
Abstract
Little is known about how distance learning impacts delivery of the National Diabetes Prevention Program (DPP) despite a rapid shift to this platform during the coronavirus disease 2019 (COVID-19) public health emergency. We explored how a workplace DPP, delivered via distance learning, impacted knowledge, motivation, and behavioral skills of participants throughout the program. We conducted repeated qualitative interviews with distance learning participants at baseline, 6 months, and 12 months from September 2020 to July 2022. Three study team members coded interview data using individual responses as the unit of analysis. We used a thematic approach, using the information–motivation–behavioral skills framework, to analyze responses and generate understanding of the program’s impact. The 27 individuals who participated in the interviews (89% women, mean age 56 years) reported the distance learning platform was effective in changing their behavior. The program’s focus on food logging and setting limits on specific types of caloric intake was perceived as essential. Education on ideal levels of fat and sugar consumption, lessons on how to read food labels, and dissemination of recipes with healthy food substitutions allowed participants to initiate and sustain healthy decision-making. Strategies to increase physical activity, including breaking up exercise throughout the day, made reaching their goals more feasible. Participants reported food logging and weight reporting, as well as group support during sessions, either sustained or increased their motivation to adhere to the program over time. A workplace DPP delivered via distance learning successfully prompted improvements in the knowledge, motivation, and behavioral skills necessary to increase healthy eating and physical activity among participants.
Introduction
Several large randomized controlled trials have demonstrated Type 2 diabetes (T2DM) can be prevented or delayed in high-risk adults through structured lifestyle interventions that focus on nutrition and physical activity to result in modest weight loss (Albright & Gregg, 2013; Haw et al., 2017). In 2010, the U.S. Congress authorized the Centers for Disease Control and Prevention (CDC) to establish and lead the National Diabetes Prevention Program (DPP) as the mechanism to coordinate the process of translating research findings to the community level (Albright & Gregg, 2013). Employers are ideal partners for implementing and disseminating programs like the National DPP, which focus on reducing the burden of diabetes and obesity in the United States. In total, 60% of U.S. adults 16 years and older are employed (U.S. Bureau of Labor Statistics, 2023), and worksites are a crucial source of information, communication, and social support for employees (Sigursteinsdottir & Karlsdottir, 2022). Preventing diabetes could have substantial financial benefits for employers since more than 70% of working individuals receive employment-based health insurance coverage (Keisler-Starkey et al., 2022) and the annual medical expenditures for people living with diabetes are more than twice as much as for those without diabetes (“Economic Costs of Diabetes in the U.S. in 2017,” 2018).
The CDC established the Diabetes Prevention Recognition Program (DPRP) to assure program quality, fidelity to scientific evidence, and broad use of effective T2DM prevention lifestyle change programs across National DPP providers (Ely et al., 2017; U.S. Bureau of Labor Statistics, 2023). Initially, the DPRP certified only in-person delivery of the DPP (Cannon et al., 2022). In 2015, the DPRP began recognizing virtual delivery of the National DPP via online or distance learning delivery platforms. Distance learning is defined as the live delivery of session content in one location by a lifestyle coach while participants call-in or video conference from other locations (U.S. Bureau of Labor Statistics, 2023). Although the DPRP has accepted distance learning for the past 8 years, DPP delivery via distance learning was extremely limited prior to the COVID-19 pandemic; only 1% of National DPP participants enrolled in the program via distance learning through 2019 (Cannon et al., 2022). Mitigation strategies to prevent person-to-person transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) during the COVID-19 public health emergency prompted rapid shifts from in-person to virtual interactions throughout health care, including for the DPP. Many in-person programs shifted to distance learning to leverage their existing resources (recruitment tools, coaches, data management, etc.) to continue delivering the DPP during the pandemic (Bullock et al., 2023).
Telehealth modalities, including distance learning, have the potential to broaden the reach of in-person programs because they may eliminate, to some extent, stigma, time, and geographical barriers. However, little is known about if/how distance learning affects participants’ motivation to remain in the program, or if distance learning platforms influence if/how participants acquire knowledge and skills necessary to adopt healthy eating and increase their physical activity as strategies to promote weight loss, which was a key predictor of diabetes risk reduction in the original DPP trials (Centers for Disease Control and Prevention, 2016; Ely et al., 2017). Thus, there is a critical need for research to guide the use of distance learning as a DPP implementation strategy. We conducted in-depth interviews to explore participant knowledge, motivation, and behavioral skills over the course of their participation in a workplace DPP delivered via distance learning.
Method
Health Plus, the workplace wellness division of Vanderbilt University Medical Center, began offering the DPP (HP-DPP) as a benefit to employees in 2014; program details for the HP-DPP including eligibility criteria, curriculum, and class structure have been previously described (Chakkalakal et al., 2019). The HP-DPP was delivered in person on the Vanderbilt campus from 2014 to 2017. In 2018, the HP-DPP added a distance learning participation option to improve program reach while preserving the group structure. In response to the COVID-19 public health emergency, the HP-DPP stopped offering the in-person participation option in March 2020; since then, the HP-DPP has been delivered entirely via distance learning. HP-DPP distance learning group participants are mailed a booklet with materials they need for the yearlong program prior to Session 1. These materials are also included in email reminders before each session. Distance learning participants log in to Zoom to interact with each other and HP-DPP coaches during each session. Participants self-report their weekly program data (weight, physical activity minutes, and food logs) via REDCap (Harris et al., 2009), a secure web-based application that is compliant with the Health Insurance Portability and Accountability Act of 1996 (HIPAA).
Ethics Approval
Our evaluation of the HP-DPP was approved by our institutional review board (IRB) (IRB: 2211866). All employees who were first-time enrollees in the HP-DPP were invited to participate in a program evaluation initiative that included baseline, midpoint, and endpoint surveys and interviews. All participants signed a written consent form before any data were collected. Participants were reimbursed with a US$25 gift card per interview completed.
Recruitment of Participants for In-Depth Interviews
HP-DPP participants who chose to be interviewed were contacted by email or phone to schedule their baseline interview as soon as they expressed interest, with the baseline interview scheduled to be performed approximately 4 to 6 weeks after they began the program (Table 1). Participants who completed baseline interviews were contacted at 6 months and 11 months after they began the HP-DPP to complete midpoint and final interviews, respectively. Interviews were conducted via Zoom by staff trained in qualitative research methods.
Interview Guide.

Sample Size for Interviews
The theory of data saturation informed our final sample size: We continued to collect data from participants until we generated enough information to understand how distance learning impacts participant perceptions and experience with the DPP (Hennink & Kaiser, 2022). Prior research suggested theoretical saturation usually occurs in the range of 20 to 30 interviews (Curry et al., 2009). Since our evaluation focused on expectations and experiences over time, we completed interviews at baseline, midline, and in the last month of the program.
Data Management and Analysis
The study team recorded and transcribed all interviews within 3 weeks of completion. Two researchers reviewed transcripts for completeness and accuracy. The interviews were reviewed after each round to identify key themes and assess data saturation. We used MAXQDA 2022 software to analyze interview data, with the unit of analysis being the individual’s response and focusing on how attitudes and perceptions changed over time. Qualitative analysis was conducted by CMA and LJR, with at least two analysts reading each interview. Analysts refined their assessments until the intercoder reliability measure was >85%. Meaningful themes were selected and summarized.
We used the information–motivation–behavioral skills (IMB) model of health behavior (Suls & Wallston, 2003) to conceptualize how programmatic “inputs” of the National DPP prompt behavior change to improve weight management (Figure 1). We focused on understanding how HP-DPP delivery via distance learning impacted participant uptake of information, motivation, and behavioral skills to inform our initial codebook and added in vivo codes as they emerged. During baseline interviews, participants were asked how they learned about the HP-DPP, what motivated them to join the HP-DPP, their confidence to succeed in changing their behavior, and their expectations about the effectiveness of distance learning groups. For midpoint and final interviews, participants were asked various questions about perceived support both within and outside of the program, motivation, the information they gained, skills learned and developed from their coaches and fellow participants, and overall thoughts about the program.
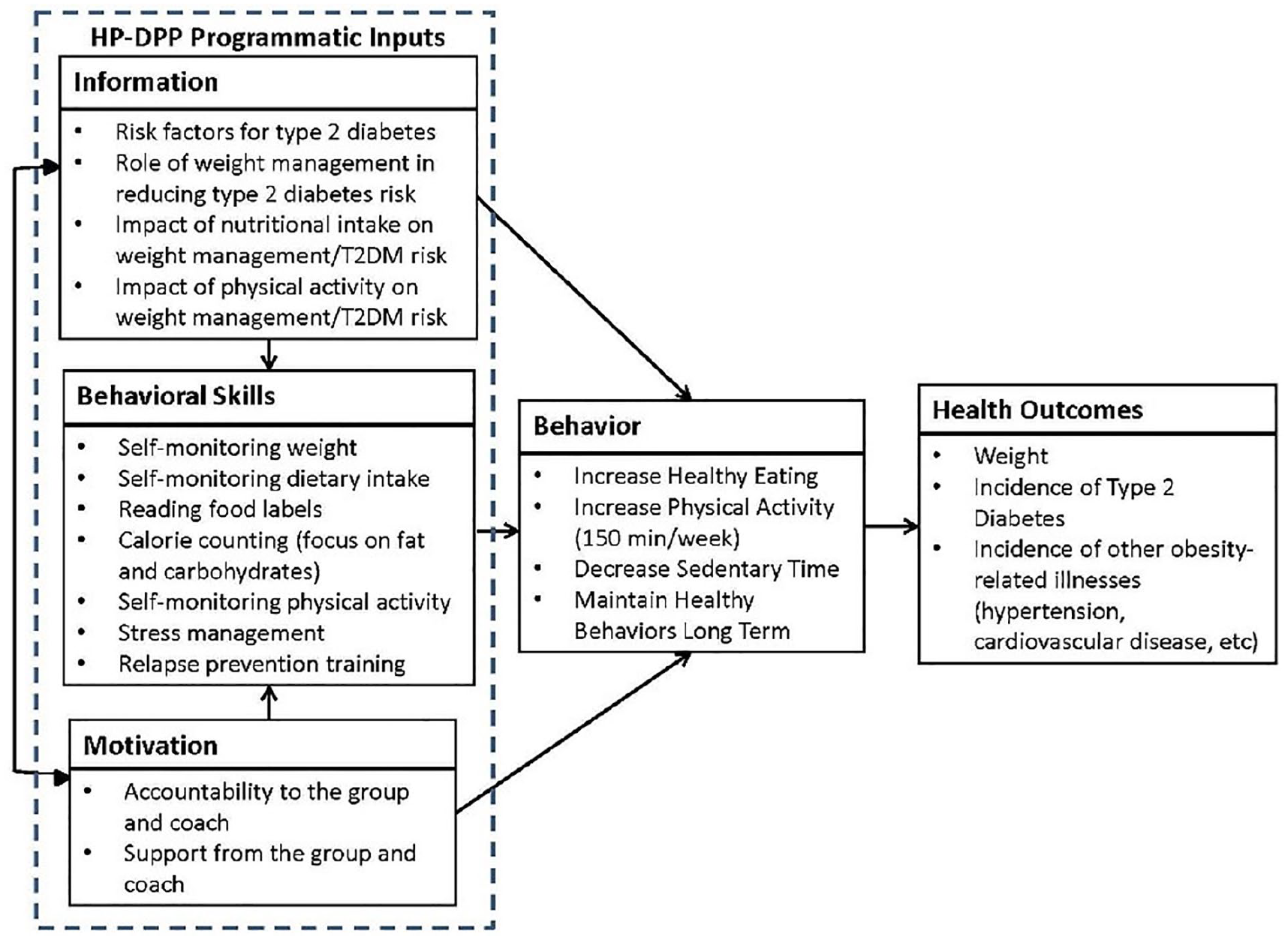
IMB Conceptual Framework.
Results
Summary of Participant Characteristics
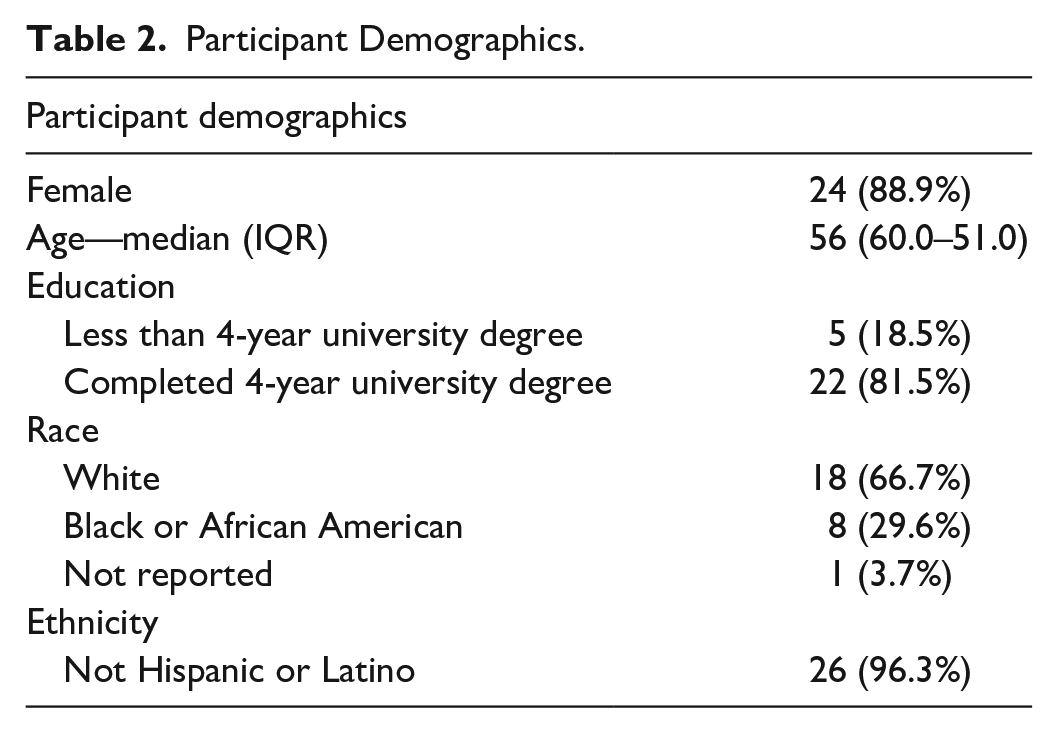
A total of 81 HP-DPP participants enrolled in the program evaluation and were, therefore, invited to complete three interviews with our study team. Thirty-six participants expressed interest in being interviewed; 29 of the 36 responded to scheduling requests for the baseline interview. Two individuals requested their data be excluded from analyses after completing their interviews which resulted in interview data for 27 participants being available for analysis. We analyzed data from 27 baseline interviews, 25 midpoint interviews, and 23 final interviews. Of our 27 participants, 24 (89%) were women. The average age of participants was 56 years (standard deviation [SD]: 8.9). Eighteen participants identified as White (67%) and 26 identified as non-Hispanic (96%). As for level of education, 22 participants have a minimum of a bachelor’s degree (81%) (Table 2).
Participant Demographics.
Information/Knowledge of Participants
At baseline, all participants reported some knowledge about the importance of good nutrition and physical activity necessary to live a healthier lifestyle. While some participants reported high levels of knowledge about appropriate food intake at baseline, the program focus on limiting consumption of fats and sugars coupled with food logging was perceived as essential to adopting healthier behaviors. This knowledge allowed participants to adjust their level of consumption of fat, as well as meticulously read food labels and nutritional content when purchasing food from a grocery store or restaurant. The nutritional information received throughout the program also allowed participants to learn about healthier substitutions they can use for the food that they prepared themselves (Table 3):
I think what I have found to be most useful is the recording and logging of food, being accountable to that caloric intake and understanding how many fat grams, and when you go over your protein and your sugars and all that. (60 years, midpoint interview)
Regarding fitness, one of the most important things participants learned throughout the program was that their daily physical activity goal did not have to be completed in one session. The program helped them understand they could distribute their daily physical activity over multiple sessions to reach their overall daily goal.
Information Gained in the DPP.

Participants greatly appreciated the knowledge they received about the psychological aspect of behavior change. The HP-DPP gave participants tools to cope with stress and negative influences:
We also talked about stressors and how to reduce stress and ideas and thoughts that didn’t revolve around food. Because a lot of times I know for me, I am eating because I’m stressed, not because I’m really hungry. One of the group members talked about, what did she call it? Something bundling, habit bundling, which I thought was really, really a neat idea. So I’ve been working on trying to incorporate habit bundling into that, and it might not have been habit bundling, but it was something similar to that. (50 years, midpoint interview)
Participants were able to understand better cues for eating other than satisfying nutritional needs, such as boredom, sadness, and loneliness and learned strategies to overcome these triggers. They similarly understood psychological barriers to physical activity participation.
Motivation of Participants
Participants reported high levels of motivation to lose weight during our baseline interviews and throughout their time in the program. They were motivated to enroll and increase their healthy behaviors by health issues related to weight (a diagnosis of prediabetes or diabetes, as well as joint pain), seeing their weight creep up over time, health issues experienced by family members, and a perceived dip in their quality of life due to the stress of trying to lose weight (Table 4):
Until I got to the point where one day I got on the scale like, “Oh my God. I cannot believe I weigh this much.” It really hurt. I said, “I can’t do this. I have to change,” because I look at my older siblings and they are overweight. I don’t want to be like that. I don’t want to have all these medical issues and medical problems. (48 years, baseline interview)
Motivation of DPP Participation.
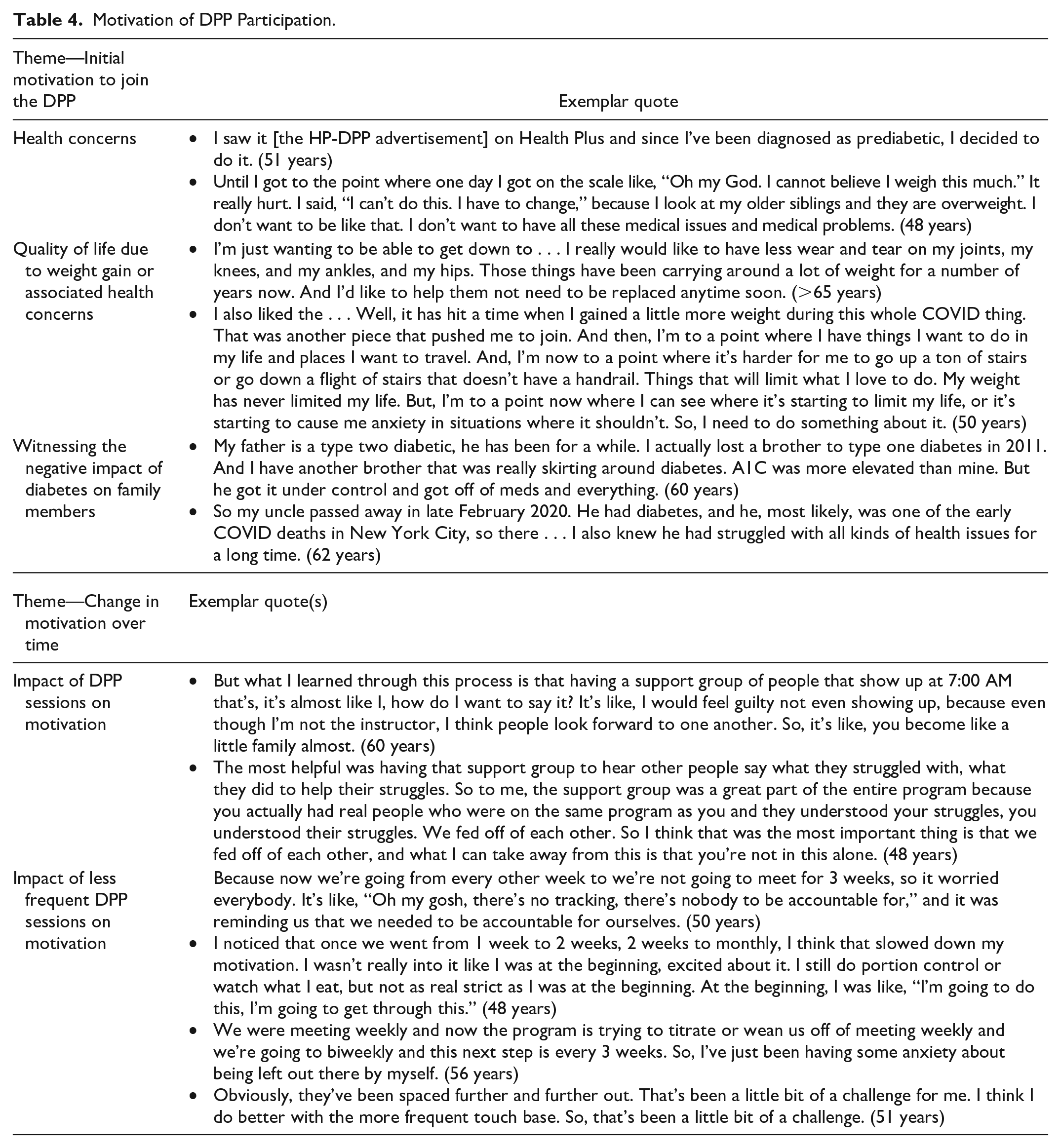
Most participants were motivated by their own health concerns, either because they were experiencing symptoms or because they were concerned that they were on the path to poor health. In addition to improving clinical outcomes, quality of life was a motivator for HP-DPP participation. Those struggling with weight were very focused on being able to play with children/grandchildren, travel, attend concerts, or be physically active outdoors with friends and family:
. . . I’m now to a point where it’s harder for me to go up a ton of stairs or go down a flight of stairs that doesn’t have a handrail. Things that will limit what I love to do. My weight has never limited my life. But, I’m to a point now where I can see where it’s starting to limit my life, or it’s starting to cause me anxiety in situations where it shouldn’t. (50 years, baseline interview)
Finally, watching family members experience weight-related health issues was a strong motivation. The fear of dying prematurely pushed people to sign up for the HP-DPP.
Most respondents reported that their motivation to lose weight increased over time (Table 4). The frequency of group sessions decreases from approximately weekly in the first 6 months of the program (“core” sessions) to biweekly and then monthly in the latter 6 months of the program (“core maintenance” sessions). The decreased frequency is designed to encourage participants to become more self-reliant to maintain their behavior change after the program concludes. But this change in program cadence generated anxiety among participants that they could lose the accountability and motivation they needed to stay on track toward their goals. “Oh, I hate it. I hate it [reducing the frequency of meetings]. I really, I mean, but I understand but that it’s part of the program to get us to take responsibility for ourselves” (>65 years, midpoint interview). With the support from program participants, coaches, and from friends and family, most participants were able to maintain their motivation throughout the program, but it was perceived as more difficult.
Participants reported that accountability from the health coach and group resulted in real changes to their behaviors and how they felt about themselves suggesting group dynamics have a strong impact on motivation even when the HP-DPP is delivered via distance learning. Participants were particularly motivated by others’ successes. Some of the competitive participants wanted to be the group member who lost the most weight or made the most improvements; every time a member of the group reported weight loss, they took it as a challenge to push harder and possibly exceed their expectations. For others, fear of being seen as a failure by other group members was enough to motivate them:
The most helpful was having that support group to hear other people say what they struggled with, what they did to help their struggles. So to me, the support group was a great part of the entire program because you actually had real people who were on the same program as you and they understood your struggles, you understood their struggles. We fed off of each other. So I think that was the most important thing is that we fed off of each other, and what I can take away from this is that you’re not in this alone. (48 years, endline interview)
Skills Developed by Participants
The skills participants developed throughout the sessions included tracking physical activity and food intake, problem-solving, and troubleshooting to overcome obstacles to healthy eating and increased physical activity (Table 5). Examples of digital tools employed in the program included MyFitnessPal to log food, Fitbit activity trackers, and wireless scales. Some of the participants who did not have much experience in using these digital tools before the program reported improvement in their technical skills. However, challenges remained, particularly among older participants. The most common complaint stemmed from the use of videoconference technology for the group sessions. One participant explained “. . . a lot of people are like me, that aren’t terribly tech savvy. I haven’t gotten used to using the Teams channel, and it’s just hard for me—(55-year-old baseline interview). Participants frequently reported issues with the breakout sessions, audio issues, and finding files associated with the program. The Fitbit and wireless scales were seen as useful for those who chose to use them:
I really like the accountability of getting that Fitbit and the scale. I really felt it was almost like you were in this, you were really in a program, because you got this package of stuff, and the accountability. (48 years, endline interview) With the fitness apps we have, the Fitbit, we have done friend groups, where we can encourage. We can see as people are logging their food. We can encourage each other, which is nice, because before if I had my Fitbit, or whatever, it was just me watching me. (48 years, endline interview)
Behavioral Skills.

Participants reported the most valuable skill they developed was learning to track physical activity and food intake:
Well, boiled down to a nutshell, it’s the technology that allows me to easily and accurately keep track of my nutrition. And, visually seeing that and keeping track of those nutritional goals has motivated me, and extremely well. And so, it’s the knowledge that is gained from the program, which is unquestioned, and the technology that enables me to manage my intake far better than I’ve ever done before combined. I think that’s what I attribute the success to. (>65 years, midpoint interview)
Through tracking, participants became more accountable for their actions and learned to adjust their routines depending on their progress throughout the week. Tracking food intake enabled participants to understand the nutritional breakdown of their meals and snacks while tracking physical activity allowed participants to see if/how they were meeting their daily physical activity goals.
Discussion
Our study highlights the impact of a distance learning delivery platform for the HP-DPP on participant motivation, knowledge, and behavioral skills throughout the 12-month program. Participants valued the information provided by the coaches and felt that sessions helped them develop the skills they needed to lose and maintain behavior change. The support from coaches and other participants increased their motivation to change their behavior. Among those comfortable with using video teleconference software, the use of technology to assist them with tracking healthy behaviors, coupled with the relationships they developed during the program, facilitated their success. When sessions transitioned from weekly to monthly, almost all participants were concerned about their ability to maintain the motivation and healthy behaviors that helped them lose weight early in the program. Our findings suggest that a distance learning DPP delivers key inputs to prompt behavior change (knowledge, motivation, and behavioral skills) as described in the IMB model. The addition of distance learning may facilitate greater program reach, to individuals unable to attend in-person sessions, but comes with the added challenge of training people to use potentially unfamiliar platforms.
While the mechanisms of DPP success implicitly include improvements in knowledge, motivation, and skills related to healthy eating and physical activity, many programs do not assess how the program affects these dimensions (Chawla et al., 2019; Ho et al., 2008; Miles et al., 2022; Whittemore et al., 2009). Our distance learning HP-DPP participants highlighted the importance of learning to read labels and understanding the quantity they should eat daily. Prior studies of in-person DPP participants have found that dietary changes, spurred in part by improvements in knowledge, tend to be maintained for many years (Jaacks et al., 2014) and are correlated with weight loss maintenance (Laz et al., 2015). Our participants learned that physical activity could take many forms and be broken up throughout the day. Participants in DPPs who increase their physical activity significantly reduce their risk of developing diabetes (Kriska et al., 2020), highlighting the importance of encouraging sustainable lifestyle changes during the program.
We were concerned that participation in the HP-DPP via distance learning could limit meaningful interactions with other group members, decreasing motivation to continue in the program. Studies have shown that group interaction within a DPP can foster accountability, and lead to improved success in the program (Gruß et al., 2022; Metzgar et al., 2015; Mohr et al., 2011). A prior study of online DPP delivery found that participants did not experience the accountability component, given limited interaction with group members (Gruß et al., 2022). Both online and distance learning platforms are recognized as virtual DPP delivery options, but they differ markedly in the synchrony of interactions with peers and coaches. In online platforms, participants engage in asynchronous interactions with peers and coaches outside of the time they spend completing self-paced sessions; in distance learning platforms, participants interact with peers and coaches synchronously during group sessions (similar to in-person platforms) (Cannon et al., 2022). Unlike prior reports from online participants, our distance learning participants reported feeling accountable to the group, particularly the desire not to fail peers who are all striving for the same goal, as an important source of motivation. Indeed, when sessions became less frequent, the most common fear among participants was the loss of accountability that group sessions provided.
Limitations
This study has limitations. First, we evaluated a single employer based DPP. Most participants were non-Hispanic white, women, and all participants were employed, which limits the generalizability of our results to more vulnerable populations who are at higher risk for prediabetes and T2DM (Haw et al., 2017). Second, we conducted these interviews during the COVID-19 public health emergency, when many facilities for in-person activities (including workplaces, restaurants, and gyms) were closed or operating modified schedules. Thus, participant behavior may have been influenced by lifestyle changes imposed by the public health emergency, independent of their participation in the HP-DPP. Finally, the focus of this evaluation was limited to the impact of a distance learning DPP on changes in participant information, motivation, and behavioral skills associated with program success.
Despite these limitations, this study fills an important gap in knowledge about DPP delivery via distance learning at a critical point in National DPP implementation and dissemination efforts. The COVID-19 pandemic prompted in-person DPPs to rapidly shift to distance learning; this shift seems likely to be sustained long-term (alone or in combination with in-person options), given overall trends in telehealth use and preferences expressed by patients and providers during and after the COVID-19 pandemic (Shaver, 2022). Sustaining a distance learning participation option may be especially valuable to employers seeking to make the program accessible to employees who now have greater flexibility in where they can work (i.e., on-site, remote, and hybrid) (Peters et al., 2022).
Conclusions
This study highlights the feasibility of delivering the DPP via distance learning without losing key programmatic “inputs” identified in the IMB model that prompt behavior changes for diabetes risk reduction. These elements include knowledge about healthy eating and physical activity, group interactions to motivate participants, and behavioral skills to facilitate tracking and overcoming psychological barriers to weight loss. With the increase in employees working from home, distance learning may improve program accessibility. Future research comparing the effectiveness of distance learning and in-person DPP delivery in terms of key health outcomes such as weight loss will further inform efforts to improve the reach of these important programs.
Footnotes
Acknowledgements
The authors would like to thank the participants for providing comprehensive feedback on the HP-DPP.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The National Institute of Diabetes and Digestive and Kidney Diseases (R01 DK120814) supported the salaries of the authors.