
Abstract
Background
Concussion education is recommended to increase concussion knowledge, beliefs, and reporting intentions. The Concussion Awareness Training Tool for Youth (CATT-Youth) is a 40-minute e-Learning module developed for high school–aged youth.
Aim
The aim of the study was to evaluate changes in concussion knowledge, beliefs, and reporting intentions in high school youth from Calgary, Canada, following completion of the CATT-Youth
Methods
This study used a modified stepped-wedge trial design. High school classes were randomly assigned to an intervention (Ix) or delayed intervention (DIx) group. Ix group participants completed a pre-CATT survey immediately followed by the CATT-Youth, then a post-CATT survey 2 to 6 weeks later. DIx group participants completed two pre-CATT surveys 2 to 6 weeks apart, with the CATT-Youth completed immediately following the second pre-CATT, then a post-CATT survey 2 to 6 weeks later. The pre-/post-CATT survey encompassed 11 subtests evaluating concussion knowledge, beliefs, and reporting intentions. Independent mixed linear regression models were conducted to examine changes in scores for each subtest.
Results
Participants included 454 high school students: five Ix schools (16 classes, n = 323) and two DIx schools (six classes, n = 131). The CATT-Youth significantly increased general concussion knowledge, Ix δ = 0.546/8 (95% confidence interval [CI] = [0.243, 0.849]), DIx δ = 0.728/8 (95% CI = [0.389, 1.106]), and beliefs about capabilities, Ix δ = 2.462/28 (95% CI = [1.086, 3.838]), DIx δ = 3.219/28 (95% CI = [1.594, 4.844]) for both groups. For some subtests, improvements were noted in the DIx group only.
Conclusion
The CATT-Youth module improved concussion knowledge and beliefs about capabilities for students in both groups. Future studies should explore the utility of the CATT-Youth in changing knowledge, beliefs, and reporting intentions in high school students.
Concussions are commonly occurring injuries, with approximately 25% of youth reporting a concussion in their lifetime (Veliz et al., 2017, 2021). Despite the high prevalence of concussion, it is likely that many go unreported (Meehan et al., 2013). Concussions result in signs and symptoms that can affect a youth’s ability to engage in daily life, school, and sports (Purcell et al., 2019; Reed et al., 2021). As there are many possible signs and symptoms of concussion, this injury may not be obvious to youth (McCrory et al., 2017; Reed et al., 2021). Concussion education is suggested to increase knowledge in youth, and concussion education is a mechanism to change concussion-related attitudes and reporting intentions (Chandran et al., 2020; Glang et al., 2015; Kroshus et al., 2015; Mallory et al., 2022; Register-Mihalik et al., 2013, 2018).
Over the past 10 years, there has been increased awareness of the importance of concussion education for youth. Recent cross-sectional survey studies assessed differences in concussion-related behavior change domains, including knowledge, intentions, or attitudes, at a single point in time (Chandran et al., 2020; Glang et al., 2015; Register-Mihalik et al., 2013, 2018). Although these studies may describe a change in short-term knowledge, the observed change is less demonstrative of future behavior if retained learning is not examined. One study measured concussion knowledge and attitudes at multiple time points and showed increased knowledge scores were maintained beyond the initial posteducation time point, but no long-term changes were observed for attitudes or behaviors (Caron et al., 2018). In addition, a scoping review showed inconsistent findings when trying to establish whether concussion education is maintained long-term (Ramsay & Dahinten, 2020). However, many concussion education studies reporting changes to concussion knowledge in the shorter or longer (i.e., 2–6 months) terms referred only to concussion knowledge, and not to other behavior change indicators (Ramsay & Dahinten, 2020).
Behavior change theories, such as the Theory of Planned Behavior, Health Belief Model, and Social Norms Theory (Ajzen, 1991; Perkins & Berkowitz, 1986; Strecher & Rosenstock, 1997), are used to design interventions to address concussion knowledge and behaviors in youth populations. Although the use of theory in concussion education has increased over time, Caron and colleagues (2018) showed that a change in concussion knowledge does not necessarily lead to changes in attitudes, behaviors, or intentions. Caron et al.’s (2018) study highlighted that education may change knowledge, but not necessarily change behavior, which is consistent with findings from other prospective cohort and cross-sectional studies (Carpenter et al., 2020; Kroshus et al., 2014, 2015).
Education appears to be less effective at improving knowledge and attitudes when not theory-based or based loosely on theory (Albarracín et al., 2005; Michie & Prestwich, 2010). The Theoretical Domains Framework is an amalgamation of behavior change theories compiled and validated by experts, encapsulating individual and systems-level constructs (Atkins et al., 2017; Cane et al., 2012). The Concussion Awareness Training Tool for Youth (CATT-Youth), adapted from the CATT for Athletes, was developed using the Theoretical Domains Framework to provide evidence-informed education, tailored to high-school-aged youth, and incorporates behavior change strategies to increase the uptake of concussion reporting and management behaviors (Atkins et al., 2017; Cane et al., 2012).
The objective of this study was to evaluate changes in concussion knowledge, beliefs, and reporting intentions among high school students following completion of the CATT-Youth e-Learning module.
Impact Statement
The CATT-Youth e-Learning module increases general concussion knowledge and increases beliefs about capabilities, or the confidence to recognize and report concussion symptoms, for high school students. The CATT-Youth is freely accessible, available in French and English, and can be implemented in high schools and community youth sports associations to promote concussion education.
Methods
Study Design
This modified stepped-wedge trial was designed with two groups, a rolling recruitment schedule, and 2- to 6-week periods between data collection points. The second postintervention follow-up of the intervention group (Ix) was omitted to reduce participant burden. The Ix was surveyed twice, once before the intervention (pre-CATT) and once following completion of the CATT-Youth (post-CATT). The delayed intervention group (DIx) was surveyed at three time points, twice before the intervention (pre-CATT1, pre-CATT2) and once following completion of the CATT-Youth (post-CATT). Change in survey scores from pre-CATT to post-CATT was examined in both groups and compared between groups (Ix: pre-CATT to post-CATT; DIx: pre-CATT2 to post-CATT). The change during the control period in the DIx group (pre-CATT1 to pre-CATT2) was compared with the change from pre-CATT to post-CATT in both groups. The Conjoint Health Research Ethics Board (REB 18-2107) provided ethical approval for this study.
Participants
From December 2021 to June 2022, high schools partnered with the Surveillance in High Schools and Community Sport to Reduce Concussions and their Consequences (SHRed Concussions) research program in Calgary, Canada, were invited to participate in the current study. Schools were onboarded when the sports medicine class teachers expressed interest. Sports medicine is an optional course for high school students and there are three levels: introductory, intermediate, and advanced. All three levels of sports medicine classes were recruited for participation in this study. Sports medicine classes were selected as they include a concussion education module per the curriculum; thus, the CATT-Youth could be used for curricular content for the sports medicine course. Students could individually opt-in to participate in the study. All participants provided either electronic consent or electronic assent with parental/guardian consent.
Procedure
Eligible high schools (n = 12) were randomly assigned to the Ix group or DIx group. Participating classes were onboarded and nested within the arm to which the school was randomized. Students could access the CATT-Youth e-Learning module even if they chose not to participate.
The study was implemented during class time within each sports medicine class. Participants in the Ix group completed a demographic questionnaire and the baseline (pre-CATT) survey, then immediately completed the CATT-Youth e-Learning module. Two to six weeks later, they completed the follow-up survey (post-CATT). Participants in the DIx group completed a demographic questionnaire and the first baseline survey (pre-CATT1). Two to six weeks later, they completed the second baseline survey (pre-CATT2), followed by the CATT-Youth e-Learning module and then 2 to 6 weeks later, they completed the post-CATT survey. The 2-to-6-week timeline allowed flexibility for classes to complete the surveys and the timeline was in collaboration with teachers in each participating class. See Figure 1.

Flowchart of Modified Stepped-Wedge Design.
Concussion Awareness Training Tool for Youth
The CATT-Youth is a 40-minute e-Learning module that provides up-to-date, evidence-informed concussion education (e.g., Consensus Statement on Concussion in Sport, Canadian Guideline on Concussion in Sport, Living Guideline for Pediatric Concussion Care; McCrory et al., 2017; Parachute, 2017; Reed et al., 2021). It is available in English and French. The language and the examples used are developmentally appropriate for high-school-aged youth. The CATT-Youth employs a variety of learning techniques (e.g., videos, personal experience stories, graphics, text). Youth are guided through six topic areas: What is a concussion? Do I have a concussion? Why is reporting a concussion important? How can a concussion affect my life? What is my road to recovery from a concussion? and How can I cope with concussion? A certificate of completion is available following completion of the module.
The CATT-Youth was adapted from the CATT for Athletes module, developed for high-performance athletes, and modified to include information relevant to high-school-aged youth. The CATT-Youth development included five iterations. The CATT-Youth module underwent content validation and face validation. Content validation was completed by 14 members of the project team with expertise in concussion and knowledge translation. The team members reviewed module content and provided feedback via Zoom meetings and email. Face validation was completed with four high-school-aged youth (n = 3 females, 1 male) via one Zoom focus group.
Measurement Tool
The pre-/post-CATT survey was adapted by the project team from the survey designed to evaluate the CATT for Athletes. The pre-/post-CATT survey was developed in alignment with the Theoretical Domains Framework (Atkins et al., 2017; Cane et al., 2012). It underwent face validation with seven high-school-aged youth (n = 5 females, 2 males) via three Zoom focus groups and one in-person one-on-one interview.
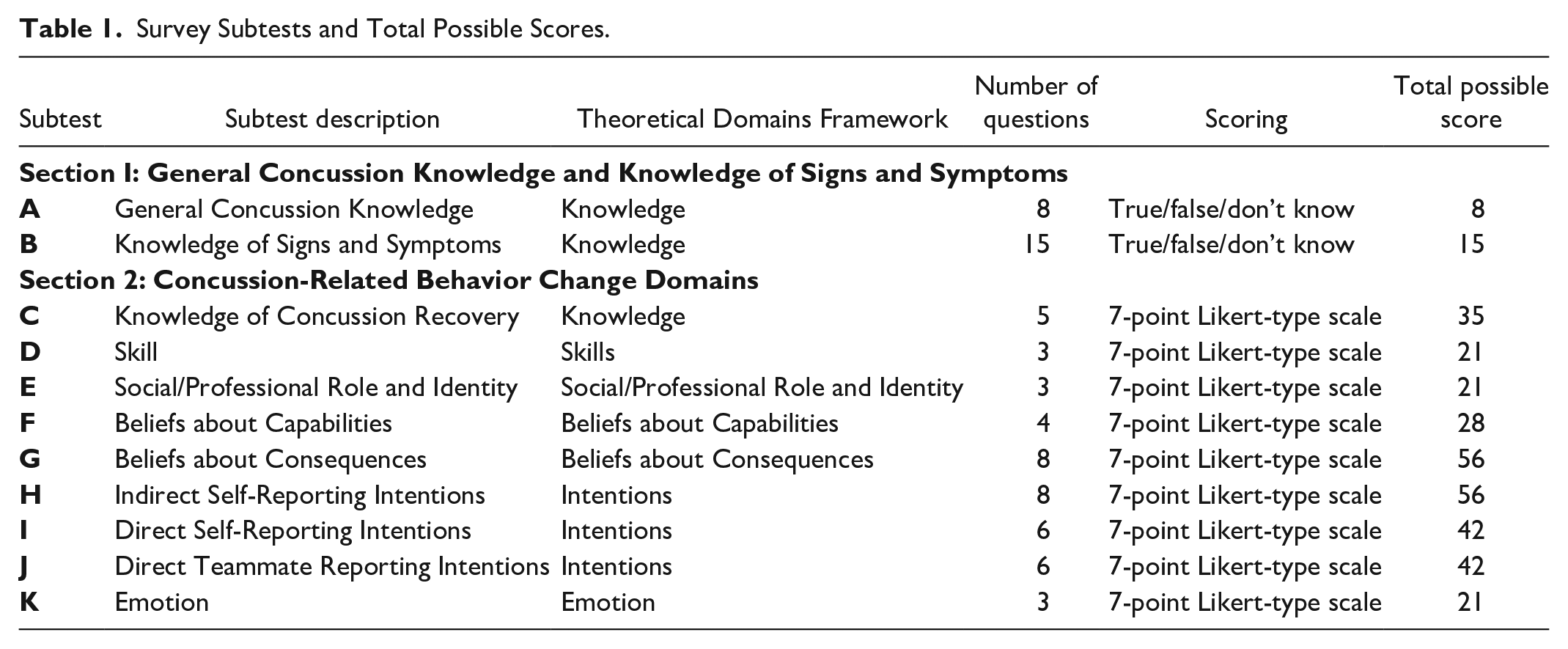
The survey was divided into two sections: Section 1 evaluated general concussion knowledge and knowledge of concussion signs and symptoms using true-yes/false-no/don’t know questions; Section 2 evaluated agreement using a 7-point Likert-type scale (completely disagree to completely agree). The survey contained 11 subtests (Table 1), encompassing 7 of 14 domains from the Theoretical Domains Framework (Atkins et al., 2017; Cane et al., 2012), and took approximately 15 minutes to complete (Supplementary A).
Survey Subtests and Total Possible Scores.
The study data were collected and managed using REDCap (Research Electronic Data Capture), hosted at University of Calgary (Harris et al., 2009, 2019; REDCap, n.d.). REDCap is a secure, web-based software platform designed to support data capture for research studies (REDCap, n.d.).
Statistical Analyses
Independent mixed linear regression models were conducted to examine changes in pre-CATT to post-CATT scores for each of the 11 subtests, with fixed effects for test occasion and randomization arm while also including an interaction of the two terms. To produce a flexible correlation structure, a four-level model was fit with a random effect for classroom, cross-classified specification for test occasion nested within classroom, and individual students nested within classroom. A small sample correction was applied using Kenward-Roger degrees of freedom and restricted maximum likelihood to account for the small number of classrooms randomized to each arm (Hooper et al., 2018). This formulation allowed for an examination of both mean changes from pre-CATT to post-CATT scores overall, and examined whether overall changes from pre-to post-CATT were attributable to the intervention above and beyond potential learning effects seen in the DIx group, referred to as mean unbiased change (MUC). In addition, this allowed verification of whether there were learning effects in the DIx group by examining mean changes from pre-CATT1 to pre-CATT2.
Models were adjusted for sex, grade, concussion history, previously learning about concussion, and number of weeks between completion of the CATT-Youth and the post-CATT survey. An additional term was tested, defined by each of the control variables (excluding weeks since entry) interacting with the test occasion. This enabled testing the effects that each of the control variables may have had on change in scores, achieved by computing linear combinations of parameters tested (z test) against zero for each cell, and retained if any linear combinations were associated with changes in knowledge, beliefs, or reporting behavior scores. Overall significance of categorical variables with more than two levels was obtained using a Wald chi-square test. In this analysis, all participants with a complete set of covariate responses were included in Section 1 (general concussion knowledge and knowledge of signs and symptoms). Only participants who selected “yes” to participation in organized sport or physical activity in the demographic survey were included for Section 2 questions, as some questions related to experience in sport or physical activities, to which students who did not participate in sport would not have a reference point for response. In addition, Cronbach’s alpha was computed for each of the 11 subtests at each time point individually and both pre-CATT scores were averaged to examine internal consistency (Supplementary B).
Results
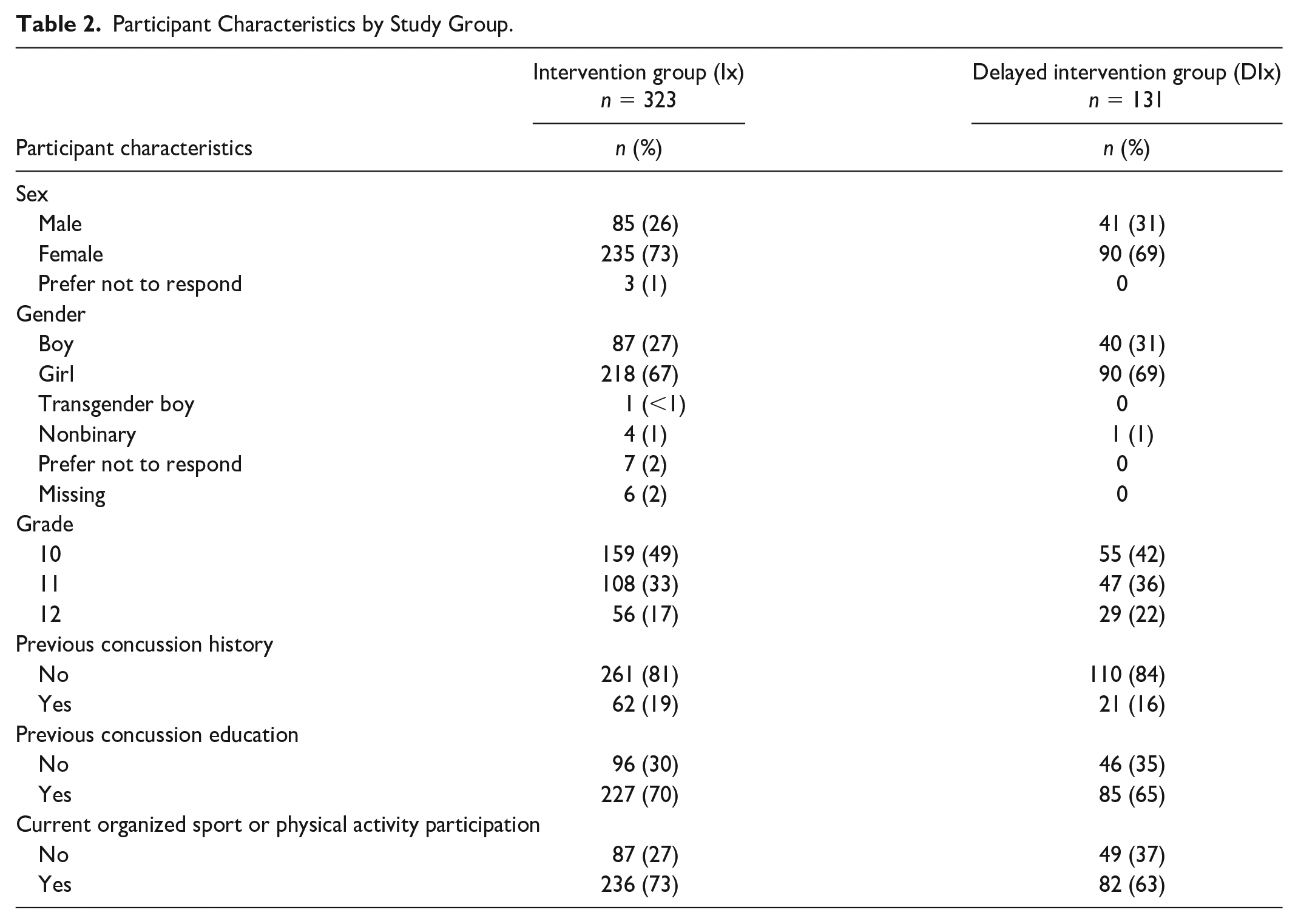
Participants included 454 high school sports medicine students in Grades 10 to 12 (Table 2). Three students from the Ix group opted to not report their sex, resulting in small cell sizes. These participants were dropped from the final analysis. One participant provided no responses for the general concussion knowledge questions at any time point but was included for subsequent analyses where they contributed valid responses.
Participant Characteristics by Study Group.
Teachers in seven of the 12 eligible schools agreed to participate. Reasons for nonparticipation included scheduling difficulties, lack of class time, and limited teacher engagement. The original 12 schools with initial agreement to participants were randomized into the Ix or DIx groups. Five schools in the Ix group (n = 16 classes) and two schools in the DIx group (n = 6 classes) participated in the study. The time between pretest and posttests was targeted for 2 to 6 weeks (see Figure 1). The mean time to completion overall was 3.9 weeks. For the Ix, the mean time from pre-CATT to post-CATT was 4.2 weeks, and for the DIx, the mean time from pre-CATT1 to pre-CATT2 was 3.0 weeks and from pre-CATT2 to post-CATT was 3.4 weeks. The unadjusted mean changes for the 11 subtests, by group and occasion, are detailed in Supplementary C. Overall, internal consistency of the 11 subtests at each time point individually, and averaging both pre-CATT scores, was found to be moderate using Cronbach’s alpha (Supplementary B).
Section 1: General Concussion Knowledge and Knowledge of Signs and Symptoms
The model derived for the change in general concussion knowledge following completion of the CATT-Youth included 450 participants with 789 observations. A total of 319 participants were included from the Ix group, of whom 156 had both pre-CATT and post-CATT records. Of the 131 participants in the DIx group, 68 had a complete record (two pre-CATT records and post-CATT record), nine had one pre-CATT record and post-CATT record, and 54 had only a pre-CATT record.
General concussion knowledge scores significantly increased from pre-CATT to post-CATT, with a mean overall change across groups of 0.647/8 (95% confidence interval [CI] = [0.365, 0.929]; Table 3, Figure 2a). The mean change in general concussion knowledge from pre-CATT to post-CATT significantly increased in both groups, with the Ix group increasing by 0.546/8 points (95% CI = [0.243, 0.849]) and the DIx group by 0.728/8 (95% CI = [0.389, 1.106]). The MUC was significant with a 0.666/8 increase from pre- to post-CATT (95% CI = [0.308, 1.024]). Previously learning about concussion increased general concussion knowledge, while sex, grade, and history of concussion were not significantly associated (Supplementary D, Table D1). Although grade was not found to be significantly related to overall general knowledge, it was associated with changes over time. The marginal predicted scores from the fully adjusted model, showing the increase in general knowledge by intervention group, are displayed in Figure 2a.
Changes to Concussion-Related Behavior Change Domains Following Administration of the CATT-Youth.
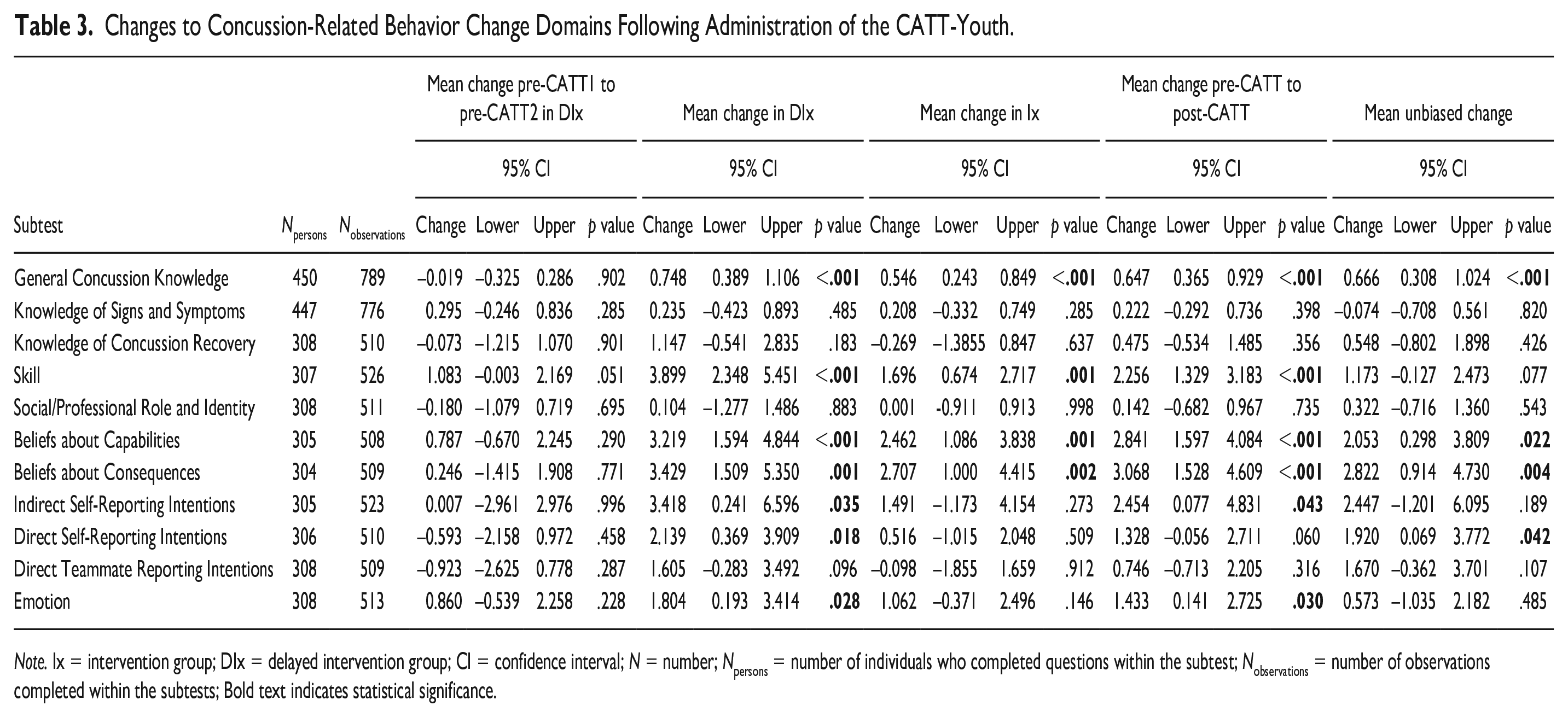
Note. Ix = intervention group; DIx = delayed intervention group; CI = confidence interval; N = number; Npersons = number of individuals who completed questions within the subtest; Nobservations = number of observations completed within the subtests; Bold text indicates statistical significance.
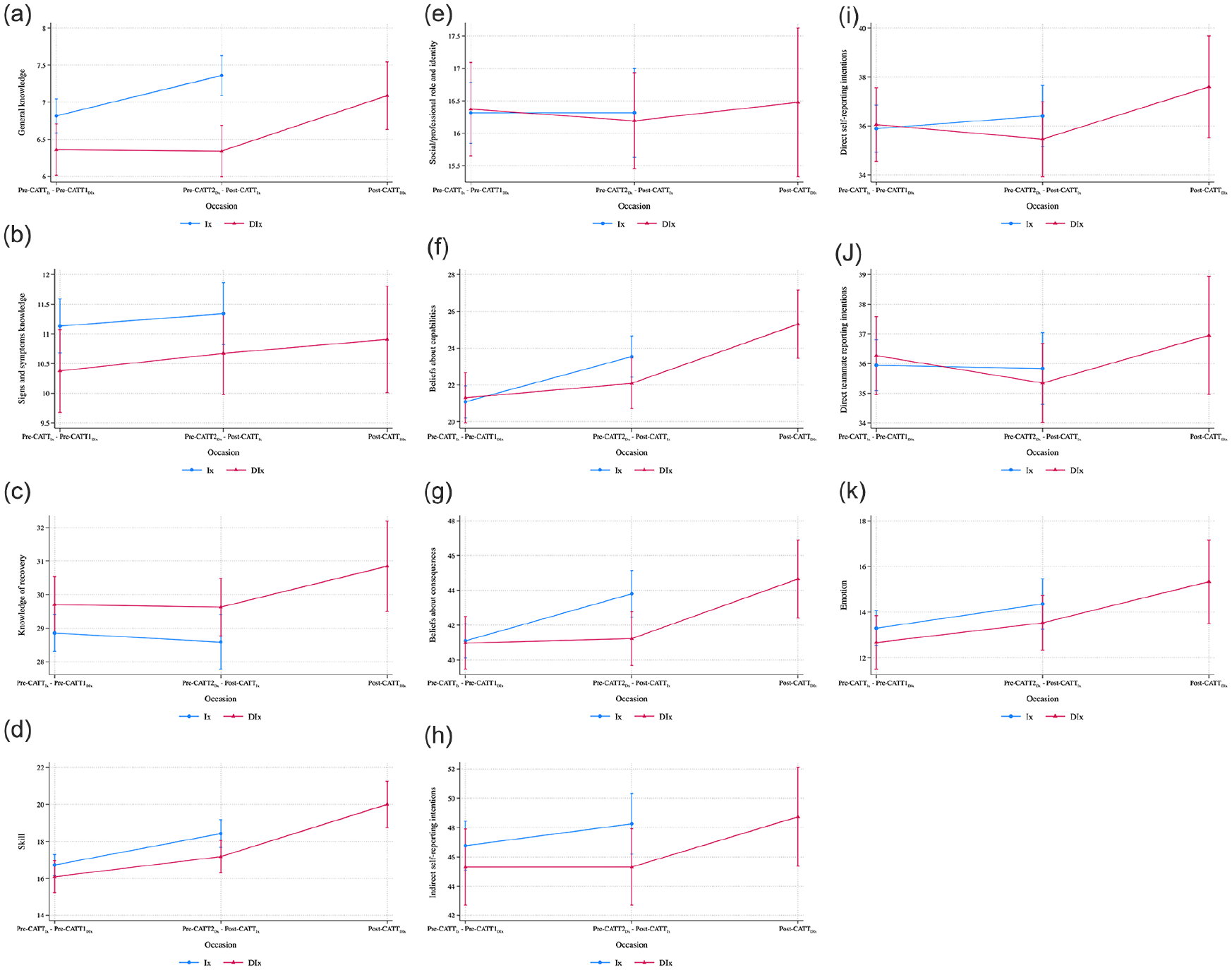
Adjusted Subtest Scores Over Test Occasion From the Mixed Effects Model: (a) General Concussion Knowledge; (b) Knowledge of Signs and Symptoms; (c) Knowledge of Concussion Recovery; (d) Skill; (e) Social/Professional Role and Identity; (f) Beliefs About Capabilities; (g) Beliefs About Consequences; (h) Indirect Self-Reporting Intentions; (i) Direct Self-Reporting Intentions; (j) Direct Teammate Reporting Intentions; (k) Emotions.
The mean change in knowledge of signs and symptoms did not significantly improve from pre-CATT to post-CATT in either group, Ix: δ = 0.208/15 (95% CI = [–0.332, 0.749]), DIx: δ = 0.235/15 (95% CI = [–0.423, 0.893]), nor were there significant overall changes (Table 3; Figure 2b). Sex and grade were significantly associated with changes in knowledge of signs and symptoms over time; however, sex, grade, concussion history, and previous learning about concussion were not significantly associated with overall changes (Supplementary D, Table 2D).
Section 2: Concussion-Related Behavior Change Domains
In total, 307 participants were included in the final model for the nine subtests analyzed using a 7-point Likert-type scale (Table 1), resulting in 507 observations. The Ix group comprised 233 participants, with 101 completing both the pre-CATT and post-CATT surveys, 131 completing only the pre-CATT survey, and one completing only the post-CATT survey. For the DIx group, 74 participants were included in the analysis, 35 of whom had a complete record, 36 with only pre-CATT records, and three with one pre-CATT and one post-CATT record.
Knowledge of Concussion Recovery, Skills, and Social/Professional Role and Identity
Knowledge of concussion recovery did not change significantly on the aggregate nor on the MUC (0.548/35, 95% CI = [–0.802. 1.898]). No changes were observed by group, nor any learning effects in the DIx group (Table 3; Figure 2c). The final model showed significantly higher scores in females relative to males, while linear combinations from the interaction term retained showed that, within Grade 12, the change from pre-CATT to post-CATT was significantly larger in the delayed group than the intervention group (Supplementary D, Table 3D).
Skills changed significantly on the aggregate (δskills = 2.256/21, 95% CI = [–1.329, 3.183]) and neared significance when removing the potential learning effects (MUC = 1.173/21, 95% CI = [–0.127, 2.473]; Table 3; Figure 2d). The final model showed participants who had previously learned about concussions had a significantly lower score relative to those without previous concussion education (Supplementary D, Table 4D).
The social/professional role and identity questions did not significantly change from pre- to post-CATT scores in either group on the aggregate or MUC (Table 3; Figure 2e). The final model showed females scored significantly higher on this subtest, and older (Grades 11 and 12) students performed better than younger (Grade 10) students (Supplementary D, Table 5D).
Beliefs About Capabilities and Beliefs About Consequences
Beliefs about capabilities and beliefs about consequences showed significant increases in both Ix and DIx groups (Ix δcapability = 2.462/28, 95% CI = [1.086, 3.838]; DIx δcapability = 3.219/28, 95% CI = [1.594, 4.844]; Ix δconsequences = 2.707/28, 95% CI = [1.000, 4.415]; DIx δconsequences = 3.429/28, 95% CI = [1.509, 5.350]), with both mean changes and the MUC remaining significant (δcapability = 2.841/28, 95% CI = [1.597, 4.084]; MUC = 2.053/28, 95% CI = [0.298, 3.809]; δconsequences = 3.068/28, 95% CI = [1.528, 4.609]; MUC = 2.822/28, 95% CI = [0.914, 4.730]) (Table 3; Figure 2f and g). Previously learning about concussion was significantly related to overall beliefs about capabilities (Supplementary D, Table 6D). Females were significantly more likely to disagree that there are consequences to reporting a concussion, but no differences in beliefs about consequences were seen in students from higher grades or in those with a history of concussion (Supplementary D, Table 7D). For beliefs about capabilities and consequences, prior learning about concussion was associated with smaller changes from pre-CATT to post-CATT.
Indirect Self-Reporting Intentions, Direct Self-Reporting Intentions, and Direct Teammate Reporting Behavior Intentions
Indirect self-reporting showed significant improvements from pre-CATT to post-CATT overall (δindirect = 2.454/56, 95% CI = [0.077, 4.831]) and for the DIx group (DIx δindirect = 3.418/56, 95% CI = [0.241, 6.596]). However, when accounting for changes in pre-CATT measurements within the DIx group, the MUC was not significant (MUC = 2.447/56, 95% CI = [–1.201, 6.095]; Table 3; Figure 2h). Median scores for indirect self-reporting intentions were 48/56 on the pre-CATT. Previously learning about concussion was associated with a reduced change from pre-CATT to post-CATT (Supplementary D, Table D8).
Overall, there were no significant changes for direct self-reporting intentions. The MUC was significant when accounting for changes in pre-CATT measurements within the DIx group (MUC = 1.920/42, 95% CI = [0.069, 3.772]; Table 3; Figure 2i) and only the DIx group showed significant improvements in direct self-reporting intentions from pre-CATT to post-CATT (DIx δdirect self-reporting = 2.139/42, 95% CI = [0.369, 3.909]). Median scores for direct self-reporting intentions were 36/42 on the pre-CATT. Previously learning about concussion was associated with a reduced change from pre-CATT to post-CATT. Being female was associated with overall higher scores (Supplementary D, Table D9).
For direct teammate reporting intentions, neither group (Ix, DIx) showed a change from pre- to post-CATT, nor were the mean changes or the MUC significant (Table 3; Figure 2j). Median scores were 36/42 on the pre-CATT. There was a sex effect for direct teammate reporting intentions; females improved while males did not (Supplementary D, Table D10).
Emotion
The DIx group showed a significant increase in emotion, such as increased comfort and decreased nervousness when reporting a concussion, from pre-CATT to post-CATT (δemotion = 1.804, 95% CI = [0.193, 3.414]), while the change for the Ix group was not significant (δemotion = 1.062, 95% CI = [–0.371, 2.496]) (Table 3; Figure 2k). The overall change remained significant on the aggregate (δemotion = 1.433, 95% CI = [0.141, 2.725]), but the MUC showed the overall unbiased change was not significant (MUC = 0.573, 95% CI = [–1.035, 2.182]). Grade 12 students showed higher overall scores relative to Grade 10 students (Supplementary D, Table D11).
Discussion
This study aimed to evaluate changes in concussion knowledge, beliefs, and reporting intentions of high-school-aged youth following completion of the CATT-Youth concussion e-Learning module. Completion of the CATT-Youth resulted in significant improvements to general concussion knowledge, skills, beliefs about capabilities, and beliefs about consequences for both Ix and DIx group participants. Significant improvements were observed for indirect self-reporting intentions, direct self-reporting intentions, and emotion for only DIx group participants. No significant improvements were observed for either group on knowledge of signs and symptoms, knowledge of concussion recovery, or direct teammate reporting intentions. Females demonstrated significantly higher scores than males for knowledge of concussion recovery, social/professional role and identity, and beliefs about consequences.
Through an exploratory analysis of the knowledge of signs and symptoms subtest, examining solely true signs and symptom scores of concussion (i.e., excluding “distractor” symptoms), most participants correctly identified all concussion signs and symptoms both pre- and post-CATT (7/7). Thus, the distractor signs and symptoms added variability. Changes to the CATT-Youth module to address both “true” and “distractor” signs and symptoms may be warranted to better support youth to delineate concussion symptoms.
Although previously learning about concussions increased general concussion knowledge scores, it was associated with lower skills scores. An explanation may be that the information presented in the CATT-Youth, or previous concussion education, contrasted participants’ previous experiences with the items on the skills subtest (e.g., when to seek support, who to ask for support). This highlights the importance of not only providing education to improve knowledge but also providing strategies to change concussion-related reporting and management behaviors in youth. Moreover, youth scored moderate-to-high on preintervention skill, at 75% to 82%, measured by three questions, providing small opportunity for change.
Preintervention scores were high (>80%) for knowledge of concussion recovery and indirect self-reporting intentions, which may have limited the ability to achieve significant improvement. Also, direct self-reporting and direct teammate reporting intentions had high (>80%) preintervention scores and no overall changes postintervention. This may be due to limited opportunity to improve. Alternatively, direct self-reporting and teammate reporting intentions may be a stable state for individuals, as previous studies showed a decreased likelihood of changes to domains pertaining to intentions to report symptoms of concussion (Beran & Scafide, 2022; Kroshus et al., 2015; Sullivan & Molcho, 2018; Weber Rawlins et al., 2020). Furthermore, reporting a concussion may be associated with reporting skills and self-efficacy, rather than knowledge alone (Warmath & Winterstein, 2019), and concussion education modules may not be sufficient to change reporting skills and self-efficacy surrounding reporting intentions. Future iterations of the CATT-Youth could integrate ways to improve reporting skills into the module. In addition, females were more likely to report a concussion (direct self-reporting intentions) or report a peer’s suspected concussion (direct teammate reporting intentions), than males. Beran and Scafide (2022) noted similar reporting-related sex differences in their systematic review. Future research could explore the drivers behind sex and gender differences on concussion reporting intentions and reporting behaviors in youth.
Previously learning about concussion was associated with higher general concussion knowledge among youth and beliefs about capabilities. Smaller improvements in both indirect and direct self-reporting intentions were also seen among youth with previous concussion education, potentially due to less opportunity for improvement. There are limits to what an educational intervention can accomplish in isolation of specific strategies to address the behaviors intended to be targeted by the education intervention.
The Theoretical Domains Framework can be used in conjunction with the COM-B (Capability-Opportunity-Motivation Behavior) model and the Behavior Change Wheel to target future concussion education interventions with the goal of influencing concussion-related reporting and management behaviors (Michie et al., 2014). For example, direct concussion reporting intentions for self or teammate could be mapped to the Motivation and Opportunity domains of the COM-B (Michie et al., 2011, 2014). The Behavior Change Wheel could be used to characterize which interventions may be used to drive behavior change. Reflective motivation can be changed through education, persuasion, and incentivization, while opportunity can be changed through changing the environment (Michie et al., 2011). Thus, to change intentions to report a concussion in a youth population, concussion education could be partnered with environmental changes such as fostering an environment that promotes reporting or incentivizing reporting of concussion symptoms (Sullivan & Molcho, 2016). Future interventions should incorporate both education and environmental changes, which involves organizations, leaders, and youth.
Strengths and Limitations
This study has many strengths. First, this study is one of the first to evaluate concussion-related behavior change domains in a youth sample beyond a single time point. Second, the evaluation of the CATT-Youth was developed in alignment with the Theoretical Domains Framework, which encapsulates multiple behavior change theories (Atkins et al., 2017; Cane et al., 2012). The use of the Theoretical Domains Framework aimed to create a behavior-modification-driven tool to understand and address knowledge, beliefs, and reporting intentions associated with concussion management behaviors (Atkins et al., 2017; Cane et al., 2012). Third, the CATT-Youth e-Learning module underwent content and face validation. Also, the constructs within the survey demonstrate moderate internal consistency.
Study limitations include low buy-in from schools randomized to the DIx group resulting in a smaller sample size than the Ix group, low participant engagement at follow-up, and restricting the analysis of Section 2 of the survey to only those participating in sport and/or physical activities. Also, some classes experienced technical difficulties when accessing the CATT-Youth due to a temporary internal error with the e-Learning system; thus, some participants had to review the material in pairs or small groups, which may have influenced individual engagement with the material. Furthermore, there is still limited and inconsistent evidence to support what is considered “knowledge retention” and there continues to be limited information that outlines the optimal time to assess for knowledge retention following concussion education. Future research should explore the optimal time to evaluate both knowledge retention and changes to behavior following concussion education modules, such as the CATT-Youth.
Implications for Practice
The CATT for Youth is an accessible, online concussion education module that can be incorporated into school and sport curricula for high-school-aged youth. It has demonstrated an ability to increase general concussion knowledge and increases beliefs about capabilities, or the confidence to recognize and report concussion symptoms, for high school students for up to 6 weeks post-education, providing evidence of retained learning. The CATT for Youth may promote positive changes to concussion-related behaviors for youth who may experience concussion, including recognizing and reporting a concussion, the importance of removal from play or activity, and gradually returning to activities.
Conclusion
Concussion education is an important step to encourage concussion recognition, response, and reporting among high-school-aged youth. The CATT for Youth e-Learning module can be freely accessed and can improve general concussion knowledge and increase beliefs about capabilities specific to recognizing and reporting symptoms of concussion for high school students. Overall, students in this study had high concussion knowledge, attitudes, and reporting intentions prior to CATT-Youth administration. Future research could explore differences in sex, gender, age/grade, and previous concussion education, and the mechanisms that drive these factors, in a larger study sample size and evaluate long-term changes to concussion behavior change.
Supplemental Material
sj-docx-1-heb-10.1177_10901981241263577 – Supplemental material for Concussion Awareness Training Tool for Youth: Impact on Concussion Knowledge, Beliefs, and Reporting Intentions
Supplemental material, sj-docx-1-heb-10.1177_10901981241263577 for Concussion Awareness Training Tool for Youth: Impact on Concussion Knowledge, Beliefs, and Reporting Intentions by Heather A. Shepherd, Jean-Michel Galarneau, Matthew Neill, Shazya Karmali, Kate Turcotte, Rylen A. Williamson, Stephanie Cowle, Alison Macpherson, Nick Reed, Kathryn J. Schneider, Kathy L. Belton, Isabelle Gagnon, Amanda M. Black, Carolyn A. Emery and Shelina Babul in Health Education & Behavior
Footnotes
Acknowledgements
The Sport Injury Prevention Research Centre is one of the International Research Centres for Prevention of Injury and Protection of Athlete Health supported by the International Olympic Committee. We acknowledge the support of SHRed Concussions (National Football League Play Smart Play Safe Program) and Integrated Concussion Research Program (University of Calgary). We acknowledge the support of the SHRed research team and the SHRed participants for their engagement in this study. We would like to acknowledge Alex Zheng (BC Injury Research and Prevention Unit) for his assistance in reviewing this manuscript. C.A.E. holds a Canada Research Chair (Tier 1) in Concussion. N.R. holds a Canada Research Chair (Tier 2) in Pediatric Concussion.
Authors’ Note
Heather A. Shepherd is now at the University of Toronto, Toronto, Ontario, Canada.
Amanda M. Black is now at Brock University, St. Catharines, Ontario, Canada.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is aligned with the Surveillance in High Schools and Community Sports to Reduce Concussions and Their Consequences study (SHRed Concussions), which is supported by the National Football League’s Scientific Advisory Board Play Smart Play Safe Program.
Ethical Approval
The study was approved by the University of Calgary Conjoint Health Research Ethics Board (REB #18-2107).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.