
Abstract
Background
Religious institutions play a crucial role in health promotion and hold significant influence in the public health field.
Aim
The aim of this review is to examine outcomes of health-promoting interventions involving the use of mosques as the intervention venue, its role in promoting health behavior change, and the role of theory in each intervention.
Methods
A scoping review was conducted across 17 databases for relevant publications published up to and including August 2023 that involved the use of mosques as the intervention venue. Fourteen articles met inclusion criteria and were reviewed.
Results
The studies featured a wide range of interventions. However, only eight of these studies integrated theoretical frameworks into their approaches, indicating a need for more structured guidance in this field. These theoretical frameworks included Participatory Action Research (PAR), the theory of planned behavior, behavior-change constructs, the patient-centered outcomes research (PCOR) framework, and prolonged exposure techniques within Islamic principles. The review identified three main health-focused intervention categories: mental health, prevention, and communication, each providing valuable insights into initiatives within Muslim communities.
Conclusions
This review underscores the significance of inclusive and culturally sensitive health interventions, emphasizing the effectiveness of faith-based approaches in improving health outcomes, promoting positive health behaviors, and addressing communication and cultural barriers. The reviews findings stress the need for further research that incorporates theoretical frameworks and tailored interventions to meet the specific cultural needs of these communities, ultimately contributing to enhanced well-being within them.
Impact Statement
Religion and religious institutes play a role in community health and well-being interventions by educating the community about chronic diseases and health disparities. This review highlights opportunities and areas for improvement by examining mosque-based health interventions. The review of 14 studies sheds light on the potential of interventions within Muslim communities to improve mental and physical health outcomes, promote positive health behaviors, and overcome communication and cultural barriers. The review also acknowledges that, based on the diversity of viewpoints among Imams, the structure of the Mosque and the community it serves, individual Mosques may not be an ideal intervention setting in all instances. This review highlights the need for more studies to incorporate explicit theoretical models into their methodologies and tailor interventions to meet the specific cultural needs of Muslim communities.
Recent research has highlighted the complex interplay of cultural, religious, and racial factors in health interventions, particularly among Muslims (S. Ahmad et al., 2022; S. S. Ahmad & Koncsol, 2022; McLaren et al., 2021; Wehbe-Alamah et al., 2021). For example, Sabado et al. (2022) and Khan et al. (2019) both found that acculturation to American values and less cultural beliefs about mental health were associated with more favorable attitudes toward seeking mental health services. Mitha (2020) emphasized the need for a nuanced understanding of mental health in Muslim communities, drawing on historical Islamic approaches. Hunt et al. (2020) underscored the unique mental health challenges faced by Muslim young adults and women, respectively, due to experiences of racial and religious discrimination. S. Ali et al. (2022) and Saherwala et al. (2021) identified the role of religious and cultural beliefs, stigma, and familiarity with health services in shaping attitudes toward professional mental health care. Finally, S. S. Ahmad and Koncsol (2022) highlighted the influence of collectivism on stigmatizing attitudes toward mental illness in Pakistani emerging adults. These studies collectively underscore the importance of culturally competent health care and the need for interventions that address the specific challenges faced by Muslim communities.
Retention and satisfaction levels with mental health and public health care services are lower for ethnic minorities compared with Whites (Castro-Olivo, 2014; Fortuna et al., 2010). People from marginalized backgrounds face challenges in accessing evidence-based care and often hesitate to seek psychological assistance due to stigma (Cook et al., 2017). The underutilization of mental health services is linked to increased stigma within some racial/ethnic minorities and concerns about therapy aligning with diverse cultural or religious beliefs (Khan et al., 2019; Wong et al., 2018). Negative perceptions of psychological treatment contribute to the reluctance to use mental health resources, emphasizing the importance of recognizing cultural and religious influences on individuals’ mental health experiences. While considerable efforts have been made in addressing the dimensions of culture, religion, and race in underserved populations (S. Ahmad et al., 2022; Mitha, 2020; Tanhan & Young, 2021; Weisman de Mamani et al., 2021), a need for further exploration of and action on how to appropriately contextualize and offer evidence-based care persists.
Studies have shown that culturally responsive interventions can lead to greater satisfaction, acceptance, and better health outcomes (G. C. Hall et al., 2016; Lauricella et al., 2016; Smith et al., 2011). Recent research highlights the enduring significance of religion in the lives of individuals, including health care providers (Palmer Kelly et al., 2020a, 2020b). Religious institutions, such as mosques and churches, play a vital role in community health and well-being interventions, traditionally serving as sanctuaries of hope, spiritual guidance, and social service (McLaren et al., 2021). Recognizing the importance of interventions aligning with the values, perspectives, and preferences of the target population, these endeavors are presumed to be more effective (Jumper-Reeves et al., 2014; Kaholokula et al., 2018). Religious institutions are shown to promote well-being (Brown et al., 2019; Flórez et al., 2020; Franz et al., 2017). Recently, religious institutions have also focused on educating the community about chronic diseases and health disparities, such as hypertension, diabetes, depression, anxiety, and obesity (Brewer & Williams, 2019).
With over 1.8 billion followers, Islam is the second largest religion in the world and is expected to exceed 3 billion followers by 2060, with the majority living in Africa, the Middle East, and Asia (Pew Research Center, 2017). It is common for Muslims to seek guidance from Imams in addition to medical professionals to address health and spiritual issues (O. M. Ali & Milstein, 2012). To provide culturally competent care, health care providers must respect and understand the cultural values and beliefs of Muslim patients (Gupta, 2015; Haque & Keshavarzi, 2014; Hussain, 2017; Owens et al., 2023).
A recent study shows that using Islamic moral belief systems makes it easier for health care providers and family members to promote medication adherence and provide comprehensive homebound care to Muslim elders (Perngmark et al., 2023). In addition to satisfaction with the program components, primary caregivers reported improved self-confidence, knowledge, and skills. In another study, it was found that the Muslim-Based Health Behavior Modification Program motivates patients to adopt healthier habits and lower their blood sugar levels (Makeng et al., 2018). However, it is critical to note that not all Muslims or Imams would find the use of mosque-based interventions appropriate. Caution should be exercised to ensure that the individual mosque and community it serves would be accepting of using the mosque for activities beyond communing and prayer; attention should be given to the culture and values of the mosque, including how it is structurally organized and governed, as well as the beliefs and expectations of its congregation before proposing it as a site of an intervention (Abu-Ras, 2011; Abu-Ras et al., 2008; Abu-Ras & Laird, 2011; King et al., 2017). Collaboration with community stakeholders, including Imams, community members, and health care practitioners can be a good way to understand how and where to best offer interventions (Abu-Ras, 2011; Abu-Ras et al., 2008; Christie-de Jong et al., 2022; Heirali et al., 2021; McLaren et al., 2021).
A recent systematic review proposed an exploratory conceptual framework to further understand how Islamic beliefs, traditions, practices, values, and identity could contribute to health inequities among Muslims as well as the interplay between constructs that contribute to these disparities in Muslim communities (Padela & Zaidi, 2018). However, according to Padela and Zaidi (2018), a major limitation was the lack of examination and assessment of the influence of Islamic religious figures and mosques in promoting health care behaviors or health promotion. Therefore, this scoping review of the literature on the outcomes of health-promoting interventions that use mosques as the location of the interventions aims to address this gap. It also aims to investigate the role of mosques in promoting behavioral health change and assess the role of theory in each intervention. By highlighting opportunities and areas for improvement and examining the role of theory in each intervention, this scoping review can guide future mosque-based health interventions.
Methods
Literature Search Procedures
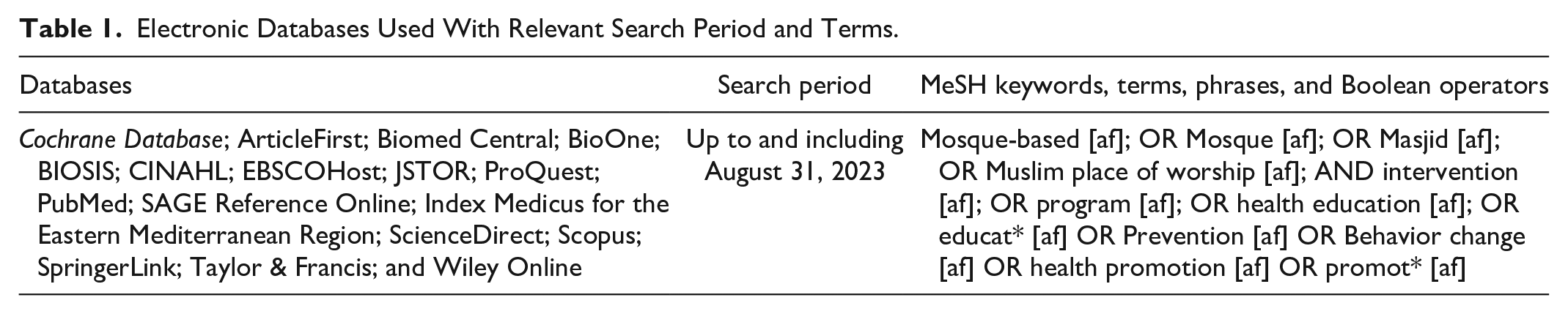
For this review, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Scoping Reviews (PRISMA-ScR) guidelines were followed (Tricco et al., 2018). In addition, the proposed review protocols Mustafa et al. (2017) outlined were incorporated. Seventeen databases were searched using keywords, terms, phrases, and Boolean operators relevant to the topic (see Table 1). The search strategies were adapted according to the indexing systems of each respective database. The reference lists from retrieved articles were also manually reviewed to ensure all relevant articles were captured. Finally, all articles were screened for eligibility, relevance, and alignment with the review’s objectives.
Electronic Databases Used With Relevant Search Period and Terms.
Selection Criteria
To develop the inclusion and exclusion criteria for this review, the Population, Intervention, Comparison, Outcomes, and Study (PICOS) design guidelines were followed (Higgins et al., 2019) (see Table 2). Peer-reviewed articles published in either English or Arabic languages were focused on, while excluding interventions reported outside the scope of traditional peer-reviewed articles. The search was conducted in the summer of 2023, and the literature reported in this review was published up to and including August 2023.
PICOS Criteria for Inclusion and Exclusion of Studies.
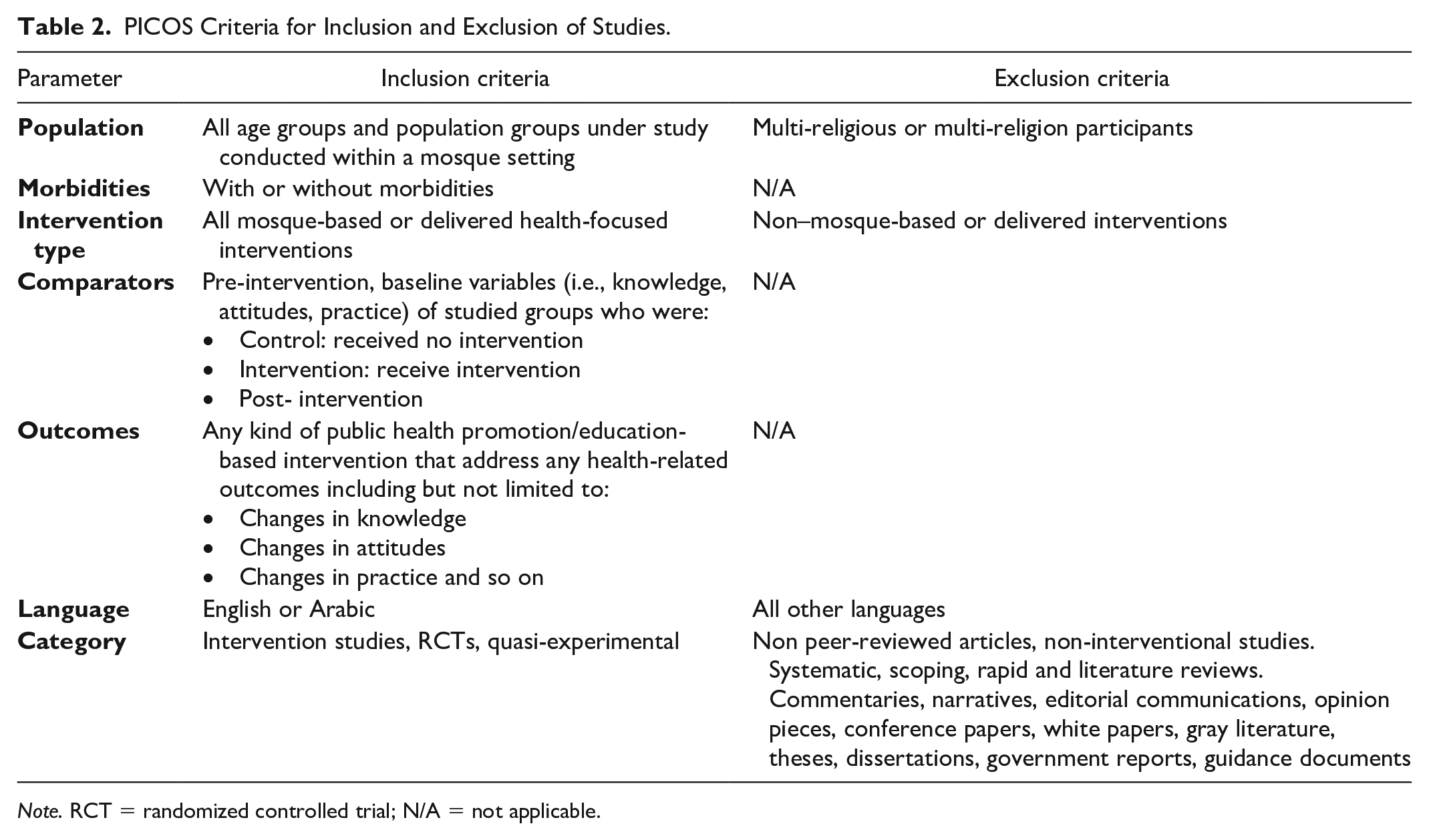
Note. RCT = randomized controlled trial; N/A = not applicable.
Study Selection and Data Extraction
Two authors conducted the literature search independently and selected relevant studies for inclusion. Any potential differences were discussed, and consensus was reached; one author resolved discrepancies if needed. One author did the extraction and tabulation of data and the data were independently checked by two other authors (Ouzzani et al., 2016) to assist in the screening process and study selection. Titles and abstracts were screened for relevancy and reviewed by three authors. Relevant studies for inclusion were independently evaluated by each author for relevance, merit, and inclusion/exclusion criteria (Table 2). All selected articles were then discussed with the primary author before the final decision for inclusion (Figure 1 and Table 3). Once the list of selected studies was finalized, all five authors extracted and cross-checked the following for each study: Authors (year), the study included information on Location and settings, Sample size, Study Design, Program Focus, Length of intervention, Aim of Intervention, Theory Applied/ Intervention Characteristics, and Outcomes/Findings (see Table 3). As this review solely focused on published journal articles, institutional review board’s (IRB) approval was not necessary nor obtained. In addition, since methodological quality assessment is not required for scoping reviews, the included studies were not appraised (Peters et al., 2020).
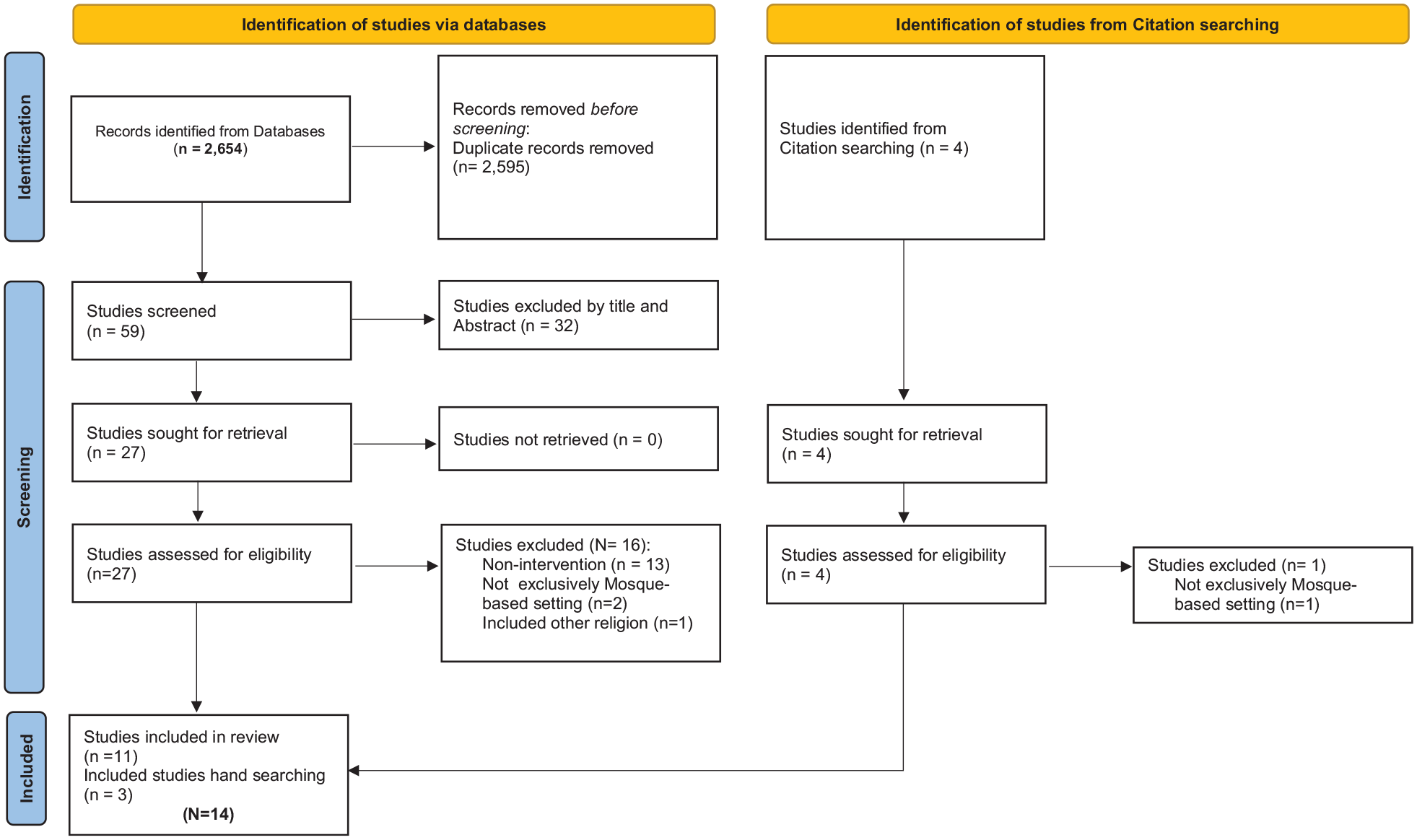
PRISMA 2020 Flow Diagram.
Summary of Literature Search (N = 14).
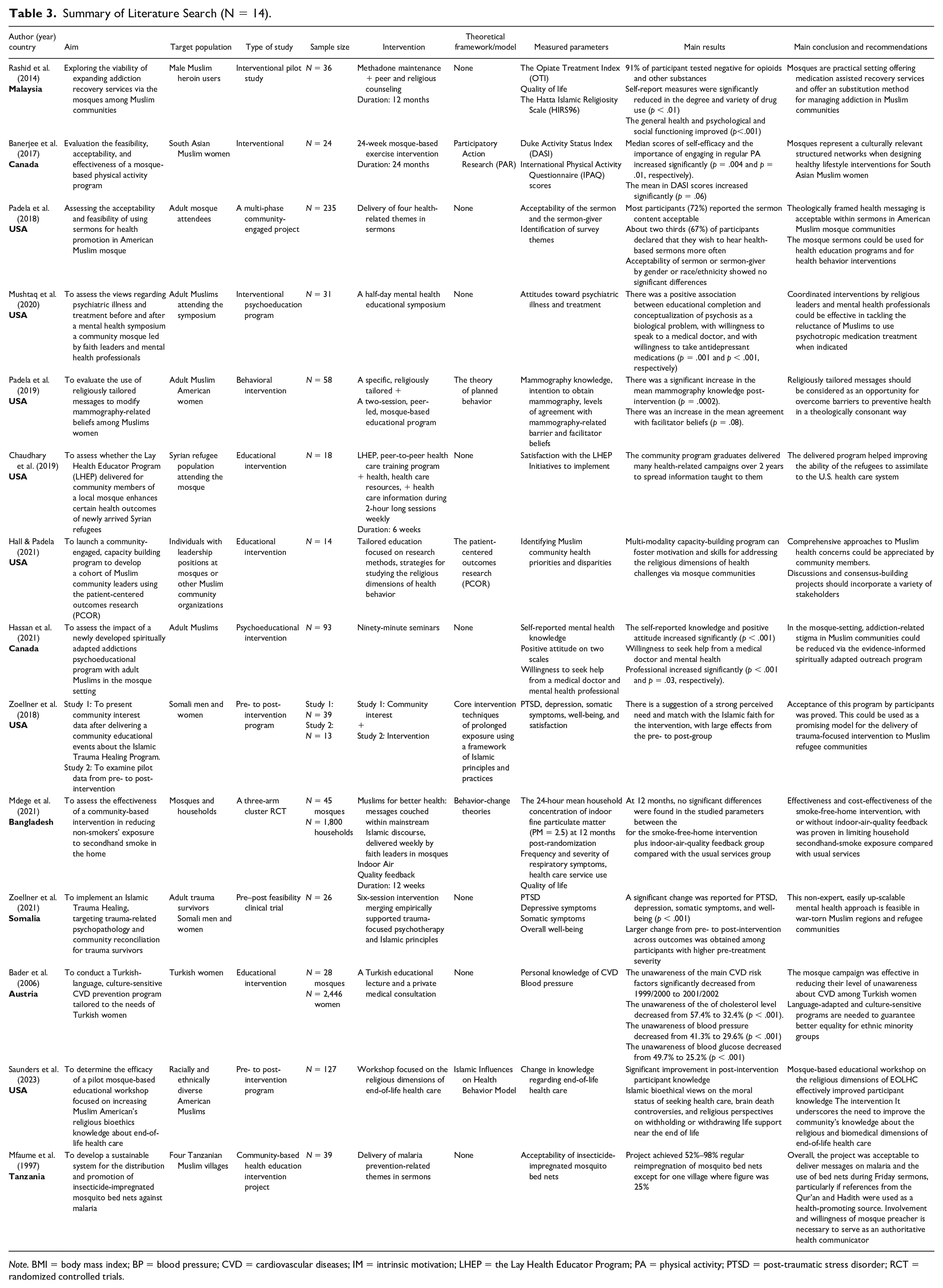
Note. BMI = body mass index; BP = blood pressure; CVD = cardiovascular diseases; IM = intrinsic motivation; LHEP = the Lay Health Educator Program; PA = physical activity; PTSD = post-traumatic stress disorder; RCT = randomized controlled trials.
Results
This review analyzed 14 studies conducted between 1997 and 2023 across six different countries, including the United States (Chaudhary et al., 2019; S. Hall & Padela, 2021; Mushtaq et al., 2020; Padela et al., 2018, 2019; Saunders et al., 2023; L. Zoellner et al., 2018), Canada (Banerjee et al., 2017; Hassan et al., 2021), Bangladesh (Mdege et al., 2021), Malaysia (Rashid et al., 2014), Somalia (L. A. Zoellner et al., 2021), Tanzania (Mfaume et al., 1997), and Austria (Bader et al., 2006). The studies featured a range of research designs, with the majority being interventional studies (Bader et al., 2006; Banerjee et al., 2017; Chaudhary et al., 2019; S. Hall & Padela, 2021; Hassan et al., 2021; Mushtaq et al., 2020; Padela et al., 2019; Rashid et al., 2014; Saunders et al., 2023; L. Zoellner et al., 2018). Two studies were community-engaged projects (Mfaume et al., 1997; Padela et al., 2018), and one study utilized a three-arm cluster randomized controlled trial (RCT) design (Mdege et al., 2021). In addition, a pre–post feasibility clinical trial was also included in the review’s analysis (L. A. Zoellner et al., 2021).
Of the studies that were examined, six of them used a theoretical framework or model in their methodologies. In one study (Banerjee et al., 2017), the Participatory Action Research (PAR) model was utilized to evaluate a mosque-based physical activity program. Another study (Padela et al., 2019) used the theory of planned behavior to evaluate the use of religiously tailored messages to modify mammography-related beliefs among Muslim women. One study (Mdege et al., 2021) examined behavior-change constructs in their community-based intervention to reduce non-smokers’ exposure to secondhand smoke. One study (S. Hall & Padela, 2021) employed the patient-centered outcomes research (PCOR) framework in their initiative to develop a cohort of Muslim community leaders through a community-engaged capacity-building program. One study (L. Zoellner et al., 2018) integrated core intervention techniques of prolonged exposure within an Islamic principles and practices framework in their study on community interest in the Islamic Trauma Healing Program. Finally, one study used Islamic influences on Health Behavior Model as part of an end-of-life health care workshop (Saunders et al., 2023).
Across the 14 studies, a diverse range of interventions was implemented, encompassing clinical methodologies, religiously tailored educational programs and sermons, and a hybrid of both. Educational seminars and sessions were featured in six of the studies (Bader et al., 2006; Chaudhary et al., 2019; S. Hall & Padela, 2021; Hassan et al., 2021; Mushtaq et al., 2020; Saunders et al., 2023). In one study (Chaudhary et al., 2019), a peer-to-peer health care training program was utilized, consisting of 2-hour-long weekly sessions over 6 weeks, aimed at improving knowledge of health, health care resources, and information. Another study (Bader et al., 2006) incorporated these sessions with private medical consultations.
Several interventions have been implemented to address health-related issues within Muslim communities. One intervention involved methadone maintenance combined with peer and religious counseling for 12 months (Rashid et al., 2014). Another intervention was a 24-week mosque-based exercise program (Banerjee et al., 2017). Health-related themes were also delivered in sermons (Padela et al., 2018). The “Muslims for Better Health” program involved weekly messages from faith leaders in mosques, using mainstream Islamic discourse and feedback on indoor air quality. This program lasted for 12 weeks (Mdege et al., 2021). In addition, a six-session program was developed to merge empirically supported trauma-focused psychotherapy with Islamic principles (L. A. Zoellner et al., 2021). Finally, one study utilized prolonged exposure using Islamic principles and practices (L. Zoellner et al., 2018).
Various physical, mental, and religious health metrics were measured in these studies. For example, the Opiate Treatment Index (OTI), quality of life, and the Hatta Islamic Religiosity Scale (HIRS96) were assessed in one study (Rashid et al., 2014). Physical activity was evaluated using the Duke Activity Status Index (DASI) and the International Physical Activity Questionnaire (IPAQ) scores in another study (Banerjee et al., 2017). Sermons were evaluated for acceptability (Padela et al., 2018), while surveys identified key themes and attitudes toward psychiatric illness and treatment (Mushtaq et al., 2020). One study (Padela et al., 2019) measured mammography knowledge, intention to obtain mammography, and barriers and facilitators. The effectiveness of the Local Health Education Program (LHEP) and the initiative to implement it was measured in one study (Chaudhary et al., 2019), while another study examined post-traumatic stress disorder (PTSD; L. Zoellner et al., 2018; L. A. Zoellner et al., 2021), depression (L. A. Zoellner et al., 2021), somatic symptoms and well-being (L. Zoellner et al., 2018; L. A. Zoellner et al., 2021), and patient satisfaction (L. Zoellner et al., 2018). Finally, one study (Mdege et al., 2021) focused on environmental health, specifically indoor fine particulate matter (PM = 2.5) levels, respiratory symptoms, health care service use, and quality of life. Personal knowledge of cardiovascular disease (CVD) and blood pressure were included as health metrics in the study (Bader et al., 2006). The review’s results fall into three categories:—mental health, prevention, and communication and culture.
Mental and Psychological Health
Six studies (Hassan et al., 2021; Mushtaq et al., 2020; Rashid et al., 2014; Saunders et al., 2023; L. Zoellner et al., 2018; L. A. Zoellner et al., 2021) focused on mental health, trauma, end-of-life health care, and addiction recovery. Two studies (L. Zoellner et al., 2018; L. A. Zoellner et al., 2021) implemented an Islamic Trauma Healing program among Somali men and women, showing significant changes in PTSD, depression, somatic symptoms, and well-being. Hassan et al. (2021) reported that a spiritually adapted addictions psychoeducational program significantly increased self-reported knowledge and positive attitude. Mushtaq et al. (2020) found that a mosque-based mental health promotion program significantly improved mental health literacy and reduced stigma. Rashid et al. (2014) explored the viability of expanding addiction recovery services via mosques among Muslim communities, with 91% of participants testing negative for opioids and other substances after their intervention. One study (Saunders et al., 2023) was designed to determine the efficacy of a mosque-based educational workshop focused on increasing religious bioethics knowledge about end-of-life health care.
Prevention and Health Behavior
Seven studies (Bader et al., 2006; Banerjee et al., 2017; Chaudhary et al., 2019; Mdege et al., 2021; Mfaume et al., 1997; Padela et al., 2018, 2019) were conducted on health behavior and lifestyle. Banerjee et al. (2017) evaluated the feasibility, acceptability, and effectiveness of a mosque-based physical activity program. They discovered that the program increased self-efficacy and emphasized the importance of engaging in regular physical activity. Bader et al. (2006) conducted a Turkish-language, culture-sensitive CVD prevention program tailored to Turkish women. The study revealed that the mosque campaign was effective in reducing the level of unawareness about CVD. Mdege et al. (2021) assessed the effectiveness of a community-based intervention in reducing non-smokers’ exposure to secondhand smoke. The intervention was found to be effective. Chaudhary et al. (2019) assessed whether the Lay Health Educator Program (LHEP) delivered to community members of a local mosque enhances certain health outcomes of newly arrived Syrian refugees. They found that the community program graduates delivered many health-related campaigns over 2 years to spread information taught to them. The delivered program helped improve the ability of the refugees to assimilate into the U.S. health care system. One community-based health education intervention project (Mfaume et al., 1997) developed a mosque-based sermon-led program for the distribution and promotion of insecticide-impregnated mosquito bed nets for malaria prevention among Tanzanian villagers. Finally, Padela et al. (2018, 2019) conducted two studies to describe religiously tailored, peer-led group education programs to address barrier beliefs impeding mammography screening among Muslim American women. Both studies were significantly effective.
Communication and Culture
In the realm of communication and culture, two studies were conducted. One study (Padela et al., 2018) examined the feasibility of using sermons to deliver health-related messages, with most participants finding the sermon content acceptable. S. Hall and Padela (2021) launched a community-engaged, capacity-building program to develop a cohort of Muslim community leaders using PCOR, finding that community members appreciated comprehensive approaches to Muslim health concerns.
Discussion
The results of this review study include 14 studies conducted between 1997 and 2023 in six different countries, utilizing various research designs. Predominantly focused on interventions, the studies underscore the importance of addressing health concerns within Muslim communities. However, only six studies incorporated a theoretical framework or model into their methodologies, suggesting a need for established theories to guide research in this field.
Among the theoretical frameworks and models used, the PAR model was employed in one study, emphasizing community engagement in evaluating a mosque-based physical activity program. The theory of planned behavior was utilized in another study to assess the effectiveness of religiously tailored messages in modifying mammography-related beliefs among Muslim women. Behavior-change theories were applied in two studies that aimed to reduce non-smokers’ exposure to secondhand smoke through community-based interventions. The PCOR framework played a role in developing a cohort of Muslim community leaders through a capacity-building program. In addition, core intervention techniques of prolonged exposure were integrated within an Islamic principles and practices framework in one study focused on the Islamic Trauma Healing Program. Ritual communication was used in assessing the effects of a communication intervention designed to improve Jordanian religious leaders’ communication about family health.
Throughout the 14 studies, a diverse array of interventions was examined, encompassing clinical techniques and educational programs tailored to religious beliefs, as well as those that combined both. The review included various research designs and interventions for improving health in Muslim communities across nations. However, there is an opportunity for more studies to use explicit theoretical models and tailor interventions to meet the cultural needs of these communities. Three main health-focused intervention categories emerged from this review: mental health, prevention, and communication, all providing valuable insights into the impact of such interventions in Muslim communities.
Mental and Psychological Health
The findings in this category highlight the effectiveness of culturally tailored programs in addressing mental health, trauma, end-of-life health care, and addiction recovery. Each of the articles reviewed had positive findings in this category L. Zoellner et al. (2018), L. A. Zoellner et al. (2021), Hassan et al. (2021), Mushtaq et al. (2020), Rashid et al. (2014) and Saunders et al. (2023).Other reviews have found varying neutral to positive outcomes from culturally tailored mental and psychological health interventions offered in religious settings (Hankerson & Weissman, 2012; Hays & Aranda, 2015; Singh et al., 2012). The literature also notes the positive effects of culturally tailored mental health interventions in various other settings (Caplan, 2019; Castro-Olivo, 2014; Codjoe et al., 2021; Hays & Aranda, 2015; Kohn-Wood & Hooper, 2014; Owens et al., 2023). While promising work has been done in this area, the literature notes that research gaps remain in determining the most effective approaches to the design and implementation of faith-based interventions including those offered in a religious setting, as well as reducing stigma that might be related to mental health interventions in religious settings (Caplan, 2019; Codjoe et al., 2021; Hankerson & Weissman, 2012; Hays & Aranda, 2015; Pottinger et al., 2021).
In addition to the limitations noted and need for future research regarding mental health interventions in religious settings, other areas for investigation emerged. These include the need to address the role of religious leaders comfort with and ability to offer guidance around mental health; several studies investigated the comfort levels of spiritual leaders with mental health counseling and noted that collaboration with local social work or mental health practitioners is imperative when considering the development of such interventions, and/or referrals to professionals. Depending on the willingness of the spiritual leaders, the resources available, and the receptivity of the spiritual community, places of worship, including mosques, could be ideal settings for culturally tailored mental health-based interventions due to the regularity of gatherings, existing sense of belonging, and community support (Abu-Ras et al., 2008; O. M. Ali, 2016; Burse et al., 2021; Campbell & Winchester, 2020; Goodman & Witztum, 2002; Mushtaq et al., 2020; Ojelade et al., 2023; Schnall et al., 2016).
Prevention and Health Behavior
The seven studies (Bader et al., 2006; Banerjee et al., 2017; Chaudhary et al., 2019; Mdege et al., 2021; Mfaume et al., 1997; Padela et al., 2018, 2019) in this category focused on promoting positive health behaviors within Muslim communities, and found positive effects across the reviewed literature. Culturally tailored health promotion and health behavior-change interventions have also been found to be accepted and effective in other religious settings and communities (Bopp et al., 2012; Burton et al., 2017; Freund et al., 2017; Hou & Cao, 2018; Schwingel & Gálvez, 2016). Furthermore, evidence exists that culturally tailoring health promotion and health behavior-change interventions can increase the effect of and adherence to the target behaviors in a variety of settings, including schools, community centers, and through web-based interventions. However, gaps remain in assessing long-term impacts of such behavior-change interventions, the best approaches to integrating cultural adaptations to theoretical or behavioral change frameworks that may include more “westernized” constructs, and the varying degrees of training that those offering the intervention might have with the culture they are working with (Chandler et al., 2021; Ehrlich et al., 2015; Heo & Braun, 2014; Joo & Liu, 2021; Leinberger-Jabari et al., 2024; McCurley et al., 2017; Nierkens et al., 2013).
Similar to mental health and psychological interventions, religious leaders may have varying levels of comfort with offering their places of worship for conducting such interventions. Therefore, the design of the interventions should be a collaborative effort with input from religious leaders, their communities, health professionals, and if different from the practitioners, the individuals offering such initiatives (Carter-Edwards et al., 2012; Cohen-Dar & Obeid, 2017; Fagan et al., 2012; Heward-Mills et al., 2018; Peterson et al., 2002; Schoenberg & Swanson, 2017; Zini et al., 2015). While this review finds that the mosque can be an effective setting in which to offer health promotion and health behavior-change interventions, the willingness of mosque preachers, as well as proactive involvement and collaboration with them is necessary to implementing such initiatives (Mfaume et al., 1997).
Communication and Culture
The final area of focus in this review explores how communication and culture can contribute to better health outcomes in Muslim communities. The research indicates that incorporating cultural and religious beliefs into faith-based interventions can have a positive impact on health outcomes. Communication and culture have emerged as an important theme in the literature as related to other health- and faith-based initiatives as well (Allegranzi et al., 2009; Anshel & Smith, 2014; Baldwin & Poje, 2020; Kwon et al., 2017; Lumpkins et al., 2013; Rivera-Hernandez, 2015; Schwingel & Gálvez, 2016). Indeed, this is an important topic that has been analyzed and discussed in terms of culture regardless of religious affiliation (Baezconde-Garbanati et al., 2014; Betsch et al., 2015; Dickerson et al., 2020; Estrada et al., 2018; Lohr et al., 2022; Netto et al., 2010). Culturally tailored interventions are effective, emphasizing the importance of community-based approaches to enhance well-being.
This review highlights the effectiveness of culturally tailored interventions in addressing mental health, addiction recovery, and promoting positive health behaviors within Muslim communities. It emphasizes the significance of designing health care programs that respect and incorporate cultural beliefs, norms, and practices. In addition, the research underscores the value of faith-based approaches in improving mental and physical health outcomes. Faith-based interventions, such as the Islamic Trauma Healing program and addiction recovery services through mosques, have demonstrated positive results. This suggests that religious institutions can play a pivotal role in providing support and guidance for community members facing mental health and addiction challenges.
The review also suggests that this intervention may help in reducing stigma related to mental health and addiction issues. Mosque-based mental health promotion programs and addiction recovery services have successfully reduced stigma and improve mental health literacy. This indicates that addressing stigma can be a crucial step in encouraging individuals to seek help and support. Furthermore, the success of community-based programs like the LHEP and community-led education initiatives emphasizes the value of community engagement in promoting health. These programs not only enhance health outcomes but also help Muslim refugees and immigrants integrate into health care systems and showcasing the potential for community-driven solutions. Moreover, the findings in the Communication and Culture category stress the importance of incorporating cultural and religious beliefs into health interventions. These interventions, such as faith-based programs for breast cancer screening and tobacco cessation, have proven effective in aligning with the unique cultural context of Muslim communities.
Limitations
The limitations of this review include the limited use of theoretical frameworks in the reviewed studies, which may impact the depth of intervention design. The diversity of interventions, lack of standardized approaches, and geographical variability across countries make it challenging to draw generalized conclusions. In addition, there is limited theoretical diversity in the frameworks employed, potential publication bias due to reliance on published studies, and a lack of long-term follow-up data to assess intervention sustainability. Methodological heterogeneity, variations in cultural sensitivity, and a focus on positive outcomes rather than negative ones further contribute to the limitations. Sampling bias within the study samples may affect the generalizability of findings to broader Muslim communities. Addressing these limitations through future research will enhance our understanding of health interventions within these communities.
Implications for Future Research
Building on the insights derived from the reviewed studies, and the study results, future research directions should prioritize the incorporation of explicit theoretical models to guide interventions within Muslim communities. The limited use of theoretical frameworks in the existing literature underscores the need for a more structured approach to intervention design and evaluation. Researchers should consider embracing a diverse range of theoretical foundations to enrich the depth and comprehensiveness of health care programs.
Moreover, there is a significant opportunity for studies to adopt standardized approaches and overcome geographical variability, allowing for more robust cross-cultural comparisons. The diversity of interventions, while valuable, necessitates a move toward establishing common frameworks for assessment, enabling more reliable generalizations and facilitating the development of best practices.
In addition, addressing the identified limitations, such as potential publication bias, methodological heterogeneity, and the lack of long-term follow-up data, should be prioritized. Future studies should aim for more extensive and diverse sampling to enhance the generalizability of findings to broader Muslim communities. A focus on negative outcomes alongside positive ones will provide a more comprehensive understanding of intervention efficacy and sustainability.
To conclude, future research endeavors should focus on refining intervention methodologies, incorporating diverse theoretical frameworks, standardizing approaches, and addressing existing limitations. This will contribute to advancing the field of health care interventions in Muslim communities, ensuring culturally sensitive, effective, and sustainable programs that cater to the unique needs of these populations.
Conclusion
This review sheds light on the potential of interventions within Muslim communities to improve mental and physical health outcomes, promote positive health behaviors, and overcome communication and cultural barriers. The studies collectively emphasize that culturally sensitive and faith-based interventions can be highly effective. They underscore the significance of designing health care programs that respect cultural norms and religious beliefs, as well as the role of religious institutions like mosques in providing support and guidance. In addition, the research highlights the need for more studies to incorporate explicit theoretical models into their methodologies and tailor interventions to meet the specific cultural needs of Muslim communities. Such approaches can further enhance the effectiveness of health care interventions and contribute to improved well-being within these communities. In conclusion, this study emphasizes the value of inclusive and culturally sensitive health interventions, promoting the importance of community-based approaches and the potential for religious institutions to play a vital role in supporting mental health, addiction recovery, and positive health behaviors in Muslim communities.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.