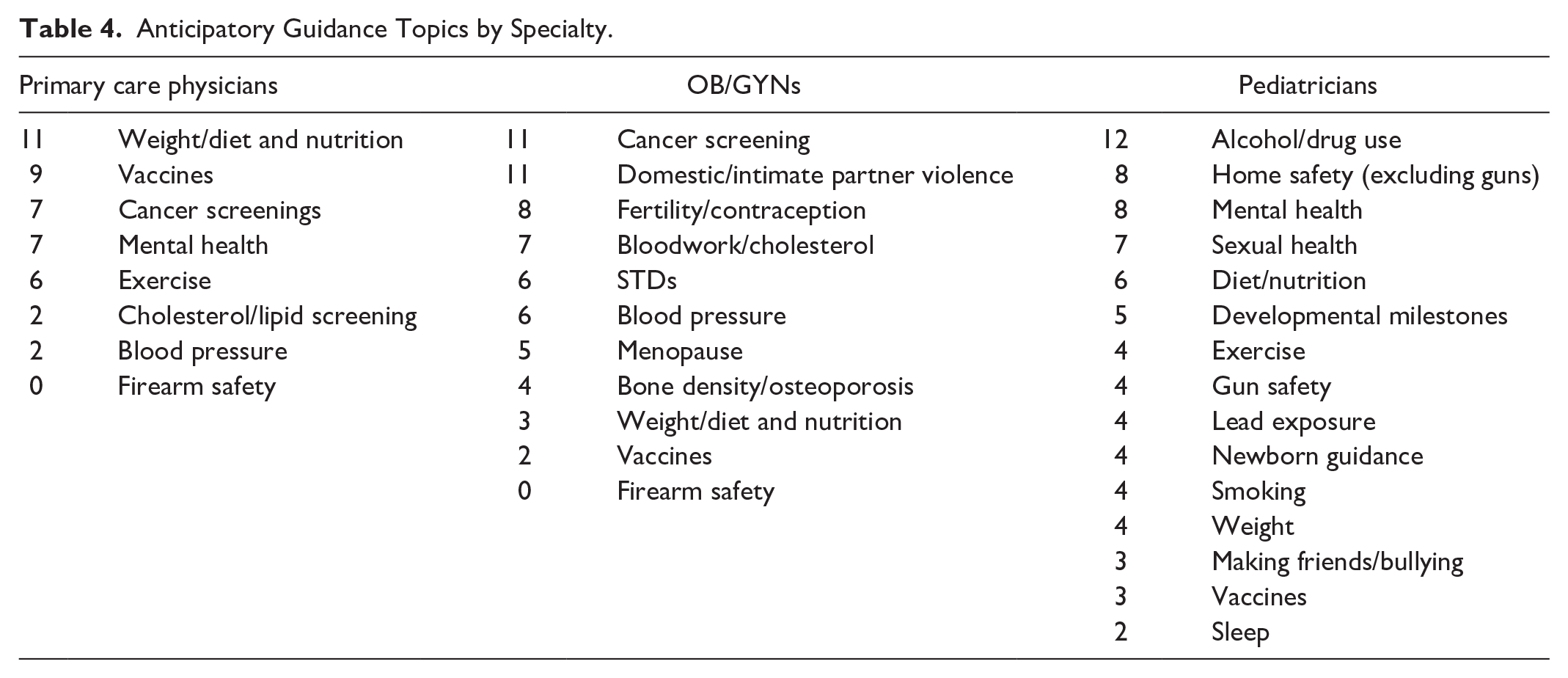
As seen in prior work, physicians rarely mentioned secure firearm storage or general firearm safety as an anticipatory guidance topic. Only four physicians, all pediatricians, included firearm safety in anticipatory guidance. An internist explained, “If there has been a tragedy around the time of their visit, I may mention it . . . It’s not something I’m typically going to discuss . . .” An Ob-Gyn commented, “It’s more important for me to talk to them about STI prevention; I don’t really think that’s my job to talk to them about firearm prevention.”
Comfort With Firearm Safety Conversations Varies by Specialty
Interviews also explored participants’ comfort and perceived preparedness for various well-visit health education topics. In short, physicians report that comfort is not a barrier to anticipatory guidance conversations, including conversations about firearms. But, when asked specifically about their own comfort with firearm safety conversations, responses varied among and within specialties. An internist noted, “I’d be comfortable, but I wouldn’t think to ask. We live in an area where [most] who do carry weapons do know about safety. It’s common sense . . .” An Ob-Gyn commented that “. . . those kinds of questions where the patient might be uncomfortable about what I’m going to ask them can sometimes make me feel a little uncomfortable as well.” Despite pediatricians being the most likely to include firearm safety in anticipatory guidance, comfort varied. One noted that firearm safety is a “[big comfort issue. I think some people find it offensive that I’m asking. [The patient thinks] ‘I’m bringing my kid to get a checkup; I want to get him his shots; I have no interest in talking to you about guns.’”
Physicians Across Specialties Express Concerns About Patient and Chaperone Receptivity to Firearm Safety Conversations
Three quarters of the internists interviewed identified concerns about patient receptivity to firearm safety conversations as a barrier to including such discussions in the anticipatory guidance portion of well-visits. One shared, “It becomes a political issue . . . you don’t want to get into a political debate with a patient, Second Amendment, and all that . . .”
For the Ob-Gyn and pediatricians who, more often than internists, have patient family members present during a well-visit, concerns about receptivity extend to the patient’s chaperone. Physicians expressed concern for this dynamic 11 times in Ob-Gyn interviews and nine times in pediatrician conversations. One Ob-Gyn explained, “If I have a patient that is very pro-gun policies, I’m not going to engage in that conversation . . . because I don’t feel the same about it.” A pediatrician shared, . . . I don’t think parents would appreciate me bringing the topic up. Any parent who owns guns, if they don’t have their guns locked up in the house, I don’t think in my ten-minute visit where we’re talking about shots and development, if I say, “You better lock up your guns,” they’d say “That’s a great idea . . .”
Lack of Screening, Time, and Lack of Training are Physician-Identified Barriers to Including Firearm Safety in Patient Education
Physicians, across specialties, mentioned time as a significant barrier to including firearm safety in anticipatory guidance. One participant explained, It’s mostly time and . . . monetary pressures. . . insurance companies whittling us down to not getting reimbursed. It’s driving [us] to see more and more patients. . . anticipatory guidance is being compromised . . .
In addition to time, the lack of a screening mechanism to prompt firearm storage conversations was consistently mentioned. As one pediatrician described, “Firearm safety isn’t part of the template. . .We [don’t bring up anything] about guns in the house.” An internist explained, [o]n the EMR, there are quality measures that light up red if you’re not done, and I’m looking at those all the time to see who is meeting the targets for blood pressure, AIC, mammograms, going to the dentist—there’s a long list depending on what people have.
Training and professional guidance around firearm safety conversations ranked second to screening as crucial for including such conversations in patient education. Twenty-three of the 36 study participants mentioned training or professional guidance as necessary for including firearm safety in physician-provided anticipatory guidance. A provider noted, There are guidelines about how to talk to people about mental health, and eventually, there will be guidelines on how to discuss this. . . we’ll learn that, too. There are the medical society’s medical guidelines on what vaccines people should get. That’s where it would fit. Official guidelines on asking in a more objective fashion. Conferences, newsletters, societies—those are the ways I get my information.
Similarly, an Ob-Gyn explained, . . . we need some information and guidelines . . . I would like something from the American College of Ob-Gyns, some guidelines of what . . . to ask . . . Most of the screeners are based on the guidelines we have . . . There has been some basis of reason to have that be brought up.
Participants Were Largely Unfamiliar With ERPO and Did Not Think of It as a Tool for Secure Storage
Study participants were asked to explain ERPOs in their own words and their level of familiarity with such laws. Whereas four participants reported being very familiar with ERPOs, none of those four provided explanations consistent with New Jersey law. The seven participants who identified as “somewhat familiar” with ERPOs reported having heard of the laws but had no specific knowledge. An Ob-Gyn commented, “I don’t know enough about what that entails; who enforces that if that’s through a court order or the police department? What’s unclear . . . is the path itself, who do I call?”
The most common response to the question about familiarity with New Jersey’s ERPO law was “not familiar.” An internist explained, “I’ve not heard of either one. Nothing from the medical community or the New Jersey Board of Medicine on advising on discussing with patients.” An Ob-Gyn commented, “I know zero about that. I don’t know what that means.”
While study participants did not consider ERPO a form of secure firearm storage before our conversations, following our discussions, many saw potential for New Jersey’s ERPO law to be a lifesaving form of secure storage. An internist commented, I haven’t heard of this . . . but it’s important to know. The family, friends . . . who know they [at-risk individual] have a gun and . . . could self-harm or harm others if they can legally take the gun out of that person’s hands . . .
Although physicians understand that ERPO provides a tool to reduce firearm injury and death, a lack of awareness and knowledge of ERPO processes leaves them unsure of how to employ such a tool. A pediatrician offered, “I need to be a bit better educated about this . . . I don’t think I’d be comfortable talking to them about it today . . .” An Ob-Gyn commented, I would be uncomfortable [talking about ERPO] because I don’t know what the next thing would be. If they say, “My boyfriend carries a gun, and sometimes it threatens me. I don’t know what that next step would be . . . I don’t feel I’m equipped enough to handle that.”
Physicians’ Perceptions of Firearm Prevalence and Injury Risk Are Barriers to Anticipatory Guidance
Physicians provide their perceptions of gun injury risk to their patient population as a rationale for not including firearm safety in patient education conversations. Patient demographics (age, parent status), geography, and state culture were given as reasons why firearm safety guidance for patients is unnecessary. An internist noted, “I have a large geriatric population . . . a suburban population, so it’s not really an issue,” and an Ob-Gyn shared, “[n]o one ever has told me that her husband has a gun. I’m not in the inner city; I’m in a blue-collar neighborhood.” From a pediatrician, we heard, “At least in this area, the number of patients who have firearms is so small, it’s not worth wasting our time bringing it up.” These physician perceptions tend not to align with evidence regarding who is at risk for firearm injury (Price and Khubchandai, 2021).
Physicians Recommended Universal Screening and Insurance Billing to Facilitate Secure Firearm Storage Conversations
After exploring barriers to including firearm-safe storage information in well-visit anticipatory guidance, physicians were asked what, if anything, could be done to facilitate such conversations. Across specialties, physicians suggested the same three mechanisms for ensuring firearm storage conversations are included in patient education. Interview participants in all three specialties offered that a question about firearm access would need to be added to the Electronic Medical Record (EMR)/intake questionnaires. “The most efficient way is adding [firearm screening] to the questionnaire, and if you see it there, you can ask about it.” Another participant explained, “If it’s not on the list of things you think are important, you’re not going to bring it up with a lot of patients.”
Physicians also identified guidance from professional associations, including the ACOG, AMA, and AAP, as an effective mechanism for facilitating proactive physician firearm safety conversations. As one participant explained, “[t]he guidelines tell me I have to do so much anticipatory guidance, that’s my whole job description really. That’s why I do what I do in pediatrics: prevent disease instead of treat disease.”
Finally, physicians pointed to insurance—both screening requirements and billing—as a mechanism to facilitate firearm storage conversations and create time in the visit to accommodate the additional anticipatory guidance topic. An internist recommended, If [it]became part of the MIPS measure—the quality metrics attached to Medicare reimbursement, bonus payments/penalty payments for the physician practice, people would ask it all the time. It must be part of something. . . . either do it as part of the USPTF wellness visit recs, add it to the MIPS, or even better, do both. Then physicians will report on an annual basis how many times they are asking the question . . .
Another internist noted, “If insurance payers made it part of their value-based care, then health systems would do a lot of education and build around this . . .”
A pediatrician explained how insurance currently limits their time on anticipatory guidance topics: . . . we’re asked to do more and more in anticipatory guidance, but we don’t get more time to spend with a patient . . . the insurance companies tend to pay a certain fee for a well-visit, and you could spend 15 minutes or an hour, but there’s no difference in how much we get reimbursed for it.
An Ob-Gyn shared a similar sentiment, It’s mostly time and . . . monetary pressures . . . insurance companies whittling us down to not getting reimbursed. It’s driving [us] to see more and more patients . . . anticipatory guidance is being compromised.
Study Limitations
Employing rigorous methods is essential for reducing researcher bias. Despite employing a thorough methodology, this study has limitations. We used two large health care provider panels to randomly select 36 participants who practice in the State of New Jersey and identified as specializing as internist/family medicine, obstetrician/gynecologist, or pediatrician. The lack of probability-based methods, small “n” size, limited geographic coverage, and a single type of practice setting do not allow for generalizations to the population of health care providers whom patients see as trusted information providers.
Discussion
Firearms are the leading cause of death for America’s children and a top cause of death for adults in this country. Despite evidence that secure firearm storage reduces accidental and non-accidental firearm injury, few participants report routinely engaging in medical education regarding firearms. Participants were unfamiliar with ERPOs, making the orders unavailable as a tool when a patient is at risk for injuring themselves or others with a firearm.
Physicians-identified barriers to secure firearm storage in well-visit guidance, include the lack of screening, provider training, and in-visit time constraints. Researchers identified physicians’ concerns about patient receptivity and misperceptions of firearms injury and risk prevalence among patients as additional barriers to firearm safety anticipatory guidance.
Consistent with prior work, physicians identified increased training in medical school and residency and through Continuing Medical Education credits (CMEs) as facilitators of firearm safety and secure storage conversations with patients. As patient views of securely storing firearms vary by a number of factors (Grasso et al., 2024), training needs to include strategies for providing guidance that accounts for varying firearm attitudes and experiences. Participants were clear that universal screening regarding firearm storage is an important mechanism to increase the frequency of these conversations. Utilizing standardized screening measures built into physicians’ systems is critical. EMR systems, such as EPIC and Athena, can provide a tool for facilitating screening and prompting physicians to have these conversations.
Guidance from professional associations influences physician practice, including what to include in anticipatory guidance discussions. The U.S. Preventive Services Task Force (USPSTF) guidelines shape well-visits across specialties, and Medicare wellness visits align with USPSTF recommendations. Currently, USPSTF lacks firearm safety guidelines (O’Connor et al., 2013). Physicians also rely on specialty societies like ACP, AAFP, AAP, and ACOG for guidance. AAP provides clear firearm safety guidance, with pediatricians leading the way. Other societies have positions, though less known. USPSTF-specific guidelines and increased awareness of specialty society guidance would enhance provider firearm safety discussions.
Finally, participants across specialties point to insurance coverage as important facilitator discussed by physicians across these specialties. Multiple physicians noted that the list of topics to be covered during preventive visits is already long and that much of what they discuss during these visits is not reimbursed by insurance. As time for well-visit appointments is limited, those non-reimbursable items are less likely to be addressed. Allowing insurance reimbursement for firearm safety and secure storage counseling during a preventive visit would enable physicians to prioritize these conversations and carve out additional time.
This study underscores the structural hurdles to physician-initiated discussions on firearm safety and secure storage, which must be tackled before implementing conversation-focused interventions. The results illustrate the need for a comprehensive screening approach for assessing gun injury risk, utilizing both EMRs and patient screening. Besides updating EMR systems, physicians require training, starting in medical school and continuing through professional development, to better identify individuals at risk of gun injuries and effectively engage in firearm safety conversations, irrespective of patient receptivity. Future research should explore the perspectives of other health care professionals who interact with patients in the screening process (e.g., nurses and medical assistants) and examine the effectiveness of various methods of communicating secure storage information with different patient populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in large part with funding provided by the New Jersey Center on Gun Violence Research at Rutgers University. The Center works in collaboration with and is supported by New Jersey’s Office of the Secretary of Higher Education.